
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care Volume 9 (2024), Article ID: JCNRC-194
https://doi.org/10.33790/jcnrc1100194Research Article
Cross Validation of the Post Event-Cardiovascular Risk Perception Survey Instrument among Cardiac Rehabilitation Patients
Kathy Prue-Owens, PhD, RN1*, Laura Smith, MBA-HC, BSN, RRT, CCRP2, Janell Sinclair, BSN, RN, CCRP2, Garvita Thareja, PhD, MS, MHA, PT, CHES3,
1Assistant Professor, Helen and Arthur E. Johnson Beth-El College of Nursing and Health Sciences, University of Colorado Colorado Springs (UCCS), 1420 Austin Bluffs Parkway, Colorado Springs, CO 80918, United States.
2Manager Cardiac/Pulmonary Rehabilitation, UCHealth 175 S. Union Blvd, Suite 230 Colorado Springs, CO 80910, United States.
3Assistant Professor, Department of Health Profession, Metropolitan State University of Denver, 890 Auraria Pkwy, Denver, CO 80204, United States.
Corresponding Author Details: Kathy Prue-Owens, PhD, RN, Assistant Professor, Helen and Arthur E. Johnson Beth-El College of Nursing and Health Sciences, University of Colorado Colorado Springs (UCCS), 1420 Austin Bluffs Parkway, Colorado Springs, CO 80918, United States.
Received date: 01st November, 2023
Accepted date: 04th January, 2024
Published date: 09th January, 2024
Citation: Prue-Owens, K., Smith, L., Sinclair, J., & Thareja, G., (2024). Cross Validation of the Post Event-Cardiovascular Risk Perception Survey Instrument among Cardiac Rehabilitation Patients. J Comp Nurs Res Care 9(1):194.
Copyright:©2024, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Background: By 2035, nearly half of U.S. adults will have some form of heart disease. COVID-19 altered the delivery of care for cardiac rehabilitation patients who experienced a cardiac event.
Objective: To cross-validate the Post Event-Cardiovascular Risk Perception Survey (PE-CRPS).
Methods: A cross-sectional and descriptive study was conducted to validate CVD risk perception survey. Explorative factor analysis (EFA) was utilized to explore the factors, validate the scale, and measure variance in the data.
Results: Of the 261 individuals, majority were males (71%, mean age: 65.77 years), Caucasian-Non-Hispanic origin (94%) with co morbidities (hypertension, hyper-lipidemia and diabetes). EFA identified 16 latent (eigenvalues >1) with 45 observed variables to measure CVD risk perception. Factors explained 68% of the variance. Bartlett’s test of sphericity was significant (p=.001), indicating variances not significant and the factors correlated.
Conclusions: PE-CRPS was valid and can be used to assess cardiac risk perceptions among cardiac rehabilitation individuals.
Key Words: Cardiac Rehabilitation, Psychometric Testing, Cardiac risk Perception
Introduction
By 2035, nearly half of U.S. adults will have some form of cardiovascular disease (CVD), coronary heart disease (CHD) and/or coronary artery disease (CAD) which include modifiable risk factors such as smoking, obesity, high blood pressure, high cholesterol, diabetes, lack of physical activity and an unhealthy diet [1-7]. Although, adhering to national exercise guidelines and a healthy diet can lower rates of morbidity and mortality,[1,2] we know that patients with heart disease fall short of reducing cardiac risk factors or even estimating their risk for further cardiac events [8-13]. Everett and colleagues (2016) indicated that those patients who perceive themselves to be at high risk for heart disease will more likely engage in behaviors to lower this risk [9]. Robinson and colleagues (2018) indicate significant discrepancy in African American women when it comes to the association between CVD risk factors and risk estimation [14]. Others indicate there is a difference in perception of symptoms for myocardial infarction; [15] recognizing a heart attack;[16] and how family members perceive risk during an out-of hospital cardiac arrest and general health [17,18]. Education about how to decrease cardiac risk factors is often the priority for staying heart healthy [1-3,19-21]. However, estimating risk perception as it relates to modifiable cardiac risk factors is limited in the literature; particularly when it comes to addressing cardiac risk factors among individuals with known heart disease.
