
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care Volume 7 (2022), Article ID: JCNRC-181
https://doi.org/10.33790/jcnrc1100181Review Article
Herbal Treatment for Infertility in Women: A Systematic Review
Nor Ashikin Mohamed Noor Khan1, Mohamad Rodi Isa2*, Nurrin Nabilla Md Rashidi3, Nur Iman Izzati Mohammad Zaip3, and Nik Nur Syazleen Nik Rohaimi3
1 Department of Physiology, Faculty of Medicine, UniversitiTeknologi MARA Selangor Campus, Jalan Hospital, 47000 Sungai Buloh, Selangor
2Department of Public Health Medicine, Faculty of Medicine, UniversitiTeknologi MARA Selangor Campus, Jalan Hospital, 47000 Sungai Buloh, Selangor, Malaysia.
3Faculty of Medicine, UniversitiTeknologi MARA Selangor Campus, Jalan Hospital, 47000 Sungai Buloh, Selangor, Malaysia.
Corresponding Author Details: Mohamad Rodi Isa, MBBS, DAP&E, MPH, DrPH, Department of Public Health Medicine Faculty of Medicine, UniversitiTeknologi MARA Jalan Hospital, 47000 Sungai Buloh, Selangor, Malaysia. E-mail: rodi@uitm.edu.my
Received date: 23rd March, 2021
Accepted date: 06th April, 2022
Published date: 09th April, 2022
Citation: Mohamed Noor Khan, N.A., Isa, M.R., Md Rashidi, N.N., Mohammad Zaip, N.I.I., & Nik Rohaimi, N.N.S. (2022). Herbal Treatment for Infertility in Women: A Systematic Review. J Comp Nurs Res Care 7(1):181.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Infertility is a disease of the male or female reproductive system defined by the failure to achieve pregnancy after 12 months or more of regular unprotected sexual intercourse. This study aimed to systematically review the mechanism, benefits and causes of using herbal treatment in treating infertile women of reproductive age. The search for suitable studies was carried out using Google Scholar, PubMed, Scopus and Science Direct using the search string “Herbal Treatment'' AND (“Infertility Women” OR “Infertility Female” AND (“Mechanism” OR “benefits” OR “cause”). The inclusion criteria were herbal treatment, herbal medicine or alternative treatment and women in the reproductive age. The exclusion criteria were men, older women (beyond reproductive age) and females before menarche. A total of 7 articles were systematically reviewed and appraised. The herbal treatment of interest includes Huoxue Xiaoyi Granule (HXG), Bushen Zhuyun Granule (BZG), Dan’e mixture, Ziyin recipe (ZR), Liuwei Dihuang Granule (LDG), Erzhi Tianghui Granule (ETG), Jiutengzhuyu tablets and Macrophage – activating Chinese mixed herbs (MACH). The herbal treatments had many benefits such as to improve female infertility in terms of increasing the number of high-quality oocytes and embryos, improving follicular development, ovulation, clinical pregnancy rates, blood circulation, clinical symptoms, live birth rate and endometrial receptivity. Many evidence-based traditional Chinese medicine practices were made. Before conducting more investigations, closer monitoring, toxicology studies, standardized dosage and extract used, adequate design of multicentred, randomized, parallel-controlled and blinded trials are required to deliver improved evidence for future research.
Keywords: Herbal Treatment, Infertility, Women
Introduction
The World Health Organization (WHO) terms infertility as a disease of the male or female reproductive system defined by the failure to achieve pregnancy after 12 months or more of regular unprotected sexual intercourse [1]. It is estimated that infertility affects between 48 million couples and 186 million people worldwide [2-4].
Infertility can be divided into primary and secondary infertility. Primary infertility refers to infertility that occurs before the first pregnancy. Secondary infertility is classified as the inability to become pregnant or incapable of carrying a pregnancy to a live birth after either a previous pregnancy or a previous ability to carry a pregnancy to live birth. Patients in this category have repeated spontaneous miscarriages and are unable to carry a pregnancy to live birth [5].
