
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care Volume 2 (2017), Article ID: JCNRC-114
https://doi.org/10.33790/jcnrc1100114Research Article
Comparison of Primiparas Using Non-painless and Painless Resulting in Physical Symptoms and Apgar Score
Hsiao Lu Lee*, Lee Ching-lan
Department of Nursing. Yuhing Junior College of Health Care & Management, Taiwan.
Corresponding Author Details: Hsiao Lu Lee, Department of Nursing, Yuhing Junior College of Health Care & Management,Taiwan. E-mail: smart@ms.yuhing.edu.tw
Received date: 30th July, 2017
Accepted date: 13th September, 2017
Published date: 29th October, 2017
Citation: Lee, H.L., & Lee, C. (2017). Comparison of primiparas using non-painless and painless resulting in physical symptoms and Apgar score. J Comp Nurs Res Care 2(2): 114.
Copyright: ©2017, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Comparison of primiparas using non-painless and painless resulting in physical symptoms and Apgar score background Using painless methods for childbirth can indeed help mothers relieve pain, blocking sensory nerves that cause labor pain. However, primiparas would not be able to feel uterine contractions at the same time, or difficultly put a lot of strength into labor, sometimes even applying forces incorrectly during the second stage of labor, leading to extended labor time. Another study showed the opposite result – reduction in labor time. Due to less painless labor studies conducted on Asian women, this study aims to explore the impact painless labors have on maternal Asians.
Purpose: The purpose of this study is to investigate the effects on physical symptoms and Apgar score by use of painless and nonpainless labour among Asian primiparas.
Methods: This study is a comparative descriptive research design. The subjects was without chronic diseases, obstetric complications and mental illnesses. She was a primipara, able to communicate with Taiwanese language, and fetus was without any abnormality during pregnancy, in the normal fetal position; labour was a normal spontaneous delivery. Primipara received explanation on the study and informed consent. Analysis were conducted on whether pain has been reduced at childbirth, and two groups of the total production process auxiliary production were compared for differences.
Result: Most of painless primiparas felt numbness, bladder sensitivity being low, and prolonged labor, then obstetricians gave them catheterization and injection pitons on first stage. Painless primiparas assisted instrumental delivery were much more nonpainless primiparas, the relative risk was in range of 1.11-1.38.
Conclusion:Primiparas whether to take painless, medical staffs should be inform them pros and cons of painless, such as if women take painless will reduce labor pain, but more postpartum physical symptoms and reduce Apgar scores.
Keywords: Painless, Apgar Scores , Instrument-assisted Delivery, Primiparas, Physical Symptoms.
Introduction
Painless childbirth methods are often preferred by mothers. Pharmacological methods are recognized as the most effective to relieve the pain of childbirth [1]. The WHO promotes natural birth and has established a practical guide. WHO supports no-pharmacological methods of pain relief [2]. Painless childbirth has both pros and cons in terms of efficiency and impact on the childbirth process for a woman and her newborn. The use of epidural anesthesia increased the risk of instrumental delivery(relative risk: 1.38) [3]. Using epidural anesthesia and recorded that need for forceps assisted delivery was increased posing a health threat to the mother and child [4]. The risk ratio of cesarean section (CS) between the use and non-use of epidural anesthesia was 2.9 [5]. Nulliparous women took epidural use was associated with a 2.4 relative risk (95%CI: 1.5, 3.7) for cesarean delivery [6]. When the second stage prolonged then senior obstetrician make decision to use instrumental delivery to avoid CS, instrumental delivery include forceps and vacuum suction [7]. The WHO recommends that the induction rate should not exceed 10% [8]. Whether painless childbirth methods influence physiology of the mother and newborn.101 primiparas had a longer second stage of labor time, then a lower of Apgar score in 1 minute and higher incidence of asphyxia. Moreover, the incidence of cesarean section and increased postpartum hemorrhaging [9]. Women used epidurals, mothers’ experienced low blood pressure and had an increased risk ratio of fetal distress being 1.42. urinary retention with a risk ratio of 17.05 [3]. If a mother used narcotic analgesics, that passes easily through the placenta, making more fetal and neonatal distress, and existed an increased risk ratio for caesarean section, fetal bradycardia [10]. Above the empirical studies of painless labor were from Europe or US, Therefore, this study would explore Taiwanese women taking painless labor, they were from the East, what did they and their newborn be influence on their physiology by painless labor
Methods
This study followed a comparative descriptive research design. Primiparas were randomization to be the study’s participants, they were informed the purpose and process of the study. Painless primiparas were injected analgesia macaine 3cc and xylocaine 3cc into lumbar epidural to reduce labor pain. Non-Painless primiparas were not injected or took analgesia. Participants without chronic diseases, obstetric complications and mental illnesses were chosen for this study Participants were primiparas, and able to communicate in Taiwanese and Mandarin Chinese. The fetuses of the participants did not have any abnormalities during pregnancy, single, and were in the normal fetal position. Labor was a normal spontaneous delivery.
