
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care Volume 2 (2017), Article ID: JCNRC-110
https://doi.org/10.33790/jcnrc1100110Research Article
The Benefits and Issues Regarding Sick Child Care Services in Doubleincome Nuclear Families with Children
Chizuko Edagawa1, Ikuko Sobue2*
1Department of Nursing, Faculty of Health Sciences, Ehime Prefectural University of Health Sciences, Japan
2Division of Nursing Science, Graduate School of Biomedical & Health Sciences, Hiroshima University, Hiroshima 734-8553, Japan
Corresponding Author Details: Ikuko Sobue, Graduate School of Biomedical & Health Sciences, Hiroshima University, 1-2-3 Kasumi, Minami-ku, Hiroshima 734-8553, Japan. E-mail: sobue@hiroshima-u.ac.jp
Received date: 13th May, 2017
Accepted date: 09th July, 2017
Published date: 25th August, 2017
Citation: Edagawa, C., & Sobue, I. (2017). The benefits and issues regarding sick child care services in double-income nuclear families with children. J Comp Nurs Res Care 2(1): 110.
Copyright: ©2017, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Purpose: As the benefits of sick child care services are usually evaluated based on parents’ work-related views, very few studies have reported those on health recovery or parenting of sick children. This study investigated the usage and evaluation of sick child care services in double-income nuclear families, in order to clarify their benefits and issues.
Methods: This study used a qualitative and descriptive approach. Semi-structured interviews were conducted involving 27 mothers of double-income nuclear families after obtaining their written consent.The survey consisted of: the age and number of children, child-raising status, strategies to cope with children’s illness, and usage and needs of sick child care services and pediatric emergency medical care services.
Results: The mothers of double-income nuclear families worked with hope of self-realization. They used sick child care services to balance their child-raising and career in a situation where there is no one to rely on. By experiencing positive reactions and early recovery of their children, the mothers developed a sense of security and trust towards high quality medical, nursing, and child nursery care of the service and childcare education provided to mothers. On the other hand, they desired improvement with regard to expensive care fees, short-hours of service, and the capacity to accept children, as well as the operation of transportation service from nursery school to the sick child care facility
Conclusions: The results of this study demonstrated that sick child care services were beneficial in promoting healthy recovery of children and for improving childcare skills of mothers of doubleincome nuclear families. The results also suggest the need to develop measures based on the needs of sick child care users.
Keywords: Benefit, Child-raising support, Double-income nuclear family, Sick child care services
Introduction
With a rapidly declining birthrate and growing trendof nuclear families, the number of double-income households is increasing every year. Of the general households with children, the number of double-income families has increased from 6.42 million (34.0%) in 1990 to 7.08 million (42.0%) in 2010 [1]. For working parents, the care of sick children often presents a dilemma, particularly for parents with small babies who are susceptible to infections,as it places a great burden.
Parents’ actions taken when their children become sick included placing children in the care of their grandparents, taking the day off from work, or using sick child care services [2]. However, another study also reported the presence of mothers who have no relatives to look after their child and feel difficulties taking the day off from work [3].
Sick child care service is provided by the government [4]. If parents are unable to care for a sick child, such as because of their job, the child is cared for temporarily by nursery staff and nurses. This service provides total child care, and allows parents to both raise children and work [5,6]. More than 2,200 sick child care facilities were used by about 610,000 children in 2015 [7].
To provide sick child care, it is necessary to secure an appropriate number of facilities and service in accordance with the number and characteristics of users [8]. However, as far as the authors are aware, the needs of users are evaluated with the aim of supporting parents’ career [2,9]; thus, very few studies have reported the benefits on children’s health and child-raising [10,[11]. To provide sick child care according to the needs of users, the investigation of the characteristics of users and evaluation of supporting measures are essential. In this study, we investigated the usage of sick child care services by double-income nuclear families in order to examine the benefits and issues for such families.
Study Purpose
1. To clarify the usage and evaluation of sick child care services by double-income nuclear families. 2. To clarify the benefits and issues of using sick child care services for double-income nuclear families.
Study Methods
Study design: Qualitative and descriptive research
As a part of a study titled, “The examination of child-raising support to promote parents’ sense of security towards and appropriate use of pediatric emergency medical care services”, we conducted semistructured interviews between April and May 2011 involving 27 of double-income nuclear families residing in A City.In this study, we reported the benefits of sick child care services for double-income nuclear families. The subject inclusion criteria were: (1) parents who use sick child care services, (2) parents who have children under 6 years of age, (3) both parents work full time, and (4) parents who have used pediatric emergency medical care services(during out-ofservice hours).
Semi-structured interviews were conducted using an interview guide. The survey consisted of the age and number of children, childraising status, strategies to cope with children’s illness, and usage and needs of sick child care and pediatric emergency medical care services.
Subjects were recruited through the website as well as printed advertisements placed in and application forms distributed by 8 sick child care facilities located in the prefecture. Written informed consent was obtained from the subjects after explaining the study’s purpose and design, and that their rights to participate in this study should be based on free will, that there will be no penalty even if they choose not to participate, and that they are free to withdraw at any time,in both oral and written forms. Considering the convenience of the subjects, the interviews were conducted in private rooms within 4 public facilities in A Prefecture or the researchers’ institution where the subject’s privacy is ensured. Each subject received an approximately one-hour interview. The interviews were recorded when consent was granted. To prevent the identification of individuals, linkable anonymized data were created from the obtained information. This study was conducted with the approval of the research ethics committee of the research director’s institution (Approval No. Heisei22-75).
The interview data of each subject was transcribed verbatim, and descriptions about the use and evaluation of sick child care services were extracted and encoded by content. The encoded data were labeled according to their similarities, based on which the data were divided into categories and subcategories. To ensure the credibility and validity, the data analysis was supervised by researchers specializing in pediatric nursing. In the text, categories, subcategories, and labels are indicated in [ ], < >, and “ ”, respectively.
Results
The subjects were 27 mothers (mean age: 34.1+4.26 years) from double-income nuclear families residing in A Prefecture. Twenty-one mothers (77.7%) worked full time. The mean number of children was 1.9 +0.9, and mean age of infants was 3.0 +1.33 years.
The [employment status] of the mothers was divided into
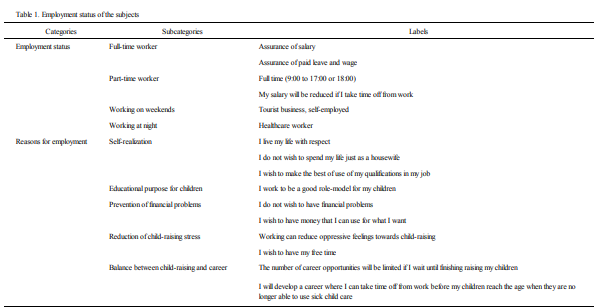
Table 1: Employment status of the subjects.
1. Use of sick child care service (Table 2)
The mothers obtained [information] on sick child care services from
their
[Reasons] for using sick child care service included:
< Public opinions> included: “Mothers are sacrificing their children
for their career”and “I feel pity for the children”. At the [initial use of
the service], “refusal of the service” and “crying and screaming”were
observed as
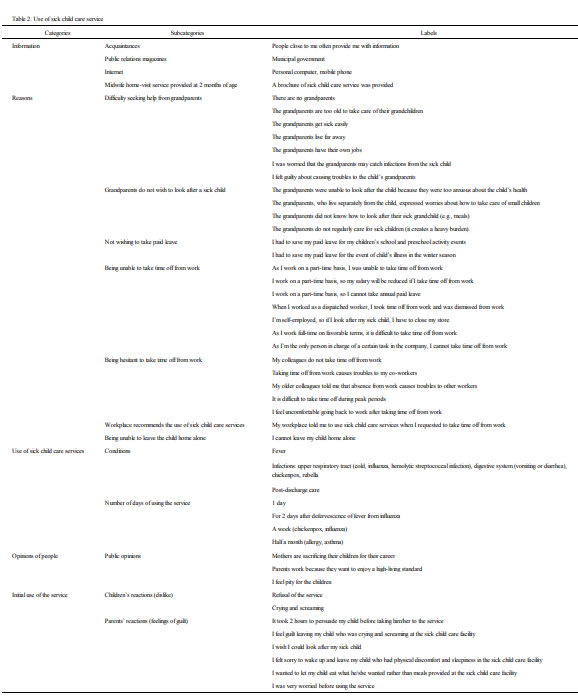
Table 2: Use of sick child care service.
2. Care and benifits of sick child care services (Table 3)
As [medical, nursing, and child nursery care], the parents highly
evaluated
The parents recognized the sick child care’s [benefits for children]
through positive reactions of their children, such as “children enjoy
staying at care facilities”and “children look forward to going to care facilities”. In addition, the parents felt that “the disease does not
last long”and “children can recover earlier when they were cared
by the facility” based on
Sick child care’s [benefits for parents] included:
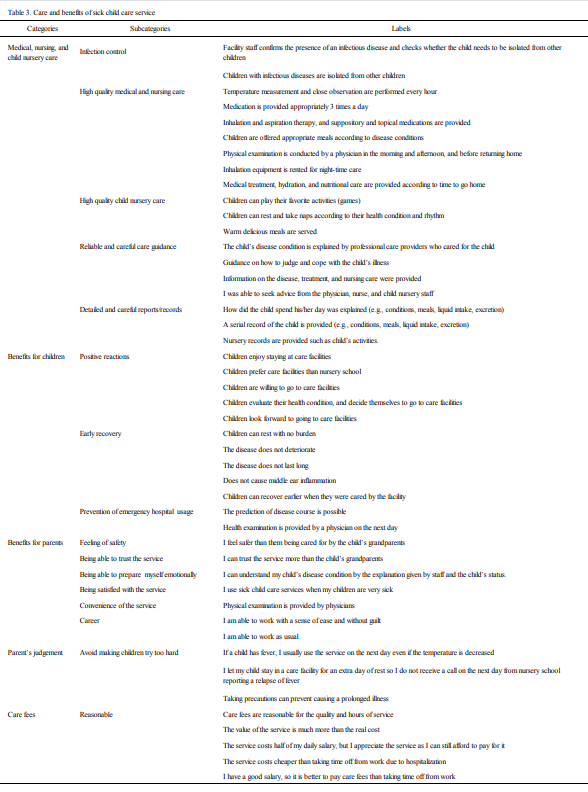
Table 3: Care and benefits of sick child care service.
3. The needs for sick child care (table 4)
The parents’ [problems] of using sick child care services included:
The parents’ [requests] regarding sick child care services included:
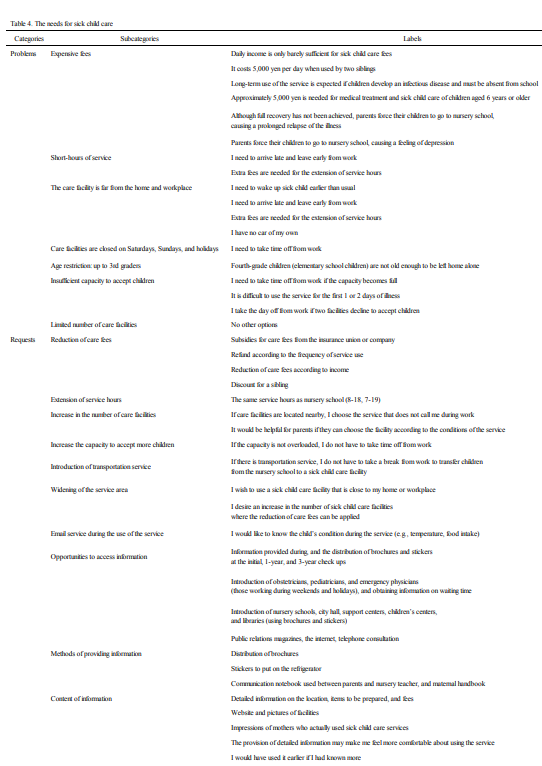
Table 4: The needs for sick child care.