Infertility is considered a global issue for childbearing couples who are unable to conceive [6]. It can be attributed to a variety of abnormalities with the ovaries, uterus, fallopian tubes, and endocrine system. According to Adams J, Lui CW [5], infertility can be caused by many distinct factors of the reproductive system, in either women or men. In women, infertility can be due to tubal, uterine, ovarian, or endocrine disorders such as blockage of the fallopian tube, endometriosis, disorders, polycystic ovarian syndrome, and pituitary cancers, respectively [7]. However, infertility can sometimes be unexplained due to multiple factors of both partners. Age over 35, diabetes, eating disorders, excessive alcohol use, exposure to environmental toxins, such as lead and pesticides, radiation therapy or other cancer treatments, sexually transmitted diseases (STDs), smoking, stress, and weight problems (obesity or underweight) increase the risk of female infertility [7].
Treatment of infertility includes the use of fertility drugs or surgery [7]. However, the cost of medical infertility treatment is very expensive. It is estimated that the successful outcomes (delivery or ongoing pregnancy by 18 months) were higher than USD61,377 for In-vitro fertilization (IVF) [8]. Therefore, the majority of women opted for complementary and alternative treatments due to the lower cost, safer, or more effective solution [9]. These include pelvic physical therapy, hypnosis, yoga, homoeopathy, spiritual healing, as well as acupuncture and herbal therapy pelvic physical therapy, hypnosis, yoga, homoeopathy, spiritual healing, as well as acupuncture and herbal therapy [10].
Herbal medication may also be used as an alternative treatment for infertility. It is estimated that herbal medicine use during pregnancy ranges from 1% to 87%, worldwide [11]. In countries where access to standard clinical infertility treatment is limited, women opt for herbal medicine to conceive. Herbal remedies are chosen due to their low cost, local accessibility, integration with cultural and religious values, perceived efficacy and safety, lower side effects as well as dissatisfaction with conventional healthcare delivery [12]. Despite the popularity of traditional and complementary medicine, evidence of its safety and efficacy remains inconclusive. Hence, in this review, our focus will be on the effectiveness of using herbal treatment to treat infertility in women. We hypothesize that herbal treatment may improve the chances of pregnancy in infertile women of reproductive age. Therefore, the objective of this study is to systematically review the mechanism, benefits and causes of using herbal treatment in treating infertile women of reproductive age.
Material and Methods
The review was carried out following the reporting standards as suggested in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.
Performing Formulated Questions
The review was performed by identifying the type of evidence needed to answer the research question. The strategy using Domain, Determinant, and Outcome (DDO) format was used in the study to obtain any relevant answers and to identify the question and concentrate the mind. The strategy is shown below.
Domain – “Infertility Female” OR “Infertility Women”
Determinant – “Herbal Treatment”
Outcome – “Mechanism” OR “benefits” OR “cause”
Comprehensive Literature Review
The searching procedure was conducted using four bibliographic databases i.e Science direct, Google Scholar, Scopus and PubMed and other evidence sources to address the review question. The comprehensive literature search involved looking at the eligibility of articles, searching strategy for identification of studies, study selection, and data extraction.
Eligibility Criteria
This research examined herbal fertility treatment in published articles. The inclusion criteria in this study were herbal treatment, herbal medicine or alternative treatment and women in the reproductive age. The exclusion criteria were men, older women (beyond reproductive age) and females before menarche. The studies that did not meet the specific inclusion and exclusion criteria were excluded from being reviewed and appraised.
Search Strategy for Identification of Studies
The process of searching strategy for identification of studies includes all published studies. The boolean search was performed on each database using the search term: “Herbal Treatment” AND (“Infertility Women” OR “Infertility Female” AND (“Mechanism” OR “benefits” OR “cause”). The published literature was carefully searched for this study.
Published Articles
Published articles referred to any published original journal article. The databases used in the search were Science Direct, Scopus, PubMed, and Google Scholar.
