
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care Volume 2 (2017), Article ID: JCNRC-117
https://doi.org/10.33790/jcnrc1100117Review Article
Suicide: A look Through
Abin Varghese*, Sam Jose, Gigini George
Nursing,Tutor, Bhopal Nursing College, Bhopal memorial Hospital And Research Centre, Department of Health Research, Ministry of Health And Family Welfare, Government of India.
Corresponding Author Details: Abin Varghese, Nursing,Tutor, Bhopal Nursing College, Bhopal memorial Hospital And Research Centre, Department of Health Research, Ministry of Health And Family Welfare, Government of India. E-mail: abinvarghese143@gmail.com
Received date: 30th July, 2017
Accepted date: 13th September, 2017
Published date: 29th November, 2017
Citation: Varghese, A., Jose, S., & George, G. (2017). Suicide: A look Through. J Comp Nurs Res Care 2(2): 117.
Copyright: ©2017, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Suicide is one of the leading causes of death worldwide. A thorough review on various factors leading to suicide are vital parameters helping the government and policy makers to tailor readymade interventions. The multifactorial risks associated with suicide is hindering the public health delivery system globally since it is not possible to isolate and deliver a few interventions in preventing suicide but a comprehension of all the risk factors of suicide are essential. The purpose of study was to identify the multiple risk factors of suicide. Furhermore the collaboration of governmental agencies especially the public health department along with multiple agencies is crucial to attain a fruitful result in preventing suicide.
Key words: Suicide, self injurious behaviors, public health, risk factors
Introduction
Suicide is among the global concern to which the world public health system is paying its full attention as it is increasing at an alarming rate. The statistics provided by World health Organization (WHO) with respect to suicide will make each individual to think about the venomous disability that has interwoven human kind. Indeed a figure of more than 800000 people dies due to suicide every year-one person every 40 seconds. Eventhough suicide occurs at any point of life, the age group of 15-29 years witnessed it as the second leading cause of death worldwide [1]. Suicide is a type of deliberate self-harm and is an intentional human act of killing one self. However many of those people who attempts suicide does not kill themselves. Suicide is a mental health problem that requires urgent intervention for to save the life. The exact cause of suicide is unknown but multiple factors such as illness, family problems, psychological, sociocultural, neurological, cognitive problems and others may bring suicidal thoughts which eventually leads to suicide [3,4]. Moreover the multifactorial causation for suicide is being highlighted everywhere and interventions are being tailored depending upon the different factors involved. The association of suicide with psychiatric disorders such as depression, schizophrenia, alcoholism, drug abuse, panic disorder, personality disorder and OCD are robust. More than 90% of suicide victims have psychiatric illnesses at the time of their deaths. It is important to consider mental illness in general and not just depression, as an important risk factor for suicide [5-7]. The core sympton symptomatology of hopelessness, helplessness and worthlessness seen in depression are invariably seen in almost all individuals who commit sui- cide. The common methods adopted for suicide includes hanging, drowning, ingestion of poisonous substances and self immolation. Every suicide is disastrous to the entire family, community, nation and to the entire human kind so the phenomenon of suicide should be conceptualized in terms of risk factors so that the public health delivery can incorporate the strategies for prevention of suicide.
Search strategy
The databases of PUBMED,INDMED,MEDLINE,EMBASE,P ROQUEST and Ovid platform was searched using the key words Suicide, Attempted Suicide, Risk Factors AND suicide by three independent reviewers. The inclusion criteria included studies done from 2000 to 2017, published in English with full text availability, significant suicide risk factors as the central theme, The exclusion criterion included review articles,opinion studies,unpublished research articles and the data was conceptualized by the primary reviewer .
Risk factors
There is no single cause for suicide. Suicide occurs when stressors exceeds current coping abilities of an individual. The stressors could be anything that can disturb the coping mechanism of an individual.
