
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care Volume 7 (2022), Article ID: JCNRC-183
https://doi.org/10.33790/jcnrc1100183Review Article
Implementation of a Universal Suicide Risk Screening Tool in the Emergency Department of a Rural Hospital
Catherine Harmston DNP, APRN, FNP-BC1*, & Mary Anne Reynolds RN, PhD, ACNS-BC2
1,2 Annie Taylor Dee School of Nursing, Weber State University, Ogden, Utah, United States.
Corresponding Author Details: Catherine Harmston, DNP, APRN, FNP-BC, Associate Professors- Annie Taylor Dee School of Nursing, Weber State University, Marriott Health Building, 3875 Stadium Way, Dept 3903, Ogden, Utah, United States. E-mail: catherineharmston@weber.edu
Received date: 15th March, 2022
Accepted date: 09st June, 2022
Published date: 11th June, 2022
Citation: Harmston, C., & Reynolds, M. A., (2022). Implementation of a Universal Suicide Risk Screening Tool in the Emergency Department of a Rural Hospital. J Comp Nurs Res Care 7(1):183.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Purpose: Rural communities are disproportionately burdened by suicide. Isolation, poor economics, a lack of mental health resources, and the use of firearms are major contributing factors to high suicide rates in nonmetropolitan communities. This article will discuss the benefit of implementing the Patient Safety Screener (PSS-3), a universal suicide screening tool, in a rural emergency department as a means to improve identification and suicide care for high-risk individuals.
Methods: Data from electronic health records was analyzed to determine how many emergency room patients completed the PSS-3. These values were compared to the total number of patients evaluated in the emergency department each month in order to determine the total percentage of patients screened.
Findings: There was an average of 37% increase in suicide screening over four months. Implementing universal suicide screening in a rural emergency department led to improved detection of high-risk suicidal individuals in medical settings.
Conclusion: Suicide rates are higher in rural locations than in urban settings. Identifying suicidal patients through suicide screening in an emergency department promotes behavioral health intervention leading to reduced suicide rates.
Keywords: Rural Suicide, Suicide Screening, Universal Suicide Screening
Introduction
Suicide
According to the World Health Organization, more than 700,000 people in the world die by suicide each year [1]. In the United States, suicide is the tenth leading cause of death. On average, there are 132 suicides per day in the United States alone [2]. Suicide rates among males are approximately four times those among females, and by age group, suicide rates are highest among those aged 35-64 years and ≤75 years. By race/ethnicity, non-Hispanic whites and American Indian/Alaska Natives have the highest rates of suicide [3].
Rural communities are disproportionately burdened by suicide, with those residing in nonmetropolitan areas exhibiting a 1.5 times higher incidence of suicide [4]. Suicide is problematic in rural locations due to various factors. Geographical isolation, poor economics, and the lack of access to mental health services all contribute to high suicide rates in rural regions.
When an individual feels isolated, the feelings of sadness perpetuate withdrawal from social situations which reinforces feelings of disconnectedness [5]. In adults over the age of 60, social isolation leads to increased suicidal ideation [6]. Thus, older adults living in geographically isolated settings pose a higher risk of suicidal behavior. Kposowa found that divorced and separated persons were over twice as likely to commit suicide as married persons, and divorced men were more likely to commit suicide than were married men [7]. Stack looked at suicide rates using five independent variables, and the results suggested that social isolation, hurt, and guilt, which are prominent characteristics of divorced populations, influence suicide rates [8].
Poverty and unemployment play a significant role in areas with high suicide rates. According to a cross-sectional study completed by Steelesmith et al., suicide rates in rural counties were disproportionately associated with deprivation when compared with large metropolitan counties [9].
The National Advisory Committee on Rural Health and Human Services found that sixty-five percent of rural county residents had no psychiatrist (compared to 27 percent of metropolitan counties), and forty-seven percent of rural counties were without a local psychologist (versus 19 percent). Social workers and counselors are also less available in rural regions than in urban settings [10]. Limited funding and the lack of sufficient mental health services often prevent the rural resident from receiving adequate suicide care [11]. Common factors that prevent people from obtaining adequate mental health treatment are the cost of services, perceived stigma, concerns about confidentiality, busy schedules, shortage of psychiatrist physicians in rural/underserved areas, and lack of transportation [12].
