
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care Volume 11 (2026), Article ID: JCNRC-224
https://doi.org/10.33790/jcnrc1100224Research Article
Implementation of the Montreal Cognitive Assessment (MOCA) Tool for Early Detection of Dementia
Nadege Djeukui DNP, APRN, FNP-BC, CCRN, Shirlean Pelham-Bennett, DNP, RN, CHE, and Chizoba Anako*, DNP, APRN, FNP-C, CNEn, CNEcl
Department of Nursing, Bowie State University, 14000 Jericho Park Rd, Bowie, MD 20715, United States.
Corresponding Author Details: Chizoba Anako, DNP, APRN, FNP-C, CNEn, CNEcl, Assistant Professor, Department of Nursing, Bowie State University, 14000 Jericho Park Rd, Bowie, MD 20715,United States.
Received date: 15th November, 2025
Accepted date: 05th March, 2026
Published date: 07th March, 2026
Citation: Djeukui, N., Pelham-Bennett, S., and Anako, C., (2026). Implementation of the Montreal Cognitive Assessment (MOCA) Tool for Early Detection of Dementia. J Comp Nurs Res Care 11(1):224.
Copyright: ©2026, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
As the population ages, the prevalence of cognitive impairment increases. According to the World Health Organization (WHO), approximately 10 million new cases are reported annually, and over 55 million people worldwide are currently living with dementia, a number projected to increase to 78 million by 2030. Dementia is a growing public health concern that is often underdiagnosed in primary care, leading to missed opportunities for early intervention, care coordination, and patient support. Early detection of dementia is crucial for timely intervention, effective care planning, and enhanced patient outcomes. In our quality improvement (QI) project, we used the Montreal Cognitive Assessment (MOCA) as a standardized cognitive screening tool for adults aged 55 and older in a primary care outpatient clinic to identify patients for cognitive impairment and refer patients for further evaluation. The results indicated a significant increase in the rate of cognitive screening, improved provider confidence in identifying early cognitive decline, and improved referral patterns to specialists for further evaluation. These findings highlight the critical role that healthcare professionals play in identifying dementia early enough, facilitating timely intervention, and ultimately improving patient outcomes.
Keywords: Cognitive impairment, Montreal Cognitive Assessment, Healthcare providers, Neurocognitive disorders, Early detection, Screening tools, and Patient outcomes
Introduction
Dementia is a global health concern, with over 10 million new cases reported annually and over 55 million people worldwide currently living with dementia, a number projected to increase to 78 million by 2030 [1]. