
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care Volume 8 (2023), Article ID: JCNRC-193
https://doi.org/10.33790/jcnrc1100193Research Article
The Collaborative Nursing Practice Between Registered Nurses and Certified Nurse Specialists in Family Health Nursing Regarding Diagnosis Disclosure to a Pediatric Female Patient with Osteosarcoma
Orie Koizumi*, RN, CNSF, MSN, Reiko Inoue, RN, PhD, and Atsushi Sugimura, RN, PHN, MSN
School of Medicine Nursing, Department of Tokai University, 143 Shimokasuya Isehara Kanagawa, 259-1193, Japan.
Corresponding Author Details: Orie Koizumi, RN, CNSF, MSN, School of Medicine Nursing, Department of Tokai University, 143 Shimokasuya Isehara Kanagawa, 259-1193, Japan.
Received date: 01st November, 2023
Accepted date: 26th December, 2023
Published date: 28th December, 2023
Citation: Koizumi, O., Inoue, R., & Sugimura, A., (2023). The Importance of Putting Yourself in Someone’s Shoes: A Case Study of a Workshop at a Medical University in Japan on Multicultural Understanding in Healthcare Services. J Comp Nurs Res Care 8(1):193.
Copyright:©2023, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Objective: This study will illustrate the collaborative nursing practice of registered nurses and certified nurse specialists in family health nursing in a case study focusing on the diagnosis disclosure to pediatric female patients with osteosarcoma.
Methods: The research method is a case study. Data was collected from the patient's medical record regarding the patient's behavior and symptoms, patient care, and family situation and interventions from admission until discharge by a registered nurse, the attending nurse. Data were compiled in chronological order. The analysis method was to summarize nursing practice's characteristic situations in short sentences and create a progress chart. Several researchers discussed the questions, ideas, and intentions that led to the decision to increase the progress charts' reliability. Consistency was ensured by member checking of collaborative nursing practice according to a progress chart. The review committee approved ethical considerations, and the patient's family was verbally informed about the publication, and their consent was obtained.
Results: A pediatric female patient with osteosarcoma. At the start of treatment, chemotherapy was done without diagnosis disclosure to the patient due to family objections. The patient was to undergo tumorectomy, so the patient needed to be informed of the disease. Under the collaborative nursing practice of a registered nurse and certified nurse specialist in family health nursing, the diagnosis is disclosed to the patient for the patient's decision-making. After that, the patient and her family were able to leave the hospital with a positive mindset about treatment.
Discussion: In Japan, the intention of the family greatly influences the diagnosis disclosure to children with pediatric cancer. The results suggest that collaborative nursing practice between registered nurses and certified nurse specialists in family health nursing can lead to the best benefits and outcomes for the patient's family.
Key Words: Pediatric cancer, Diagnosis disclosure, Registered nurse, Advanced practice nurse, Certified nurse specialist in family health nursing, and collaborative nursing practice.
Introduction
Pediatric cancer is said to occur in one case per 10,000 children per year in Japan, and despite the declining birth rate, a certain number of patients are certainly being diagnosed. The study of cancer diagnosis disclosure to children in Japan began in the late 1990s. According to a survey by Horii [1] et al., while only a few children were informed of their disease in 1998, more than 70% of patients themselves wished to be informed in a survey of patients' families in 2018. However, parental intention remained slight at only 5.3% after 20 years. Horii [1] noted that although about 60% of pediatric oncologists have a policy on diagnosis disclosure, there is a disparity in opinion among patients, parents, and physicians. This is due in part to the fact that Japan is a country where education on bioethics and other aspects of life and death is rarely provided in childhood [2], and cancer diagnosis disclosure to children is difficult in Japan, where the majority of the population is not religious.
Osteosarcoma is a very rare category of pediatric cancer, with only about 200 cases per year [3]. The standard therapy usually takes two to three months of drug therapy followed by extensive resection of the tumor and bone reconstruction, with several months of additional drug therapy. Because of the extensive resection, the surgery is very damaging to the adolescent patient as it alters his or her body image. Consequently, patients must comprehend the illness and get motivated to overcome it. Therefore it is crucial that you explain the disease to them.