Mortality rates for heart disease have declined but there is still concern for patients who perceive themselves at risk and will adhere to healthy behaviors and exercise even after participating in a formal cardiac rehabilitation program [14,22-25]. Cardiac risk perception can have a role in cardiac rehabilitation programs, particularly among patients with a known history of heart disease. Sadeghi and colleagues (2018) demonstrated the value of assessing patient’s perception of illness to reduce particularly stress when helping patient’s adherence to cardiac rehabilitation. Stress is one component of cardiac risk factors [26]. Therefore, risk perception must not be limited to individuals before a cardiac event occurs, it must be addressed throughout the spectrum of health. Prue-Owens and colleagues (2023) examined the psychometric properties for an instrument called Post Event-Cardiovascular Risk Perception Survey (PE-CRPS) among hospitalized inpatient and outpatient cardiac rehabilitation patients who had a known history of heart disease. Although individual patient demographic information was not collected, the study found the PE-CRPS reliable and valid but more importantly, participants did not indicate a risk for developing further CVD [27].
COVID-19 had a major impact on the delivery of healthcare; particularly programs where groups of patients met in person. The pandemic has in some sense delayed cardiac rehabilitation standard of care for patients who have experienced post cardiac events such as open-heart surgery, myocardial infarction, stroke and other events [28,29]. The challenge between underestimation of perceived risk for heart disease and delayed care for patients with known heart disease is important because engaging patients with already known heart disease can promote healthy behaviors and lifestyle modifications even after having a post cardiac event [14,25,30-34]. Cardiac rehabilitation has demonstrated value in engaging patients in a formal exercise program, health promotion education and improving quality of life [20,35-38]. However, there is limited research particularly in the United States related to cardiac risk perception among patients with a known history of a cardiac event (as defined by a known history of heart disease) and those who participate in a formal cardiac rehabilitation program. Cardiac rehabilitation programs provide cardiac health education, but risk perception is not a common concept addressed; possibly due to the idea that if a risk of heart disease is already present then there is no need to change behaviors. Perception of cardiac risk should be determined when participating in a cardiac rehabilitation program in order to inform patients about continued risk for heart disease and ensure appropriate management is implemented [26,39-40]. The Health Belief Model by Becker (1974) was used as the framework for how patients perceive their risk perception even for those patients with known heart disease [41-42]. This study was unique in that it examined cardiac risk perception in patients who had a post cardiac event (known history of heart disease) and who participated in a formal cardiac rehabilitation program.
Methods
This was a cross-sectional descriptive study. The purpose of this study was to test the validity of the revised Post Event-Cardiovascular Risk Perception Survey (PE-CRPS) among patients who had a post cardiac event defined as a positive history of heart disease.
Participants and Data Collection
All patients referred to the local healthcare system cardiac rehabilitation program due to coronary artery disease, myocardial infarction, coronary artery bypass surgery, stable or unstable angina and stent/percutaneous transluminal coronary angioplasty (PTCA) were eligible to participate in the study. These diagnoses reflect heart disease and/or a post cardiac event. The inclusion criteria for participants in this study were men and women over the age of 18 with a diagnosis of known heart disease (post cardiac event) and were enrolled in the cardiac rehabilitation program. Those not included in the study were patients with takotsubo, heart failure without coronary heart disease, cardiomyopathy, left ventricular assistance device, mentally incompetent. Informed consent was obtained by a member of the research team. After informed consent, the following demographic data was collected: age, gender, race/ethnicity, height/ weight, BMI, systolic/diastolic blood pressure, smoking history, exercise level, cholesterol level, glucose level, current medications, individual/family health history. Patients then completed the PE CRPS survey. Institutional Review Board (IRB) ethics approval was obtained by the organization’s committee. Due to COVID restrictions, recruitment of subjects was paused with completion of data collection in May 2022.
Sampling
To test the psychometric validity of the PE-CRPS, the participants were recruited from a local major healthcare system cardiac rehabilitation clinic that serves central and southern Colorado. Participants were a convenience sample of n = 261 with diagnosis of known heart disease and/or cardiac event. The PE-CRPS reliability (Cronbach’s alpha .81) and validity was determined in the prior study conducted by Prue-Owens and colleagues (2023) [27].
Measure: PE-CRPS
In addition to demographic information, participants’ perception of developing CVD using the 10-item PE-CRPS were collected. Cardiac risk perception measurement is often identified in the literature using the Framingham 10-year risk score [43] but in this study, a modified psychometric instrument first derived from the original Cardiovascular Risk Perception (CRPS) by authors, Prue Owens, Graham & Ramesh which was first examined in active-duty service members without diagnosis of heart disease [44]. In other words, the CRPS was tested in healthy active young men and women. The CRPS was then modified from its original version to the PE CRPS using the construct “What do you think your chance is of …” as it relates to cardiac risk factors (Figure 1) [27].
Demographic Information
Of the 261 participants who completed the PE-CRPS, majority were males (71%) with mean age of 65.77 years (Std dev = 11.13), Caucasian (90.4%) and non-Hispanic origin (94%) with co-morbidities (hypertension, hyper-lipidemia and diabetes). Approximately 48.7% were nonsmokers while 51.4% were either previous or current smokers. Approximately 66% were physically active and 54% either exercised every day or every other day. Most of the participants (56.7%) walk as a primary method of exercise. Participants mean cholesterol, A1c and glucose was 156.90, 6.12 and 115.48 respectively.
Statistical Analysis
Data was analyzed using Exploratory Factor Analysis (EFA) with direct oblimin rotation and principal component axis [45]. Items such as cardiac risk factors form a scale by having a common underlying construct (cardiac risk perception). EFA helps disentangle the relationship between the items (cardiac risk factors) and determines if these items fit together as a unified concept. Upon analysis or this disentanglement, the underlying dimensionality of a set of items such as cardiac risk factors and perception now become called “factors.” These factors are a weighted combination of items which helps to determine the validity of the overall scale or tool (PE-CRPS). Statistical significance was determined to be a p-value of <.05. Descriptive statistics and exploratory factor analysis were used to analyze data. Data analyses were performed using IBM SPSS Statistics (Version 27) [46]. The reliability was examined using Cronbach’s Alpha coefficients and component relationships similar to the study conducted by Prue-Owens and colleague [27].
Results
To explore the factorial structure of PE-CRPS, all 45 items of the instrument were subjected to an exploratory factor analysis with direct oblimin rotation and principal component axis. The Bartlett’s test of sphericity χ2 (990) = 4580.377, p = .001, indicating that correlation structure is adequate for factor analysis. Kaiser-Meyer Olkin measure of sampling adequacy suggested that our sample was adequate (KMO = .612). The Kaiser’s criterion of eigenvalues greater than 1 yielded a sixteen-factor solution as the best fit for the data, accounting for 68% of the variance. Scree plot had an ideal pattern. Factor loadings of >.30 were included in the final model such as Diabetes, health history, current Medications, exercise, BMI, demographics, cholesterol, blood pressure, stress and diabetes. The results of this exploratory factor analysis are represented in Table 1.
Upon review of the table, there are 45 items that were loaded onto 16 factors. In order to under the results, the authors suggest reviewing each factor in relationship to the respective item or variable. Begin with reviewing the 45-items are on the left side of the table. These items make up the construct of cardiac risk factors. Next, review the 16 factors or what SPSS calls “components” are on the top of the table, 1 through 16. These are based on the Principal Component Analysis and EFA.
Here are how the 16 factors can be explained:
• Factor 1: Examine Table 1, look at column 1 (Factor 1) which had seven items loaded onto Factor 1. The factor loadings reported are the level of age, FM, stress level, ethnic background, cholesterol, high blood pressure and overweight. These seven items relate to each other and are labeled as “chance of cardiac risk factors with age, ethnic background.”
• Factor 2: Examine Table 1, look at column 2 (Factor 2) which had three items loaded onto Factor 2. The factor loadings were all related to physical activity. This factor measured if the participants exercised or not, how many days a week they exercised and which exercise was their primary method to be physically active. This factor was labeled as “physical activity.”