Questionnaire about demographics included primipara’s age, education, marital status, living status, religion, occupation, place of birth, frequency of exercise (per week), average length of exercise each time, height, weight, gestational period(week) and number of abortion. The use of drugs and instrumental delivery data, the use of drugs were recorded from cases’ chart Piton-s (amp), Buscopan (amp), PGE2; Instrument-assisted delivery data included women requiring an episiotomy, Episiotomy laceration, help from staff such as a nurse using a hand to dilate the cervix and perineum (stretch cervix), and tools such as a vacuum suction and nurse’s hand pressure uterine fundus of abdomen. Questionnaire about the proposed study examined the physical condition of mother and newborn during intrapartum. In the case of mothers’ conditions such as on Foley, move leg difficulties, urinary difficulties, urinary retention, motor block, perceived difficulties, itchy skin, leg pain, nausea, vomit, blurred vision, back pain, dyskinesia, BP drop, and dizziness were recorded. For the neonatal conditions included the neonatal Apgar score (1 and 5 minutes) and caesarean section for fetal distress.
Data were coded by SPSS 20.0. Data analysis and comparing the effects of painless and non-painless childbirth methods, and the relationship with instrument-assistance delivery and birth outcome. In this study, descriptive statistical including the mean, standard deviation, frequency distribution, percentage were computed for to pres- ent information. The McNemar, fisher’s exact test, relative risk to comparison non-painless and painless groups on instrument assistance.
This study was approved by the Yuhing Junior College’s Academic Research Institutional Review Board (study no.100-S04). Researchers obtained the target hospital’s informed consent from medical staff including participating obstetricians, director of nursing and other nursing staff before data was collected. Primiparas were informed consent was given after the explanation of study. All participants signed a consent form. The participants took about 20 minutes to fill out the questionnaire. Participants who completed the questionnaire and interview received a small beautiful gift for their participation.
Result
A total of 77 participants were participated in this study. Those mothers were selected who meet the inclusion criteria, from a local maternity hospital in Kaohsiung, Taiwan. The data was collected during a period between January and December, 2013. Participants were divided into two groups. One group (42 cases) used painless labor methods, and the other group (35 cases) did not use any drugs to reduce labor pain. 59 (76.7%) women were under the age of 35, and18 (23.3%) women were older than 35 years old. The average age of the participants was 30.29±3.95 (M±SD) years old (ranges from 21 to 40 years old). Other demographic data between painless and nonpainless women was no significantly difference in age, height, etc. Only the number of abortions’, and length of prenatal exercise were significantly different in the two groups (p <0.05). Painless women were more exercise time than non-painless ones, and non-painless labor were more times of abortion then non-painless ones (Table 1).