In Japan, most hospitals that treat pediatric oncology are government-designated medical facilities. In addition to pediatric oncologists, Certified Nurse Specialists (CNS) and Certified Nurses (CN) provide advanced practice in pediatric and oncology nursing. Hospital school and family residential facilities are also available to support patients and families requiring long-term hospitalization. The medical environment for pediatric cancer patients has improved in recent years. On the other hand, since the initial induction therapy for pediatric cancer can be physically and mentally damaging for the patient, a Registered Nurse (RN) is usually in charge of patient and family care as the attending nurse. In addition, when there are significant challenges to the patient and family's condition that cannot be resolved by the RN alone, a CNS or other Advanced Practice Nurse (APN) may intervene in collaboration with the RN. Especially in the case of refractory cancers such as osteosarcoma, APNs often coordinate with physicians, patients, and family members, as they are forced to make decisions with little time to spare and little understanding or acceptance of their child's disease. Consequently, despite the fact that they practice nursing while collaborating with RNs and others, the details of their nursing interventions remain unclear.
Therefore, this study will illustrate the role of APNs in Japan and the characteristics of their nursing practice. In addition, it will focus on cancer diagnosis disclosure to children (Informed Assent) and report on collaborative nursing practice with Certified Nurse Specialists in Family Health (CNSF) among RNs and APNs, based on the case study.
The Study's Purpose
This study will illustrate the collaborative nursing practice of registered nurses and certified nurse specialists in family health nursing in a case study focusing on diagnosis disclosure to a pediatric female patient with osteosarcoma.
Key Terms
Terms definition
(i) Registered Nurse: A person who holds national certification as a registered nurse after completing three or four years of nursing study in Japan.
(ii) Collaborative Nursing Practice: CNSs, including RNs and APNs, provide patient and family care—a series of assessment perspectives, practices, and evaluation processes.
(iii) Informed Assent: Explain the treatment of pediatric cancer in a way that is easy to understand according to the child's level of understanding, and children themselves must be convinced of the contents.
Types and roles of Advanced Practice Nurses in Japan
In 1987, in response to the advancement of medical care, the Ministry of Health, Labour, and Welfare (MHLW) proposed to develop capable CNSs to provide education in specialized fields to nurses to enable them to perform nursing tasks smoothly. Accordingly, the Japanese Nursing Association launched the "CNS System" in 1994, and the CNS field began in graduate education in 1995, with 14 fields now in existence. To qualify, the applicant must have five years of nursing experience, earn 38 credits in a graduate master's program designated by the Japanese Nursing Association, and pass a certificate examination [4]. As of December 2022, 2,901 professional nurses worked in clinical settings throughout Japan. In recent years, we have also begun certifying nurse practitioners (NPs) as those who assume the role of APNs like CNS [5]. NPs in Japan exist in one area of primary care, including those who have taken a certain level of training in medical practice and those who have completed a specific graduate doctoral program. Numerous educational programs and certification schemes are available.
Methods
Research design
This is a case study describing a collaborative nursing practice situation.
Data collection methods
Japanese nursing practice comprises multiple team members, one of them often taking on the role of the primary nurse who centrally conducts nursing interventions. In this study, the RN, the attending nurse, reviewed nursing records and nursing practice. From the time of admission until discharge, information about the patient's behavior and symptoms, patient care, family circumstances, assessment interventions, and nursing practice for the family was gathered from the patient's medical record and organized chronologically.
Analytical methods
Based on a progress chart summarizing characteristic situations about the patient's progress and nursing practice in short sentences, the researcher and practitioners discussed questions, thoughts, and intentions that led to the decisions to increase reliability. Consistency was ensured by member-checking the contents of the analyzed family nursing practice.
Ethical considerations
The approval for publication was obtained from the review committee of the nurse's institution. The patient's family was verbally informed of the case study's strict adherence to personal information and the paper's publication, and their consent was obtained.
Case Presentation
The target facility was Pediatric Oncology, an affiliated hospital in Kanagawa Prefecture. The RNs in this study were in their 20s and had less than 5 years of nursing experience. The CNSF, who was also the APN, had more than 20 years of nursing experience and had been certified as the CNSF for less than 5 years at the time of this study.