Another notable factor contributing to high suicide rates in rural regions is that suicides in rural populations are often carried out using firearms [13]. Using a firearm is the most lethal method of completing suicide in the United States [14]. In the United States in the year 2017, suicide by firearms accounted for 23,854 total deaths, more than any other means including poisonings and suffocations [15]. Other common lethal means of completing suicide include drug poisoning, poisoning by gas, jumping, and drowning.
Impact of suicide
Suicide has a profound negative impact on families and their communities. In the United States, the average cost of an individual suicide is approximately 1.3 million dollars. The most significant part of this cost is due to lost productivity [16]. According to the National Funeral Directors Association, the average cost of an adult funeral with viewing and burial in the United States is approximately $7,000 [17]. The annual cost in the United States for both suicides and suicide attempts is over $93 billion per year due to lost productivity [16]. These costly consequences create a heavy financial burden for families and associated communities.
While the financial costs of suicide can be devastating, the emotional impact of suicide on families and communities has equally negative consequences. The loss of a loved one by suicide is typically shocking, painful, and often unexpected. There are stigmas that surround death by suicide. Surviving family members and friends are often left with feelings of guilt, sadness, anger, and sometimes shame [18]. People within close-knit rural communities such as emergency medical personnel, law enforcement, clergy, and others who provide support to survivors can all potentially be impacted by suicide [19].
Suicide in Rural Idaho
Idaho is consistently among the states with the highest suicide rates. In 2016, Idaho had the 8th highest suicide rate in the U.S. with a rate of 20.8, 50% higher than the national average. The 2nd leading cause of death for Idahoans ages 15-34 is suicide. The suicide attempt rate in adults from 2012-2016 was 686 per 100,000 [13]. Every two years in Idaho the youth are surveyed in grades 9-12 to identify high-risk behavior. Results from the 2019 survey identified concerning trends in increased suicidal thoughts and feelings of hopelessness [20].
Oneida County is in the Southeastern region of Idaho and has one of the highest suicide rates in Idaho. According to the U.S. Census Bureau, in 2018, Oneida County had a population of 4,488 persons, and the median age of the Oneida county resident was 39.5 with a median household income in 2017 of $43,491 [21]. Malad City is the most populated region of Oneida County and provides healthcare services for residents living in the immediate area and neighboring communities.
Emergency Departments
The Emergency Department (ED) routinely serves as a frontline setting for monitoring suicidal risk in near real time. The CDC 24 estimates that there are over 130.0 million ED visits in the United States each year [22]. Approximately 50% of persons who complete suicide are seen in a healthcare setting by a healthcare provider in the month prior to their death, and over 25% in the week prior to death, making the ED an opportune place to screen for suicidal risk [23].
Suicide screening
The key to reducing suicides in both rural and urban settings is to identify at-risk individuals early on so that appropriate suicide care can be provided. Screening tools assist in identifying people who are experiencing suicidal thoughts and behaviors. Screening tools can easily be administered in primary care settings as well as health care settings such as hospitals. Healthcare organizations can administer screening tools universally to all patients or to a select few who present with a behavioral health complaint. Screening patients for suicidal risk in the hospital emergency department setting has been found to have a twofold increase in detection [24].
The Patient Safety Screener 3 (PSS-3) is a validated suicide screening tool developed specifically for use in Emergency Departments. This tool consists of three short questions administered to patients upon arrival to the ED. The PSS-3 helps identify patients who are feeling suicidal or who have attempted suicide in the past [25].
Methods
The need to reduce suicide rates in Oneida County, Idaho prompted the development of a quality improvement project team within the local healthcare organization. This team consisted of members motivated to ease the burden of suicide within the community. Once the team was organized, a general project implementation plan and timeline were created and a screening tool was selected. Health care providers and emergency department personnel then attended training sessions for ED staff that focused on the need for change within the organization, and taught them how to deliver and score the selected suicide screening tool. Prior to implementation, this project was approved by Weber State Universities Internal Review Board (IRB) and determined safe for patients prior to implementation.
In November 2020, universal suicide screening using the PSS-3 questionnaire was implemented in the emergency department in rural Malad, Idaho. The PSS-3 is reliable and valid with a Cohen’s K score of .94 [26] From November 2020- February 2021 there was an average of 114 patients evaluated in the ED each month. Electronic health records (EHR) were reviewed to determine which ED patients had been screened for suicide using the PSS-3 screening tool. If screening tools were completed in full, and the patient scored positive, charts were reviewed further to determine if an individualized plan of care took place and if the patient was admitted, transferred, or discharged to home.
Results
Chart reviews reflect that following implementation of this quality improvement project, 26-47% of patients evaluated in the emergency department were screened monthly. Prior to implementation of this project, universal screening was not taking place in the emergency department. Table 1 reflects the percentage of screening tools administered in the ED from November 2020-February 2021. The average increase in suicide screening over the measured four-month period of time was 37%. Prior to the completion of this quality improvement project, no suicide screening was being performed in the Nell J. Redfield Memorial Hospital emergency department. Table 1 demonstrated significant improvement in suicide screening when compared to the previous baseline of zero screening.
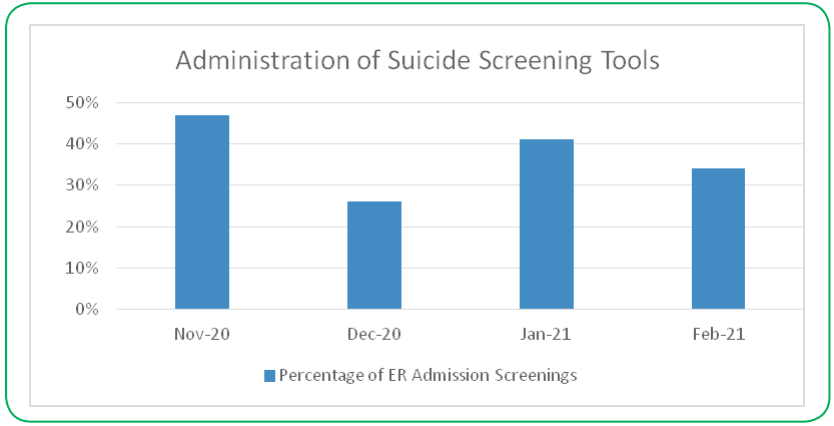
Figure 1: Percentage of ER Admission Screenings
Findings indicate that identifying patients at high risk for suicide improves significantly when universal suicide screening is performed. These findings also suggest that healthcare teams can be motivated to improve screening for suicide risk in rural emergency departments.
Discussion
Patients involved in this quality improvement project who presented to emergency department were provided evidenced based best suicide care. There was minimal risk to patients involved in the implementation of this project. Suicidal patients are vulnerable and confidentiality was carefully protected. Protective factors were in place that limited identifying information such as patient demographic data and other protected health information.
Barriers to the success of this project included organizational elements that challenged made delivering and scoring the suicide risk screening challenging. The hospital in Malad, Idaho was unable to embed the screening tool into the electronic health record. If the screening tool had been embedded, with a prompt that notified healthcare provider when a patient screened positive, it is expected that more patients would have been screened, and positive screens would not have gone unrecognized. For this project, the screening tool was, and continues to be, delivered via paper and pencil. Completed screening tools are then uploaded into the patient’s electronic record.
Another primary barrier was the potential for patients to avoid answering the screening questions with honesty. This barrier is not in the control of those administering the screening tool. Male gender, older age, poor social connectedness, and those with a lower education level are associated with greater odds of non-disclosure [27]. If patients chose to falsify answers on the screening tool, they were not properly identified and the treatment plan did not indicate a need for suicide care.
The cost of implementing this quality improvement was not burdensome and did not present as a barrier. This project had a large amount of support from both the Southeastern Idaho Public Health Department, and the administration team of the hospital. The primary stakeholders live within the community supported improved outcomes for their family members, neighbors and friends.
Conclusion
Suicide rates in rural regions are high secondary to feelings of isolation, the use of guns as lethal means, and a lack of mental health resources. These high suicide rates can be emotionally and financially devastating to surviving family members and communities. This quality improvement project demonstrates that universal suicide screening improves the odds of identifying individuals at high risk for suicide. Once high-risk individuals are identified, the healthcare team can intervene. Intervention reduces suicide risk, thereby saving families and communities from experiencing the loss that is felt when a loved one completes suicide.
Conflict of interest:
The authors have no personal, commercial, political, governmental, academic, or financial conflicts of interests related to the content of this submission.
Acknowledgements:
I would like to thank Dr. MaryAnne Reynolds, John Williams, Rhonda D’Amico and Alica Bell for their encouragement and support of this quality improvement project. I would also like to thank the patients and staff at Nell J. Redfield Memorial Hospital.
References
I would like to thank Dr. MaryAnne Reynolds, John Williams, Rhonda D’Amico and Alica Bell for their encouragement and support of this quality improvement project. I would also like to thank the patients and staff at Nell J. Redfield Memorial Hospital.
Centers for Disease Control and Prevention (CDC). Underlying Cause of Death 1999-2019 results. https://wonder.cdc.gov/ucd-icd10.html. Accessed November 29, 2021View
Kegler, S.R., Stone, D.M., Holland, K.M. (2017). Trends in suicide by level of urbanization-United States, 199902015. MMWR. Morbidity and Mortality Weekly Report. 66: 270-273. https://doi.org/10.15585/mmwr.mm6610a2View
Centers for Disease Control and Prevention. (2021). Suicide in rural America.https://www.cdc.gov/ruralhealth/Suicide.html. Accessed November 30.View
Santini, Z.I., Jose, P.E., Cornwell, E.Y., Koyanagi, A., Nielsen, L., Hinrichsen, C., Meilstrup, C., Madsen, K.R., & Koushede, V. (2020). Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older Americans (NSHAP): A longitudinal mediation analysis. The Lancet Public Health. 5(1): e62–e70. https://doi.org/10.1016/S2468- 2667(19)30230-0View
Bennardi, M., Caballero, F.F., Miret, M., Ayuso-Mateos, J.L., Haro, J. M., Lara, E., Arensman, E., & Cabello, M. (2019). Longitudinal relationships between positive affect, loneliness, and suicide ideation: age-specific factors in a general population. Suicide and Life-Threatening Behavior; 49(1): 90–103. https:// doi.org/10.1111/sltb.12424View
Kposowa, A. J. (2000). Marital status and suicide in the national longitudinal mortality study. Journal of Epidemiology & Community Health; 54: 254–261. https://doi.org/10.1136/ jech.54.4.254View
Stack, S. (1980). The effects of marital dissolution on suicide. Journal of Marriage and Family. 42(1), 83–92. JSTOR. https:// doi.org/10.2307/351936View
Steelesmith, D.L., Fontanella, C.A., Campo, J.V., Bridge, J.A., Warren, K.L., Root, E.D. (2019). Contextual Factors Associated With County-Level Suicide Rates in the United States, 1999 to 2016. JAMA Netw Open. 2(9): e1910936. doi:10.1001/ jamanetworkopen.2019.10936View
National Advisory Committee on Rural Health and Human Services. (2021). Understanding the impact of suicide in rural America: policy brief and recommendations. https://www. hrsa.gov/sites/default/files/hrsa/advisory-committees/rural/ publications/2017-impact-of-suicide.pdf. Accessed November 30.View
Cohen Veterans Network. America’s mental health (2018): attitudes and access to care. https://www.cohenveteransnetwork. org/AmericasMentalHealth/. Accessed November 30, 2021.View
Singh, R. (2017). Rural mental health: Technology, collective intelligence, and community. Academic Psychiatry; 41(1): 135–137. https://link.springer.com/article/10.1007%2Fs40596- 016-0550-y. Accessed May 4,View
Miller, M., Warren, M., Hemenway, D., et al. (2015). Firearms and suicide in US cities Injury Prevention; 21: e116-e119. https://injuryprevention.bmj.com/content/21/e1/e116.short Accessed November 30, 2021.View
Suicide Prevention Resource Center. (2021). Means of Suicide. https://www.sprc.org/scope/means-suicide. Accessed May 23.View
National Center for Health Statistics. (2021). Suicide and Self-Harm Injury. https://www.cdc.gov/nchs/fastats/suicide.htm. Accessed June 15, View
Suicide Prevention Resource Center. Costs of Suicide. https:// www.sprc.org/about-suicide/costs. Accessed November 30, 2021View
National Funeral Directors Association. (2021). Statistics. https://www.nfda.org/news/statistics. Accessed April 26.