Screening of Titles and Abstracts
All citations were identified by screening and organizing titles and abstracts of the published articles studies using Microsoft Excel. Duplicate articles were identified and deleted. The coding study guide was used to screen relevant articles and theses. Study screening looking for suitable titles and abstracts was conducted by three independent researchers. When all researchers agreed to the suitability of title and abstract, the articles with full text were obtained.
Obtaining Full Text of Articles
All published articles were searched. Full-text articles were obtained and downloaded from the established resources i.e., Science Direct, Scopus, PubMed and Google Scholar using similar search terms. Articles without full text were excluded from the study.
Selection of Suitable Full-Text Articles
The process of selecting suitable full text published articles was carried out by all group members. An agreement of inclusion and exclusion criteria was made before starting the review process.
Critical Appraisal
Critical appraisal was performed by two independent researchers to assess study quality and appropriateness of study design to the research objective. The articles which do not fulfil the criteria and poor-quality studies were excluded. The articles have been appraised using the Consolidated Standards of Reporting Trials (CONSORT) statement to maintain the quality of the articles [13].
Data Extraction
Data extractions were performed by two independent researchers to establish inter-rater reliability and to avoid data entry errors. Study context factors of published articles were included in the information describing the study and its subjects. Reported findings of the remaining studies were extracted onto a data extraction form. Lists of included studies were then generated stratified by name of study, study design, type of patient, dose, sample size, result and conclusion of the study.
Flowchart of the Study
The article searching and selection process are shown in Figure 1.
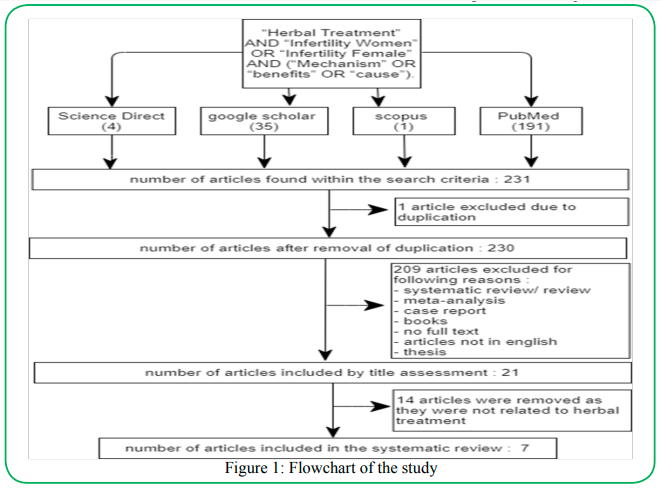
Figure 1: Flowchart of the study
Data Management
All relevant articles were manually coded in the spreadsheets as described in the Evidence Table (Table 1). The electronic spreadsheets were utilized to import the data into Excel sheets for data analysis.
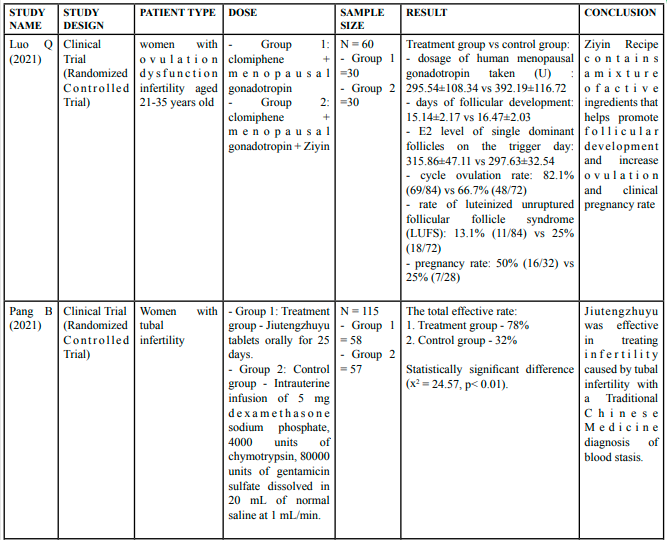
Table 1: Summary of the Articles
Statistical Analysis
Data were analyzed using descriptive statistics. The numerical outcome was analyzed using mean and standard deviation. The categorical outcome was analyzed using frequency and percentage.
