
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care Volume 3 (2018), Article ID 1: JCNRC-122
https://doi.org/10.33790/jcnrc1100122Research Article
Self-Control Trial: A Qualitative Grounded Theory Study on the Decision Making Process in Patients with Ulcerative Colitis Who Choose to Use Complementary and Alternative Medicine
Maya Nunotani
Graduate School of Nursing, School of Nursing, Mukogawa Women’s University, 6-46 Ikebiraki-cho, Nishinomiya-city, Hyogo, 663- 8558, Japan
Corresponding Author Details: Maya Nunotani, Department of Nursing, Mukogawa Women’s University, 6-46 Ikebiraki-cho, Nishinomiya-city, Hyogo, 663-8558, Japan. E-mail: nunotani@mukogawa-u.ac.jp
Received date: 16th September, 2017
Accepted date: 08th January, 2018
Published: 15th February, 2018
Citation: Nunotani M (2018) Self-Control Trial: A Qualitative Grounded Theory Study on the Decision-Making Process in Patients with Ulcerative Colitis Who Choose to Use Complementary and Alternative Medicine. J Comp Nurs Res Care 3: 122.
Copyright: ©2018, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Purpose: This study aimed to explore the decision-making process in patients with ulcerative colitis who were interested in and chose to use complementary and alternative medicine.
Methods: This descriptive study used a grounded theory approach to study the decision-making process in patients with ulcerative colitis, including semi-structured interviews and constant comparative analysis. The study subjects were recruited from a self-help group for patients in Japan. A total of 14 adult patients with ulcerative colitis that was in remission participated in this study.
Results: In this grounded theory study of patients with ulcerative colitis who choose to use complementary and alternative medicine, a core category was identified, i.e., “self-control trial,” along with five other categories included in the patients’ decision-making process: “health condition,” “feasibility,” “influenced by others,” “desire to restore my health,” and “distrust.” Patients whose health condition was not improved by their current treatment were interested in complementary and alternative medicine. While being influenced by others and examining the feasibility of complementary and alternative medicine, these patients weighed their desire to restore health with their distrust. When their desire to restore health outweighed their distrust, patients chose to use complementary and alternative medicine
Conclusions: This study provides an insight into patients’ decision-making processes about their choice of complementary and alternative medicine. Such insights might help nurses to better understand and respect patient choice. The findings may also be useful in the development of support programs addressing concerns about the choice of complementary and alternative medicine by patients with ulcerative colitis.
Keywords: Complementary and alternative medicine, Decision making, Grounded theory, Ulcerative colitis
Abbreviations: CAM, Complementary and alternative medicine; TNF, Tumor necrosis factor; UC, Ulcerative colitis.
Introduction
Ulcerative colitis (UC) is an inflammatory bowel disease that causes ulcers in the mucous membrane of the large intestine. Its characteristic symptoms are diarrhea, viscous blood in stool, and abdominal pain. Complications may develop out of the intestinal tract,such as joint pain or iritis. The prevalence of UC in the Japanese population is 134.4 per 100,000, which is approximately half that of the prevalence in European and American populations [1]. However, the number of Japanese patients with UC is increasing annually; approximately 170,000 people contracted the disease in 2015 [2].
UC is considered an autoimmune disease. On the one hand, treatment with anti-tumor necrosis factor (TNF) agents or an immunomodulator is often provided to control inflammation caused by an abnormal immunoreaction in the intestinal tract. On the other hand, these medications have the problems of severe side effects or loss of response. A Japanese study reported that approximately 70% of patients with UC using an anti-TNF agent went into remission after 12 weeks, but 40% of them showed relapse or loss of response within 1 year [3]. Therefore, it is difficult to suppress the disease completely even if these medications are used. In recent years, patients with UC have become increasingly interested in complementary and alternative medicine (CAM). Nearly half of patients with UC in Europe and America are reported to use some type of CAM, such as acupuncture, vitamin compounds, probiotics, and herbs [4,6].
The Japanese Society for Complementary and Alternative Medicine defines CAM as a generic term for medicine produced by a traditional or complementary medical system using materials that have not undergone scientific inspection or application in the modern Western medicine and clinical system [7]. Unlike medications prescribed by a doctor in a medical institution, whether CAM is used depends on individual patients’decision-making processes. Therefore, the choice to use CAM may change due to individual patients’ perceptions or thoughts about CAM. Although patients with UC widely use CAM, few studies have explored how patients decide whether to use CAM.
Purpose:
This study aimed to explore the decision-making processes used by patients with UC on deciding to choose and use CAM.
Methods
Design
A grounded theory approach was used in this qualitative study design to enable the description and exploration of the basic social processes leading to the decision to use CAM. Grounded theory is a research method used to discover new dimensions of social processes at play in people’s lives [9]..
Participants
The subjects in this study were patients aged over 18 years old with UC in remission who lived at home and could participate in an interview investigation. To avoid bias by selecting patients treated by a physician in the specific medical institution, the study participants were recruited from a self-help group for patients with inflam- matory bowel disease based in the Kansai region of Japan.
Data Collection
All semi-structured interviews were conducted by the author, who was trained and experienced in conducting such interviews, and had no prior relationship with the participants. The interview guide included the following topics: user’s experience of CAM, thoughts about CAM, reason for choosing or not choosing CAM, health condition,and life before and after choosing CAM. The interviews started with open-ended questions regarding the participants’ experiences with CAM, followed by more detailed and probing questions depending on their responses. The interviews lasted 27 min to 63 min (median time of 39 min). All interviews were audiorecorded and transcribed verbatim.
Analysis
The grounded theory approach was used in a constant comparative analysis, where every piece of data was compared with other pieces of data [10].. The analysis was performed using the following procedure:1) Data for individual participants were produced using a phrase or paragraph unit chosen depending on the meaning of the key word, transcribed verbatim, and then summarized. 2) Each summarized piece of data was interpreted and conceptualized based on the question:how do patients with UC decide to choose and use CAM. 3) Each interpreted piece of data was abstracted into its category and subcategory compared with other interpreted pieces of data from the participant, in addition to interpreted pieces of data obtained from other participants. 4) The relationship between categories was examined using a timeline to explore the progress of processes in the decision-making process. If a category played a key role in the progress of the process, it was identified as a core category. After the analysis of 14 participants,saturation was considered to have been reached because no new findings or categories emerged and a unified figure that could sufficiently explain the relationship between categories was completed. To confirm the validity of the analysis, an expert, who was familiar with qualitative study and nursing chronic illnesses, supervised all aspects of the data collection and analysis. In addition, confirmation from participants was obtained about whether the identified categories and subcategories captured their intended meaning correctly.
Ethical Considerations
After the chairperson of a self-help group consented to cooperate in this study, a document was sent to all group members inviting them to participate in the study. In response to members who agreed to participate, the researcher explained that they could leave the study at any time, that their anonymity would be maintained, the method of data management, the purpose of the study, and the data collection method (oral and written). All participants signed their written consent after being fully informed of the nature of the study. In addition, all participants were informed verbally and in writing that they could go to the restroom during the interviews and report to the researcher at any time when they felt uncomfortable. The research proposal was approved by the ethics committee of Tenri Health Care University.
Results
A total of 14 participants were interviewed. Nine were male. The mean age was 53 years (range,40–68 years). The mean period after the UC diagnosis was 11 years (range, 1–31 years). All participants had used some type of CAM after the diagnosis. Ten participants had used CAM at the time of the interview. Participants used the following types of CAM: diet therapy (i.e., limited fatty or fibrous food and restricted use of stimulants like alcohol or coffee); supplements, including vitamins and probiotics;fitness-related exercise, such as swimming, Qigong, or Tai Chi; or traditional Chinese medicine.
The following sections outline the interview findings, which begin with an overview of the core category,- self-control trial, and a description of the process leading to the construction of the core category, as illustrated in Figure 1.
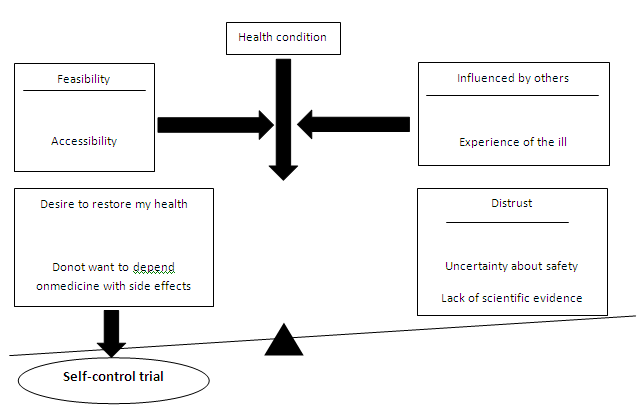
Figure 1: Decision-making process in patients with ulcerative colitis who choose to use complement ary and alternative medicine
Self-control Trial
This category reflected participants’ desire to manage their disease by choosing to use a CAM because they felt that they were not receiving enough benefit from only the treatment regimen provided by their doctor. Prior to making this decision, participants actively assessed and weighed the benefits and risks for using CAM.
I want to keep my health balanced by some means or other if I can achieve balance by myself. (Participant C)
Health Condition
This category reflected participants’ awareness of his/her own health condition based on their UC symptoms. Participants who felt wellconditioned did not feel the need to use CAM. However,participants who still felt unwell even following medical treatment from their doctor came to doubt its efficacy and became interested in CAM. This category was a starting point for participants’ decision-making process in deciding to use CAM.
Because I am well-conditioned after changing my medication, I do not need to use it [CAM] in particular. I do not search for CAM anymore because my health condition is good. (Participant I)
Symptoms resumed after a month when I stopped taking a steroid. So, I will try it[CAM]to be self-responsible. (Participant J)
Feasibility
This category reflected the participants’ examination of whether CAM was practically obtainable. Three subcategories support this category:accessibility, cost, and time.
Accessibilit
This category describes participants’ geographical access issues, such as whether they could visit the specific facilities regularly to maintain their continual use of CAM. Participants who experienced difficulties accessing these facilities stopped using CAM.
In the self-help group, someone talked about traditional Chinese medicine from Hiroshima. I am interested in it, but I cannot go there. (Participant J)
Cost
This category expressed participants’ economic issues in paying for a constant use of a specific CAM.Participants hesitated to use CAM if they judged that the burden of the expense outweighed the actual effect.
All of the components [of CAM]are expensive. Thus, it is hard to continue CAM therapy when it costs 3,000, 5,000, or 10,000 yen per month if it does not readily show some effect. (Participant N)
Time
This category expressed participants’ issue in finding time to use a specific CAM continuously.Working partic- ipants in particular struggled to find the time to engage in CAM.
After I retire and if I have time, I intend to work on exercise. (Participant B)
Influenced by Others
This category showed that other people influenced participants into using or ceasing their use of CAM. This factor also included participants who considered or avoided CAM use because they wanted to maintain their relationship with others. Two subcategories support this category: experience of the ill and the health-care professionals’ opinion.
Experience of the ill
This category reflected participants who were inspired by the experiences of the ill whose health condition improved after using a specific CAM.
In the self-help group, a middle-age woman talked about how she felt that “I should make my body better by myself! I began yoga and improved my health very much.”Because of her influence, I also started practicing yoga 2 years ago. (Participant B).
Health-care professionals’ opinion
This category captured the health-care professionals’ perceptions or thoughts about the use of specific CAM. Recommendations from a reliable professional became the guarantee of safety and evidence about the CAM. However, professionals’ negative attitudes to CAM promoted participants’ distrust of CAM. In addition, some participants continued using CAM and hid their use from their health-care professionals because they had recommended not using it or refused to provide it to them When I said, “I take both Pentasa and traditional Chinese medicine,” a doctor and a nurse scolded me badly. So, I now take traditional Chinese medicine without disclosing it to them. (Participant J).
Desire to Restore My Health
This category reflected participants’ desire or need to cope with their ill-health and improve or maintain their health. Two subcategories support this category: do not want to depend on medicine with side effects and want to make the whole body better.
Do not want to depend on medicine with side effects
This category reflected participants’ need to avoid depending on only medication in their treatment. Although the medication recommended by a doctor could have its expected effects, it also included side effects. Partic- ipants considered steroids, anti-TNF agents, or an immuno modulator as “strong medicine.”However, partici- pants demanded a treatment that “was kind to my body,”with fewer side effects. As participants had experienced the side effects of medication in the past, their statement of this need was clear.
I came to think that I did not want to depend on medicine even more after experiencing the side effects of Imuran. I had thought it would be cured if I took medicine. I did not expect that the side effects of the medicine would be so hard to experience. Other medicines probably have similar side effects, more or less. (Participant C)
Want to make the whole body better
This category reflected participants’ need to improve their whole body, including not only their gastrointestinal symptoms, but also the treatment of complications. Participants were dissatisfied with having to be referred to specialist doctors under their hospital’s system, which was compartmentalized into specialized fields, instead of being treated holistically by a single doctor.
Gastroenterologists divide the work. They examine only a single digestive organ. If it isOK as a digestive organ, it is OK. Even if I say, “I have some complications other than the gastrointestinal symptoms,” they say, “please contact the orthopedics department about it.”We want the doctors to see us holistically because various complications manifest in one body. However, none of the doctors understand the whole. (Participant B).
Distrust
This category reflected participants’ attitude or perception of distrust of CAM because of uncertainty about its safety and vague scientific evidence. Participants who had strong distrust avoided using CAM. Two subcatego- ries support this category: uncertainty about safety and lack of scientific evidence.
Uncertainty about safety
This category reflected participants’ uncertainty about the safety of CAM that led to uneasiness that their health conditions were deteriorating while using CAM because its safety was insufficiently guaranteed. Participants who had this strong uneasiness hesitated to use CAM.
For example, herbs, traditional Chinese medicine, acupuncture, and moxibustion…. I am worried that some adverse effects may impact my healthwhen I use them. I am concerned about their safety. (Participant G)
Lack of scientific evidence
This category reflected participants’ feeling that there was no point in using CAM because the scientific evidence about their therapeutic effect was unclear. An individual participant had different criteria for scientific evidence:
I believe that the treatment included in the guidelines by Ministry of Health, Labour and Welfare is reliable because it shows the effective rate of treatment to some extent. Therefore, as for me, that will be enough and I think that there is no point in even trying additional treatments. (Participant L)
Discussion
The grounded theory approach used in this study identified a core category,“self-control trial.”Participants evaluated their “health condition” and compared their “desire to restore health” with their “distrust” of CAM while examining the “feasibility” of CAM and being “influenced by others.” As a result, participants tried a CAM when their desire to restore health outweighed their distrust of CAM. A Canadian national survey [11]. also showed that the most common reason given for using CAM was,“I wanted greater control over my life and my inflammatory bowel disease.”
Clutching at straws, cancer patients hopefully use CAM in an expectation of an effect controlling the cancer progression [12].. Radical cure of either UC or cancer is difficult and the risk of recurrence is always common. However, UC appears most commonly in youth in their twenties and the life prognosis of patients with UC is equal to a physically unimpaired person [13]. Therefore, it is thought that patients with UC experience less of a sense of crisis based on a fear of death compared with that in cancer patients when they choose CAM.However, patients with UC have a longer period of living with disease than cancer patients. Therefore,cancer patients are considered to entrust CAM with their hope to live and use CAM to suppress the cancer progression, while patients with UC choose to use CAM as a realistic means of self-control over their disease and future life. In other words, participants’ trial periods of self-control indicate their active intention to grasp the initiative over their disease and adjust their lives instead of being frightened by the uncertainty of disease recurrence.
