
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care Volume 2 (2017), Article ID: JCNRC-115
https://doi.org/10.33790/jcnrc1100115Research Article
Comparative Study of High Frequency Chest Wall Oscillation and Traditional Chest Physical Therapy in Intensive Care Unit Patients
Yu-Ping Lin1*, Heng-Hsin Tung2, Tsae-Jyy Wang2
1Department of Nursing, Oriental Institute of Technology, Taipei, Taiwan.
2School of Nursing, National Taipei University of Nursing and Health Sciences,Taiwan.
Corresponding Author Details: Yu-Ping Lin, Assistant Professor, Department of Nursing, Oriental Institute of Technology, Taipei, Taiwan. E-mail: fk014@mail.oit.edu.tw
Received date: 07th August, 2017
Accepted date: 20th September, 2017
Published date: 06th November, 2017
Citation: Lin, Y.P., Tung, H.H., & Wang, T.J. (2017). Comparative Study of High Frequency Chest Wall Oscillation and Traditional Chest Physical Therapy in Intensive Care Unit Patients. J Comp Nurs Res Care 2(2): 115.
Copyright: ©2017, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Aims and objective: The aim of this study was to compare the efficacious treatment in intensive care unit patients: high frequency chest wall oscillation (HFCWO¸VEST) versus chest physiotherapy (CPT).
Background: Patients with lung disease often have respiratory infections and hospitalization caused by sputum retention. Intensive care unit patients usually have intubated and ventilator and this make it difficult to clean the airway.
Methods: A comparison study with random sampling was carried out 559 patients in the intensive care unit were recruited in the study. Patients either received HFCWO therapy using the vest system (n=208) or received CPT (n=351). The primary outcomes were length of stay in intensive care unit and the duration of mechanical ventilation, comfortable with therapy and lung condition were compared between the two groups
Result: The patients treated by the high frequency chest wall oscillation, their duration of mechanical ventilation (p=0.014), chest X-ray (p<0.0001) and their comfortability (p<0.0001) were significantly better than the chest physiotherapy patients. The sputum volume did not differ significantly between the two groups (p=0.085).
Conclusion:HFCWO was associated with better comfort, produced an improvement in lung condition, and reduced the number of days to use the ventilator on patients who are in intensive care units, compared to manual percussion of CPT. HFCWO can be performed in acutely ill patients who may be unable to use handheld devices effectively. Those patients need airway clearance in intensive care units; this treatment could be included among the options in chest physiotherapy.
Keywords: High Frequency Chest Wall Oscillation, Chest Physiotherapy, Intensive Care Unit
Introduction
Patients with acute or chronic lung disease often have respiratory infections and hospitalization caused by sputum retention. The early clearance of mucus and secretions from the airways is important in the treatment of pulmonary diseases. Patients in the intensive care unit (ICU) are usually intubated endotracheal tub and monitored through mechanical ventilator. This makes it difficult to clean the airway passages of these patients [1-3]. Chest physiotherapy has several secretion management techniques and equipment which could mobilize the secretions, make the coughing effective, and improve cleaning of the airway. These include modified postural drainage, position, and percussion [4-6], positive expiratory pressure devices [4-6], breathing technique [4,5], intrapulmonary percussive ventilation [7], and high-frequency chest wall oscillation (HFCWO) [8,9]. The conventional chest therapy (CPT) is consisting of postural drainage, position, and manual percussion technique, and has been applied for many years and used empirically. Likewise it has been reported that CPT is time-consuming, labor intensive, and may not be available as frequently as desired during hospitalization [10,11].
HFCWO is performed with a mechanical device (Hayek Oscillator). It produces high velocity, low amplitude oscillatory airflows when applied through a pneumatic vest worn over the thorax. HFCWO delivers an intermittent airflow into the vest which compresses and releases the chest wall at different frequencies. An oscillation in airflow within the airways is achieved. By this mechanism, an oscillation of airflow is produced within the airway; mucus is dislodged from the bronchial walls and mobilized to larger airways, where it could more easily be removed by coughing or suctioning [12,13]. It has an important advantage for making standard mechanical therapy without dependent nurses or therapists. Recently, HFCWO therapy has been used in many diseases, such as cystic fibrosis [8,12,14-17], chronic obstructive pulmonary disease (COPD) [10,18,19] thoracic trauma [9,20], and bronchial asthma [18,21,22] Improving lung function, safety, tolerability after using of the HFCWO has been reported in the treatment of these diseases. To our knowledge, few studies have examined the use of HFCWO in the management of acute lung condition among patients in the ICU. Hence, how to safely and effectively removal of sputum, and prevent or treat respiratory tract infections, has become a clinically important issue. The main purpose of this study was to compare the efficacy of HFCWO and CPT in ICU patients, particular on the length of ICU stay and duration of mechanical ventilation, comfortable and lung condition.