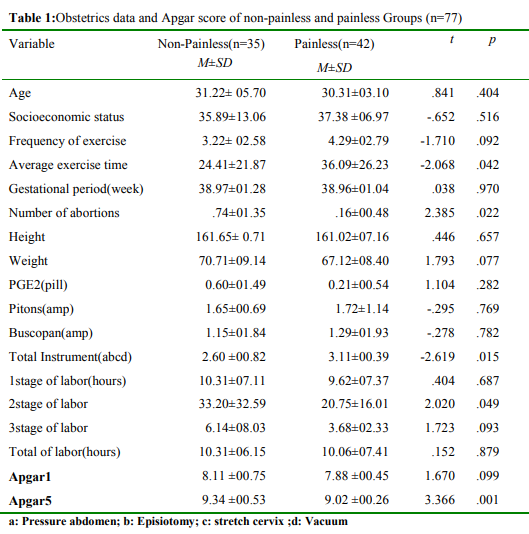
Table 1: Obstetrics data and Apgar score of non-painless and painless Groups (n=77)
a: Pressure abdomen; b: Episiotomy; c: stretch cervix; d: Vacuum;
Painless labor methods needed more instrumental assistance, such hand pressure from staff on the primiparas’ abdomen (p= 0.027), and fingers of staff to stretch the cervix(p=0.041), but there is no significant difference existed in the degree of episiotomy laceration (p=0.183) and use of drugs such as Pitocin, bascopan, PGE2 between the two groups. It is interesting to note that if the 4 instrumental assistance variables such as hand pressure uterine fundus of abdomen , episiotomy, stretching the cervix with fingers and vacuum are total as one variable, then there existed a existed a significant difference in instrument-assisted delivery between the two groups (t = -2.619, p=0.015), showing that painless labor required more instrumental assistance(Table 2). Painless primiparas took the risk of vacuum instrumental delivery was less than non-painless primiparas, relative risk (RR) 0.72, but Painless primiparas took the risk of stretching the cervix with fingers, nurse’s hand pressure uterine fundus of abdomen, episiotomy instrumental delivery were much more than nonpainless primiparas, relative risk (RR)1.33, 1.38, 2.22 (Table2).

Table 2: Comparison non-painless and painless groups on instrument assistance
aMcNemar; bfisher’s exact test; crelative risk(Painless use instrument /Non-painless use instrument) dBinomial test
Painless primiparas’ postpartum physical symptoms up to five were urination difficulties, dizziness, vomit, urinary retention, and motor block. Non-pain less primiparas had postpartum physical symptoms up to five were Back pain, dizziness, Leg pain, urination difficulties, urinary retention (Table3). Painless primiparas got more postpartum physical symptoms than non-pain less primiparas, the results shown that there were significant difference existed on foley, urinary difficulties, urinary retention, motor block, perceived difficulties, nausea, vomit, blurred vision,dyskinesia, BP drop, itchy skin, and caesarean section. A few painless primiparas had insomnia(n=1), tachycardia (n=1),shiver (n=1) and dyspnea(n=1) (Table3).
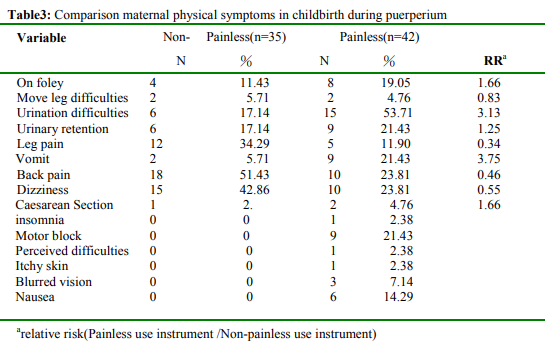
Table 3: Comparison maternal physical symptoms in childbirth during puerperium
arelative risk(Painless use instrument /Non-painless use instrument)
Whether or not to use painless childbirth was no significant difference Apgar score in 1 minute, but painless primiparas newborn Apgar scores was significantly lower than non-painless primiparas newborn in fifth minute (Table1). Two painless primiparas had fetal distress, so they took cesarean section, but one non-painless primiparas took cesarean section for fetal distress. Apgar scores in first and fifth minute showed significant negative correlation to drug of painless, xylocaine(r=-.284; r=-.347, p<.05), macaine(r=-.285; r=-.338, p<.05), buscopan (r=-.275, p<.05)and inject painless times(r=-.252; r=-.359, p<.05), so if painless primiparas got more drug of painless will affect Apgar scores.