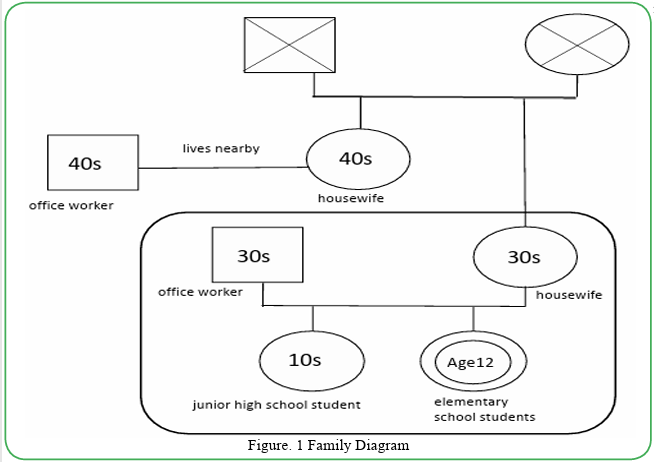
Figure. 1 Family Diagram
Family Composition (Figure. 1)
Patient:
12-year-old girl, 6th-grade elementary school, osteosarcoma of left femur.
Family:
Father is 30 years old and has no medical history. The mother is 30 years old and has no medical history. Sister is 10 years old and has no medical history.
The course of treatment:
In May 201X, the patient was admitted to the hospital with a chief complaint of pain and swelling in the left lower limb. After emergency hospitalization, she was diagnosed with osteosarcoma by pathological and clinical diagnosis. When the tumor was discovered to have shrunk after five months of chemotherapy, a tumorectomy and limb salvage surgery were carried out. The patient was discharged from the hospital following a six month hospitalization.Content of Collaborative Nursing Practice
The progress of collaborative nursing practice between RNs and advanced practice CNSFs is shown in Table 1. The characteristic situations and intervention details for patients and families were summarized in short sentences, and the collaborative nursing practice from admission until discharge was described in chronological order.
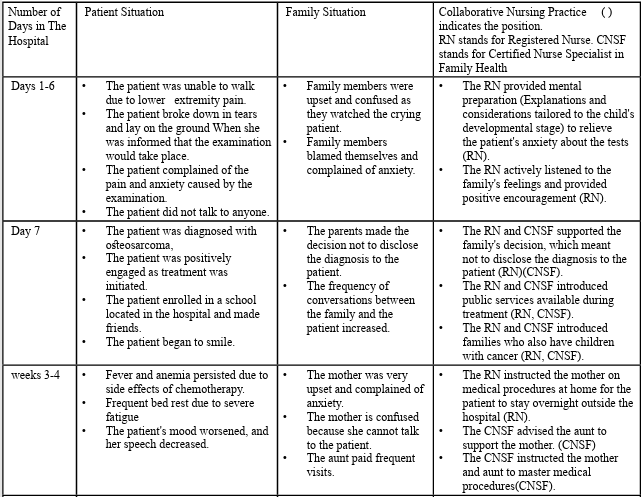
Table.1 The process of disclosing a diagnosis from diagnosis to discharge.
Nursing Practice
The patient continued to undergo tests for a definitive diagnosis from the day after admission. The patient spent most of the time crying due to the pain caused by tests and anxiety about hospitalization. The family was upset and felt remorse for their child. The RNs provided mental preparation (Explanations and considerations tailored to the child's developmental stage) to relieve the patient's anxiety about the tests. They attended to the patient to ensure that the tests would be performed smoothly. We also actively listened to the family's feelings and provided positive encouragement. One week later, the patient was diagnosed with osteosarcoma, and in order to begin treatment immediately, diagnosis disclosure to the patient and obtaining informed assent for treatment were necessary. However, the family stubbornly refused to disclose the name of the disease to the patient. The physician was unable to persuade the family. As a result, the decision was made to proceed with treatment without diagnosis disclosure to the patient, stating that 'there is something wrong with the leg and that needs treatment.' The Registered Nurse (RN) observed potential confusion among the patient and family regarding future treatments. Concerned about potential confusion, the RN reported the situation to seek guidance and a situational assessment from a Clinical Nurse Specialist in Family Nursing (CNSF), who is an Advanced Practice Nurse (APN). The CNSF respected the family's decision not to disclose the name of the disease to the patient. The CNSF then referred and encouraged the family to enroll in a school located in the hospital. In addition, available public services during treatment and families who also have children with pediatric cancer (peer supporters) were introduced to the families to provide emotional stability for the patient and the family. The patient started to smile during the second week of treatment, and the tension and anxiety of the family members decreased.