Methods
Design
A comparison study with random sampling was carried out. The specific aims of this study were to compare the effectiveness of HFCWO and conventional CPT in patients in the ICU.
Sample and Setting
A sample of 559 adults who were admitted to the ICU via the emergency room inTaiwan. Patients who met the following eligibility criteria were recruited: (1) endotracheal intubation with mechanical ventilation, (2) blunt or penetrating chest wall injury, (3) pneumonia, and (4) 18 years of age or older. Potential participants were excluded if they (1) Glasgow Coma Scale score were below than 7, or (2) unstable condition.
Data collection
The study was approved by the research ethics committees of the hospital where the participants were recruited. Patients or legalized families agreed to participate in the study and were assigned following a computed randomized list to high frequency chest wall oscillation (HFCWO) or to chest physiotherapy (CPT).
Measurements
The study questionnaires include questions on demographics (age, gender, and ICU attributes), the length of ICU stays, duration of mechanical ventilation, improvement of lung condition, sputum volume, and patients’ comfortable. The improvement of pneumonia and lung collapse was recorded by listening to both lungs and chest X-ray films by two senior physicians. Patient comfort with treatment was measured using a visual analog scale, increasing score reflects greater discomfort.
HFCWO and CPT procedures
CPT consisting of chest percussion and postural drainage was performed by ICU nurses. The HFCWO was set to an optimum oscillating frequency of 10-15 Hz, with a slight pressure on the chest, performing by respiratory therapists (RTs). Both treatments were given every 4 h per day and last 30 minutes per session. Patients’ condition was monitored during CPT or HFCWO procedures. Nurses and RTs followed the standard of research program.
Statistical analysis
SPSS for Windows 21.0 (SPSS Inc., Chicago, IL, USA) was used for all statistical tests. Continuous variables were expressed as mean ± standard deviation and categorical variables, expressed as frequency or percentage, were compared using the χ2 test. Values of p ≤ 0.05 were considered statistically significant.
Results
Characteristics of the samples
The mean age of the HFCWO and CPT groups were 62.36 (SD 16.65) and 62.16 (SD 15.52) years, respectively. One hundred and thirty-five (64.9%) and 230 (65.5%) were male in the HFCWO and CPT groups. None of the baseline patient characteristics differed significantly between the two groups. The patients’ characteristics are presented in Table 1.
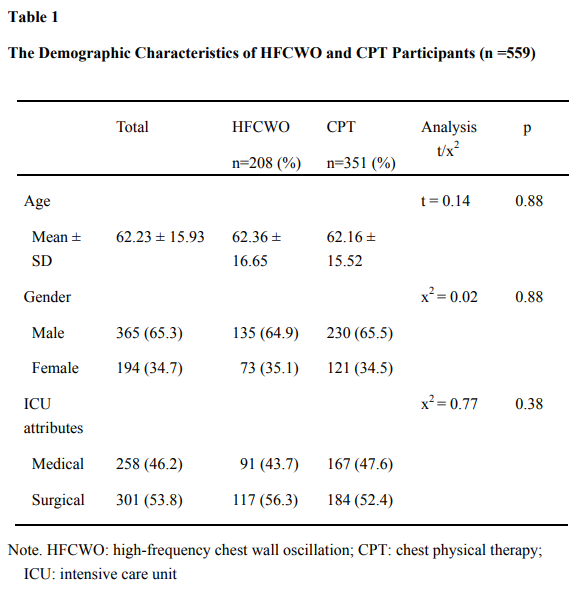
Table 1: The Demographic Characteristics of HFCWO and CPT Participants (n =559)
Note. HFCWO: high-frequency chest wall oscillation; CPT: chest physical therapy; ICU: intensive care unit.
ICU length of stay and ventilation duration
The ICU length of stay of the HFCWO and CPT groups were 12.37 (SD 11.06) and 14.39 (SD 13.83) days, respectively. It showed nearly significant difference between the two groups (t= -1.90, p=0.059). The duration of mechanical ventilation was 10.68 (SD 10.60) days in the HFCWO group and 13.28 (SD 14.22) days in the CPT group. This measurement showed differs significantly between the two groups (Table 2).

Table 2: Comparison of Parameter about the Length of Stay and Duration of Mechanical Ventilation (n = 559)
Note. HFCWO: high-frequency chest wall oscillation; CPT: chest physical therapy; ICU: intensive care unit; * p-value < 0.05
Differences in comfort, sputum volume, pneumonia and lung collapse between HFCWO and CPT participants
Table 3 shows a comparison of the comfort, sputum volume, and pneumonia and lung collapse between two groups. There was a significant difference in the comfort (p <0.0001), pneumonia and lung collapse (p <0.0001). However, the amount of sputum did not differ significantly between the two groups (p=0.085).
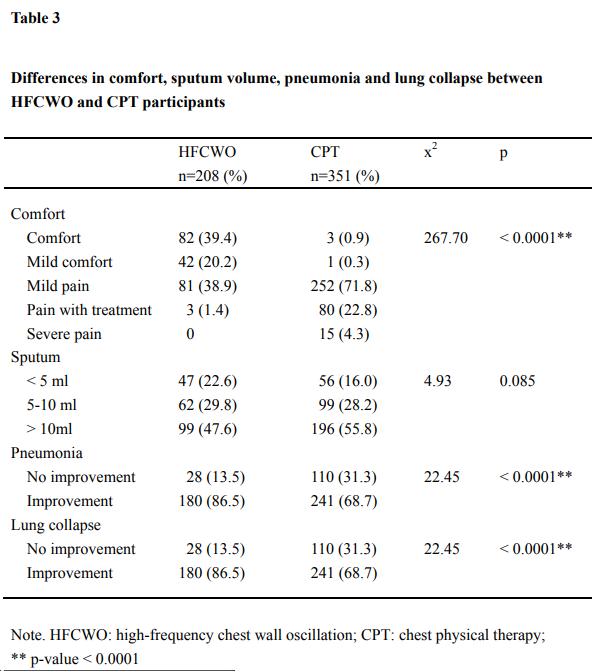
Table 3: Differences in comfort, sputum volume, pneumonia and lung collapse between HFCWO and CPT participants
Note. HFCWO: high-frequency chest wall oscillation; CPT: chest physical therapy; ** p-value < 0.0001
Discussion
This study examined the efficacy of HFCWO using the Vest system compared with traditional CPT for patients with medical or surgical conditions who admitted to ICUs. It was found that patients in the HFCWO therapy was shorter length of ICU stay and duration of mechanical ventilation and better comfortable with treatment and lung conditions than those in CPT group. The results of the present study provide empirical support for the effectiveness of HFCWO in the management of patients’ conditions in ICUs.
In our study, 82 (39.4%) patients felt comfortable with HFCWO, whereas only 3 patients in the CPT were comfortable and 71.8% of them felt mild pain with therapy. These findings were consistent with previous researches [9,23-25], It has been reported that traditional CPT for airway clearance is labor intensive and discomfort for patients [11]. Researchers have found that HFCWO system was safe and comfort for patients with lung and chest wall injuries. Patients experienced no pain and no increased bleeding or need for further surgical treatment [9,18,20,23-25]. Moreover, the safety of the HFCWO Vest system was evaluated by observing patients’ vital signs, and during the study period, sudden changes in vital signs were not observed and without adverse events.
We did not find difference in sputum volume between two groups. There are possible explanations. First, this study had medical and surgical patients who may have other comorbidities to detect improvements in this outcome. Second, we may not have measured markers of airway clearance with adequate precision. Sputum collection was made by suction from the endotracheal tube with sputum box. It is possible the nurses may have suction sputum direct into suction bottle. The design of future studies of airway clearance need to include procedures to assure collection of sputum and to measure wet or dry sputum weight.
The present study shows that there were effect of HFCWO in the length of ICU stay, duration of mechanical ventilation, and lung condition. These results were consistent with previous studies [10,26,27]. It may contribute to expectoration and thus improve lung collapse among ventilated patients in ICUs. A study of 22 hospitalized patients with hypersecretive COPD with recurrent exacerbations found that the treatment with HFCWO led to improvement in lung function, quality of life, and reduction of symptoms, but not in sputum production [10]. One study was no difference in the length of hospital and ICU stay, and duration of mechanical ventilation between two the therapy groups [9]. Their patients in the HFCWO group were higher pulmonary contusion score than those in CPT group. Thus, ventilation was used more frequently in the HFCWO group than in the CPT group (100% vs. 78%).
A new study of systematic review by Morrision et al. [8] have demonstrated that there were no clear evidence that oscillation was more or less therapy than other techniques of physiotherapy for people with cystic fibrosis. However, compared with the HFCWO Vest system, traditional CPT (manual percussion or postural drainage) requires much time and assistance from trained health care personnel. HFCWO can be performed in acutely ill patients who may be unable to use handheld devices effectively, such as intubated patients, and may therefore offer a practical advantage compared to chest physiotherapy. Moreover, HFCWO Vest chest therapy is a safe, comfortable and effective alternative pulmonary clearance method and can be used on patients who are on ventilators in ICUs.
Limitations
This study had several limitations. First, the participants were recruited from a teaching hospital in the northern Taiwan, so there are limitations in the study of inference, suggesting that future studies can expand the study areas to increase the inference. The participants of this study set the inclusion criteria (with medical or surgical) may be too complex, some of patients who were with other comorbidities that may influence the results of measurements. Future study could be simplified the standard of patients’ condition.
Conclusions
HFCWO was associated with better comfort, compared to manual percussion of CPT; despite the use of HFCWO equipment was high cost. This study shows that HFCWO produced an improvement in lung condition, patients’ comfort, and reduced the number of days to use the ventilator on patients who are in ICUs. Long-term studies are needed to examine the effectiveness of different airways clearance devices or their cost-effectiveness. More clinical researches are needed in order to use this knowledge to ICU practices.
Conflict of Interest
Authors declares no conflict of interest
References
Kuyrukluyildiz, U., Binici, O., Kupeli, I., Erturk, N., & Gulhan, B., et al. (2016). What is the best pulmonary physiotherapy method in ICU? Canadian Resp J.View
Esguerra-Gonzalez, A., Ilagan-Honorio, M., & Fraschilla, S. (2013). Pain after lung transplant: high-frequency chest wall oscillation vs chest physiotherapy. Am J Critical Care 22: 115-124.View
Braverman, J. (2007). A practical intervention for secretion retention in the ICU. Respiratory Ther 2: 26-29.
Mutalithas, K., Watkin, G., Willing, B., Wardlaw, A., & Pavord, I.D., et al. (2008). Improvement in health status following bronchopulmonary hygiene physical therapy in patients with bronchiectasis. Respirat Med 102: 1140–1144.View
Patterson, J.E., Bradley, J.M., Elborn, J.S. (2004). Airways clearance in bronchiectasis a randomized crossover trial of active cycle of breathing techniques (incorporating Postural drainage and vibration) versus test of incremental respiratory endurance. Chron Respirat Disease 1: 127–130.View
Oermann, C.M., Swank, P.R., & Sockrider, M.M. (2000). Validation of an instrument measuring patient satisfaction with chest physiotherapy techniques in cystic fibrosis. Chest 118: 92-97.View
Paneroni, M., Clini, E., Simonelli, C., Bianchi, L., & Degli Antoni, F., et al. (2011). Safety and efficacy of short-term intrapulmonary percussive ventilation in patients with bronchiectasis. Respiratory Care 56: 984-988.View
