
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care Volume 3 (2018), Article ID: JCNRC-128
https://doi.org/10.33790/jcnrc1100128Research Article
Nurses’ Perception of Caring Using a Relationship-Based Care Model
Annette Peacock-Johnson
Department of Nursing, Science Havican Hall Saint Mary’s College, Notre Dame, IN 46556, United States of America
Corresponding Author Details: Annette Peacock-Johnson, Department of Nursing Science, Havican Hall Saint Mary’s College, Notre Dame, IN 46556, United States of America. E-mail: ajohnson@saintmarys.edu
Received date: 18th June, 2018
Accepted date: 27th August, 2018
Published date: 01st September, 2018
Citation: Peacock-Johnson A (2018) Nurses’ Perception of Caring Using a Relationship-Based Care Model. J Comp Nurs Res Care 3: 128.
Copyright: ©2018, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Aim: Studies are lacking which examine nurses’ perception of caring when using a relationship-based care (RBC) model. This study examines nurses’ perception of caring using the Caring Assessment for Care Givers instrument (CACG).
Methods: A cross-sectional, descriptive design was used to study responses of medical-surgical nurses who work primarily providing direct patient care in a 267 bed United States hospital. A demographic questionnaire was administered along with the Caring Assessment for Care Givers (CACG) instrument.
Results: The average respondent was female, held a Bachelor’s of Science Degree, and had 7.9 years of nurse employment experience. Results revealed an overall high perception of caring for the sample population with a mean total score of 107.14 (range of 25-125) using the CACG instrument. Of the five CACG subscales, the subscale for the caring process of ‘doing for’ had the highest overall composite score of 21.68 (range 5-25) while the subscale for the caring process of ‘knowing’ had the lowest overall composite score of 21.10 (5- 25 range). Further analyses found a small to moderate, positive relationship between the overall nurses’ perception of caring score and the number of years of experience in nursing (r = .29, p<.01) with high perceptions of caring reported by nurses with more experience. Using a Spearman Rho, no relationship was found between the nurses’ perceptions of caring and the highest level of nursing education (rs = -.02).
Conclusions: This study expands what is known about RBC and discusses implications for nursing practice and leadership. While nurses report an overall high perception of caring, lower mean scores on the subscales of ‘knowing’ and ‘being with’ suggest that there is still room for improvement. Further research is needed to examine more fully the meaning of these caring behaviors for nurses to support and cultivate these interpersonal, relationship-based skills..
Keywords: relationship-based care, relationship-centered care, caring, nursing, and research
Abbreviations: RBC – Relationship-Based Care CACG – Caregiver Assessment for Care Givers CBI – Caring Behavior Inventory
Introduction
Throughout its history caring has been a central tenet to the practice of nursing. Nurse caring has been positively linked with increased patient outcomes, patient satisfaction, and nurse satisfaction [1-3]. It is believed that caring facilitates patients’ health, safety, and wellbeing [1,4-7] in addition to promoting healing, comfort, dignity, and security [6-9]. Through acts of caring nurses develop professional identify and often cite caring as a reason for becoming a nurse [10]. Conversely, the absence of caring can increase patients’ perceptions of isolation, despair, helplessness or vulnerability [9]. When nurses are prevented from caring or not recognized for caring, professional identity and job satisfaction are diminished [10]..
Despite the significance of caring, multiple factors today threaten the ability of nurses to engage in caring and compassionate roles. The evolution of nursing science and emphasis on evidence-based practice have contributed to a shift from holistic care to a more technically oriented practice contributing to an erosion in the ethos of compassion [11]. Socioeconomic factors may play a role by students who enter the profession for non-altruistic reasons including salary and job security [11]. This trend is coupled with an underlying organizational culture and fast-paced unpredictable work environment which challenge the ability of the nurse to engage in caring relationships [11-13].
In a study with oncology patients, Sheldon, Barrett, and Ellington [13] found that time constraints and difficult situations such as changing patient conditions or demanding circumstances hindered thoughtful, therapeutic responses. Tay, Hegney, and Ang [14] suggested that nurses in oncology may be unprepared or unwilling to handle emotions associated with life-challenging conditions. Inadequate staffing levels and the increased use of non-licensed assistive personnel to provide basic hands-on care also decrease caring opportunities for nurses to engage in therapeutic relationships with patients and families [10]. The heavy overall demands of care giving contribute to physical and emotional exhaustion for the nurse. Emotional exhaustion increases professional stress and burnout [11] which are negatively linked with nurse caring [15]. Given the challenges but significance of caring, the purpose of the study is to examine what is known about nurses’ perceptions of caring using a Relationship-Base Care (RBC) Model.
Relationship-Based Care
A model on Relationship-Based Care (RBC) was developed as a method for transforming the health care environment to facilitate patient-centered, relationship-based care [5]. At the center of relationship-based care is the concept of caring. Based on the Theory of Human Caring by Watson [7] and the middle range Theory of Caring by Swanson [6], the model includes dimensions of leadership, teamwork, professional practice, care delivery, resources, and outcomes [5].
Important to the model is a focus on relationships including the relationship to self, the relationship to other health care providers, and the relationship with patients and families. Of essence is the establishment of a therapeutic nurse-patient relationship that fosters dignity along with patient values and preferences [5]. Nurse-patient relationship-based care employs the use of presence, therapeutic listening, and a priority on the identification and implementation of therapeutic interventions to meet patient and family needs, creating an environment which facilitates healing and promotes caring [5].
Literature on RBC has described the influence of the model on patients including patient satisfaction and patients’ perceptions of caring [2,3,16]. While more is known regarding the influence of a RBC model on patients, less is known about the influence on nurses’ perceptions of caring. It is important to study nurses’ perceptions of caring when using a RBC model given the importance of caring and the obstacles which inhibit nurses from forming caring relationships.
Conceptual Framework
The Theory of Human Caring by Watson [7] and more specifically the mid-range Theory of Caring by Swanson [6] provide a conceptual framework for the proposed study on caring using a relationshipbased care model. In her Theory of Caring, Swanson [17]proposes that caring consists of the five processes of knowing, being with, doing for, enabling, and maintaining belief. The process of knowing involves understanding the experience of others while avoiding assumptions. The process of being with includes being emotionally present, sharing in the range of emotions experienced by the recipient. The provider demonstrates the ability of doing for when the provider does for the recipient what he or she would do independently given the knowledge, time, skill, or capacity. Enabling supports the recipient’s ability to manage when supported, validated, and informed. The process of maintaining belief provides hope that the recipient will get through an event or transition, finding meaning or purpose while maintaining hope for the future. As a result of these five processes, the recipient feels “understood, valued, safe and comforted, capable, and hopeful for the future” [17] p. 530, which contributes to a sense of wholeness for the recipient.
Review of literature
A review of literature was conducted to examine the influence of a relationship-based care model or caring behaviors on patient and nurse outcomes including patient satisfaction as well as nurse and patient perceptions of caring.
Patient Satisfaction
Several studies found positive relationships between patient’s perceptions of caring and patient satisfaction [2,3,18] following the implementation of nurse caring behaviors. Of the RBC studies reviewed, all reported an increase in patient satisfaction scores following implementation of relationship-based care [19-24]. However, the instruments used to measure patient satisfaction varied widely from anecdotal information [22] to use of the standardized Hospital Consumer Assessment of Healthcare Provider and Systems (HCAHPS) survey. Using the HCAHPS survey, Woolley et al. [24] found a steady upward trend, with scores ranging from 86% to 100% on four specific nursing behaviors. Field [25] collected data on the HCAHPS survey using a large system-wide and inpatient sample of patients from medical-surgical groups prior to as well as at six months and 12 months post-implementation of a RBC model. Results from an analysis of variance (ANOVA) showed a slight increase in post intervention HCAHPS scores. Winsett and Hauck [23] found an increase in patient satisfaction scores from a range of 8.55 to 8.81 pre-implementation to 9.02 (on a 10-point scale), but the instrument and its validity were not reported. Results of two studies [19, 21]
Perceptions of Caring
A comparative, descriptive cross-sectional study by Poirier and Sossong [16] used the Caring Behaviors Inventory-Elders to compare patients’ and nurses’ perceptions of caring on an inpatient oncology unit. Nurses rated their caring behaviors significantly higher than the patients. Patients placed greater importance on caring related to meeting technical needs versus emotional needs. A young mean age of the nurses may have contributed to inexperience and influenced the patients’ perceptions regarding the importance of technical competence. No significant differences were found in patients’ or nurses’ perceptions of caring related to the age, gender, or education of the nurse [16].
Nurses’ Perceptions of Caring
There is limited research that examines nurses’ perceptions of their own caring behaviors. Winsett and Hauck [23] measured nurse caring behaviors using the Caring Behavior Checklist before and following implementation of RBC. An observed statistically significant increase in both verbal and nonverbal caring behaviors by nurses was found between the pre-implementation and 3-month and 12-month post-implementation periods [23].
Results of a study by Porter, Cortese, Vezina, and Fitzpatrick [26] found that participants had high perceptions of caring behaviors using the Caring Behavior Inventory (CBI-24), with a mean total score of 5.54 out of a possible total mean score of 6.0 following the implementation of a caring, professional practice model. Highest scores were reported for the subscale related to knowledge and skill while lowest scores were reported for the positive connectedness subscale. While high perceptions of nurse caring were evident, the study did not report the nurses’ perception of caring behaviors prior to implementation of the Relationship Centered Care Professional Practice Model. Relationships could not be determined between the nurses’ perceptions of caring and age, years of practice experience, or other demographic factors due to an overall lack of variability in the scores.
While considerable attention has been given to the importance of caring on patient outcomes, there is limited research on outcomes for nurses. This study aims to expand what is known about nurses’ perceptions of caring. Further, this study will use a new instrument, the Caring Assessment for Care Givers instrument (CACG), which was specifically developed to be used in settings that have implemented the RBC model. The nurses’ overall perception of caring will be explored as well as the dimensions of caring that are most and least important to nurses.
Methods
Design, Setting, Sample
A cross-sectional, descriptive correlational design was used to study responses of nurses to the experience of working in a 267 bed United State acute care facility. In 2015, hospital administration at this facility adopted a strategic initiative to implement the RBC model for the medical-surgical division. All regular part-time and full-time registered nurses who work primarily providing direct patient care on the medical-surgical units were invited to participate.
Sample and Recruitment
Data collection was conducted over a one month period during town hall meetings that were held with the director for the medicalsurgical division. Nurses unable to attend the town hall meeting were identified with assistance from unit managers by using the attendance sheet. Eligible nurses who did not attend the town hall meeting were contacted individually by email and invited to participate. An oral or written explanation of the study was provided to all nurses along with a statement specifying that the returned surveys indicated consent to participate. This research study was submitted for approval prior to data collection to the institutional review board of Case Western Reserve University as well as the institutional review board of the regional hospital where the studied was conducted.
Data Collection and Measures
A demographic questionnaire was used to obtain descriptive statistics regarding the sample population. The Caring Assessment for Care Givers (CACG) instrument was used to measure nurses’ perception of caring. The CACG, a valid and reliable instrument [27], is based on the five processes or dimensions of Swanson’s midrange theory of caring and includes the five processes of knowing, being with, doing for, enabling, and maintaining belief. Unlike the Caring Behavior Inventory-24 (CBI-24) which has been used with both patients and nurses, the CACG instrument was developed specifically for use with nurses in settings that use a RBC model. The instrument consists of five subscales with five scaled items for each of the five caring processes. Each scaled item is dichotomous in nature, with a behavior describing a low caring orientation on the left and a behavior describing high caring orientation on the right. The total score for each subscale ranges from 5 to 25, with the total score for the instrument ranging from 25 to 125. The higher the score, the greater or stronger the overall caring orientation of the caregiver [27]. Authorization was received to use the CACG instrument.
Description of Instrument
The CACG was tested and found to be both valid and reliable [27]. The content validity index of the instrument was found to be acceptable at 0.84. Internal consistency reliability was completed and the overall alpha coefficient was .939 for the instrument [27]. In the current study, the Cronbach alpha coefficient was .934.
The total mean score (25-125 range) on the CACG for the sample population was determined to identify nurses’ overall perception of caring. The mean score (5-25 range) for each of the five subscales for the sample population was determined to identify the dimensions of caring that were most and least important to nurses.
Additional analyses was conducted to determine the relationship between nurses’ perception of caring and the mean years of nursing experience. A Spearman Rho was used to explore the relationship between the nurses’ perceptions of caring and the highest level of nursing education.
Results
A total of 94 usable surveys were returned from 149 eligible nurses for a response rate of 63.0%. There was an equitable distribution of respondents from each of the four nursing specialty units. Years of experience in nursing ranged from 6 months to 40 years. Additional demographic characteristics of the sample population are seen in Table 1.
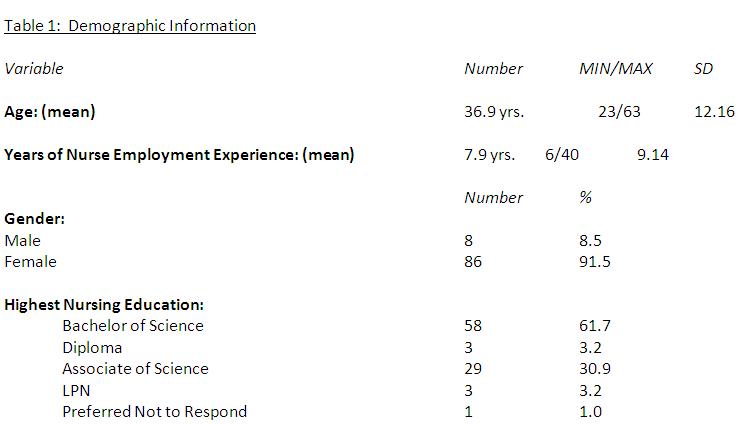
Table 1: Demographic Information
Results revealed an overall high perception of caring for the sample population with a mean total score on the CACG of 107.14 (25-125 range) as shown in Table 2. Of the five subscales, the subscale for the caring process of ‘doing for’ had the highest overall composite score of 21.68 (5-25 range) while the subscale for the caring process of ‘knowing’ had the lowest overall composite score of 21.10 (5-25 range) as shown in Table 3.
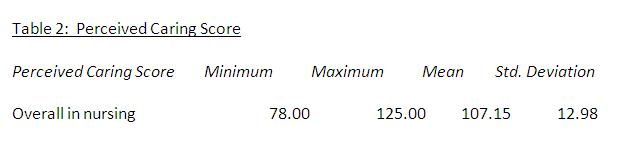
Table 2: Perceived Caring Score
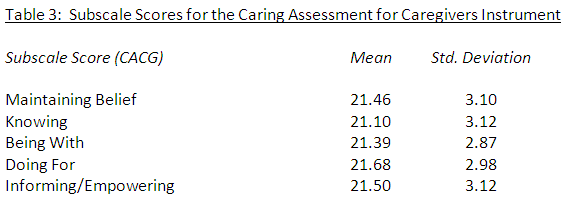
Table 3: Subscale Scores for the Caring Assessment for Caregivers Instrument
Analyses were done to determine the relationship between nurses’ perception of caring and the highest level of nursing education and years of nursing experience. A small to moderate, positive relationship was found between the overall nurses’ perception of caring score and the number of years of experience in nursing and (r = .29, p < .01) with higher perceptions of caring reported by nurses with more experience. Using a Spearman Rho, no significant relationship was found between the nurses’ perceptions of caring and the highest level of nursing education (rs = -.02).
Discussion
The finding of a high perception of caring using a relationshipbased care model is consistent with previous studies that examined caring behaviors and nurses’ perception of caring following the implementation of a caring, professional practice model [23,26]. Despite challenges of a complex, fast-paced, unpredictable health care environment, nurses reported an overall high perception of caring using a relationship based-care model. Emphasis placed on caring behaviors as part of the relationship-based care model may account for the high perceptions of caring by nursing respondents. Ongoing educational programs and unit specific strategies are used to maintain staff awareness and enhance the implementation of relationship-based care principles.
Of the five subscales, the subscale for the caring process of ‘doing for’ had the highest overall composite score of 4.32 (out of a possible 5). This subscale describes the care nurses provide for patients who are unable to provide for themselves and includes caring behaviors which could be described as more technically oriented than the other four subscales. Previous studies using the Caring Behaviors Inventory-24 (CBI-24) to measure nurses’ perception of caring found that the subscale of knowledge and skill received the highest ratings [26]. Direct comparison between the subscales on the CBI-24 and the CACG cannot be made. However, results from studies using the CBI-24 [23, 26] and the findings from this study using the CACG suggest that nurses highly value clinical knowledge and skills. Nursing competence and technical skills represent highly valued caring behaviors that many nurses associate with good nursing care.
Results found that the subscale for the caring process of knowing had the lowest overall composite score of 4.25 (out of a possible 5) followed closely by the subscale of being with (4.28 out of a possible 5). The subscale of knowing focuses on the nurse’s desire to understand events and the lived realities of those in the nurse’s care while the subscale of being with describes the nurse’s ability to be emotionally present to others. Studies on caring [16,26,28,29] using the CBI-24 found the lowest mean scores on the CBI-24 for the subscale on positive connectedness. The dimension of connectedness is described as the provision of constant assistance to patients with readiness. Direct comparison between the subscales on the CBI-24 and the CACG cannot be made. However, both the subscale of being with for the CACG and the subscale of positive connectedness for the CBI-24 include items that reflect the nurses’ ability to spend time with the patient, listening to the patient while being present.
The nurses’ low perception on the subscale of being with may reflect a belief that nurses are unable to spend time at the bedside due to competing demands for their time. Further, being with patients requires emotional presence with the patient and family. Being with involves the use of higher level listening and therapeutic communication skills beyond those used routinely to convey information or provide teaching. Nurses who have not received education in the use of therapeutic presence and communication may be uncomfortable or less prepared to engage in difficult conversations and thus place lesser importance on these aspects of nurse caring.
A small to moderate, positive relationship was found between the overall nurses’ perception of caring score and the number of years of experience in nursing with higher perceptions of caring reported by nurses with more experience. Amendolair [10] previously found a weak correlation between nurses’ perceptions of caring and years of nursing experience. The finding that more experienced nurses report higher perceptions of caring suggests that caring might be a skill that can be enhanced through situation-based, experiential learning.
Nurse theorist, Patricia Benner, proposed that expert nurses develop skills and understanding of patient care from not only proper education but experiential learning, growing in their mastery of pattern recognition and the nature of clinical situations [30]. Thus, nurses with more years of practice experience may respond with greater competence and skill to many of the caring behaviors and technical items found on the CACG.
No relationship was found between the nurses’ perceptions of caring and the highest level of nursing education. The curricular content of the basic nursing program rather than the type of program could be a stronger factor influencing nurses’ perception of caring.
Limitations
A major limitation to this study is the lack of a measure for nurses’ perceptions of caring prior to implementation of the relationshipbased care model. While a high level of caring was reported, to what extent the model played a role is unknown. There was a small sample size of convenience for this study. The findings are site-specific and cannot be generalized to other institutions that have adopted a relationship-based care model. Further, the CACG instrument is new instrument. No published research could be located at the time of this study which used this particular instrument. Therefore, no direct comparisons could be made to other studies for similarities or differences based on the use of this measurement tool.