• Factor 3: Examine Table 1, look at column 3 (Factor 3) which had seven items loaded onto Factor 3. The factor loadings were measuring diabetes, history of diabetes, fasting glucose levels, A1C levels, individual health history 1, medication 4 (indicating at least four cardiac medications were taken by the participants). and family health history 1. This factor was labeled as “diabetes risk.”
• Factor 4: Examine Table 1, look at column 4 (Factor 4) which had six items loaded onto Factor 4. The factor loadings were diabetes, body mass index (BMI), weight in pounds, chance of being overweight, HDL level and physical inactivity. HDL and physical inactivity variables are usually associated with high BMI. This factor was labeled as “body weight influences DM and physical inactivity.”
• Factor 5: Examine Table 1, look at column 5 (Factor 5) which had four items loaded onto Factor 5. The factor loadings were cholesterol level, LDL level, HDL level and triglycerides. This factor was labeled as “lipid profile.”
• Factor 6: Examine Table 1, look at column 6 (Factor 6) which had three items loaded onto Factor 6. The factor loadings were height, weight and gender. This item was labeled as “unmodifiable risk factors.”
• Factor 7: Examine Table 1, look at column 7 (Factor 7) which had three items loaded onto Factor 7. The factor loadings were physical inactivity, family health history 3 and 4 (indicating at least four health histories that are cardiac in nature). This item was labeled “modifiable and nonmodifiable risk factors.”
• Factor 8: Examine Table 1, look at column 8 (Factor 8) which has two items loaded onto Factor 8. The factor loadings were race and ethnicity of our participants, based on the definitions by National Institute of Health (NIH). This factor was labeled as “racial identity.”
• Factor 9: Examine Table 1, look at column 9 (Factor 9) which had three items that measured blood pressure. The factor loadings were chance blood pressure, diastolic blood pressure and systolic blood pressure. This factor was labeled as “blood pressure.”
• Factor 10: Examine Table 1, look at column 10 (Factor 10) which had three items loaded onto Factor 10. The factor loadings were triglycerides level and individual health history 3 and 4 (indicating at least four health histories that are cardiac in nature). This factor was labeled “history of hypercholesterolemia.”
• Factor 11: Examine Table 1, look at column 11 (Factor 11) which has two items that loaded onto Factor 11. The factor loadings were individual health history 5 and family history 5 (indicating at least five health histories that are cardiac in nature). This factor was labeled “individual-family history.”
• Factor 12: Examine Table 1, look at column 12 (Factor 12) which has four items that loaded onto Factor 12. The factor loadings were medications 0, medications 1, medications 2 (indicating at least two cardiac medications were taken by the participants) and family health history 2 (indicating at least two health histories that are cardiac in nature). This factor was labeled “medications-family history.”
• Factor 13: Examine Table 1, look at column 13 (Factor 13) which has three items that loaded onto Factor 13. The factor loadings were individual health history, family health history and chance of physical activity. Thirteenth factor has three items with high factor loadings of >.3. A high factor loading indicates health history influenced chance of physical activity. This factor was labeled “health history-chance of physical activity.”
• Factor 13: Examine Table 1, look at column 13 (Factor 13) which has three items that loaded onto Factor 13. The factor loadings were individual health history, family health history and chance of physical activity. Thirteenth factor has three items with high factor loadings of >.3. A high factor loading indicates health history influenced chance of physical activity. This factor was labeled “health history-chance of physical activity.”
• Factor 14: Examine Table 1, look at column 14 (Factor 14) which has three items that loaded onto Factor 14. The factor loadings were chance of using nicotine product, smoking history, chance of physical activity. Chance of physical activity item has a comparatively lower item loading so this factor was labeled “smoking history.”
• Factor 15: Examine Table 1, look at column 15 (Factor 15) which has three items that loaded onto Factor 15. The factor loadings were family health history 1, medications 3 and medications 4 (indicating at least four cardiac medications were taken by the participants). This factor was labeled “family health history medications.”