Discussion
1. Use of sick child care servicesin double-income nuclear families
The employment status of the 27 mothers from double-income nuclear families was divided into different types, such as full-and part-time workers, working on weekends,and working at night. They continued their job because they had positive attitudes towards their work and had to resolve life-related problems. The mothers tried to be a good role-model for their children while living their life with respect. Although sick child care services were available until 7 pm, because children are no longer able to use it after entering elementary school, the mothers tried to seek an optimal work-life balance in their career with a long-term perspective, as expressed in their opinion, “I will develop a career where I can take time off from work before my children reach the age when they are no longer able to use sick child care”. For mothers of double-income families, their career is not only a means of earning a living, but also a means of establishing their life based on their values while caring about themselves as parents.
The reasons for using sick child care services included having no nearby relatives to look after their child, being unable to take time off from work, and being unable to leave children home alone. The increase in the number of double-income nuclear families can bring about both financial independence of grandparents and a decline in mutual support functions of extended families such as taking care of grandchildren. Grandparents observed in this study also had difficulty supporting the mothers because of their career or the lack of involvement with their grandchildren who live separately from them. The mothers had developed a conflict between work and childraising due to the lack of support from grandparents, anxiety over salary reduction and employment, and difficulties taking time off from work for school activities.
The presence of supporters with whom parents can leave their children safely is essential in order to resolve a dilemma between parental and career responsibilities [12]. In Japan, in responding to the collapse of social capital, including family structures [13], the government has been promoting several child-raising measures (e.g., child-raising leave and child care system) [14]. People who provide child-raising support will soon change fromthegrand parents to nursery centers or sick child care facilities, and such care services have now become an important resource to support the career-child raising balance of double-income nuclear families.
2. Care and benefits of sick child care services
The mothers positively evaluated sick child care services as high
quality medical, nursing,and child nursery care.Many previous
studies evaluated the benefits of the services based on parents’
work-related views [2,9]; however, in this study, medical, nursing,
and child nursery care of the service, and detailed reports /records
and care guidance provided by facility staff were evaluated as
beneficial by the mothers. This evaluation was consistent with the
philosophy of sick child care of Japan Sick Children Association [5]
and functions of sick child care services perceived by sick child care
staff [6,15-17]. The philosophy of sick child care is to guaranstee
total care of children, and the purpose of child-raising support for
parents is to promote the sound growth and development of children.
Based on this philosophy, nurses and nursery staff at sick child care
facilities perceive its functions as the achievement of pain relief and
early recovery of sick children, and the provision of care guidance
and child-raising advice toparents. The care practiced based on this
philosophy has promoted comfortable care and early recovery of
children, as well as mothers’ knowledge on appropriate care for their
children, contributing to providing mothers and children with a sense
of security, trust, and satisfaction regarding sick child care services.
Moreover, health management performed by the mothers,
3. Future issues regarding sick child care services
Difficulties of using sick child care services in double-income nuclear families included care fees, service hours, and the age limit for utilizing the services. These problems were also reported in the previous studies [18,[19].For example, Takahashi [20] reported the issues of sick child care servicesas follows: (1) Too much personal expense for care fees, (2) short hours of service, (3) a limited number of sick child care facilities within the area of everyday social activities, and (4) the lack of publicity about sick child care services. In this study, the mothers considered care fees expensive because of their lower-income, simultaneous use by 2 or more siblings at one time, prolonged use of the service, and burden of paying fees for both nursery school and medical treatment. Short-hours of service and long-distance travel to the service caused problems of late arrivals to and early departures from work as well as the need to pay extra fees to extend service hours. In addition, due to problems with an insufficient capacity to accept children, a limited number of care facilities, and no service on Saturdays, Sundays, and holidays, the parents had no choice but to take time off from work.
