
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care Volume 2 (2017), Article ID: JCNRC-118
https://doi.org/10.33790/jcnrc1100118Research Article
Experiences of Living with Dyspnea Among Taiwanese People with Chronic Obstructive Pulmonary Disease: A Qualitative Study
Wei-Chun Lin1, Tsuey-Yuan Huang2, Shiow-Li Hwang3*
1Department of Nursing, Min-Hwei Junior College of Health Care Management, Tainan, Taiwan.
2College of Nursing, Chang Gung University of Science and Technology, Taoyuan, Taiwan.
3*Department of Nursing, Asia University, Taichung, No. 500, Lioufeng Rd., Wufeng, Taichung, 41354, Taiwan.
Corresponding Author Details: Shiow-Li Hwang, Professor, Department of Nursing, Asia University, Taichung, Taiwan. E-mail: slhwang2@gmail.com
Received date: 09th September, 2017
Accepted date: 24th November, 2017
Published date: 11th December, 2017
Citation: Lin, W.C., Huang, T.Y., & Hwang, S.L.(2017). Experiences of Living with Dyspnea Among Taiwanese People with Chronic Obstructive Pulmonary Disease: A Qualitative Study. J Comp Nurs Res Care 2(2): 118
Copyright: Copyright: ©2017, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Purpose: Dyspnea is the primary complaint among patients with chronic obstructive pulmonary disease (COPD) and is a subjective physical experience responsible for considerable distress in patients. However, to date, research has tended to focus on measuring the severity of dyspnea, with few studies considering the subjective experiences among people living with COPD. The current study explored the experiences of living with dyspnea among patients with COPD.
Methods: In this qualitative descriptive study, we examined 12 purposively sampled outpatients with COPD from the Pulmonary Medicine Department. One-on-one in-depth interviews were conducted to collect information. Data reduction, data display and conclusion drawing that three-step method was adopted to analyze the data.
Results: Based on interview data analysis, 6 themes were devised regarding the dyspnea experiences of participants: (a) internal urgent situation signal resulting from a life-threatening incapability to respire; (b) triggering and straining; (c) constraints in life caused by insufficient inhalation; (d) immediate self-rescue strategies; (e) awareness of maintain health in daily life; and (f) coexistence with the disease and redefine self-concept.
Conclusions: As COPD progresses, people living with COPD experienced discomfort and developed self-rescue strategies by identifying the risk factors for dyspnea as well as measures for symptom deterioration. Most participants experienced loss of activity or physical functions in their daily lives, prompting them to begin reposition themselves. To maintain the existing functions of the patients is the main goal for both medical staffs and patients. The findings of this study can serve as a reference for medical teams to devise self-management plans for patients with COPD.
Key words: COPD; Dyspnea; Qualitative study; Self-care; Symptom management.
Introduction
Chronic obstructive pulmonary disease (COPD) is the third leading cause of death worldwide according to the World Health Organization [1]. The mortality rate of COPD is ranked seventh among the top 10 causes of death in Taiwan, according to the Department of Health of the Executive Yuan [2]. The number of patients with COPD increases annually and is responsible for the substantial economic burden of this disease [3]. COPD is an irreversible disease characterized by airflow obstruction that cannot be completely cured by medicines, and dyspnea is the primary symptom of COPD [4].
Search strategy
Dyspnea is a subjective perception of breathing discomfort that consists of qualitatively distinct sensations of varying intensity. This experience is derived from the influences of physiological, psychological, social, and environmental factors and results in physiological and behavioral reactions [5,6]. In patients with COPD, dyspnea is a constant perception that constrains their daily lives. Patients must adapt to the constraints caused by such symptoms of COPD [7]. Studies have revealed that constraints to daily life provoke negative psychological emotions, which affect the quality of life of patients with COPD [8,9]. In addition, the subjective experience of dyspnea includes several qualitative descriptions. According to a relevant study, approximately 51% of patients stated “my breathing requires effort,” 49% stated, “I feel out of breath,” and 38% stated, “I cannot get enough air in” [10]. The intensity of dyspnea plays a crucial role in determining the overall quality of life of patients and their reactions to treatments; therefore, evaluating and measuring the intensity of dyspnea is essential for managing such patients effectively. Clinically, medical staffs use device- (pulse oximeter) and laboratory-based examinations (arterial blood gas analysis) to measure dyspnea intensity. However, such objective tools often fail to manifest the subjective experience of dyspnea, thus prompting the need for self-report tools [11].
Risk factors
As COPD progresses, the lung functions of patients deteriorate and the severity of acute exacerbation increases. Studies have shown that patients with COPD adjust their lifestyles and seek medical treatment to avoid dyspnea [12]. Clinically, we found that patients with COPD may have at-home personal respiratory equipment (e.g., an oxygen concentrator or sprayer), but most patients require emergency care at a hospital when such equipment cannot alleviate their symptoms quickly. In addition, a Taiwanese study indicated that most patients with COPD lack sufficient self-care skills. Therefore, understanding the experiences of patients is the first priority to improve effectiveness of self-care [13].
The severity of dyspnea affects the quality of life of patients, and its complex mechanisms alternately also provoke physiological, psychological, and emotional changes [9,14]. Objective clinical examination reports cannot completely express the perceived intensity of dyspnea, and self-report tools also fail to encompass the essence of this experience [11]. There are limited studies considering the subjective experiences of living with dyspnea from patients’ perspective. Few qualitative studies reported the experiences of selfmanagement in patients with COPD [15,[16]. The aim of this study is to explore the experiences of living with dyspnea among people with COPD. To describe the subjective perceptions and experiences of dyspnea in-depth, this study adopted a qualitative method, focusing on the patient-centered perspective.
Methods
Study design
A qualitative descriptive study was conducted using one-on-one face to face in-depth interviews, comprising semistructured questions (Table 1).
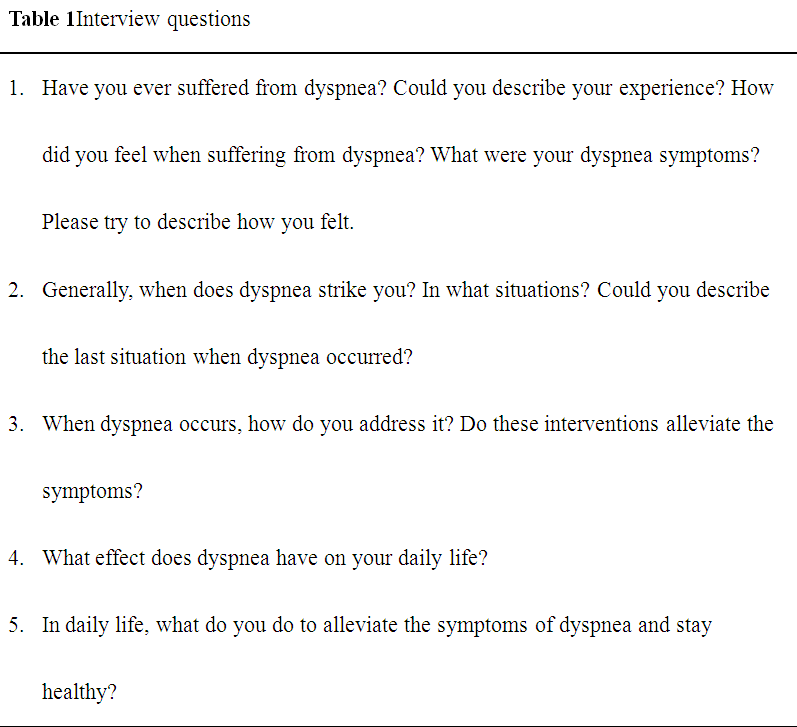
Table:1 Interview questions
Participant selection
The study participants were diagnosed with COPD by a thoracic physician and were selected using purposive sampling. Participants who were diagnosed with COPD and lung function of forced expiratory volume in first second/ forced vital capacity (FEV1/ FVC) < 70%, had experienced dyspnea, were sufficiently lucid to communicate in Mandarin Chinese or Taiwanese were included in this study. The thoracic physician identified and invited participants in research.
Data collection
Data were collected at the Pulmonary Medicine Department of a medical center in Central Taiwan. The researcher (primary author) used semi-structured questions and interviewed the participants individually. Each interview was audio recorded and subsequently transcribed. Each interview lasted 30 to 50 minutes. The study data were simultaneously collected and analyzed, and text compilation, encoding, and analysis were conducted after each interview. When the data analysis failed to yield new themes, data saturation was considered, and data collection was discontinued.
Ethical considerations
This study was approved by the Institutional Review Board of the organization where the research was conducted. The interviewer presented the purpose of the study and the participants completed the informed consent form before interview. Considering that the patients may experience difficulty in breathing while speaking, the researcher adjusted the interview period according to their convenience and ended the interview if the patient experienced any discomfort. To protect the privacy of the participants, the audio files and written documents were encoded, without the names of participants.
Data analysis
Content analysis with three-step method [17] was adopted to analyze the data by the researchers. Step 1: Data reduction: After reading the interview transcripts several times to gain a comprehensive understanding of the participants, the researcher identified the crucial statements, line by line, without making any assumptions. Step 2: Data display: In this step, diagrams were developed to display the relationships between codes, followed by pattern coding. Step 3: Conclusion drawing: By organizing the aggregate formulated meaning into clusters of themes, themes and subthemes were identified and named to describe the dyspnea management experiences of each patient. Furthermore, after complete data analysis, the text is translated by a trilingual who knows Taiwanese, Chinese and English. The authors have reconfirmed the wording in English and the original intent in Chinese are the same.
Rigor
The rigor of this study was based on the four evaluation criteria proposed by Lincoln and Guba [18] to establish the trustworthiness in qualitative research (credibility, transferability, dependability, and confirmability). Only patients with COPD who clearly met the inclusion criteria were enrolled in the study, and data collection was performed until saturation to ensure that these findings were transferable to similar contexts. Voice recording and note taking were conducted throughout the interviews, and the audio files were subsequently transcribed. Before and after each interview, the researcher highlighted the thoughts relevant to the study aims and objectives. Moreover, the researcher recorded reflections after each interview. During analysis, the researchers endeavored to remain objective and neutral. Two qualitative research experts categorized the thoughts according to the codes provided. Finally, two participants read and validated the derived conclusions.
Result
Participant characteristics
The participants comprised nine males and three female patients, with a mean age of 67 years, possessing an FEV1/FVC value between 42 and 68, and FEV1% of the predicted value between 28% and 79%. According to Global Initiative for Chronic Obstructive Lung Disease (GOLD) [3] the severity classification of COPD is based on airflow limitation (FEV1% of the predicted value), among these participants, six, four, and two of them belonged to GOLD Stages II (moderate, 50% < FEV1< 80 % predicted), III (severe, 30% < FEV1 < 50% predicted), and IV (very severe, FEV1 < 30% predicted), respectively. Table 2 lists the themes and sub-themes deduced from the data which will be discussed in turn.
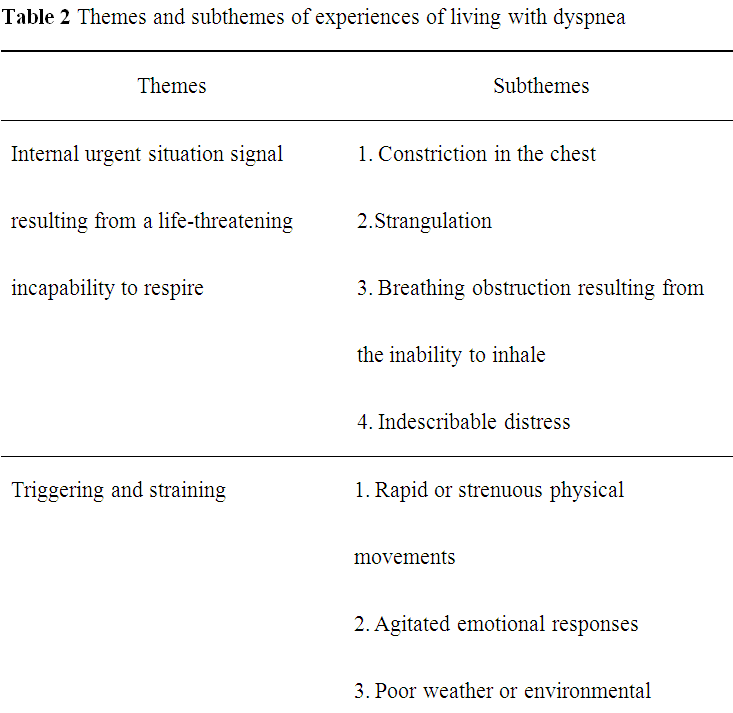
Table:2 Themes and subthemes of experiences of living with dyspnea
Theme 1: Internal urgent situation signal resulting from a lifethreatening incapability to respire
Dyspnea often begins with constriction, tightness, and pain in the chest. When the dyspnea attacked, the participants in this study experienced unpleasant feelings including constrictions and strangulations in the chest, an inability to inhale perceived as stoppage of breathing, and an indescribable distress. The participants feel life threatening when attacked by dyspnea. These feelings of dyspnea of the participants are the emergency signals that threaten to life.
When gasping, I felt tightness in my chest. It was like being pressed by something [touching the chest] and like someone was strangling me. I could not breathe. . .
(Participant 1) When gasping, I could not breathe. My heart going to stopped and feeling dying… (Participant 4) I felt extremely uncomfortable. I could not inhale air. I gasped heavily, and suddenly it seemed that I could not breathe anymore and I was going to faint. (Participant 6)
Theme 2: Triggering and straining
The participants realize that dyspnea is easily triggered in certain situations that are likely or inevitable in daily life, such as rush actions and intense physical activities, over emotional responses, poor weather or poor environment changes, and respiratory tract infections, after they experiencing dyspnea acute exacerbation.
Strenuous activities often trigger dyspnea in the participants, including walking rapidly, climbing stairs, stooping and standing back, completing chores, lifting and carrying heavy objects, and speaking loudly.
Mostly when I am walking! I gasp when I walk and speak loudly. (Participant 1) . . . I gasp when I walk faster than normal, or stoop and stand back. (Participant 2) . . . Of course when I carry heavy things! I have to use my arm strength, and immediately start gasping. (Participant 3) . . . I gasp when I hang or take down clothes and wash bowls. It would be fine if I did not move my hands. (Participant 4)
Emotional fluctuations are reported as another cause of dyspnea by participants, with nervousness being the most common condition, which is often provoked by an urgent need to urinate or bodily pain. Anger can also trigger dyspnea.
I am too nervous. Because I am impatient, I feel nervous even when taking off my trousers to urinate. When I feel the urgent need to urinate, I have to go. When I am nervous, I start gasping. If I am irritated, or angered by a conversation, I gasp when I am mad. (Participant 1)
I stumbled and hurt my waist. It was extremely painful when I moved. I felt nervous when I felt the pain, and I gasped when I felt nervous . . . (Participant 4)
In addition, common colds exacerbate the respiratory illness of participants, thereby increasing the intensity of their dyspnea.
I gasp heavily! I have a weak immune system. If I catch a small cold and cough, it is really uncomfortable to cough and gasp with phlegm in my mouth [a rise in the tone]. (Participant 2) I caught a cold a while ago and I coughed, which made me gasp. . . (Participant 3).
Unstable weather conditions and temperature changes can also trigger dyspnea. Low temperatures in winter, humidity on rainy days, and typhoons concern COPD participants the most because climate changes can increase the frequency of dyspnea episodes.
In that heavy rain…The rain on that day was very heavy. I gasped heavily. Cold weather often triggers my illness. I am really afraid of the cold! I am worried if the weather condition is terrible, which easily induces my gasp. My body is only vulnerable to winter. When typhoons come, dyspnea often occurs. (Participant 4).
In addition, air quality is critical for participants with COPD. Inhaling smoke from the air causes participants to experience discomfort in their chest, triggering dyspnea.
My son did not put out his cigarette, and I smelled it. The smoke kept coming out, and I felt very uncomfortable when smelling and inhaling the smoke. I was going to gasp . . . (Participant 4).
The dust caused by sweeping and the smoke and poor-quality air make me gasp. (Participants 7).
Theme 3: Constraints in life caused by insufficient inhalation
In general, patients suffering from irreversible COPD gradually lose the ability to move as their lung function deteriorates. Dyspnea causes numerous inconveniences in daily life, thus requiring participants to alter their lifestyle, and often results in a helplessness to deal with daily-life activities, a decrease in social and entertaining activities, and an inability to sleep on back, which results in insufficient sleep.
Dyspnea renders participants unable to perform daily chores around the house or any laborious tasks. All participants must stop working when dyspnea occurs; thus, they may be considered incompetent and are frequently unemployed.
I gasped even though I just made a few movements, and I could not continue if I gasped. In the end, I did not go anymore. My work was laborious, and I had to carry heavy things! I use my arm strength, but I gasped when I did this. I just could not work. (Participant 3).
I cannot work, including washing and hanging clothes. If I do, I start gasping. The gasping starts right away! (Participant 4)
Regarding daily-life activities, participants with dyspnea require help from others to use the toilet, shower, change clothes, and eat food. Moreover, the symptoms of certain participants necessitate 24-h care from family members.
I gasp when attempting to put on or change clothes and trousers. It is better if someone is near to help. (Participant 1)
There are also miscellaneous problems in daily life! To sum up, it is very tough! I need my family to take care of my life, even when I want to go to the toilet. I cannot put on clothes and trousers or take a shower by myself! I gasp as soon as I start walking. Now I spend more time sitting. I need someone to bring my meals. I need someone to be with me all day long. (Participant 2)
Dyspnea also limits the range of activities for patients with COPD, thus preventing them from participating in leisure activities. Some participants seldom go out and interact with other people, lest their illness frighten their friends.
Healthy people are afraid of contacting with patients. I go out less often. Because I am empathetic, I do not want to scare, bother, contact, or frighten other people. I practice celestial doctrines to be relatively thoughtful. (Participant 1)
I always stay at home. I rely on the oxygen. If my situation improves, my daughter-in-law sometimes takes me out in my wheelchair, but not for long. (Participants 2)
I seldom go out. In the past, I shopped in traditional markets, walked, played, and saw beautiful clothes! Now I cannot do so! (Participant 4)
Dyspnea also prevents participants from sleeping on their back, leading to insufficient sleep. In addition, respiratory symptoms, such as coughing, are easily triggered by low night-time temperatures, which interrupts sleep and results in poor sleep quality.
When I lie down I feel difficulty in breathing, I have to sit up. Gasping makes me to sit up. I cannot fall asleep because I cannot lie down . . . (Participant 1) I feel tightness in my chest when lying down, then I gasp. If I gasp, I have to sit up. If I cough, I wake up, and I cannot get enough sleep. It is like [sleeping] lightly. Therefore, my sleep quality becomes poor. (Participant 3)
Theme 4: Immediate self-rescue strategies
Participants with COPD who chronically suffer from dyspnea accumulate experience and health knowledge during their illness, with these experiences and knowledge they develop self-rescue strategies. Thus, they know about the immediate management for alleviating the discomfort caused by dyspnea. When dyspnea occurs, participants can adopt several self-rescue strategies including halting an ongoing activity, changing positions (sitting up or down in a comfortable position), taking a bronchodilator or inhaling oxygen, adjusting breathing, and calming emotions. When these immediate strategies do not alleviate discomfort, most participants seek medical assistance at a hospital or a clinic.
When gasping, I have to hold myself. I have to sit down and rest. I do not bend my legs but stretch them to facilitate blood circulation. (Participant 1) I use the sprayer first. I bear the discomfort and tell myself to breathe lightly. Breathe lightly and steadily. Inhale lightly and exhale lightly. Adjust your strength so that you do not have to spend effort breathing. Oxygen helps a little, and it makes me gasp less. But, when I gasp really heavily, it does not work; even if I switch it to the highest level 5 and use the sprayer, the symptoms are not eased. In this situation, I have to go to the hospital. (Participant 2)
When gasping and feeling uncomfortable, I go to the clinic. Sit down and do not move and the symptoms gradually disappear. (Participant 3)
Theme 5: Awareness of maintain health in daily life
Participants with COPD recognize that their full lung function is irreversible; thus, they adopt defensive measures in their daily lives, such as altering their lifestyle to reduce the frequency of dyspnea episodes. Regularly visiting a physician and following medical advice are basic for decelerating the speed of exacerbation and reducing the frequency of such episodes.
I have been with Doctor Tsao for many years. I come back for follow-up examinations unless I am busy with other things. I use inhaled medications according to the instructions. (Participant 3)
Regarding diet, participants are aware that stimulant and strong tonic foods can harm them; thus, they must not eat cold-nature foods. In addition, the participants have to adjust their dietary habits and quit smoking and consuming alcohol. In addition, some participants consider their lungs to be dirty and clean them using herbal medicines.
I quit smoking, drinking, and eating irritating foods. Now, I do not eat strong tonic foods anymore. For example, dishes with sesame oil and stews are bad. (Participant 3) Do not eat spicy and irritating foods. Do not eat icy or cold-nature foods, such as Chinese radish, Chinese cabbage, and watermelons. These foods should be avoided. (Participant 5)
… If I breathe in dirty air, I must clean my lungs. Lungs are too dirty. Therefore, it is better to evacuate my body timely. I eat some detoxification herbs from time to time. In the mountains where I live, there are detox herbs. (Participant 1)
With the progression of COPD, participants identify the factors causing breathing difficulties and adopt countermeasures. They know that changeable weather is an unavoidable cause and thus focus on keeping warm, particularly the regions around their neck.
When the weather is cold, I wear a high-collared shirt to protect my neck. In winter, I cannot expose my neck to the cold air, or dyspnea occurs. (Participant 4)
Theme 6: Coexistence with the disease and redefine self-concept
Because of physical restrictions, participants with COPD cannot carry out many daily activities; hence their self-concepts become altered. Some participants consider themselves handicapped and useless or even dead because of the loss of physical functions. They feel that they can sit only like a fool and are unable to act on their own volition. The presence of an irreversible pulmonary disease causes participants to feel as though they are heading toward death, implying that they can only wait for the end to come. However, some participants think that the time of death cannot be predicted and thus attempt to remain optimistic and take care of their bodies.
I cannot do what I want to do. I am as useless as a dead person. I can only complain that I am ill-fated and unlucky. (Participant 1)
I do nothing and sit like a fool. I cannot do anything, nothing! (Participant 4) I am finished! I am so disabled and incompetent! When thinking about the future, I see little hope. (Participant 6)
I am not a person who does not feel upset, I have that feeling, but I still go out and sit with my friends. We can spend the day chatting, or feel upset and keep thinking about the annoying things, which makes us feel unhappy and wear a sad face. We can spend a day in either way. To sum up, do not think too much. Be optimistic and do whatever you want to do. (Participant 3)
Discussion
In this study, when experiencing dyspnea, people living with COPD experienced a life-threatening inability to breathe, with a feeling of constriction and strangulation in their chest, an inability to inhale, and indescribable pain; consequently, their body sent emergency signals. Tsou et al. [16] reported that patients with COPD were attentive to and observed the changes within their body. In the event of dyspnea, participants experienced a tightened chest, feeling of choking, and heavy breathing. In addition, Victorson et al. [19] observed that patients with COPD described their experience with dyspnea as heavy and laborious breathing, an inability to breathe, or a lack of oxygen; this clearly indicates that the physiological discomfort of dyspnea is unbearable. Thus, clinicians and medical staffs must consider whether objective clinical evaluation methods encompass the actuality of life for patients with COPD and adequately demonstrate the degree of their discomfort. The intensity or acute exacerbation of dyspnea may be ameliorated or prevented if the involved clinical staff understands the primary symptoms of a patient and informs them about the emergency signals transmitted through their systems.
The current study also revealed the causes of dyspnea, including rapid or laborious physical movements, excessive emotional responses, respiratory tract infections, and poor weather or environmental conditions. These findings are consistent with those reported by Victorson et al. [19]. The obstruction of peripheral airways impedes the airflow, thereby increasing the physical burden of moving [10,20]. In addition, long-term intake of steroids weakens the immune system of patients with COPD, thereby increasing their vulnerability to contract other respiratory diseases. Respiratory infection is the major cause of acute exacerbation and hospitalization in patients with COPD [3]. However, excessive emotional responses triggered the dyspnea was rarely reported in previous studies. Thus, medical staffs must evaluate the experiences reported by such patients, identify the factors that are most likely to trigger dyspnea, and instruct them to avoid such factors.
COPD causes numerous inconveniences in daily life. People living with COPD can no longer undertake daily activities and lose their ability to work. Concurrently, such people also reduce or eliminate their social and recreational activities. The heavy burden on the heart and lungs caused by COPD prevents participants from sleeping on their backs, thereby resulting in insufficient sleep. These constraints to daily activities correspond with the findings reported by Hasson et al. [21] regarding the experiences of patients with COPD. Dyspnea affects every aspect of the patients’ lives, forcing them to rely on their caregivers. Barnett [22] indicated that patients with COPD become anxious, frightened, scared, distressed, and exhausted because of dyspnea to the degree that they stop participating in social activities. In the current study, in addition to physical discomfort, the most influential secondary reactions identified were the inability to perform physical movements and the loss of endurance. Few previous studies have addressed the sleep disorder reported by the current study participants; however, sleep is a critical requirement for every human, and thus, the problems caused by sleep disorders should not be ignored. The participants in the current study primarily comprised patients with severe and very severe COPD (FEV1% <50). Cor pulmonale and right heart failure often occur in the later stages of COPD, and sleeping on the back increases the burden on the heart, which results in breathing difficulties and indirectly affects the sleep quality of such patients. Therefore, both medical staffs and home-based caregivers can provide appropriate assistance to people living with COPD by adequately understanding the constraints on their daily lives.
This study also revealed that people living with dyspnea strove to self-rescue by devising countermeasures and learning how to alleviate the symptoms when they occur. O’Neill [23] investigated the coping strategies of patients with COPD and determined that the most common strategies included adjusting breathing patterns, taking medications, resting, and undertaking appropriate preventive measures; these findings correspond with those reported in the current study. In the event of dyspnea, stoppage of the ongoing activity and resting can reduce the need for oxygen, and patients with COPD often change their positions to alleviate the symptoms [24]. When experiencing acute episode of dyspnea, the participants reacted according to their past experiences or the health knowledge provided by the medical staff; however, a visit to a physician remained the only certain safety assurance. In future, personal treatment or maintenance plans to cope with COPD symptoms should be devised to implement home-based self-management mechanisms in daily life.
Moreover, to maintain their existing health, most participants undertook daily measures to protect against and prevent dyspnea. There are some behaviors to maintain a healthy lifestyle, such as changing dietary habits for example, not eating cold-nature foods, avoiding irritating or overly nutritious foods. Furthermore, keeping their body warm, quitting smoking and alcohol consumption. Some participants also used complementary therapy such as taking herbal medicines, that relatively rare in Western countries. This was similar to results of a Taiwanese study that indicated most patients with COPD maintain healthy lifestyle based on traditional Chinese medicine [15]. This indicated that cultural factors influence self-care behaviors in people living with COPD. Therefore, medical teams should be multicultural and healthcare providers must consider the cultural differences.
In this study, most participants repositioned themselves to live with the disease, whereas other participants pessimistically regarded that they were incompetent; such participants not only accepted misfortune but also awaited death or intended to commit suicide. However, some participants remain optimistic, endeavoring to change their mindset. According to previous studies, patients with COPD often feel melancholy, anxious, distressed, and frightened, and worry about their future. When such patients feel disappointed, the thought of dying inevitably provokes the fight against breathing [21,22]. Another study indicated that patients with COPD adjusted their emotions and strove to shift from negative to positive moods [15]. The current study revealed that the people living with COPD repositioned themselves to attain balance between the disease and their lives. Considering themselves to be dead or foolish did not offer additional ideas or behaviors to their lives. Despite being less discussed in previous studies, this finding is a message, suggesting that medical teams determine how patients perceive themselves and help and encourage them to re-establish confidence and live with their disease.
Study limitations
There are two limitations in this study. First, this study lacks the experiences from patients with mild COPD. In general patients who suffer from acute exacerbations of dyspnea typically exhibit moderate to severe COPD. Nevertheless, the current study still presents the dyspnea experiences of people living with COPD. Second, the data have been collected in a medical center, the differences in medical care pattern which may have had some influence on research results. Therefore, the participants’ experiences do not represent all the patients with COPD. The results of this study are as references only for relative study in the future.
Conclusions
In this study, we investigated the dyspnea experiences of people living with COPD. Based on their descriptions, people living with COPD experienced discomfort caused by dyspnea and developed self-rescue strategies by identifying the risk factors for dyspnea as well as measures for symptom deterioration. Because COPD is irreversible, patients who experienced loss of activity or functions in addition to several other inconveniences in their daily lives began to reposition themselves. Medical interventions should be administered based on patient needs to provide solutions and intervention plans that adequately satisfy the patients. The findings of this study can serve as a reference for medical teams to devise interventions such as self-management plans. Additional interventional experimental studies could be performed in the future to evaluate the effects of such management plans.
Conflict of interest
The authors of this paper have no conflicts of interest to report.
Acknowledgment
The authors are grateful for the cooperation of the participants in this study, and the assistance from the staff at the Pulmonary Clinic of the Department of Internal Medicine of Chung Shan Medical University Hospital.
References
World Health Organization. The 10 leading causes of death in the world.View
Taiwan (R.O.C.): Ministry of Health and Welfare. Cause of death in 2015.View
Global Initiative for Chronic Obstructive Lung Disease.Global Strategy for Diagnosis, Management, and Prevention of COPD.View
Lopez-Campos, J.L., Calero, C., & Quintana-Gallego, E. (2013). Symptom variability in COPD: a narrative review. Int J Chron Obstruct Pulmon Dis 8: 231-238.View
American Thoracic Society (1999). Dyspnea. Mechanisms, assessment, and management: A consensus statement. Am J Respir Crit Care Med159: 321-340.View
Lee, Y.H., Yang, C.C., Wang, K.Y., & Tang, Y.Y. (2005). Dyspnea: A concept analysis. J OncNurs5: 43-50.
Harris, S. (2007). COPD and coping with breathlessness at home: a review of the literature. Br J Community Nurs 12: 411-415.View
Paz-Diaz, H., Montes de Oca, M., Lopez, J.M., & Celli, B.R. (2007). Pulmonary rehabilitation improves depression, anxiety, dyspnea and health status in patients with COPD. Am J Phys Med Rehabil 86: 30-36.View
Iguchi, A., Senjyu, H., Hayashi, Y., Kanada, R., & Iwai, S., et al.(2013). Relationship between depression in patients with COPD and the percent of predicted FEV(1), BODE index, and health-related quality of life. Respir Care 58: 334-339.View
O’Donnell, D.E., Banzett, R.B., Carrieri-Kohlman, V., Casaburi, R., & Davenport, P.W., et al. (2007) Pathophysiology of dyspnea in chronic obstructive pulmonary disease: a roundtable. Proc Am Thorac Soc 4: 145-168.View
Meek, P.M. (2004). Measurement of dyspnea in chronic obstructive pulmonary disease: what is the tool telling you? Chron Respir Dis 1: 29-37.View
Chen, Y.M., Hsin, H.C., Hsu, J.Y., & Wu, L.F.(2004). The lived experience of self-care in the elderly with chronic obstructive pulmonary disease.VGH Nursing 21: 105-118.
Lee, C.Y., Yeh, L.L., Chen, C.Z., Lin, P.Y., Hsiue, T.R., et al. (2005). Exploring self-management in patients with chronic obstructive pulmonary disease. J Nurs 55: 45-55.
Scano, G., Gigliotti, F., Stendardi, L., & Gagliardi, E. (2013). Dyspnea and emotional states in health and disease. Respir Med 107: 649-655.View
Chen, K.H., Chen, M.L., Lee, S., Cho, H.Y., & Weng, L.C. (2008). Selfmanagement behaviours for patients with chronic obstructive pulmonary disease: a qualitative study. J Adv Nurs 64: 595-604.View
Tsou, C.T., Lu, Z.Y., Lin, H.C., & Maa, S.H.(2009). The self-management living experience of patients with chronic obstruction pulmonary disease. J Nurs Health Res5: 293-301.
Miles, M.B., & Huberman, A.M. (1994). Qualitative data analysis: An expanded sourcebook. (2nd ed.), Thousand Oaks, CA: Sage Publications.View
Lincoln, Y.S., & Guba, E.G. (1985). Naturalistic inquiry. Beverly Hills, CA: Sage Publications.View
Victorson, D.E., Anton, S., Hamilton, A., Yount, S., & Cella, D. (2009). A conceptual model of the experience of dyspnea and functional limitations in chronic obstructive pulmonary disease. Value Health 12: 1018-1025.View
O’Donnell, D.E., & Laveneziana, P. (2007). Dyspnea and activity limitation in COPD: mechanical factors. COPD 4: 225-236.View
Hasson, F., Spence, A., Waldron, M., Kernohan, G., & McLaughlin, D., et al. (2008). I can not get a breath: experiences of living with advanced chronic obstructive pulmonary disease. Int J Palliat Nurs 14: 526-531.View
Barnett, M. (2005). Chronic obstructive pulmonary disease: a phenomenological study of patients’ experiences. J Clin Nurs 14: 805-812.View
O’Neill, E.S.(2002). Illness representations and coping of women with chronic obstructive pulmonary disease: a pilot study. Heart Lung 31: 295-302.View
Gosselink, R. (2003). Controlled breathing and dyspnea in patients with chronic obstructive pulmonary disease.J Rehabil Res Dev 40: 25-33.View