• Factor 16: Examine Table 1, look at column 16 (Factor 16) which as three items that loaded onto Factor 16. The factor loadings were medication 4 (indicating at least four cardiac medications were taken by the participants, individual health history and family health history. This factor was labeled “health history medications.”
Based on the EFA, the items (cardiac risk factors) fit together as a unified concept and loaded onto 16 in a dimensionality fashion indicating that the PE-CRPS is a valid scale measuring cardiac risk perception. Another approach to validate the PE-CRPS is to examine the eigenvalues in a scree plot. The eigenvalues are equal to the sum of the squared item weights for the factor with an established cutoff point of 1.0 or greater. Based on Table 1 and Figure 2, the 45 items and 16 factors indicate eigenvalues > 1. This number tells the reader how much variance there is in the data and to retain those factors with a eigenvalues greater than 1.0 (Figure 2). Therefore, 16 factors were worthy of keeping indicating the construct of cardiac risk perception.
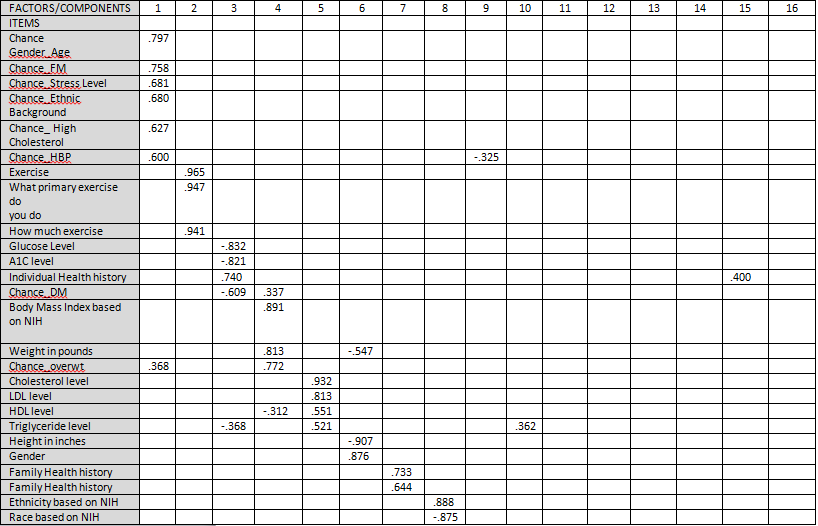
Table 1. Exploratory Factor Analysis Results
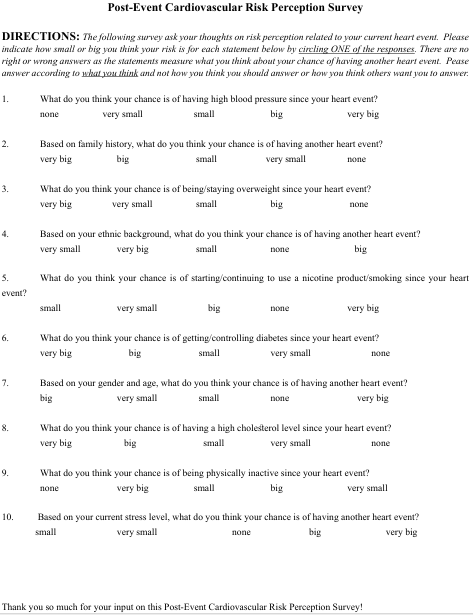
Figure-1. Post-Event Cardiovascular Risk Perception Survey
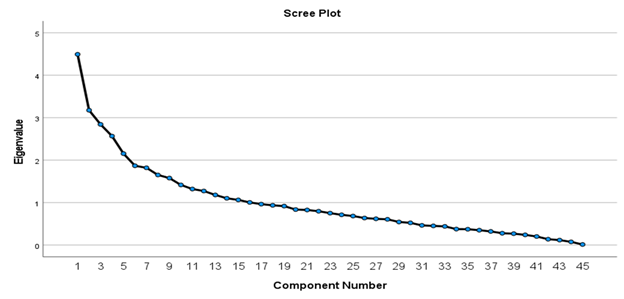
Figure-2. Eigenvalues
Discussion
Testing the PE-CRPS in a larger population with demographic data such as age, gender, health history, family history are important to the validity of a scale particular when engaging patients in cardiac rehabilitation. Similar to authors, Amini et al. and Percy et al., there is value in using the PE-CRPS to patients who already have a history of heart disease [28,29]. Those with a history of heart disease should not be ignored when it comes to estimating their added risk and should be encouraged to change behaviors in order to prevent further development of CVD [25,32]. The PE-CRPS is a validated tool that can be adopted to influence and promote healthy education and quality of life among patients with known heart disease or those who experienced a cardiac event.
Conclusion
Utilizing such a tool as the PE-CRPs could identify areas in which to focus the education to have a positive health outcome. The interdisciplinary team at the Cardiopulmonary Rehabilitation are in a position to identify early in the process of rehabilitation and incorporate it into the Individualized Treatment Plan for each person enrolled in the program. Referrals can also be made to specialty areas, such as diabetes education, behavioral medicine counseling, and tobacco cessation specialist to strategically intervene in assisting with co-morbidities and/or complications.
Acknowledgements:
The authors would like to thank the cardiac rehabilitation patients who participated in this study.
Sources of Funding:
The author(s) declare that there is no funding associated with this project.
Conflicts of Interest:
The author(s) declare there are no conflicts of interest.
Ethical source of approval:
IRB approval from the UCHealth Memorial Hospital COMIRB
References
Tsao, C.W., Aday, A. W., & Almarzooq, Z. I., et al. (2022). Heart disease and stroke statistics—2022 update: a report from the American Heart Association. Circulation. 145(8):e153-e639.View
Centers for Disease Control and Prevention, National Center for Health Statistics. (2022). About Multiple Cause of Death, 1999 2020. CDC WONDER Online Database website. Atlanta, GA: Centers for Disease Control and Prevention. Accessed February 21, 2022. https://wonder.cdc.gov/mcd-icd10.htmlView
Agency for Healthcare Research and Quality (2022). Medical Expenditure Panel Survey (MEPS): household component summary tables: medical conditions, United States. Accessed December 2nd. https://meps.ahrq.gov/survey_comp/household.jspView
Gaalema, D. E., Pericot-Valverde, I., & Bunn, J. Y., et al. (2018). Tobacco use in cardiac patients: Perceptions, use, and changes after a recent myocardial infarction among US adults in the PATH study (2013-2015). Prev. Med. 117:76-82. View
Moxley, E., & Habtzghi, D., (2019). A systematic review comparing dose response of exercise on cardiovascular and all cause mortality. Home Health Care Manag. Pract. 31(4):263-273.View
Riley, H., Headley, A., & Winter, C., et al. (2018). Effect of smoking status on exercise perception and intentions for cardiac rehabilitation enrollment among patients hospitalized with an acute cardiac condition. Journal of Cardiopulm Rehabil. 38(5):286-290. View
Jingjie, W., Yang, L., & Jing, Y., et al. (2022). Sedentary time and its association with risk of cardiovascular diseases in adults: an updated systematic review and meta-analysis of observational studies. BMC Public Health. 22(1):286-295. View
Goff, D. C., Lloyd-Jones, D. M., & Bennett, G., et al. (2014). ACC/AHA guideline on the assessment of cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 63(25):2935-2959.View
Everett, B., Salamonson, Y., Rolley, J. X., & Davidson, P. M.,(2016). Underestimation of risk perception in patients at risk of heart disease. Eur J Cardiovasc Nurs. 15(3):e2-e9.View
Lotfi-Tokaldany, M., Karimi, A., & Shahmansouri, N., et al. (2020). Beliefs, risk perceptions, and lipid management among patients with and without diabetes: Results from the PALM registry. Am. Heart J. 225:88-96.View
O’Donovan, C. E., Skinner, J. R., & Broadbent, E., (2020). Perceptions of risk of cardiac arrest in individuals living with a cardiac inherited disease: Are the doctor and the patient on the same page? Heart Lung Cir. 29(6):851-858.View
Ramirez, F. D., Chen, Y., & Santo, P. D., et al. (2017). Association between self-reported potentially modifiable cardiac risk factors and perceived need to improve physical health: A population based study. Am Heart J. 6(5):1-12View