The requests of the parents included resolving the present issues and expanding the service, such as the reduction of care fees, longer service hours, and anincrease in the number of care facilities and the capacity to accept children. They also desired for the development of new types of services such as transportation service from the nursery school to sick child care facility and opportunities for parents to visit care facilities.
The number of sick child care facilities has increased from 577 in 2005 to 2,217 in 2015 [21]. Sick child care services have been carried outnot only as facility-based but also as home-visit-based by visiting nurses [4]. In 2016, the government initiated an offer to subsidize the costs of facility-run transportation between nursery schools and sick child care facilities [22]. Care fees have also started to be subsidized for low-income households (those receiving public assistance and those exempt from residential tax) by the government from 2009 [23,24].
However, as sick child care services are operated by the municipality, not all measures are implemented in all municipalities. For example, A City has not yet offered subsidies for low-income households, and home visit based sick child care services have also not been implemented as of 2017. In 2012, the mean annual income of households with children, those with children under 3 years of age, and those whose youngest child is aged between 3 and 5 years,was 6,732,000, 6,046,000, and 6,450,000 yen, respectively, indicating that the lower the age of the youngest child, the lower the income [25]. The standard monthly child care fee for the first child (aged <3 years)is 44,500 yen, and that for the first and second child aged <3 years is 66,750 yen [10]. When a child develops influenza is required to be absent from nursery school for at least 5 days due to the School Health and Safety Act, a fee of 10,000 yen (2,000yen/ day for 5 days) for sick child care is necessary [26]. However, it may be very difficult for households, in which both parents must work for financial reasons, to pay sick child care fees (prolonged use of such care and simultaneous use of the service by 2 or more siblingsat one time) in addition to nursery school fees. The mean annual income of single-mother households is reported to be 2,434,000 yen, making it more difficult for such mothers to use sick child care services.
In this study, the mothers perceived negative public attitudes towards double-career couples with small children and their use of sick child care services. Before using the service, they themselves also had anxiety over the care because they had no information on the service; thus, the mothers required dissemination of information on sick child care services through several opportunities during their pregnancy in order to ensure its safety and security for their children. Such a request indicates that sick child care service is provided not to help mothers work,but for their children.
This study was conducted in one municipality involving only mothers of double-income nuclear families. To improve and expand the quality of sick child care services based on the needs of users, it is necessary to assess the effects of using the services according to the characteristics of children and parents who use it. It is also necessary to investigate and compare the characteristics of service users and different measures taken by municipalities.
Conclusions
The mothers of double-income nuclear families worked with hope of self-realization,and used sick child care servicesto achieve a balance between career and child-raising. By experiencing positive reactions and early recovery of their children, the mothers developed a sense of security and trust towards high quality medical, nursing, and child nursery care of the service and childcare education provided to them. The results of this study demonstrated that sick child care services were beneficial inpromoting healthy recovery of children and for improving child-care skills of mothersof doubleincome nuclear families. The results also suggest the need to develop measures to respond to the needs of users of sick child care services.
Acknowledgements
We are very grateful to all those who participated in this study.
Funding
This study was funded by a Grant-in-Aid for scientific research expenses of the Japan society for the Promotion of Science (22659412)and (16H05586).
Conflict of Interests
The authors have no conflicting interest in this study
Reference
Imperial Gift Foundation Boshi-Aiiku-Kai. Aiiku research institute (ed) (2017). The declining birthrate and child-raising environment: 2017 Almanac of data on Japanese Children.KTC Chuoh Publishing.72-81.