Moreover many other attributes are linked or associated with the risk factors of suicide which includes the following: 1. Gender: The suicide rates among males are higher than females. However the “gender paradox” prevails wherein female’s attempts suicide more than males. The common method used by males for both suicide and attempted suicide includes violent methods while those employed by females includes self poisoning. [21] 2. Age: The younger age group between 15-24 years are vulnerable and highly prone to commit suicide but the suicide risk increases with progression of age [22] 3. Marital status: Many studies have reported lower incidence of suicide among married individuals than divorced, separated and single individuals. Marriage provides an emotional bonding and provides psychological stability and helps the individual to maintain an integration with the society and community [22]. 4. Religion: Religion has a moderating effect on suicide. The spiritual values embodied in any religion equip the individual with the confidence and self realization to achieve an effective integration of body and mind [24]. 5. Unemployment: The association between unemployment and suicide are complex because several factors come into interaction. Unemployment leads an individual into many disadvantages-economic breakdown, social isolation and ego inferiorities. [25]. 6. Sexual orientation: There has been no robust studies that have examined the rates of suicide among gay, lesbian and bisexual individuals however available evidence suggests higher rates of suicidal behaviors among them [26]. 7. Psychiatric Illness: Many psychiatric illness namely depression, schizophrenia, substance abuse and conduct disorders are highly associated with suicide. Suicide is more common in bipolar depression than unipolar depression.The schizophrenic patients presents another major category exhibiting suicide. The life time suicide risk estimated in people with schizophrenia is 4.9% and an estimate of 5-13% dying by suicide [27]. The autopsy reports of suicide victims have identified significant blood alcohol levels [30-40%] which earmarks the strong association of substance abuse with suicide. Substance abuse increases the suicidal risk among females [28]. The conduct disorder may be one of the most common psychological findings among adolescence suicide victims. Studies revealed that conduct disorder, PTSD were the strongest predictors of individuals with ideations who were at higher risk of making suicide plans and attempts [29]. The chronic medical conditions which puts the individual to a lifelong agony such as coronary heart disease, stroke, chronic obstructive pulmonary disease, cancer, renal failure increases the chances of suicide however depression has found to be a strong confounder among physically ill people for increasing suicidal risk [30].
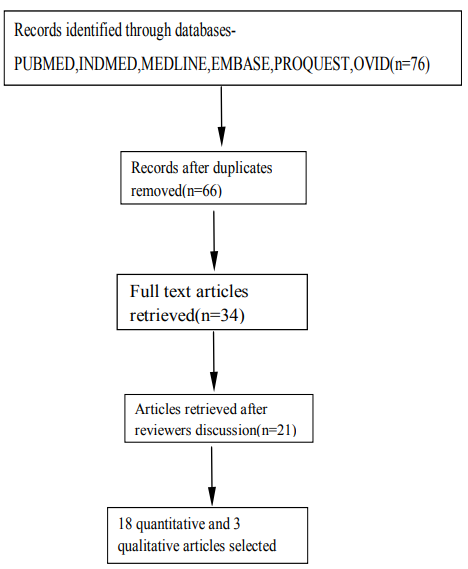
Figure 1: Flow chart showing literature search
Prevention
The prevenive strategies can be tailored on the basis of the risk factors addressed above.Suicide is a global phenomenon occurring all over the world at varying rate among different age groups. The World Health organization (WHO) has addressed the issue of suicide and a commitment was made by the member states of WHO to reduce the suicidal rate to 10% by 2010. The mental health gap action programme launched in 2008, includes suicide prevention as a priority and provides evidence based technical guidance to expand service provision in countries [31]. The preventive strategies could be better identified with primary, secondary and tertiary levels.
Primary prevention focus on reducing the number of new suicide cases in the community. Primary prevention is mainly focus on reduce the risk factors of suicide and improving the protective factors related with suicide. A comprehensive strategy involving different departments such as public health, education and employment are needed for primary prevention.The various measures includes: a) suicide awareness educational programmes detailing-what is suicide, warning signs, high risk factors and ways to use supporting systems in the communi- ty b) Improving and maintaining good communication between the child and parents-The modern day nuclear family system has increased communication gap between the child and parent leading to decreased ventilation of problems in children which may progress to suicide. Improved communications helps to solve their problems and offer them the emotional support in youths [32,33]. c) Emotional educational programmes in school helps to reduce suicidal ideation and suicidal attempts in school children d) Professional training programmes regarding suicidal assessment, planning, implementation, and evaluation of suicide prevention help to find out high risk group in the community and reduce the incidence of suicide. [34] e) Parents and teachers expectation level should be realistic about a child f) Parents and teachers should notify any deviations in the behavior of children to a health personnel especially a psychologist. g) Measures to tackle substance abuse and domestic violence should be initiated.

Figure 2: Multifactorial risk factors of suicide
Secondary prevention aims to reduce the suicidal attempts especially in the high risk groups identified through screening by interviews and administering questionnaire. Secondary prevention focus on the early detection of warning signs and high risk groups and treatment of mentally disturbed people. People experiencing suicidal ideation will exhibit a behavior change or an entirely new behavior manifested through covert or overt actions. These may include: substance abuse, social isolation, poor judgment or behavior, violent uncontrolled anger, seeking revenge, change in sleep pattern, mood changes, taking unnecessary risks, looking methods to kill themselves, such as searching in internet for different methods of suicide, apathy, breaking the law, cruelty towards others and to animals, self directed violence and violence directed towards others [35,36]. Early detection of high risk groups especially people affected with depression help to reduce the suicide. Antidepressant medications are widely used for the treatment of people who tries to commit suicide. Follow up of treatment with antipsychotic drugs helps to develop an adherence in people with suicidal attempts and reduce suicidal ideation [37]. The suicide incidence can be reduced by decreasing the access to the means of suicide. This in turn implies restricted access to poison substances such as pesticides, drugs, mercury, organophosphorus compounds and chemicals. Collaboration of health sector with other government sector will help to reduce easy availability of suicidal poisons [38]. The mass media such as news paper, television, internet, movies has a negative influence on suicide and increases the incidence by imbibing negative thoughts through exposure of social incidence exactly as it is Mass media exposes different methods of suicide and availability of lethal substances in the community. The responsible telecasting of suicidal news through mass media helps to discourage the people to commit suicide. Moreover reducing the toxicity of domestic gases, establishment of safety programs on high building and bridges help to prevent suicides and attempts [39]. The various kinds of psychotherapies such as behavioral therapy, group therapy, family therapy ,and individual therapies are more effective to reduce the suicidal attempts and incidence in high risk population since it provides an avenue to ventilate the inner conflicts and to avail emotional support [40]. The mental health of an individual is a vital component in maintaining the harmony of life which determines the overall nature of an individual-the way one thinks, feels and acts. The link between suicide and mental illness has already been proven and are robust. Henceforth the prevention of mental illness warrants the attention of public health system. In fact miniature tips such as eating well ,sleeping well, ventilating inner conflicts, active societal contact, maintenance of support systems-friends, family and significant others helps to maintain good mental health and reduces suicide rates in the community. Moreover special attention should be given to the individuals suffering from chronic somatic illness.
Tertiary prevention includes the rehabilitation and follow up. It helps to reduce the physical as well as psy- chological impairment occurred due to suicide attempts. Tertiary prevention is difficult to implement. Crisis intervention and psychosocial therapies are examples of tertiary suicidal prevention. Parental support and psy- chotherapy referrals have great impact on tertiary prevention of suicide. The role of society and family are in- dispensable in the tertiary prevention of suicide because they instill hope, encouragement and love to those who have escaped from the vicissitude of suicide.
Conclusion
Suicide is a dreaded illness that is paralyzing human life. Every effort should be initiated to arrest this illness from the incipient stage. A multispectral approach is helpful and effective in reducing the incidence of suicide. The literature review suggests the relative paucity of any specific intervention model to arrest suicide but there an enormous models of prevention which needs to be highlighted and brought to the public and to be incorporated into the public health services.
Acknowledgements
We render sincere thanks to the chief librarian Mr. Vijay Singh Chouhan of Bhopal memorial Hospital And Research centre for helping us to access the different databases. No funding has been received for the study.
Conflict of Interest
The authors report no conflict of interest.
Limitation
The study is a mini-review and the concepts addressed has not reached up to the highest level of evidencesystematic review.
References
World Health Organization, Suicide data.View
Vijaykumar, L. (2007). Suicide and its prevention the urgent need in India. Indian J Psychiatry 49: 81-84.View
National Crime Records Bureau ministry of home affairs accidental deaths & suicides in India 2014.View
Ritu, Modi., & Abha, Singh. (2012). Suicides in India and Its Preventions, shodh sanchayan 3: 15.View
Fleischmann, A., Bertolote, J.M., Belfer, M., & Beautrais, A.(2005). Completed suicide and psychiatric diagnoses in young people: a critical examination of the evidence. Am J Orthopsychiatry 75: 676-683.View