Implications and Recommendations
This study contributes to the advancement of nursing knowledge by expanding what is known about nurses’ perceptions of caring. The nurse is the single most important healthcare provider for patients during hospital encounters. It is the nurse who coordinates and communicates with the health care team regarding the patient’s plan of care, monitors and assesses for changes in the patient’s status, and serves as a patient advocate for changes in the health care plan. Nurses need to recognize the importance of their caring behaviors on patient advocation. Nurse caring has been found to be a major factor in the patient’s intention to recommend or return to a health care facility which poses implications for the financial well-being of the health care facility [15].
While nurses report an overall high perception of caring, lower mean scores on the subscales of knowing and being with suggest that there is still room for improvement. Focus groups with nurses could explore more fully the meaning these caring behaviors have for nurses or identify the need for additional education on specific aspects of relationship-based care. Exploration of these caring behaviors may identify the need for educational interventions and administrative support to cultivate these interpersonal, relationshipbased skills in nurses.
Nursing leadership along with hospital administration should maintain or enhance programs to support use of the relationshipbased care practice model. Approaches could include recognition programs for staff who demonstrate exemplary, compassionate patient care. Recognizing nurses for their exemplary care signifies a valuing of the behavior by administration and encourages continued growth of a therapeutic, caring environment. Additionally, research should be conducted to examine hiring practices and performance appraisals in facilities which have adopted the RBC model to determine if and how caring behaviors are assessed during job interviews and performance evaluations.
Further study is needed to fully explore the influence of relationship-based care on nurse outcomes such as nurse turnover and nursing satisfaction. A reduction in nurse turnover following the implementation of a RBC model was reported by Gerrie and Nebel [20] as well as Winsett and Hauck [23]. Research is needed to explore the influence of relationship-based care on nurse retention and resultant cost savings to the institution. Two studies [31, 32] suggested that relationship-based care increased nurse satisfaction using institutionally developed measures. Study is needed to explore the influence of relationship-based care on nurse satisfaction using valid and reliable instruments.
Lastly, research is needed to fully study the influence of relationshipbased care on patient outcomes. Limited studies [19, 20] examined the influence of the model on patient outcomes such as length of stay or patient safety with mixed results. Further study is recommended to explore the importance of specific caring behaviors for patients based on the nursing unit or patient attributes. Poirier and Sossong [16] found that patients placed greater importance on technical competence as opposed to the emotional aspects of caring. Research is needed to fully examine patients’ perceptions of priority. Technical competence may be preferred over interpersonal aspects of care by patients who are critically ill.
Acknowledgement
The author acknowledges with gratitude Drs. Joyce Fizpatrick, Maryjo Prince-Paul, and Patricia Keresztes for their guidance in the completion of this study and manuscript. The author also acknowledges Carol Walker, for her support and all of the nurses who graciously participated in this research study.
Conflict of Interest Disclosure
The author declares that there are no conflicts of interest.
Consent Statement
The author gives permission to Gexin publications for publication of this manuscript in the online Journal of Comprehensive Nursing Research and Care.
Reference
Dingman SK, Williams M, Fosbinder D, Warncik M (1999) Implementing a caring model to improve patient satisfaction. J Nurs Adm.29(12): 30-37.View
Wolf ZR, Colahan M, Costello A, Warwick F, Ambrose MS et al. (1998) Relationship between nursing caring and patient satisfaction. MedSurg Nurs. 7: 99-106.View
Wolf ZR, Miller PA, Devine M (2003) Relationship between nurse caring and patient satisfaction in patients undergoing invasive cardiac procedures. Med Surg Nurs. 12: 391-396. View
Khademian Z, Vizeshfar F (2008) Nursing students’ perception of the importance of caring behaviors. J Adv Nurs. 61: 456-462.View
Koloroutis M (Ed.) (2004) Relationship-based care: A model for transforming practice. Creative Health Care Management, Minneapolis, MN.
Swanson KM (1993) Nursing as informed caring for the wellbeing of others. Image: J Nurs Scholarsh. 24: 352-357. View
Watson J (1988) New dimensions of human caring theory. Nurs SciQ. 1: 175-181.