Tanihara, M., Abe, H., Mori, T., & Okada, K.(2010). Parents’ response to their sick child and the current status of sick-child-care support needs. Kawasaki Med Welf J19:2, 411-418.
Tanaka, T., Ishii, H., & Uchiyama, Y. (2008). Consideration to the status quo of consultation and system of emergency pediatrics by working mothers. J Jpn Soc EmergPediatr7:2,318-324.
Director-General of the Equal Employment, Children and Families Bureau, Ministry of Health, Labour and Welfare (2015). Provision of sick child care.
Japan Sick Childcare Association (2016) Concept of sick child care.View
Kanda, T., & Miyazu, S. (2010). Research on childcare nursing at the child care room for sick children: Based on the viewpoint of child care support. Bull Fac Educ Hirosaki Univ 103:105-109.View
Child Raising Center, Cabinet Office, Government of Japan (2017). The basic data related with children child care support new system.
Ishino, A., Kato, H., Matuda, H., & Bakke, M. (2013). Work-life balance and needs in parents used sick childcare service. J Child Health 72: 305-310.
Fukada, M., Minamimae, K., & Kasagi, T. (2001). Analysis of a method of sick child care and nursing role. J Yonago Med Ass 52: 183-195.
Sato, M. (2006). Research into the needs of day nursery users for children with sickness. J Jpn Red Cross Toyota Coll Nurs 2: 29-34.View
Tanimoto, H., & Tanimoto, K. (2006). Need and problems of the sick child care: Considering the results of a questionnaire survey of the parents. J Child Health 65: 593-599.
Yamamoto, M.(2007). The circular mechanism of maintaining the double burden of working mothers as well as the gender division of labor in Japan: from the experience of full-time working mothers in nuclear families. Kyoto J Sociol15:87-110.
Kobayashi, F. (2010). Finding ways to improve work conditions for family’s well-being and health. Trends Sci 15: 45-49.
Child Raising Center, Cabinet Office, Government of Japan (2017). New child raising support system.
Tanaka, Y. (2011). The perception of services in nurses as to the day care for sick children. J Child Health 70: 365-370.
Fujiwara, Y. (2007). The role of an institution for day care for sick children : Focusing on evaluation of the staff. Jpn Soc Res Early Child Care Educ 45: 183-190.
Kanaizumi, S., Nakashita, T., Yajima, M., & Ohno, A. (2003). Characteristics of nursing and nursing intervention skills required in a nursery room for children recovering from common illnesses. Bull Gumma Paz Gakuen Coll 5: 87-97.
Fukumoto, K., Kawamura, M., Yoshitsugu, M., & Sobue, I. (2016). Benefit of using sick child care facilities to the children and their parents. Health 8:1128-1141.View
Sakai, R., Wada, H., Yoshitsugu, M., & Sobue, I. (2016). Benefits of and issues regarding sick child care for children and their parents. J Comp Nurs Res Care 1: 1-10.
Takahashi, M.(2011). Need and problems of the sick child care. Bull Fac Soc Welf Hanazono Univ 19: 59-76.View
Imperial Gift Foundation Boshi-Aiiku-Kai. Aiiku research institute (ed.) (2017). Care and sound growth of children: 2017 Almanac of data on Japanese Children.KTC Chuoh Publishing 277-300.
Ministry of Health, Labour and Welfare (2016). Summary of the FY 2016 budget for childcare measures.View
Japan Sick Childcare Association (2009). Current status of and issues regarding sick child care.
The director of the Equal Employment, Children and Families Bureau, Ministry of Health, Labour and Welfare (2014). The implementation of programs for the promotion of child care measures.View
Statistics and Information Department, Minister’s Secretariat, Ministry of Health, Labour and Welfare (2014). From comprehensive survey of living conditions, 2013.Graphical review of Japanese household.
Ministry of Education (2013). Infectious diseases that should be prevented at schools.View