Results
A total of seven articles were suitable for the review and appraisal. The summary of the articles is shown in Table 1. Out of the seven studies, six (85.7%) studies were conducted using randomized clinical trials and one (14.3%) study was conducted using a clinical trial without mentioning any study design.
The herbal treatment is used the various causes of infertility include minimal or mild endometriosis [14, 15], ovulation dysfunction [16], tubal infertility [17], qi stagnation and blood stasis [14], and follicular developmental disorder due to kidney - yin deficiency [18, 19].
Most of the studies reviewed were conducted in China. From the seven articles, there were eight types of herbs used to treat infertility in women which are Ziyin recipe (ZR) [16], Jutengzhuyu tablet (JTZ) [17], HuoxueXiaoyi Granule (HXG) [14], BushenZuyun Granule (BZG) [14], LiuweiDiHuang Granule (LDG) [19], ErzhiTianghui Granule (ETG) medicine needs more assessment mostly in the quality of the menstrual cycle is fundamental in the management of female infertility [11]. ETG [18], macrophage-activating Chinese mixed herbs (MACH) [20] and Dan'e mixture [15].
The efficacy of traditional Chinese herbal medicine
The age of the female participants was between 20 and 52 years. The participant sample size in the studies reviewed ranged from 30 – 202 patients. Four of the reviewed articles (57.1%) had two treatment groups [14, 16- 18], while two articles (28.6%) had three treatment groups [15, 19]. However, a study by Ushiroyama et al. [20] was conducted only in one group. A total of 728 participants were involved in this systematic review. The minimum number of a participant in each subgroup was 30 and the maximum number was 101.
A majority of the reviewed herbal treatments were reported to confer many benefits and shown to improve female infertility in terms of increasing numbers of high-quality oocytes and embryos, follicular development, ovulation, clinical pregnancy rates, improving blood circulation, clinical symptoms, live birth rate and endometrial receptivity [14, 16- 20]. However, in a study by Zhu S, Liu D [15]. it was reported that the combination of laparoscopy with oral contraceptives (OC) or oral contraceptives and herbal medicine did not improve female fertility.
Discussion
In this review, it was found that all seven articles reviewed are Chinese herbal medicine (CHM). CHM have been used long ago for the treatment of infertility. CHM therapies include Chinese herb drugs with pattern identification, artificial menstruation cycle therapy, single formula therapy, combined Chinese and Western medicine therapy, acupuncture and moxibustion [21]. There are numerous studies demonstrated that CHM could regulate the gonadotropin-releasing hormone (GnRH) to induce ovulation and improve the uterus blood flow and menstrual changes of the endometrium [22, 23].
There were many benefits while using the herbal treatment for infertility women via promoting follicular development and increased ovulation. In mammals, the follicular development is divided into two phases i.e. the pre-antral or gonadotropin-independent phase which regulates by autocrine and paracrine signaling and the antral or gonadotropin-dependent phase is characterized by the rapid proliferation and secretive of granulosa cells [24]. Two major gonadotrophins stimulate follicular growth and ovulation i.e luteinizing hormone (LH) in synergy with follicle-stimulating hormone (FSH) [25]. The normal follicular growth is the result of a complementary action of LH and FSH.