Duffy JR (2003) Caring relationship and evidence-based practice: Can they co-exist? Int J Human Caring. 7: 45-50.
Hayes JS, Tyler-Ball S (2007) Perceptions of nurses’ caring behaviors by trauma patients. J Trauma Nurs. 14: 187-189.View
Amendolair D (2012) Caring behaviors and job satisfaction. J Nurs Adm. 42: 34-39.View
Straughair C (2012) Exploring compassion: Implications for contemporary nursing. Part 1. Br J Nurs. 2(3):160-164.View
Koloroutis M, Trout M (2012) See me as a person. Creative Health Care Management, Minneapolis, MN.
Sheldon LK, Barrett R, Ellington L (2006) Difficult communication in nursing. J Nurs Scholarsh. 38: 141-147.View
Tay LH, Hegney DG, Ang E (2010) A systematic review on the factors affecting effective communication between registered nurses and oncology adult patient in an inpatient setting. Johanna Briggs Institute Library of Systematic Reviews, 8(22).View
Burtson PL, Stichler JF (2010) Nursing work environment and nurse caring: Relationships among motivational factors. J Adv Nurs. 66: 1819-1831.View
Poirier P, Sossong A (2010) Oncology patients’ and nurses’ perceptions of caring. Can Oncol Nurs J. 20: 62-65.View
Swanson KM (2015) Kristen Swanson’s theory of caring. In M.C. Smith and M.E. Parker (Eds.), Nursing Theories and Nursing Practice (pp.521-531). F.A. Davis Company, Philadelphia, PA.View
Yeakel S, Maljanian R, Bobannon RW, CoulombeKH (2003) Nurse caring behaviors and patient satisfaction. J Nurs Adm. 33: 434-436.View
Cropley S (2012) The relationship-based care model. J Nurs Adm. 42: 333-339.View
Gerrie J, Nebel A (2010) Improving patient outcomes with relationship-based care. Nurse Leader. 12: 51-54.View
Hedges C, Nichols A, Filoteo L (2012) Relationship-based nursing practice: transitioning to a new care delivery model in maternity units. J Perinat Neonatal Nurs. 26: 27-36.View
Schneider MA, Fake, P (2010) Implementing a relationshipbased care model on a large orthopaedic/neurosurgical hospital unit.Orthop Nurs. 29: 374-378.View
Winsett RP, Hauck S (2011) Implementing relationship-based care. J Nurs Adm 41: 285-290.View
Woolley J, Perkins R, Laird P, Palmer J, Schitter MA et al. (2012) Relationship-based care: implementing a caring, healing environment. Medsurg Nurs. 21: 179-184.View
Field L (2015) The Effect of the implementation of relationshipbased care on patient satisfaction.(Unpublished doctoral dissertation). Walden University.View
Porter CA, Cortese M, Veniza M, Fitzpatrick JJ (2014) Nursing caring behaviors following implementation of a relationship centered care professionalpractice model. Int J Caring Sci. 7: 818-822.View
Steele-MosesS, Koloroutis M, Ydarraga D (2011) Testing a caring assessment for care givers instrument. Creat Nurs. 17: 43-50.View
Green, A. (2004) Caring behaviors as perceived by nurse practitioners. J Am Acad Nurse Pract. 16: 139-148.View
Palese A, Tomietto M, Suhonen R, Efstathiou G, Tsangari H et al. (2011) Surgical patient satisfaction as an outcome of nurses’ caring behaviors: a descriptive and correlational study in six European countries. J Nurs Scholarsh. 43: 341-350.View
Benner P (1984) From novice to expert: excellence and power in clinical nursing practice. AddisonWesley, Menlo Park.View
Blanton S, James AG (2006) Branching out to others. Oncol Nurs Forum. 33: 476.
Osthed KM, Marier-Porchia M, Farnsworth J (2008) The effect of relationship-based care on RN job satisfaction. Commun Nurs Res. 41: 448.