The patient experienced side effects from the chemotherapy, including fever and anemia, as the treatment went on. Seeing this scenario, the mother became extremely distressed, and the patient's maternal aunt started accompanying her during visits. The RN informed the mother that the patient would be allowed to stay overnight outside the hospital when her side effects improved. The RN also attempted to instruct the mother on medical procedures at home in preparation for staying overnight outside the hospital. However, because of the mother's anxiety over the patient's side effects and the difficulty of the procedures, she was unable to proceed with learning the procedures. After the RN contacted the CNSF regarding the situation, the CNSF called the mother and aunt jointly to provide guidance and urged the aunt to assist the mother. With her aunt's support, the mother gradually mastered medical procedures for home care. The father also started to take part, and the family members developed cordial bonds with each other. The patient was given permission to spend the night outside the hospital following eight weeks of hospitalization.
After 20 weeks of treatment, the tumor was confirmed to have shrunk, and the patient was scheduled for limb salvage surgery. Reconstructive surgery was planned, in which an artificial joint was inserted, and a bone was transplanted. Because the patient's ADLs and growth and development, such as height, might be impacted by the surgery, it was vital to notify the patient of the surgical procedure. The patient began to frequently ask the doctor questions regarding future treatment plans and medications. Moreover, the RNs saw the patient's growth in independence as she began to take care of her medication on her own. However, the family was concerned that the patient's interest in treatment would lead to the patient discovering the name of the disease. Surgery was imminent, time was running out, and there was a need to disclose the diagnosis and explain the procedure simultaneously. Given the family's situation, the RN consulted the CNSF about how to proceed with the diagnosis disclosure to the patient. The CNSF directly informed the family of the need to support the patient's growth and to let the patient decide the future course of treatment on her own. The CNSF also told the patient, "You have worked so hard. It's great that you were able to ask questions about your treatment." Upon observing the shift in the patient's demeanor, the family also decided to inform the patient about his diagnosis.
At week 21, the CNSF and the RNs shared with the family the importance of all family members supporting the patient's decisions. They discussed and shared with the family how to disclose the diagnosis to the patient. The CNSF asked the patient, "Do you want to know about the disease and treatment?" The patient was silent for a moment and then responded, "'I'll listen to the explanation. I also want to speak my mind." The patient's wishes were taken into account by the RN and CNSF, who made arrangements for the doctor to inform the patient of the diagnosis in front of the family. The patient responded, "I understand. " She seemed to be satisfied with the explanation of the diagnosis, future treatment plan, and postoperative complication. The family was relieved that they could explain the situation to the patient before the surgery and reaffirmed their commitment to supporting the patient with the entire family. The patient successfully underwent surgery at week 22, participated fully in rehabilitation, and was released from the hospital at week 24.
Discussion
Pediatric cancer diagnosis disclosure to children
Although treatment outcomes for pediatric cancer have improved in recent years, this can be seen as the price to pay for harsh treatment. Explaining to children the reasons for undergoing such rigorous treatment, gaining their understanding, and securing their cooperation in treatment – known as "Informed Assent" can be considered an unavoidable challenge in pediatric cancer care. In addition, the development of social networks has made it easier for children to search for the name of their disease and find answers to their questions. Long-term follow-up is necessary for children with cancer even after they are cured, taking into account late complications. Hence, patients must comprehend the true name of the illness, its characteristics, and the specifics of its therapy.
On the other hand, "Informed Assent" for pediatric oncology is necessary not only in the early stages of treatment but also in end of-life care. It is the patient's right to live freely in their remaining time as much as possible, even in the terminal stage, and this is true for children as well. In Japan, the custom of discussing death is remarkably rare, and this may be due in part to the fact that most of the population is non-religious. Many healthcare workers are not comfortable discussing death with their patients and their families. Finally, in such a context, diagnosis disclosure to adults - the so called "Respect for the Patient Autonomy" - began to be supported, allowing patients to make their own treatment decisions. In the case of children, however, the issue is not only the child's ability to understand, but also the family needs the time to acknowledge the death of their child. As a result, although it depends on the stage of development, it is reported that only about 60% of patients are given some explanation in the early stages of treatment for pediatric cancer in Japan. To clarify, approximately thirty percent of patients are receiving harsh treatment without being aware of their disease [6].