Links, P. (2006). Ending the darkness of suicide. Can J Psychiatry 51: 129-130.View
Roy, A. (2001). Consumers of mental health services. Suicide Life Threat Behav 31: 60-83.View
Nakagawa, M., Kawanishi, C., Yamada, T., Iwamoto, Y., & Sato, R., et al. (2009). Characteristics of suicide attempters with family history of suicide attempt: a retrospective chart review. BMC Psychiatry 32.View
Bahk, Y-C., Jang, S-K., Choi, K.H., & Lee, S-H. (2017). The Relationship between Childhood Trauma and Suicidal Ideation: Role of Maltreatment and Potential Mediators Psychiatry Investig 14: 37-43.View
Hardt, J., Egle, U.T., & Johnson, J.G. (2007). suicide attempts and retrospective reports about parent- child relationships, evidence for the affectionless control hypothesis. Psychosoc Med 4.View
Melhem, N.M., Brent, D.A., Ziegler, M., Iyengar, S., & Kolko, D., et al. (2007). Familial pathways to early-onset suicidal behavior: familial and individual antecedents of suicidal behavior. Am J Psychiatry. 164: 1364–1370.View
Isometsä, E.T., Henriksson, M.M., Aro, H.M., Heikkinen, M.E., & Kuoppasalmi, K.I., et al. (1994). Suicide in major depression. Am J Psychiatry151: 530-536.View
Saxby, P., Anil, R. (2012). Financial Loss and Suicide. Malays J Med Sci 19: 74-76.View
Conwell, Y., Duberstein, P.R., Hirsch, J.K., Conner, K.R., & Eberly, et al. (2010). Health status and suicide in the second half of life. Int J Geriatr Psychiatry 25: 371-379.View
Runeson, B., & Asberg, M. (2003). Family history of suicide among suicide victims. Am J Psychiatry. 160: 1525- 1526.View
Miller, N.S., Mahler, J.C., & Gold, M.S. (1991). Suicide risk associated with drug and alcohol dependence. J Addict Dis10: 49-61.View
Varghese, A., Khakha, D.C., & Chadda, R.K. (2016). Pattern and Type of Aggressive Behavior in Patients with Severe Mental Illness as Perceived by the Caregivers and the Coping Strategies Used by Them in a Tertiary Care Hospital. Arch Psy Nurs 30: 62-69.View
Jagodič, H.K., Rokavec, T., Agius, M., & Pregelj, P.(2013). Availability of mental health service providers and suicide rates in Slovenia: a nationwide ecological study Croat Med J 54: 444–452.View
Hor, K., & Taylor, M. (2010). Suicide and schizophrenia: a systematic review of rates and risk factors. J Psychopharmacol 24: 81-90.View
Latalova, K., Kamaradova, D., & Prasko, J. (2014). Suicide in bipolar disorder: a review. Psychiatr Danub 26: 108-114.View
LVörös, V., Osváth, P., & Fekete, S. (2004). Gender differences in suicidal behaviour. Neuropsychopharmacol Hung. 6: 65-71.View
Scottye, J. Cash, and Jeffrey A. Bridge (2009). Epidemiology of Youth Suicide and Suicidal Behavior Curr Opin Pediatr. Curr Opin Pediatr 21: 613-619.View
Kposowa, A. (2000). Marital status and suicide in the National Longitudinal Mortality Study. J Epidemiol Community Health 54: 254-261.View
O’Reilly, D., & Rosato, M. (2015). Religion and the risk of suicide: longitudinal study of over 1 million people, Br J Psychiatry. 206: 466-470.View
Radhakrishnan, R., & Andrade, C. (2012). Suicide: An Indian perspective, Ind J Psy 54: 304-319.View
Liu, R.T., & ustanski, B. (2012). Suicidal ideation and self-harm in lesbian, gay, bisexual, and transgender youth. Am J Prev Med 42: 221-228.View
Pompili, M., Amador, X.F., Girardi, P., Harkavy-Friedman, J., & Harrow, M., et al.(2007). Suicide risk in schizophrenia: learning from the past to change the future. Annals of General Psychiatry 6:10.View
Ilgen, M., & Kleinberg, F. (2011). The Link Between Substance Abuse. Violence Suicide Psychiatric times.View
American Psychiatric Association Strong Link to Suicide Found for Anxiety (2009). Conduct Disorders Psychiatric News Clinical & Research.View
Webb, R.T., Kontopantelis, E., Doran, T., Qin, P., & Creed, F., et al.(2012). Suicide risk in primary care patients with major physical diseases. Arch Gen Psychiatry 69: 671.View
World Health Organization preventing suicide a global imperative.View
Goldney, R.D. (1991). Suicidal Behaviour. In R Kosky, HS Eshkevari, V Carr (Eds). Mental Health and Illness. Butterworth- Heinemann, Sydney.
A framework for prevention of suicide in Australia (2000). Department of Health and Aged.View
A Rudd, M.D,. Berman, A.L., Joiner, T.E. Jr, Nock, M.K., Silverman, M.M. (2006). Warning Signs for Suicide: Theory, Research,and Clinical Applications. Suicide Life Threat Behav 36:255-62.View
Caldwell, D. (2008).The Suicide Prevention Continuum. Pimatisiwin. Summer 6: 145-153.View
Brenner, L.A., Barnes, S.M. (2012). Facilitating Treatment Engagement During High-Risk Transition Periods: A Potential Suicide Prevention Strategy Am J Public Health. 102(Suppl 1): S12–S14.View
Mann, J.J., Apter, A., Bertolote, J., Beautrais, A., & Currier, D., et al (2002). Suicide prevention strategies: a systematic review. JAMA 294: 2064-2074.View
World Health Organization (2017). Public Health Action For The Prevention Of Suicide.View
Hawton, K., & Williams, K. (2002). Influences of the media on suicide Researchers, policy makers, and media personnel need to collaborate on guidelines. BMJ 325: 1374-1375.View
Erlangsen, A., Stuart, E., Lind, B.D., Stuart, E.A., & Qin, P., et al (2014). Short-term and long-term effects of psychosocial therapy for people after deliberate self-harm: a register-based, nationwide multicentre study using propensity score matching, The Lancet Psychiatry 2: 49-58.View