Ziyin recipe (ZR) and Bushen Zhuyun Granule (BZG) act by promoting follicular development. The mechanism of ZR focused on the steroid hormone-mediated signalling pathway, oxidation, reduction, and apoptosis. The PI3K-Akt signaling pathway, RAP1 signaling pathway, HIF-1 signaling pathway, estrogen signaling pathway, ovarian steroid production, and steroid hormone biosynthesis are the most enriched signaling pathways [16]. An RCT involving women with ovulation dysfunction infertility found that there were 22 active ingredients in Ziyin Recipe corresponding to 354 targets, of which 96 were common targets related to ovulation dysfunction infertility. The targets mentioned were SRC, MAPK1, HSP90AA1, MAPK3, PTPN11, ESR1, AKT1, EGFR, NR3C1, KNG1 [16]. Du XY et al., [26] reported that SRC protein (C-src) plays an important role in regulating primordial follicle activation and growth via the PI3K-PKC- ERK1/2 pathway. A study by Zhao RH et al., [14] used a combination of two CHMs i.e. HXG and BZG found a higher incidence of cumulative dominant follicles, rate of cumulative cycle ovulation and rate of cumulative cycle mature follicle ovulation but decrease the incidence of the cumulative cycle of Luteinized Unruptured Follicular Syndrome (LUFS) and incidence of luteal dysfunction (LPD) than the placebo group (p<0.05 or p<0.01) and concluded of being a safe treatment option.
ZR, BZG and Huoxue Xiaoyi Granule (HXG) promote the process of ovulation. A study conducted by Luo Q, Tan Y [16] reported the ingredients used in ZR such as stigmasterol, beta-sitosterol and 17β-estradiol act as estrogen agonists. They bind to 96 targets which are specific to ovulation dysfunction and increase the growth of primordial follicles, thus, promoting ovulation. Therefore, ZR treatment was effective to improve infertility due to ovarian dysfunction. On the other hand, HXG is suitable for infertility caused by endometriosis. HXG contains Salviae Miltiorrhizae, Radix Paeoniae Rubra, and Radix Bupleuri activate and improve blood circulation, remove blood stasis, expand endometrial blood vessels, reduce vascular resistance, promote endometrial growth and improve endometrial receptivity by soothing the Gan and regulating the qi [27].
In this review, we found that five HCM can increase the pregnancy rate which are ZR, BZG, HXG, Liuwei DiHuang (LDG) and Erzhi Tianghui Granule (ETG). BZG and HXG show a significantly higher percentage by 44.6% cases and 29.7% [14] compared to placebo and ZR increased by two-fold higher than the control group [16] on pregnancy rate. LDG increases the clinical pregnancy rate by 63.64% in the treatment group to 36.36% in the control group infertility women due to kidney yin – deficiency [19]. ETG increase in expression of DNMT1 gene in the nuclei of endometrial epithelial cells and stromal cells. It provides instructions for making an enzyme called DNA methyltransferase 1 that involves DNA methylation. The change in DNMT1 is hypothesized to alter the endometrial gene expression pattern, which in turn contributes to the improvement in endometrial receptivity and subsequent success of embryo implantation, thus increasing the clinical pregnancy rate [19]. A systematic review conducted by Reid K and Stuart K [11] found that CHM can improve 2-fold pregnancy rate within 4 months compared to Western Medical fertility drug therapy of IVF for women infertility. However, Zhu S et al., [15] found Dan’e mixture did not show any significant difference in terms of clinical pregnancy and live birth rates between treatment groups.
Tubal factor infertility is the most common female factor infertility and the most prevalent are acute salpingitides and pelvic inflammatory disease (PID) [28]. Jiutengzhuyu (JTZ) and HXG improve blood circulation via alleviating stasis for women with tubal infertility [17]. JTZ tablets included Jixueteng and Tianjixuetang which are known to nourish the blood, promote blood circulation, clear meridians, and regulate the immune system. Pang B, Pang Q [17] also conclude that the important causes of Tubal infertility were due to the expressions of Bc1-2, EGFR, and ICAM-1 and the Jiutengzhuyu tablets might have achieved good effects by interfering with the actions of Bcl-2, EGFR, and ICAM-1. Apart from that, HXG was also proven to improve blood circulation. The herb was used before ovulation. It contains ingredients such as SalviaeMiltiorrhizae, Radix PaeoniaeRubra, and Radix Bupleur that can help to activate and improve blood circulation, remove blood stasis, expand endometrial blood vessels, and reduce vascular resistance [17].