Discussion
This study showed painless primiparas were significant more instrumental delivery than non-painless ones, such nurse’s hands compress primiparas’ abdomen, nurse’s finger explored the cervix and vagina exhibition open- ing. Painless primiparas assisted instrumental delivery were much more non-painless primiparas, the relative risk was in range of 1.11-1.38, which is similar to Anim- Somuah [3] explored instrumental delivery was much more in the women randomized to epidural analgesia, relative risk (RR) 1.38. In this study, All women posture of labor were supine, so they had difficulties to push by themselves, and most painless primiparas could not feel uterine contraction, thus, nurse’s hand touched painless primiparas’ abdomen felt uterine contraction, then they told uterine contraction information to painless primiparas, they immediately had power to labor.
Compare with -using instrumentals for delivery, Taiwan obstetrician use more instrumentals for painless delivery, not only forceps and vacuum, but also obstetric nurse’s elbow press fundal, nurse’s finger explored the cervix and vagina exhibition opening and episiotomy. In this study extended the scope of instrumentals delivery. Most of obstetrician used these labor instruments from their skill and culture of obstetric department, such as the rate of episiotomy(90%) and nurse’s elbow press fundal(82.7 %) were so high rate, and exceed WHO recommendation[8]. These procedures have shown that unnecessary or harmful interventions during labor and birth outcome [11]. Midwives are potential development and will gradually take over normal delivery, the policy is support by government in Taiwan. Midwives encourage women taking mild delivery, giving empower to women and help primiparas taking comfortable posture, reducing episiotomy, no press fundal and support primiparas to labor by their power in Taiwan.
Painless primiparas were more severe physical symptoms then non-painless primiparas in during puerperium. In this study, painless primipara had nausea, vomit, hypotension, motor blocked, itching, urine retention and back pain symptoms were similar to the study [3]. 9 painless primiparas had vomit , but 2 non-painless primiparas had vomit, so painless primiparas for vomiting relative risk was 3.72. After activities such as vomiting lifting, sudden rise in intrathoracic pressure leads to increased intraocular venousn [12]. In this study 3 painless primiparas had blurred vision, but no non-painless primiparas had blurred vision, this result can be explore the relation blurred vision with vomting. 9 painless primiparas had motor block, but no non-painless primiparas had motor block , primiparas had less feeling, perception dull of lower body, leg cannot move, the result was higher risk ratio than Anim-Somuah’s study[3]. The side effect of macaine drug is hypotension, myocardial depression, bradycardia, nausea, vertigo and numbness of the tongue, light-headedness, dizziness, blurred vision and tremor followed by drowsiness, convulsions, unconsciousness and possibly respiratory arrest, weakness and paralysis of the lower extremities, hypotension, high or total spinal block, urinary retention, headache, backache, septic meningitis, meningismus, arachnoiditis, slowing of labor, increased incidence of forceps delivery, shivering [13]. In this study, one painless primiparas had shiver was similar to Anim-Somuah’s study [3]. Painless primiparas had symptoms could relate side effect of macaine drug. But, painless primiparas being less back pain, headache were similar to Obido’s literal review findings [3]. Nonpainless primiparas got much more other symptoms (leg pain, back pain, dizziness) than painless primiparas. The reason is not clear, why make difference symptoms between painless primiparas non-painless primiparas? It is worth to study further in the future.
Painless primiparas’ newborn Apgar score were less than nonpainless primiparas’ one at 5 minutes, this out- come was same Anim-Somuah’s study [3]. The drug of painless will reduce Apgar scores, so obstetrician and obstetric nurses should inform this risk of painless information to primiparas and families.