Fia’Ali’I J, Law, M., O’Donovan, C., Skinner, J. R., & Broadbent, E., (2022). Cultural differences in psychological distress and illness perceptions amongst people living with cardiac inherited diseases. Heart Lung Circ. 31(9):255-1262. View
Robinson, N., Miller, A., Wilbur, J., & Fogg, L., (2018). Subjective versus objective estimated cardiovascular disease risk and adherence to physical activity in African American women. J Cardiovasc Nurs. 33(2):111-117.View
Thomson, P., Angus, N. J., & Andreis, F., et al. (2020). Longitudinal evaluation of the effects of illness perceptions and beliefs about cardiac rehabilitation on quality of life of patients with coronary artery disease and their caregivers. Health Qual. Life Outcomes.18(1):158-172. View
Garrido, D., Petrova, D., & Catena, A., et al. (2020). Recognizing a heart attack: Patients’ knowledge of cardiovascular risk factors and its relation to prehospital decision delay in acute coronary syndrome. Front. Psychol. 11:1-11. View
Gentile, F. R., Compagnoni, A., & Baldi, E., et al. (2021). Out of-hospital cardiac arrest in patients with heart disease from family members’ perspective: high perception of risk, low sense of adequacy and the importance of training. J. Cardiovasc Med. 22(10):790-791. View
Grauman, A., Veldwijk, J., James, A., Hansson, M., & Byberg, L., (2021). Good general health and lack of family history influence the underestimation of cardiovascular risk: a cross sectional study. Eur J Cardiovasc Nurs. 20(7):676-683.View
Epstein, E., Maisel, S., Maysent, K., & Taub, P. R., (2021). Cardiac rehabilitation for coronary artery disease_ latest updates. Curr. Opin. Cardiol. 36(5):556–564.View
Sanchez-Delgado, J. C., Camargo Sepulveda, D. C., & Zapata, A. C., et al. (2020). The effects of maintenance cardiac rehabilitation A SYSTEMATIC REVIEW. J Cardiopulm Rehabil. 40(4):224-244. View
Sallis, J. F., Cerin, E., & Kerr, J., et al. (2020). Built Environment, Physical Activity, and Obesity: Findings from the International Physical Activity and Environment Network (IPEN) Adult Study. Annu. Rev. Public Health. 41(1):119-139.View
McCleary, N., Ivers, N. M., & Schwaim, J. D., et al. (2020). Interventions supporting cardiac rehabilitation completion: Process evaluation investigating theory-based mechanisms of action. Health Psychol. 39(12):1048-1061.View
Chowdhurya, M., Healda, F. A., & Sanchez-Delgadob, J. C., et al. (2021). The effects of maintenance cardiac rehabilitation: A systematic review and Meta-analysis, with a focus on sex. Heart Lung. 50(4):504-524.View
Graham, H., Prue-Owens, K., Kirby, J., & Ramesh, M., (2020). Systematic review of interventions designed to maintain or increase physical activity post-cardiac rehabilitation phase II. Rehabil process outcome. 9:1-14.View
Kreatsoulas, C., Taheri, C., Pattathil, N., Panchal, P., Kakkar, T., (2021). Patient risk interpretation of symptoms model (PRISM): How patients assess cardiac risk. J. Gen. Intern. Med. 36(8):2205-2211. View
Sadeghi, M., Alavi, M., & Mohammadi, M., et al. (2019). Perceptions of illness as predictive factors for perceived stress in patients participating in a cardiac rehabilitation program. Nurs Health Sci. 21(4):508-514. View
Prue-Owens, K., Lindsay, K., & Graham, H., et al. (2023). Post Event-Cardiovascular Risk Perception Survey: Validity and Reliability in Cardiac Patients Post Heart Event. J Nurs. Meas. 31(2):308-320.View