The need for diagnosis disclosure to children has increased as advances in pediatric cancer care have made long-term survival possible for children. A correct understanding of the disease will affect the children's future when the patients actively participate in their medical care and enhance their quality of life. For example, during life events such as going on to higher levels of education, starting their career, marriage, and childbirth, their health status may influence the choices they make to become independent. It would be better for them to be aware of their sickness to lead an active life.
Based on this principle, patient support provided after obtaining informed assent from the patient (gaining their understanding and securing their cooperation in treatment) is important. This requires " team-based care." However, the implementation of team-based care in Japan is challenging compared to Western countries, where informed consent is commonly used, including with pediatric patients. The concept of diagnosis disclosure is closely related to primary education in the nursing profession. There are diverse perspectives regarding diagnosis disclosure in the primary education of pediatric nursing. The issue has not yet been fully discussed since nurses' views on life and death are also influential. In healthcare, allocating roles among staff members for setting up an environment for explanations requires ingenuity and planning until it is established." The Japanese Society of Pediatric Oncology Nursing provides guidelines [7] regarding diagnosis disclosure to children. It states that repeated explanations are necessary according to the child's age, level of understanding, developmental stage, and what the child wants to know and thinks. It is also reported that when the family refuses, they should be supported while providing a psychological preparation period and environment. Given that the family's values and readiness to disclose the diagnosis to the child will have a significant impact, nurses should evaluate the patient's and family's circumstances and work with them to choose the best course of action while arranging medical team meetings.
Collaborative nursing practice between registered nurses and Advanced Practice Nurses
The onset period of pediatric cancer is the most turbulent time for the family, including the patient. Pediatric cancer treatment should be started early, and the family is forced to make decisions and environmental adjustments without overcoming the shock [8]. In this case, the RN promptly assessed the need for family intervention and consulted the CNSF, a specialist in family support among APNs in Japan who is highly skilled in coordinating staff within the organization, including patients, families, and healthcare workers. In this case, the CNSF assessed the family crisis in accordance with a professional assessment and always shared this perspective with the RN. While approving the option of not disclosing the diagnosis to the patient was considered the ultimate choice, the CNSF could decide in a short period, including the need to wait until the family could accept the situation on their own. In addition, because of the characteristics of pediatric cancer, the CNSF did not choose diagnosis disclosure to the patient in the first week after admission to the hospital, considering the future, and it is thought that CNSF was able to determine when it was necessary to do so. APNs in Japan are assigned six roles (practice, consultation, coordination, education, ethical coordination, and research), of which consultation provides psychological support to RNs and helps them understand patients [9]. In other words, the APN is considered an educator who promotes understanding of the RNs' families, approves their practice skills, and enhances their nursing skills. The family has become more resilient as a result of the RNs and APNs' collaborative nursing practice, which has helped them achieve emotional stability.
RNs, as primary nurses, usually focus on patient bedside care. Therefore, they can quickly detect the condition of the patient and the family members through their words and actions. The CNSF trusted the RN's assessment and judgment skills and shared information with them to find ways to intervene. Having the aunt as an informal resource to support the mother helped strengthen the cohesion within the family as a decision was made based on the information shared with the RN. Usually, the role of the CNSF is to support the family's ability to solve problems while assessing the family's crisis. In this case, the CNSF shared the patient's progress with the family, helped them realize that their child was growing despite the illness, and guided them in deciding on diagnosis disclosure to the patient. The RNs were able to provide joint assistance for the patient and family by informing the CNSF of the circumstances.
Three characteristics of collaborative nursing practice were identified through this case study. Firstly, the CNSF and RN were partners in the field. They established a relationship based on mutual respect, practices, and collaboration. This collaborative relationship is at the heart of Japanese nursing practice, and it works well in challenging and crisis situations. Secondly, in this case, it was inferred that CNSFs give advice to RNs and intervene directly with the family, depending on the situation. It suggests that the CNSF, functioning as an Advanced Practice Nurse (APN), intends to provide educational guidance to the RN in their interactions. The CNSF encouraged the growth of the RNs while consulting with them on their nursing practice and their position as APNs. Thirdly, the CNSF provided direct support to families so RNs would not have difficulty and a supportive relationship could be established with families with complex issues. It is also stated that RNs face a great deal of difficulty when assisting families that are in a state of great distress [10]. However, the CNSF provided a direct intervention that emphasized interaction between the family and the healthcare worker, which led to a preventive intervention that did not confuse the family. There are six types of nursing practice for inpatients in Japan: Functional nursing care model, individual nursing care model, team nursing care model, primary care nursing model, fixed-team nursing model, and modular nursing model. Many facilities have developed their own arranged systems. In the future, intractable cases can be efficiently and effectively obtained by using a nursing delivery system in which APNs intervene collaboratively according to the specialty of the hospital and the subject. Therefore, it is important to analyze and accumulate nursing intervention scenarios continuously.