Two subcategories supported participants’desire to restore their health: do not want to depend on medicine with side effects and want to make the whole body better.Hawthorne [14]. suggests that patients often want to control their illness by choosing what to take rather than submitting to their doctors’ decision and there is a common desire for natural therapies over chemicals.
Not wanting to depend on medicine with side effects indicates that participants perceived CAM as a gentler and safer therapy compared with the medication prescribed by doctors. Koitabashi [15]. points out the reasons why CAM is attractive to patients; i.e.,in modern medicine, a highly medical technology was developed based on the dependence on cure technology to “attack”the cause of disease, which often overlooked the patient’s original healing and restoration powers.CAM is attractive because of its principle that the care technology, i.e.,to “protect”is as important as the cure technology. In recent years, the development and application for UC cures have advanced, and current treatments consider symptom improvement and mucous membrane healing as the treatment aim. Therefore, a strong cure technology is frequently used, such as anti-TNF agents or an immuno- modulator. However, patients taking these medications are at risk of experiencing serious side effects, such as sepsis or malignant tumor [16].. On the one hand, patients expect such a technique to “attack” positively, but on the other hand, they need a technique to “protect” their body from the risk of side effects with the attacking technique in CAM.
Wanting to make the whole body better indicates that participants need holistic therapy, as shown in a previ- ous study [17].. This need came from the dissatisfaction with having to be referred to specialist doctors under their hospital’s compartmentalized system into specialized fields instead of being treated holistically by a single doctor. These patients regard CAM as a means of realizing comprehensive holistic therapy,including not only the treatment of the lesion in the large intestine, but also the treatment of complications and coping with psycho- logical stress.
Decision making in medical care is said to be a dynamic process that may change because of patients’ preferenc- es or intentions about their treatment or external influences [18].. The decision-making by patients with UC on the choice of CAM was another dynamic process that changed based on their health condition, influence by others, and the feasibility of CAM. The nurse should provide support depending on the situation of the individual patient in such a changeable process. Nurses need to understand that patients with health conditions that at first do not improve or worsen under the current treatment may be highly concerned about CAM and they should provide an environment where such patients can easily consult with them about CAM. Nurses should also become conscious that their thoughts and attitudes toward CAM will influence patients, as the result of this study shows. Nurses should not prevent their patients from using CAM, but understand that patients intend to use CAM and enable a safe environment for talking about CAM openly with their patients. As patients had used diet therapies, supplements, probiotics, among other types of CAM, it is necessary for them to consult and cooperate with doctors, pharmacists, and dieticians about their use of CAM parallel to their current medical treatment.
Although systematic reviews about the effectiveness of CAM on inflammatory bowel disease have been published [19,20]. there is still insufficient confirmation of their safety and risk based on scientific evidence for the combination of medical treatment with CAM. Nurses need to collect the latest knowledge about CAM and provide their patients with best-practice evidence. In addition, it is necessary for nurses to talk with other healthcare professionals about how to cope with patients’ requests for CAM where its safety and risk have not yet been confirmed.
Limitations
All participants in this study were members of a self-help group who had the opportunity to be influenced by other patients with the same disease, which may affect the results. Further studies should include additional participants, including patients who did not enroll in such a self-help group,to continue this investigation and analysis, and refine the decision-making model.
Conclusions
A qualitative grounded theory study was performed to explore the decision-making process in patients with UC on choosing CAM. As a result, the core category,“self-control trial” was identified. The starting point of the patients’ decision-making process was their evaluation of their health condition. Influenced by others while examining the feasibility of CAM, the patients compared their desire for restoring health with their distrust of CAM. When their desire for restoring health outweighed their distrust, the patientstried to choose and use CAM.
Acknowledgements
The author extends her gratitude to all the participants in this study. This study was supported by JSPS KAKENHI Grant Number 15K20722.
Conflict of Interest:
The author declares no conflict of interest with this paper.
Author Contributions:
NM was involved in all the process of this study from research concept and study design, data acquisition and analysis, to drafting and final approval of the manuscript.
Reference
Oh fuji S (2017) Epidemiology of inflammatory bowel disease in Japan and other countries. Extra issue; Igakunoayumi Current status of inflammatory bowel disease. (1stedn): 5-9, Ishiyaku Publishers, Tokyo.
Japan Intractable Diseases Information Center. The number of specific medical expenses (specific intractable disease) recipient owners authorized at the end of 2015.
Nakamura S, Miyasaki T, Hida N, Iimuro M (2015) Treatment effect of anti-TNF agent for ulcerative colitis. Mebio 32: 4-11.
Mountifield R, Andrews JM, Mikocka-Walus A, Bampton P (2015) Doctor communication quality and friends’ attitudes influence complementary medicine use in inflammatory bowel disease. World J Gastroenterol 21: 3663-3670.View
Sirois FM (2014) Health-related self-perceptions over time and provider-based Complementary and Alternative Medicine (CAM) use in people with inflammatory bowel disease or arthritis. Complemen Thera Med 22: 701-709.View
Koning M, Ailabouni R, Gearry RB, Frampton C, Barclay ML (2013) Use and predictors of oral complementary and alternative medicine by patients with inflammatory bowel disease: a population-based, case-control study. Inflamm Bowel Dis 19: 767-778. View
The Japanese Society for Complementary and Alternative Medicine. What is complementary and alternative medicine?
Nunotani M, Suzuki S (2016) Decision-making process about biologic therapy by patients with inflammatory bowel disease. Journal of Japan Academic of Nursing Science 36: 122-129.
Streubert HJ, Carpenter DR (2010) Qualitative research in nursing; advancing the humanistic imperative. (5th edn), 123- 139, Lippincott Williams & Wilkins, Philadelphia, Baltimore, New York, London, Buenos Aires, Hong Kong, Sydney, Tokyo. View
Suddaby R (2006) Fromthe editors: what grounded theory is not. Acad Manage J 49: 633-642. View
Li FX, Verhoef MJ, Best A, Otley A, Hilsden RJ (2005) Why patients with inflammatory bowel disease use or do not use complementary and alternative medicine: A Canadian national survey. Can J Gastroenterol 19: 567-753.View
Narui H, Homma T, Miura H, Izawa M, Suita Y, et al. (2006) Survey on cancer patients who adopt alternative therapies. J Aomori Univ Health Welf 7: 213-222.
Katoh H, Iwane S, Munakata A, Nakaji S, Sugawara K. (2000) Long-term prognosis of patients with ulcerative colitis in Japan. J Epidemol 10: 48-54.View
Hawthorne AB (2010) Complementary and alternative therapies in Crohn’s disease and ulcerative colitis. Gastrointestinal Nursing 8: 32-37. View
Koitabashi K (2006) Positioning and problem of the nursing therapy in complementary and alternative medicine. Kango Kenkyu 39: 449-456.
Crohn’s and Colitis Foundation of Japan (2016) Medical treatment guide of ulcerative colitis. (3rdedn), 46-53, Bunkodo, Tokyo.
Langhorst J, Anthonisen IB, Steder-Neukamm U, Luedtke R, Spahn G et al. (2007) Patterns of complementary and alternative medicine (CAM) use in patients with inflammatory bowel disease: perceived stress is a potential indicator for CAM use. Complementary Therapies in Medicine 15: 30-37. View
Groopman J, Hartzband P (2011)Your medical mind: How to decide what is right for you. Translated by Horiuchi S (2013) Kimerarenai Kanjatachi, 290-300, Igaku-Syoin, Tokyo.
Langhorst J, Wulfert H, Lauche R, Klose P, Cramer H, et al. (2015) Systematic review of complementary and alternative medicine treatments in inflammatory bowel diseases. J Crohns Colitis 9: 86-106. View
Quezada SM, Briscoe J, Cross RK (2016) Complementary and Alternative Medicine. Inflamm Bowel Dis 22: 1523- 1530.