
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care Volume 2 (2017), Article ID: JCNRC-119
https://doi.org/10.33790/jcnrc1100119Research Article
Tai Chi Training and Educational Intervention Improved Self-care Behaviors and Lowered Blood Pressure in Hypertensive Outpatients
Hui-Min Lo1*, Wen-Xiang Chen2, Shu-Chuan Chang2
1Department of Nursing, Catholic St. Mary’s Junior College of Medicine, Nursing and Management, Yilan, Taiwan.
2Department of Nursing, Tzu Chi University, Hualien, Taiwan
Corresponding Author Details: Hui-Min Lo, Assistant Professor, Department of Nursing, Catholic St. Mary’s Junior College of Medicine, Nursing and Management, Yilan, Taiwan. E-mail: hmlo@smc.edu.tw
Received date: 16th August, 2017
Accepted date: 10th December, 2017
Published date: 27th December, 2017
Citation: Lo, H.M., Chen, W.X., & Chang, S.H. (2017). Tai Chi Training and Educational Intervention Improved Self-care Behaviors and Lowered Blood Pressure in Hypertensive Outpatients. J Comp Nurs Res Care 2(2): 119.
Copyright: Copyright: ©2017, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Purpose: Self-care is important for numerous reasons. Self-care can reduce health costs, improve patient quality of life, and increase mental well-being. Self-care is also a mediating factor of chronic disease and increases patient confidence when facing challenges associated with the disease. However, how to improve blood pressure control and promote self-care behaviors in hypertensive cohorts is not as well understood. The purpose of this study was to assess the effectiveness of two interventions (Tai chi training and educational program) in lowering blood pressure and improving selfcare behaviors.
Methods: A quasi-experimental, two-group repeated-measures design was used. The control group (n=31) received standard medical treatment as prescribed by a supervising physician. The experimental group (n=27) received an eight-week Tai chi training and educational intervention. Self-care behavior was measured by the Self-Help Questionnaire. Blood pressure was measured at three time-points: a baseline prior to study commencement, week four, and week eight of the study.
Results: The experimental group showed significant improvement in self-care behavior (F= 6.28, P=0. 000), self-efficacy (F=3.23, P=0.001), and quality of life (F=5.44, P=0.002), as well as a significant reduction between in systolic blood pressure (t=2.57, p<0 .001) and diastolic blood pressure (t=2.86, p <0.001) compared to the control group.
Conclusions: The results are encouraging and suggest that Tai Chi training and educational program may be effective in lowering blood pressure and increasing self-care behaviors in hypertensive outpatients.
Key words: Tai Chi, self-care, behaviors, quality of life
Introduction
Hypertension (high blood pressure) is one of the world’s most common chronic health condition and is a leading cause of death in Asia and the world [1]. The World Health Organization (WHO) estimates in 2004 that >1 billion people were diagnosed with hypertension and > 7.1 million people died of hypertension or hypertension- related diseases [2]. The prevalence in the community aged 20 years and above in the United States is estimated to be 28.7% [3]. However, the prevalence in Taiwan was found to be as high as 24.9% [4]. The prevalence of hypertension in Taiwan is similar to the prevalence in western countries. It has been estimated that in Asia up to 66% of deaths from cardiovascular disease, including myocardial infarction and cerebral apoplexy, may be attributable to hypertension [5].
Reduction of blood pressure (BP) after stroke or transient ischaemic attack (TIA) prevents further vascular events [6]. According to previous findings, multifaceted interventions incorporating various methods offer a more effective and comprehensive approach to controlling BP [7]. Current clinical policy, based on the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure, recommends that peo- ple with hypertension engage in six self-care activities: adhering to anti-hypertensive medication regimens, maintaining or losing weight, following a lowsalt diet, limiting alcohol, engaging in regular physical activity, and eliminating tobacco use [8]. Reasons for patient non-adherence to six self-care activities include: quality of information received by patient, impact of self-care activities in the patient’s life, and the patient’s beliefs regard- ing their health and medication [9].
Patients’ education, their knowledge of hypertension risk factors, their perception of the benefits and potential risks of treatment, and their active participation in treatment decisions have been found to affect their compliance with treatment recommendations [10]. Selfcare plays an important role in helping patients modify unhealthy lifestyles and behaviors [11]. The research on patient compliance with hypertension control guidelines focuses on medication, diet control, and exercise [12]. There are only a few studies that specifically address the issue of compliance with recommendations for a healthy lifestyle, and self care behaviour [13], few of which were con- ducted in Taiwan. The objective of the present study was to explore factors associated with the compliance of hy- pertensive patients with lifestyle recommendations regarding exercise, medication compliance and proper diet.
Tai Chi is a traditional Chinese mind-body exercise. Tai Chi sessions incorporate a wide range of physical movements, including slow, meditative, flowing, dance-like motions. Its unique characteristics include mind concentration with breathing control, whole-body exercise in a semi-squat posture, and continuous. Tai Chi is being practiced, deep diaphragmatic breathing with mind concentration is integrated into body motions to achieve a harmonious balance between body and mind. A study conducted with a before and after design reported that Tai Chi exercise of one hour sessions, twice per week for three months improved the physical function, general health, and mental health [14]. Another quasi-experimental study with repeated measures using Tai Chi training of 50 minute sessions, two times per week for 15 weeks also proposed that Tai Chi was beneficial for sleep quality, mood, and perceived stress hypertension patients [15]. Thus, in the past, Tai Chi exercise was considered to be associated with improvements in psychological well-being, including reduced stress, anxiety, depression and mood disturbance, and increased self-esteem.
The Braden Self –Help Model has previously been applied to patients with chronic disease such as chronic pain, rheumatic arthritis or arthritis-related conditions [11]. Self-help can reduce health costs, improve quality of life, and increase mental well-being. Braden hypothesized self-help to be an important mediating factor in chronic disease, and increase patient confidence when dealing with disease challenges [11]. We developed a new Web-based selfhelp intervention, which may be used by patients with a variety of co-morbid conditions, based on problem-solving [16]. The self-care programs that are currently available have all been developed for patients with chronic disease [17], and most are based on cognitive behavioral therapy (CBT). CBT is a problem-solving therapy. It is a brief form of psychotherapy where patients identify their most immediate problems and ways of regaining control over them. CBT is not limited to one specific disorder and may be effective in treating several problem areas [18].
This study aimed to evaluate the effects of the Tai Chi training and educational intervention on the blood pressure control, selfcare behavior and self-efficacy among hypertensive outpatients. The development of the Tai Chi training and educational intervention were a multidisciplinary collaboration. The interventions focus on patient lifestyle modification through a combination of health education and exercise implementation. The Tai Chi training and educational intervention proved effective in controlling systolic BP and improving self-care behavior, self-efficacy and quality of life. These findings reveal a clear need for clinical application of interventions focusing on self-care behavior.
Methods
Study design and patient population
After approval by a local hospital institutional review board (IRB), a meeting was held with a group of hypertensive adults (n =74) in the hospital to explain the purpose and process of this study and obtain informed consent. During the study process, 16 participants withdrew because of a lack of interest, relocation to other cities or missed follow-up (s). 58 participants completed the study. These 58 participants were randomly divided into an experimental group comprised of 27 participants and a control group comprised of 31 participants (see Figure 1). The experimental group received Tai chi training and educational intervention along with their routine medical care. The control group received the routine medical care only. Routine medical care included physician prescribed medication and standard patient education without Tai chi training and educational intervention. Information about the study was distributed to outpatients through the OPD. The inclusion criteria were: Average BP>140 /90mmHg in the past 12 months, taking medication, no cardiovascular or kidney disease, no pregnancy or planned pregnancy during the duration of the study. Randomized allocation of participants was not possible for outpatients at the OPD; therefore, a non-randomized form of allocation was used. Outpatients recruited from Monday and Wednesday OPD visits were assigned to experimental group; outpatients recruited from Tuesday and Friday OPD visits were assigned to control group.
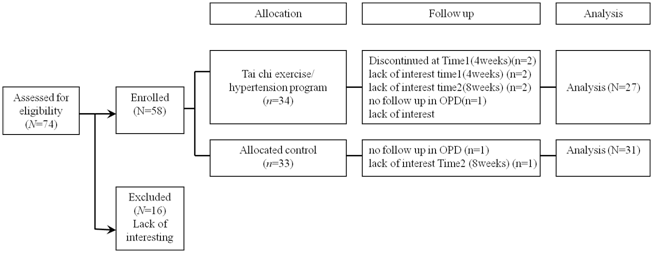
Figure 1: Flow diagram for participant Enrollment
Ethical considerations
Approval for the study was obtained from the Institutional Review Board of St. Mary’s hospital (No. SMH102231). Written informed consent was obtained from all participants who were assured of confidentiality and the ability to decline participation or withdraw from the study at any time. Permission to use the instruments were obtained from the respective copyright holders.
Hypothesis
Tai Chi training and educational intervention will be associated with a significant improvement in BP control, and be positively associated with self-care behavior, self-efficacy, and quality of life of hypertensive outpatient when compared to controls.
Procedure
All eligible recruits will provide written informed consent prior to enrolling in the study. The intervention portion of this study is based on the standardized protocol established and used in previous studies by the Lo et al [19]. There will be an initial baseline visit intervention training and material distribution. Experimental group will practice intervention for 60 minutes Tai Chi exercise three times a week for a 8 weeks period. All participants (both groups) will be seen for 6 visits (four teaching programs and two telephone-based counseling interventions). We developed an integrated health education program for hypertensive outpatient, named educational intervention. The educational intervention was based on social cognitive theory (CBT). To implement CBT effectively, teaching programs will be followed by 4 biweekly visits during the 8-week intervention with interpersonal interview to monitor compliance, correctness and satisfaction. Telephone-based counseling interventions will be followed by 2 monthly visits during the 8-week intervention to monitor lifestyle change.
Tai Chi training intervention
The intervention in this study was the 60 min Tai Chi exercise. The experimental group received a Tai Chi exercise in addition to their routine care, which involved treatment with medications and patient education. Thirty-one participants in the control group only received routine care without Tai Chi training. The experimental group received the 60 min Yang-style Tai Chi exercise in a group setting three times a week for 8 weeks. The exercise program included three phases: warm-up, the Tai Chi exercise session and cool-down. Specifically, a 15 min warm-up period followed by a 40 min Tai Chi exercise session and then a 5 min cool-down session. The Tai Chi exercise instructions were both verbal and visual. This approach is used worldwide by cer- tified instructors in the teaching of Tai Chi exercise. Trained instructor repeated the moves first then the patients did the exercise by following relaxing Chinese music with slow rhythm and tempo. Each move was repeated at least six times, and the participant performed the moves by following the instructor’s verbal cues and mimicking the instructor’s body and extremity movements.
Educational intervention (teaching program and counseling intervention)
Participants received a 40 min teaching program for four times at post 2nd, 4th ,6th and 8th week, as well as 20-minute telephone-based counseling intervention for two times at post 4th and 8th week by two researchers targeting participant-specific goals relating to lifestyle change. The goal of counseling, conducted by trained nurses, was to encourage the patients to maintain self-care behaviors, self-efficacy and to solve any current or potential problems the patient faced or with the educational intervention itself. Each intervention discussion reviewed medication, BP control, diet control, and exercise. Educational material was supplied, tailored to patients’ needs. This program made it possible to encourage active and positive participation of the patients while continuously modifying the program, according to the needs of the particular participants [7,20].
The major components (teaching and counseling) were selected through a comprehensive literature review. The needs of adults and facilitators as well as the barriers to participation were identified by needs assessments and formative evaluation. Participants completed the 8 week study, according to the specifications of their randomly assigned group (experimental or control), with the medical component of the study being conducted at an outpatient clinic when necessary. Researchers were instructed to review and record all the processes of care from their patient’s perspective and blood pressure. Where appropriate and depending on the patient’s condition, the observational data were supplemented with information derived from a conversation with the patient. Researchers collected data and described the educational interventiion after obtaining information derived from patient discussion with both the physician and researcher, as well as the researcher’s recordings of the details of each patient contact. Each patient gave informed and voluntary consent to participate in the study. Participants were asked not to reveal participation in the study to others until after study completion.
Outcome measures
Demographics
A brief questionnaire was used to collect the demographic variables which included sex, age, education, in- come, and hypertension history.
Self-Care Questionnaire
This instrument was developed by a previous study [14]. The scale is used to measure the social psychological health status of chronically ill patients. This is an 18-item questionnaire focusing on the self-care behavior of patients. Sample items include: ‘I weigh myself every day’ and ‘If my blood pressure increases, I contact my doctor or nurse.’ Responses on each item are measured on a 5-point Likert scale ranging from 1 (completely agree) to 5 (don’t agree at all). Thus, the total score can range from 8 to 40, with higher scores indicating better self-care Questionnaires used in this study were first translated into Mandarin and then back translated into English by independent bilingual translators. The reliability coefficient was 0.88-0.90 in this study.
Self-efficacy
This instrument was developed and motified by a previous study [21]. The scale is used to measure the self-efficacy of exercise. This is an 8-item questionnaire. Higher scores indicate greater self-efficacy. Questionnaires used in this study were first translated into Mandarin and then back translated into English by independent bilingual translators. The reliability coefficient was 0.88-0.90 in this study.
Quality of life (SF-36)
The Chinese version of the SF-36 Health Survey was used to assess the participants’ self-actualization of physical and mental health [22]. The SF-36 has two components and measures eight health concepts. In this study, participant pre-test scores were used and Cronbach’s alpha coefficients of 0.78 and 0.86 were found, respectively, for the physical and mental health components.
Blood Pressure (BP)
Systolic and diastolic BPs were measured at baseline, the 4th and 8th week time points. At these times, after interview completion, a manual sphygmomanometer (HEM-705IT, Omron Healthcare, Kyoto, Japan) was used to measure the participants’ resting systolic and diastolic blood pressures. A nurse obtained BP measurements using the same sphygomomanometer standardized for cuff size and position. The BP of each participant was measured using standardized protocol by the same nurse; meanwhile a BP value was derived from three measures to reduce possible measurement errors. The participants were instructed to take a rest before the BP reading and abstain from caffeine and physical activity.
Data analysis
The Statistical Package for the Social Sciences program (Windows12.0, SPSS Inc., Chicago, USA) was used to analysis the data. Descriptive statistics such as the mean and standard deviation were used to describe the characteristics of the participants from the demographic data gathered. Analysis of variance (ANOVA) with repeated measurements was used to determine the effects of different groups and the interaction of these two variables on the measurements. Analysis of variance independent t test was used to compare the differences between these two groups at the post-test with the pretest scores as covariates. The significance level was set at 0.05.
Results
Sample characteristics
In the Experimental group, the mean age was 58.29 ± 7.64 years old with 52% male. The majority (26%) had received college education. A hypertension history of 11-15 years was observed in 37% of experimental group participants. Similar characteristics were observed in the control group. Thus, there were no statistically significant differences between the experimental and the control groups’ characteristics (Table 1).
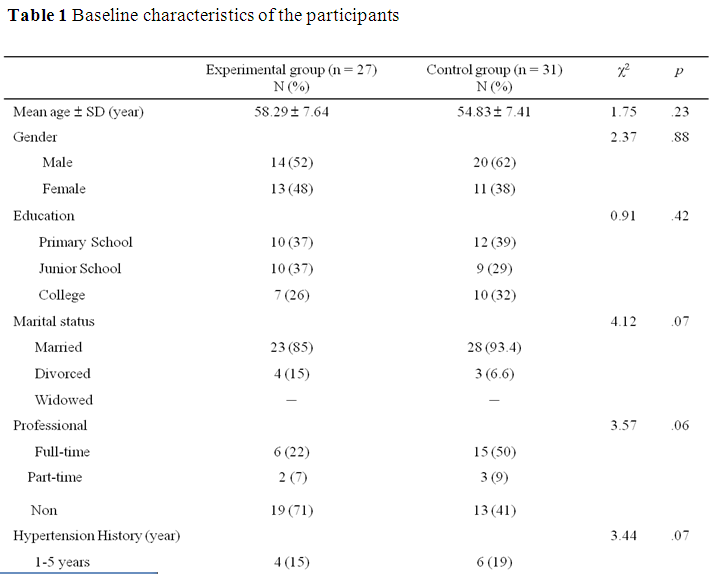
Table 1: Baseline characteristics of the participants
Self Care Behavior
The scores of the experimental group dramatically increased from a mean of 3.42 ± 0.41 at baseline to 4.11 ± 0.31 at week 8 of the combination intervention. Comparatively, the scores of the control group increased less dra- matically from a mean of 3.23 ± 0.58 at baseline to 3.75 ± 0.21 at 8th week. These findings indicate statistically significant differences between the experimental and control groups (t=1.44, p=0.01) at 8th week of intervention (Table 2).
Self-efficacy
The average self-efficacy scores of the experimental group increased from a mean of 3.12 ± 0.82 at baseline to 4.11 ± 0.66 at the 4th week and 4.21 ± 0.23 by the 8th week of intervention. The statistical points were con- siderable differences. However, the average self-efficacy scores of the control group gradually increased only marginally from a mean of 3.23 ± 0.79 at baseline to 3.33± 0.78 at the 4th week and 3.14 ± 0.44 at the 8th week after intervention. Differences between the experimental and the control group were statistically different (t=3. 44, p=0.03) (Table 2).
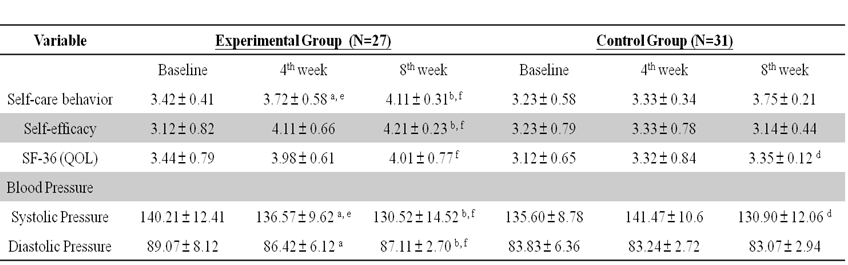
Table 2: Comparisons of mean differences between and two post-tests for self-care behavior, self efficacy and quality of life and blood pressure (N = 58)
Note. SF-36(QOL)= 36-Item Short Form Health Survey (quality of life); Data are expressed as means ± S.E.. aP < 0.05 versus the baseline in the experimental group. bP < 0.05 versus the 4th week in the experimental group. cP < 0.05 versus the baseline in the control group. dP < 0.05 versus the 4th week in the control group. eP < 0.05 versus control group in 4th week. f P < 0.05 versus control group in 8th week.
Quality of life
As shown in Table 2, the life quality of the experimental group was greatly improved by combination inter- vention. Average score quality of life was 3.44 ± 0.79 before the intervention, but by the 4th week the score had already climbed to 3.98 ±0.61 and by the 8th week average quality of life score had risen still further to 4.01 ± 0.77. Conversely, only slight changes in the life quality of the control group were observed. At baseline the average quality of life score of the control group was 3.12 ± 0.65, then 3.32 ± 0.84 at the 4th week and finally 3.35 ± 0.12 at the 8th week. The differences between the experimental group and the control group were statistically significant (t=1.11, p=0.02) (Table 2).
Blood pressure
After the 8 week combination intervention, a statistically significant difference between the experimental and control groups were observed for reduction in systolic pressure (t=2.57, p< 0.001) and diastolic pressure (t=2.86, p< 0.001) (Table 2).
Comparison of outcome variables after eight week intervention
Results of Repeat Measure ANOVA indicated no significant time effect between the three time points. There were significant improvements in self care behavior (F=6.28, P=0.000), self efficacy (F=6.28, P=0.002), and Quality of life (F=3.23, P=0.001) scores between the two groups over time (Table 3).

Table 3: Effects of Tai Chi training and educational intervention on self-care behavior, self efficacy and quality of life and blood pressure between groups (N=58)
Note. * p < .05. **p < .01.
Discussion
This study aimed to evaluate the effects of the Tai chi training and educational intervention on the blood pressure control, selfcare behavior and self-efficacy among hypertensive outpatients. The development of the Tai chi training and educational intervention was a multidisciplinary collaboration. The intervensions focus on patient lifestyle modification through a combination of health education and exercise implementation. The combination intervensions proved effective in controlling systolic BP and improving self-care behavior, self-efficacy and quality of life.
Current studies have shown that the majority of hypertensive patients are informed and have knowledge about both hypertension and the effect of a healthy lifestyle on controlling blood pressure. Most patients believed that their disease could be managed. However, the non-optimal results among hypertensive patients in Taiwan could stem from the fact that in addition to the great difficulty in lifestyle adjustment, only one-third to half of hypertensive patients reported receiving counseling from their physician on the necessity of correct diet and regular exercise in the treatment of blood pressure. We found many patients suffering from hypertension do not lead a healthy lifestyle. In fact, before accepting conbination intervention, only onethird of the respondents exercise every day and take hypertension medication on time. Our study first found that the 8 week Tai Chi training significantly reduced participants’ BPs. Tai Chi training is different from other types of exercises and might be more beneficial and effective in reducing the BP [23]. These findings suggest that patients’ lifestyle behaviors may contribute to their elevated blood pressure levels. The results of the present study indicate that implementing out- patient health intervention programs that include regular and comprehensive monitoring of patient compliance is an effective method of helping patients reach health goals.
Studies show Tai-Chi exercise involves autonomic activity, hormones, affect, sensory perception, motor control and cognition [24]. Research indicates Tai-chi has a wide range of health benefits. Our study indicated after Tai Chi training and educational intervention, decreased BP among hospital outpatients with hypertension positively correlated to improvements in measures of self efficacy and cognitive functioning. Interestingly, one area of increased blood flow associated with Tai Chi exercise was the anterior cingulate cortex (ACC) which is an area of interface for sensation, cognition, emotion as well as behavior and plays an important role in stress [25]. We also found that improved self efficacy increases the patients’ motivation about hypertension management, thus are positively correlated with self-care behavior and quality of life. Therefore, improved self efficacy with combination intervention is the central role to activate self-care behavior and improve quality of life.
Previous studies suggest that the knowledge imparted by medical staff is an important factor for inducing patients to comply with lifestyle recommendations [26]. The main finding of the multivariate analysis was that patients’ beliefs about hypertension management, patients’ knowledge about hypertension, counseling on a healthy lifestyle and self-care each have an independent effect on hypertensive patients’ reported compliance with the recommended lifestyle behaviors. The effect of beliefs and knowledge about hypertension and its management is concordant with the Self Care model relating attitudes to changes in lifestyle behaviors [27], as well as findings of former studies reporting that patient education about hypertension and lifestyle modification improved blood pressure control [20]. Our study indicated that participants’ self-care behavior, self-efficacy and quality of life had significantly improved after 8 weeks of Tai Chi training. Apparently, such patients can play a more active role in their treatment and therefore are more effective in controlling their condition. The significant improve- ment of the participants’ was congruent with the study results by Li et al. [28] and Brown et al. [29]. The special emphasis on exercise in interventions such as the Tai chi training has been shown to enhance cardiovascular function, improve health-related fitness and promote positive health status. The increase in time spent exercising by patients in the educational intervention is a novel and important secondary finding of this study.
The role of nurse counseling on the patient’s compliance with lifestyle changes is also concordant with previous studies [20]. One of the greatest challenges facing medical systems is finding effective strategies for convincing and helping patients with chronic disease, including those with hypertension to change their lifestyle and to play an active part in their treatment. The predominant theory is that there is a need to understand what motivates each patient and what affects his/her motivation and to convince him/her to make the change accord- ingly [30]. This can be achieved by organizing patientcentered workshops, to educate patients about hypertension and to enhance patients’ self-care behavior, self-efficacy, as well as quality of life to play an active role in their treatment. This study provides evidence that such workshops will result in empowering patients and making them partners in the management of their condition.
Limitations
This study has several limitations. First, the study was based on self-reporting by patients regarding their self-care behaviors. These may be inaccurate because of “social desirability” responses or recall difficulties. Nevertheless, patients are considered a reliable source of information on such topics. Furthermore, there is no alternative source of information available regarding patients’ behaviors and hypertension counseling as this is not recorded in the medical files. Second, as in previous studies on these topics [18], the study design prohibits conclusions about cause and effect, and therefore we refer only to an association between self-care behaviors and the independent variables in the multivariate regression model. In conclusion, our study showed that receiving counseling from a staff about a healthy lifestyle and self-care, being informed about hypertension and its management, and having positive beliefs with regard to managing this condition led to maintenance of self-care and self-efficacy.
The combination intervention in our study integrated the education of behavior modification (CBT) into the Tai chi training and educational intervention. The program also included individual counseling at the 4th week and 8th week to encourage the participants to maintain their self-care behaviors. All of these intervention were developed by a multidisciplinary team, which included nurses, physicians and exercise therapists. Another strength of this study was the application of program evaluation research methods. In our study, the educational intervention was developed by analysis of individual health problems and the needs of the patient as well as the staff who work at the OPD. The continuous use of both patient and medical staff feedback during the 8 week intervention in order to customize and optimize the Tai chi training and educational intervention according to the needs of the individual patient is one of this programs greatest strengths.
Conclusions
In conclusion, identifying an appropriate teaching program regimen targeted to promote and maintain health in hypertensive patients is needed. The study results substantiate the effectiveness of the Tai chi training and educational intervention. This type of intervention is classified as a teaching and consulting intervention and as such regulation and patient safety are of utmost importance. OPD staff are encouraged to take regular attendance and blood pressure of participants at the beginning of each session. From a safety perspective, it is important that patients who demonstrate signs or symptoms of physical discomfort during the research period should be stopped, at least until their discomfort has improved.
Relevance to clinical practice
Nursing staff can easily learn how to incorporate this form of educational intervention in OPD setting to meet the individual needs of patients with hypertension. The multifaceted Tai chi training and educational intervention provide an inexpensive and viable intervention which increases exercise behavior and blood pressure control in patients with hypertension. The results of this study provide evidence that participation in the combination in- terventions lead to decreases in blood pressure in patients suffering from hypertension. Healthcare professionals should be encouraged to understand this program before incorporating it into their clinical practice as an intervention for the appropriate patients.
Acknowledgements
We would like to thank the patients who participated in the project.
Competing Interests
The authors have declared that no competing interest exists.
Reference
Kearney, P.M., Whelton, M., Reynolds, K., & Whelton, P.K., He J (2004). Worldwide prevalence of hypertension: a systematic review. J Hypertens 22: 11–19.View
World Health Organization Expert Consultation (2004). Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 363: 157-163.View
Gillespie, C.D., & Hurvitz, K.A. (2013). Centers for Disease Control and Prevention (CDC). Prevalence of hypertension and controlled hypertension-United States, 2007-2010. MMWR Suppl 62: 144-148.View
Chiang, C.E., Wang, T.D., Ueng, K.C., Lin, T.H., & Yeh, H.I., et al. (2015). 2015 guidelines of the Taiwan Society of Cardiology and the Taiwan Hypertension Society for the management of hypertension. J Chin Med Assoc 78: 1-47.View
Rahman, A.R., Wang, J.G., Kwong, G.M., Morales, D.D., & Sritara, P., et al. (2015). all members of the Asian Cardiovascular Expert Forum Committee. Perception of hypertension management by patients and doctors in Asia: potential to improve blood pressure control. Asia Pac Fam Med 14: 2.View
Ritz, E. (2007). Total cardiovascular risk management. Am J Cardiol 100: 53J-60J.View
Glasson, J., Chang, E., Chenoweth, L., Hancock, K., Hall, T., & Hill- Murray, F., et al. (2009). Evaluation of a model of nursing care for older patients using participatory action research in an acute medical ward. J Clin Nurs 15:588-598.