Female infertility is one of the five diseases related to Kidney Disease Syndrome (KDS) [29]. Kidney yin deficiency syndrome (KDS-YIN) is a general term describing the deficient condition of the kidney system manifested by primary and secondary symptoms. The primary symptoms are infertility, sore waist and knees, dry vagina, dysphoria with feverish sensation in the chest, palms, and soles while secondary symptoms were delayed menstrual cycle, decreased menstrual bleeding, or even amenorrhea, dizziness and tinnitus, tidal fever and red cheek, dry mouth and throat, emaciation, insomnia, and amnesia [30]. Liuwei Dihuang Granule (LDG) treatment causes an expression of TTR and RBP4 decline significantly thus alleviating the symptoms of KDS-YIN [19]. ErzhiTianghui Granule (ETG) also provides the same effect by tonifying the kidneys. Once the normal function of the kidney was restored in the KDS-Yin, there was adequate blood to nourish the uterus and create a favourable environment for implantation [18].
LDG was found in improving the high-quality oocyte and developmental potential of embryos by restoring kidney function as well as kidney essence [19]. Melatonin improved oocyte quality and embryo quality in many in vitro and in vivo studies. The antioxidant effect of melatonin is useful during ovulation and oocyte incubation [31]. Myo-inositol (MI) plays an important role in the cytoskeleton and chromatin stabilization and is important in cellular signaling pathways [31].
Assisted reproductive technology (ART) is used to treat infertility. The procedure involves surgically removing eggs from a woman’s ovaries, combining them with sperm in the laboratory, and returning them to the woman’s body or donating them to another woman [32]. Herbal medicine may use as an adjunct to ART in women by an improvement in oocyte quality [20, 33] and ovarian function [33]. A study by Ushiroyama T, Yokoyama N [20] found that macrophage-activating Chinese mixed herbs (MACH) were safe in improving the reproductive outcomes in patients who had previously failed ART due to low embryonic quality. However, its mechanism is not well understood. It could exert its reproductive effects by regulating the immunological balance and by boosting local inflammatory response via the activation of phagocytic cells. Ushiroyama T, Yokoyama N [20] also found an increased rates of blastocyst development in 90% (27/30) of cases in the study.
In mice, the study found that extracts from the traditional Chinese herbal remedy improve the endometrial receptivity with embryonic implantation dysfunction and ovulation stimulation [34]. TCM appears to reverse the expression of endometrial leukaemia inhibitory factor (LIF) and integrin β3 subunit, improves the uterine receptivity and increases the pregnant rate and embryonic implantation [34]. However, an RCT study in the combination of laparoscopy with oral contraceptives (OCs) or OCs and Dan’e mixture did not improve fertility [15]
The majority of alternative medicine users appear more dissatisfied results with conventional medicine because they found the alternative medicine is more congruent with their values, beliefs, and philosophical orientations toward health and life [35]. Herbal treatment in women with infertility, however, possesses its disadvantages. A study by Lam TP [36] explored that it is inconvenient compared to Western medicine since the herbs must be boiled to prepare the medicine and treatment requiresa frequent visit to the Chinese practitioner before the condition is truly treated. In mice, the reproductive toxicity CHMs commonly used during pregnancy was identified, Therefore, caution should be taken in the clinical use during pregnancy while using CHM [37]. There are many challenges while using herbal medicine such as monitoring safety, assessment of safety and efficacy, quality control and safety monitoring [38]. Therefore, it has become mandatory that herbal medicines are covered by a drug regulatory to ensure that they conform with the required standard of safety, quality and efficacy [38]
Conclusion
There are many benefits of using herbal treatment for infertility in women. Many evidence-based traditional Chinese medicine practices were made in the articles reviewed. Before conducting more investigations, closer monitoring, toxicology studies, standardized dosage and extract used, adequate design of multicentered, randomized, parallel-controlled and blinded trials are required to deliver improved evidence-based medicine for future research.
Competing interests:
All authors declare that there is no conflict of interest.