Suicide Prevention Resource Center. (2021). Resources for Suicide Loss Survivors. https://suicidology.org/wp-content/ uploads/2019/07/Resources-for-Survivors-of-Suicide.pdf Accessed on November 30.View
Sandler, E.P. (2021). The Ripple Effect of Suicide. National Alliance on Mental Illness. https://www.nami.org/Blogs/ NAMI-Blog/September-2018/The-Ripple-Effect-of-Suicide. Accessed October 14.View
Idaho State Department of Education. (2021). Idaho youth risk behavior survey. https://www.sde.idaho.gov/student-engagement/school-health/files/youth/Youth-Risk-Behavior-Survey-Results-2019.pdf. Accessed July 11.View
United States Census Bureau (2021). Quick Facts: Oneida County, Idaho.https://www.census.gov/quickfacts/ oneidacountyidaho. Accessed February 4.View
Zwald, M.L., Holland, K.M., Annor, F.B., et al. (2018). Syndromic Surveillance of Suicidal Ideation and Self-Directed Violence- United States, January 2017- December. MMWR Morbidity Mortality Weekly Report. 2020; 69: 103-108. DOI: https://www.cdc.gov/mmwr/volumes/69/wr/mm6904a3. htm?s_cid=mm6904a3_wView
Ribeiro, J. D., Gutierrez, P. M., Joiner, T.E., Kessler, R. C., Petukhova, M. V., Sampson, N. A., Stein, M.B., Ursano, R.J., & Nock, M.K. (2017). Healthcare contact and suicide risk documentation prior to suicide death: Results from the army study to assess risk and resilience in service members (Army STARRS). Journal of Consulting and Clinical Psychology; 85(4): 403–408. https://doi.org/10.1037/ccp0000178View
Boudreaux, E.D., Camargo, C.A., Arias, S.A., Sullivan, A.F., Allen, M.H., Goldstein, A.B., Manton, A.P., Espinola, J., & Miller, I.W. (2016). Improving suicide risk screening and detection in the emergency department. American Journal of Preventive Medicine; 50(4): 445–453. https://doi.org/10.1016/j. amepre.2015.09.029View
Journal PSM. PSS-3: Three-Question Suicide Screener for the ER. Patient Safety & Quality Healthcare. https://www.psqh. com/analysis/pss-3-three-question-suicide-screener-for-the-er/. Published Septebmer 18, 2018. Accessed February 4, 2021.View
Edwin D. Boudreaux, Michelle, L. Jaques, Kaitlyn, M. Brady, Adam Matson & Michael H. Allen (2015). The Patient Safety Screener: Validation of a Brief Suicide Risk Screener for Emergency Department Settings, Archives of Suicide Research, 19:2, 151-160, DOI: 10.1080/13811118.2015.1034604View
Husky, M.M., Zablith, I., Alvarez Fernandez V., & Kovess-Masfety, V. Factors associated with suicidal ideation disclosure: results from a large population-based study. Journal of affective disorders. 201; 205: 36-43. https://doi.org/10.1016/j. jad.2016.06.054View