Diagnosis disclosure to children with cancer and collaborative nursing practice
The pros and cons of cancer diagnosis disclosure to children are still inconclusive as it relates to medical culture, family customs, and values. However, since children have the right to know and to choose their treatment, it is necessary to explain to them. On the other hand, since the level of understanding differs depending on the child's developmental status, the family inevitably takes on the responsibility for decision-making. The family itself cannot sort out its feelings when it is forced to disclose information to children, which is a heavy burden on the family. The diagnosis disclosure to children is a delicate issue. Therefore, it is necessary to continue promoting collaborative nursing practice so that the family and health worker can proceed with a policy they agree on, with the child at the center of the process. In recent years, with the increase in the number of complicated cases in clinical settings and the weakening of family functions, it was suggested that CNSFs form collaborative relationships with RNs within their organizations and mutually enhance their professional skills to enable a family nursing practice that provides the best benefits and outcomes for patients' families.
Conflict of Interest
The presenter and all co-presenters have no conflicts of interest with medical research corporations or other entities that should be stated.
References
Saiki,KS., Nagagawa,K., Iwata,Y, Hara,J., Deborah K., Mayer,TN., Norma C. (2005). Attitudes and practices among pediatric oncologists on truth-telling with children: The situation among Japanese oncologists concerning telling children about their diagnoses, Journal of Pediatric Hematology Oncology, 42 (1): 29-35
Hori, H., Ohta, A., Matsui, H., Yano, K., Morita T., Miyuki, LZ., Masumoto, D.(2022). Changes of cancer diagnosis disclosure to children in Japan in the last 20 years, International Journal of Clinical Oncology, 27 (1): 245₋2527.View
Tanaka, K. (2018). Kotsunikushu ni taisuru Kagakuryouhou (Chemotherapy against Osteosarcoma), The Japanese Journal of Pediatric Hematology Oncology, 55(2): 159₋162
Japanese Nursing Association. (2023). Certified Nurse Specialist, https://www.nurse.or.jp/nursing/qualification/vision/ cns/index.htmlView
Japan Association of Nursing Programs in Universities. (2023). Advanced Practice Nurses Information, https://www.janpu. or.jp/activities/committee/cnsnp/View
Wakao, F. (2021). Shonikanja Taikenchousa Houokusho Reiwagannendo Chousa (Research Report on Experiences of Patients with Pediatric Cancers 2021 Report). National Cancer Research Center Commissioned Project from the Ministry of Health, Labour, and Welfare
Japanese Society of Pediatric Oncology Nursing. (2023). Pediatric Oncology Nursing Guideline, http://jspon.sakura. ne.jp/blog/download/jspon_guideline/View
Koizumi, O. (2018). Gan wo Kakaeru AYA Sedai no Kodomo to Kazokukango: Kotsunikushu wo Hasshoshita 15sai no Kodomo to Kazoku heno Kainyu (Children in Adolescent and Young Adult with Cancer and Family Nursing: Intervention on a 15 year Old Child Developed Osteosarcorma and Her Family), The Japanese Journal of Child Nursing,Monthly,41 (10): 1277–1282.
Yamauchi, N. (2016): Consulting activities: Models and skills from the nurse's point of view, The Japanese Society of General Hospital Psychiatry, 28 (4), 324–331.View
Takemura, K. (2009): Chimu wo Enpawamento suru Apurochi (Team Empowerment Approach), Kazoku Kango,7 (2), 7–23.
Chika S., Ryoko U., Ritsuko O., Megumi N., Keiko H., Momoko S.(2015). Literature Review Transition of Nursing Method in Japan, Osaka City University Journal of Nursing, 11 (3), 45–53.