List of abbreviations
BZG: Bushen Zhuyun Granule; ART: Assisted reproductive technology; CHM: Chinese Herbal Medicine; CONSORT: Consolidated Standards of Reporting Trials; ETG: ErzhiTianghui Granule; GnRH: gonadotropin-releasing hormone; HXG: HuoxueXiaoyi Granule; IVF: In-vitro fertilization; KDS: Kidney Disease Syndrome; KDS-YIN: Kidney yin deficiency syndrome: LDG: LiuweiDihuang Granule; LUFS: Luteinized Unruptured Follicular Syndrome; LPD: Luteal Dysfunction; MACH: Macrophage – activating Chinese mixed herbs; MI: Myo-inositol; OC: oral contraceptives; RCT: Randomized Controlled Trials; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; WHO: World Health Organization; ZR: Ziyin recipe
Acknowledgement
We would like to acknowledge the immense contribution of anybody for agreeing to be part of the study.
Funding
This is self-funded research and did not receive any funding.
References
World Health Organization ICD11 - International Classification of Diseases 11th Revision. 2018.View
Mascarenhas, M.N., et al., (2012). National, regional, and global trends in infertility prevalence since 1990: a systematic analysis of 277 health surveys. PLoS Med .9(12): p. e1001356.View
Boivin, J., et al., (2007). International estimates of infertility prevalence and treatment-seeking: potential need and demand for infertility medical care. Human reproduction (Oxford, England). 22(6): p. 1506-1512.View
Rutstein, S.O. and Shah, I.H., (2004). DHS Comparative Report No. 9. Infecundity, Infertility and Childlessness in Developing Countries.View
Adams J, et al., (2009). Women's use of complementary and alternative medicine during pregnancy: a critical review of the literature. Birth, 36(3): p. 237-245.View
Centers of Disease Control and Prevention Infertility (What is Infertility). 2021.View
Cleveland Clinic Infertility Causes. 2020.View
Katz, P., et al., (2011). Costs of infertility treatment: Results from an 18-month prospective cohort study. Fertil Steril. 95(3): p. 915–921.View
Vincent, C., and Furnham, A., (1996). Why do patients turn to complementary medicine? An empirical study. The British journal of clinical psychology, 35(1): p. 37–48.View
Smith, J.F., et al., (2010). The use of complementary and alternative fertility treatment in couples seeking fertility care: data from a prospective cohort in the United States. Fertility and sterility, 93(7): p. 2169–2174.View
Reid, K. and Stuart, K., (2011). Efficacy of Traditional Chinese Herbal Medicine in the management of female infertility: a systematic review. Complementary Therapies in Medicine, 19(6): p. 319-331.View
James, P.B., et al., (2018). Prevalence and Correlates of Herbal Medicine Use among Women Seeking Care for Infertility in Freetown, Sierra Leone. Evidence-Based Complementary and Alternative Medicine: p. 9493807.View
Equator-network (2010). CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials; Available from: https://www.equator-network.org/.View
Zhao, RH, et al., (2020). Chinese Medicine Sequential Therapy Improves Pregnancy Outcomes after Surgery for Endometriosis-Associated Infertility: A Multicenter Randomized Double-blind Placebo Parallel Controlled Clinical Trial. Chinese journal of integrative medicine. 26(2): p. 92-99.View
Zhu, S., et al., (2014). Post-laparoscopic oral contraceptive combined with Chinese herbal mixture in treatment of infertility and pain associated with minimal or mild endometriosis: a randomized controlled trial. BMC complementary and alternative medicine. 14: p. 222.View
Luo Q, et al., (2021). Mechanism of Ziyin recipe for treatment of ovulatory infertility: a network pharmacology-based study and clinical observations. Journal of Southern Medical University. 41(3): p. 319-328.View
Pang, B., et al., (2012). Clinical effect of Jiutengzhuyu tablets on promoting blood circulation in women with oviducal obstruction. Journal of traditional Chinese medicine. 32(4): p. 549–553.View