Morrison, L., & Innes, S. (2017). Oscillating devices for airway clearance in people with cystic fibrosis. Cochrane Database Systematic Review.View
Lee, D.S., Park, S.W., Yeom, S.R., Han, S.K., & Lee, S.H. et al. (2011). Highfrequency chest wall oscillation therapy: Clinical effectiveness in the patients with pulmonary contusion. Korean J Critical Care Med 26: 25-260.View
Chakravorty, I., Chahal, K., & Austin, G. (2011). A pilot study of the impact of high-frequency chest wall oscillation in chronic obstructive pulmonary disease patients with mucus hypersecretion. Int J Chronic Obstruct Pulmon Disease 6: 693- 699.View
Warwick, W.J., Wielinski, C.L., & Hansen, L.G. (2004). Comparison of expectorated sputum after manual chest physical therapy and high-frequency chest compression. Biomed Instrument Tech 38: 470-475.View
Wilson, L.M., Agnew, J., Morrison, L., Akinyede, O., & Robinson, K. A. (2014). Airway clearance techniques for cystic fibrosis: an overview of Cochrane systematic reviews (Protocol). Cochrane Database Systematic Reviews 8: 1-6.View
Hristara – Papadopoulou, A., Tsanakas, J., Diomou, G., & Papadopoulou, O. (2008). Current devices of respiratory physiotherapy. Hippokratia 12: 211-220.View
Fainardi, V., Longo, F., Faverzani, S., Tripodi, M.C., & Chetta, et al. (2011). Short-term effects of high- Frequency chest compression and positive expiratory pressure in patients with cystic fibrosis. J Clin Med Res 3: 279-284.View
Bradley, J.M. (2010). High frequency chest wall oscillation in cystic fibrosis. Thorax 65: 189-190.View
Kempainen, R.R., Milla, C., Dunitz, J., Savik, K., & Hazelwood, A., et al. (2010). Comparison of settings used for high-frequency chest wall compression in cystic fibrosis. Respirat Care 55: 695-701.View
Morrison, L., & Agnew, J. (2009). Oscillating devices for airway clearance in people with cystic fibrosis. Cochrane Library.View
Mahajan, A.K., Diette, G.B., Hatipoğlu, U., Bilderback, A., Ridge, A. et al. (2011). High frequency chest wall oscillation for asthma and chronic obstructive pulmonary disease exacerbations: a randomized sham-controlled clinical trial. Respiratory Res 12: 120.View
Braveman, J., & Nozzarella, M. (2007). High-frequency chest compression advanced therapy for obstructive lung disease. Respirat Ther 2: 48–51.
Anderson, C.A., Palmer, C.A., Ney, A.L., Becker, B., & Schaffel, S.D., et al. (2008). Evaluation of the safety of high-frequency chest wall oscillation (HFCWO) therapy in blunt thoracic trauma patients. J Trauma Manag Outcomes 2: 8.View
Antonello, N., Federica, C., Norma, L., Sergio, L., & Maura, F., et al. (2013). Effectiveness of treatment with high-frequency chest wall oscillation in patients with bronchiectasis. BioMed Central Pulmonary Med 13: 13-21.View
Nicolini, A., Cardini, F., Landucci, N., Lanata, S., Ferrari-Bravo, M., et al. (2013). Effectiveness of treatment with high-frequency chest wall oscillation in patients with bronchiectasis. BMC Pulmonary Med 13: 21.View
Brierley, S., Adams, C., Suelter, J., Gooch, T., & Becker, B. (2003). Safety and tolerance of high frequency chest wall oscillation in hospitalized critical care patients. Respiratory Care 48: 1112.
Chao, L. M. (2014). The effectiveness of patient sputum clearance with high frequency chest wall oscillation therapy. Central Taiwan University of Science and Technology.
Clinkscale, D., Spihlman, K., Watts, P., Rosenbluth, D., Kollef, M.H. (2012). A randomized trial of conventional chestphysical therapy versus high frequency chest wall compressions in intubated and non-intubated adults. Respiratory Care, 57(2): 221-228.View
Huang, W-C., Wu, P-C., Chen, C-J., Cheng, Y-H., & Shih, S-J., et al. (2016). High-frequency chest wall oscillation in prolonged mechanical ventilation patients: a randomized controlled trial. Clinical Respirat J 10: 272-281.View
Chen, Y.C., Wu, L.F., Mu, P.F., Lin, L.H., & Chou, S.S., et al. (2009). Using chest vibration nursing intervention to improve expectoration of airway secretions and prevent lung collapse in ventilated ICU patients: A randomized controlled trial. J Chinese Medical Asso 72: 316-322.View