Amini, H., Habibi, S., & Islamoglu, A. H., et al. (2021). COVID-19 pandemic-induced physical inactivity: the necessity of updating the Global Action Plan on Physical Activity 2018 2030. Environ. Health Prev. Med. 26(1):32-34.View
Percy, E., Luc, J., & Vervoort, D., et al. (2020). Post-discharge cardiac care in the era of coronavirus 2019: How should we prepare? Can J Cardiol. 36(6):956-960.View
Mosleh, S. M., & Almalik, M. M. A., (2016). Illness perception and adherence to healthy behaviour in Jordanian coronary heart disease patients. Eur J Cardiovasc Nurs. 15(4):223-230.View
Meloni, A., Pistoia, L., & Maffei, S., et al. (2022). Gender differences in knowledge and perception of cardiovascular disease among Italian Thalassemia major patients. J. Clin. Med. 11(13):3736-3748.View
Mengistu Bekele, D., Yadeta Goshu, D., Worku Yalew, A., Higgins, M. K., & Gary, R. A., (2022). Low subjective cardiovascular disease risk perceptions among hypertensive patients in Addis Ababa, Ethiopia. Integr. Blood Press. Control. 15:81-96.View
Hertz, J. T., Sakita, F. M., & Manavalan, P., et al. (2019). Knowledge, attitudes, and preventative practices regarding ischemic heart disease among emergency department patients in northern Tanzania. J Public Health. 175:60-67. View
Soroush, A., Shams-Alizadeh, N., & Vahdat, A., et al. (2019). Role of perceived heart risk factors by outpatient population in predicting cardiovascular risk. J Cardiovasc Thorac Res. 11(2):100-108.View
Jafri, S. H., Duazo, C., & Imran, H., et al. (2023). Physical and psychological outcomes of patients undergoing traditional cardiac rehabilitation and intensive cardiac rehabilitation. J Cardiopulm Rehabil Prev. 43(1):31-38.View
Grace, A. L., Prior, P. L., & Mamataz, T., et al. (2021). Cardiac rehabilitation component attendance and impact of intervening clinical events, as well as disease severity and risk factor burden. J Cardiopulm Rehabil Prev. 41(1):40-45. View
Sumner, J., Harrison, A., & Doherty, P., (2017). The effectiveness of modern cardiac rehabilitation: A systematic review of recent observational studies in non-attenders versus attenders. PloS one. 12(5):e0177658.View
Friedrich, M., Karof, J., & Hinz, A., (2019). Response shift effects in patients’ assessments of their quality of life after cardiac rehabilitation. Qual Life Res. 28(9):2609–2620. View
Bennett, A. L., Lavie, C. J., & Grace, S. L., (2017). Cardiac rehabilitation following acute coronary syndrome in women. Curr Treat Options Cardiovasc. 19(8):57-67.View
Weinbergen, H., Fach, A., & Meyer, A., et al. (2019). Effects of an intensive long-term prevention programme after myocardial infarction – a randomized trial. Eur J Prev Cardiol. 26(5): 522–530.View
Becker, M. H., The health belief model and sick role behavior. Health Educ. Mongr. 974(2):409-419.View
Becker, M. H., & Kegeles, S. S., (1988). The health belief model and personal health behavior. Med. Econ. 14(3):227-229.
Woringer, M., Jones Nielsen, J., & Zibarras, L., et al. (2017). Development of a questionnaire to evaluate patients’ awareness of cardiovascular disease risk in England’s National Health Service Health Check preventive cardiovascular programme. BMJ Open. 7(9):e014413. View
Prue-Owens, K., Graham, H., & Ramesh, M., (2021). “Would you rather jump out of a perfectly good airplane or develop cardiovascular disease?” Validity and reliability of the cardiovascular risk perception survey among military personnel. J. Nurs. Meas. 29(1):E1-E17. View
Polit, D. F., & Beck, C. T., (2021). Nursing Research: Generating and Assessing Evidence for Nursing Practice. Philadelphia, Wolters Kluwer. View
IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp.View