Fang, L., et al., (2013). Effects of Chinese medicines for tonifying the kidney on DNMT1 protein expression in endometrium of infertile women during implantation period. Journal of alternative and complementary medicine. 19(4): p. 353-359.View
Lian F, et al., (2014). Effects of Liuwei Dihuang Granule on the outcomes of in vitro fertilization pre-embryo transfer in infertility women with Kidney-yin deficiency syndrome and the proteome expressions in the follicular fluid. Chinese journal of integrative medicine. 20(7): p. 503–509.View
Ushiroyama, T., et al., (2012). Clinical efficacy of macrophage-activating Chinese mixed herbs (MACH) in improvement of embryo qualities in women with long-term infertility of unknown etiology. The American journal of Chinese medicine. 40(1): p. 1–10.View
Lin, C.S., (2008). Female infertility from the perspective of Chinese medicine. Hu Li Za Zhi. 55(6): p. 22-27.View
Huang, S.T. and Chen, A.P., (2008). Traditional Chinese medicine and infertility. Curr. Opin. Obstet. Gynecol. 20: p. 211-215.View
Lee, S.H., et al., (2016). Effects of Huang Bai (Phellodendri Cortex) and Three Other Herbs on GnRH and GH Levels in GT1–7 and GH3 Cells. Evid. Based Complement. Alternat. Med. 2016: p. 9389028.View
Larose, H., et al., (2019). Chapter Eight - Gametogenesis: A journey from inception to conception. Current Topics in Development Biology. 132: p. 257-310.View
Raju, G.A.R., et al., (2013). Luteinizing hormone and follicle stimulating hormone synergy: A review of role in controlled ovarian hyper-stimulation. J Hum Reprod Sci. 6(4): p. 227-234.View
Du, X.Y., et al., (2012). The proto-oncogene c-src is involved in primordial follicle activation through the PI3K, PKC and MAPK signaling pathways. Reproductive biology and endocrinology. 10: p. 58.View
Hu, X.W., et al., (2010). Effects of Bushen Huoxue Decoction on FSH and its receptor mRNA expression in mice. Chin J Immunol (Chin). 26: p. 1003-1006.
Dun, E.C. and Nezhat, C.H., (2012). Tubal factor infertility: diagnosis and management in the era of assisted reproductive technology. Obstet Gynecol Clin North Am. 39(4): p. 551-566.View
Zhao, T., et al., (2016). Classification and differentiation between kidney yang and yin decficiency syndromes in TCM based on decision tree analysis method. Int J Clin Exp Med. 9(11): p. 21888-21899.
Yang, F., et al., (2011). Classic yin and yang tonic formula for osteopenia: study protocol for a randomized controlled trial. Trials. 12: p. 187.View
Vitale, S.G., et al., (2016). How to Achieve High-Quality Oocytes? The Key Role of Myo-Inositol and Melatonin. International Journal of Endocrinology: p. 4987436.View
Centers for Disease Control and Prevention Assisted Reproductive Technology (ART). 2019.View
Inoue, T., et al., (2013). Oocyte quality improvement using a herbal medicine comprising 7 crude drugs. Open Journal of Obstetrics and Gynecology. 3: p. 195-202.View
Yu N and Y.T. Yang J, (2011). Extracts from a traditional Chinese herbal remedy (Zhuyun recipe) improve endometrial receptivity in mice with embryonic implantation dysfunction and ovulation stimulation. J Ethnopharmacol. 137(1): p. 389-395.View
Astin, J.A., (1998). Why Patients Use Alternative Medicine Results of a National Study. JAMA. 279(19): p. 1548-1553.View
Lam, T.P., (2001). Strengths and weaknesses of traditional Chinese medicine and Western medicine in the eyes of some Hong Kong Chinese. Journal of epidemiology and community health. 55(10): p. 762–765.View
Wang, C.C., et al., (2012). Safety evaluation of commonly used Chinese herbal medicines during pregnancy in mice. Human Reproduction. 27(8): p. 2448-2456.View
Ekor, M., (2014). The growing use of herbal medicines: issues relating toadverse reactions and challenges in monitoring safety. Frontiers in Pharmacology. 4: p. 177.View