Conclusion
Women took painless, most of painless primiparas felt numbness, bladder sensitivity being low, and prolonged labor, then obstetricians gave them catheterization and injection pitons on first stage. They moved to second stage, they cannot feel the uterine contractions, no power to labor, then obstetricians used more instrumentals and made every primiparas for safety, but made newborn Apgar score were affected. The decision that women whether to take painless, medical staffs should be inform them pros and cons of painless, such as if women take painless will reduce labor pain, but more postpartum physical symptoms and reduce Apgar scores. Nurses should give their chance to consult anesthesiologists. Woman should be inform other methods of non-pharmacological pain relief, such as focusing, music therapy, water therapy [14], message [15], acupressure, acupuncture, aromatherapy, heat and cold therapy, birth ball [16]. Clinicians and nurse assist husbands of primiparas to help their wife pain relief, and support them until they maybe be discharge. This study help nurses understand that painless primiparas will have postpartum physical symptoms, nurses should pay attention these symptoms, promote painless primiparas comfort during postpartum period.
Reference
Hidaka, R., & Callister, L.C. (2012). Giving birth with epidural analgesia: The experience of first-time mothers. The J of perinatal education 21: 24-35.View
World Health Organization (2015). Recommendations for Augmentation of labour.View
Anim-Somuah, M., Smyth, R., & Jones, L. (2011). Epidural versus non-epidural or no analgesia in labour. The Cochrane database of systematic reviews 12: 1-127.View
Obido, L. (2007). Does epidural analgesia affect the second stage of labor? British J of Midwif 15: 429-435.
Sidelnick, C., Karmon, A., Levy, A., Greemberg, L., Shapira, Y., & Sheiner, E. (2009). Intra-partum epidural analgesia in grand multiparous women. J of Maternal-Fetal and Neonatal Med 22: 348-352.View
Nguyen, U.D.T., Rothman, K.J., Demissie, S., Jackson, D.J., Lang, J.M., & Ecker, J.L.(2010). Epidural analgesia and risks of cesarean and operative vaginal deliveries in primiparas and multiparous women. Maternal and Child Health J 14:705-712.View
Umbeli, T., Salah, I., & Kunna, A. (2014). Maternal and neonatal complications associated with caesarean section in the second stage of labor at Omdurman maternity hospital during 2012- 2013, Merit Research. J of Med and medical sciences 2: 225- 228.View
Reham, K., Caroline, H., & Lesley, B.A. (2009). comparison of labour and birth outcomes in Jordan with WHO guidelines: a descriptive study using a new birthrecord. Midwif 25: 11-18.
Li, W.H., Zhang, H.Y., Ling, Y., & Jin, S. (2011). Effect of prolonged second stage of labor on maternal and neonatal outcomes. Asian Pacific J of Tropical Med 4: 409-411.View
Lieberman, E., O’Donoghue, C. (2002). Unintended effects of epidural analgesia during labor: a systematic review. American J of obs and gyn 186: 31-68.View
Creedy, D., Shochet, I., & Horsfall, J. (2000). Childbirth and the development of acute trauma symptoms:incidence and contributingfactors. Birth 27: 104–111.View
Zhang, G.S., & Mathura, J.r. (2005). Images in clinical medicine. Painless loss of vision after vomiting. The New England J of Med 352: 16.View
RxList (2015). Marcaine-side effects.View
Lee, S.L., Liu, C.Y, Lu, Y.Y., & Gau, M.L. (2013). Efficacy of warm showers on labor pain and birth experiences during the first labor stage. J of Obs Gyn Neonat Nurs 42: 19-28.View
Chang, M.Y., Chen, C.H., Huang, K.F.(2006). A comparison of massage effects on labor pain using the McGill Pain Questionnaire. J of Nurs Research 14: 190-197.View
Taavoni, S., Abdolahian, S., Haghani, H., & Neysani, L. (2011). Effect of birth ball usage on pain in the active phase of labor: A randomized controlled trial. J of Midwif Women’s Health 56: 137-140.View