Chobanian, A.V., Bakris, G.L., Black, H.R., Cushman, W.C., & Green, L.A., et al. (2003). The seventh report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. JAMA 289: 2560-2572.View
Wong, S.S., & Nahin, R.L. (2003). National center for complementary and alternative medicine perspectives for complementary and alternative medicine research in cardiovascular diseases. Cardiol Rev 11: 94–98.View
Pinto, A., Di Raimondo, D., Tuttolomondo, A., Fernandez, P., & Arnao, V., et al. (2006). Twenty four hour ambulatory blood pressure monitoring to evaluate effects on blood pressure of physical activity in hypertensive patients. Clin J Sport Med 16: 238–243.View
Braden, C.J. (1990). A test of Braden self-help model: learned response to chronic illness experience. Nurs Res 39: 42-47.View
Friedberg, J.P., Rodriguez, M.A., Watsula, M.E., Lin, I., & Wylie-Rosett, J., et al. (2015). Effectiveness of a tailored behavioral intervention to improve hypertension control: primary outcomes of a randomized controlled trial. Hypertension 65: 440-446.View
Baynouna, L.M., Neglekerke, N.J., Ali, H.E., ZeinAlDeen, S.M., & Al Ameri, T.A. (2014). Audit of healthy lifestyle behaviors among patients with diabetes and hypertension attending ambulatory health care services in the United Arab Emirates. Glob Health Promot 21: 44-51.View
Wang, Y.T., Taylor, L., Pearl, M., & Chang, L.S. (2004). Effects of Tai Chi exercise on physical and mental health of college students. Am J Chin Med 32: 453–459.View
Caldwell, K., Emery, L., Harrison, M., & Greeson, J.(2011). Changes in mindfulness, well-being, and sleep quality in college students through taijiquan courses: a cohort control study. J Altern Complement Med 17: 931–938.View
van Straten, A., Cuijpers, P., & Smits, N. (2008). Effectiveness of a web-based self-help intervention for symptoms of depression, anxiety, and stress: randomized controlled trial. J Med Internet Res 10: e7.View
Kim, S.H., & Youn, C.H. (2015). Efficacy of chronic disease selfmanagement program in older Korean adults with low and high health literacy. Asian Nurs Res (Korean Soc Nurs Sci). 9: 42-46.View
Hofmann, S.G., Asnaani, A., Vonk, I.J., Sawyer, A.T., & Fang, A. (2012). The efficacy of cognitive behavioral therapy: A review of metaanalyses. Cognit Ther Res 36: 427- 440.View
Lo, H.M., Yeh, C.Y., Chang, S.C., Sung, H.C., & Smith, G.D. (2012). A Tai Chi exercise programme improved exercise behaviour and reduced blood pressure in outpatients with hypertension. Int J Nurs Pract 18: 545-551.View
Fernandez, S., Scales, K.L., Pineiro, J.M., Schoenthaler, A.M., & Ogedegbe, G. (2008). A seniorcenter-based pilot trial of the effect of lifestyle intervention on blood pressure in minority elderly people with hypertension. J Am Geriatr Soc 56: 1860-1866.View
Lapier, T.K., Cleary, K., & Kidd, J. (2009). Exercise self-efficacy, habitual physical activity, and fear of falling in patients with coronary heart disease. Cardiopulm Phys Ther J 20: 5-11.View
Brodie, D.A., Inoue, A., & Shaw, D.G. (2008). Motivational interviewing to change quality of life for people with chronic heart failure: a randomised controlled trial. Int J Nurs Stud 45: 489-500..View
Lai, J.S., Lan, C., Wong, M.K., & Teng, S.H.(1995). Two-year trends in cardiorespiratory function among older Tai Chi Chuan practitioners and sedentary participants. J Am Geriatr Soc 43: 1222-1227.View
Hogan, M. (2005). Physical and cognitive activity and exercise for older adults: a review. Int J Aging Hum Dev 60: 95-126.View
Coubard, O.A., Duretz, S., Lefebvre, V., Lapalus, P., & Ferrufino, L. (2011). Practice of Contemporary Dance Improves Cognitive Flexibility in Aging. Front Aging Neurosci 3:13.View
Dolor, R.J., Yancy Jr, W.S., Owen, W.F., Matchar, D.B., & Samsa, G.P., et al. (2009). Hypertension improvement project (HIP): study protocol and implementation challenges. Trials 10: 13.View
Bellg, A.J. (2003). Maintenance of health behavior change in preventive cardiology. Internalization and self-regulation of new behaviors. Behav Modif 27: 103-131.View
Li, F., Duncan, T.E., Duncan, S.C., Susan, C., McAuley, E., & Chaumeton, N.R., et al. (2001). Enhancing the psychological well-being of elderly individuals through Tai Chi exercise: a latent growth curve analysis. Struct equ modeling 8: 53- 83.View
Brown, D.R., Wang, Y., Ward, A., Ebbeling, C.B., Fortlage, L., & Puleo, E., et al. (1995). Chronic psychological effects of exercise and exercise plus cognitive strategies. Med Sci Sports Exerc. 27: 765-775.View
Lahdenperä, T.S., & Kyngäs, H.A. (2001). Levels of compliance shown by hypertensive patients and their attitude toward their illness. J Adv Nurs 34: 189-195.View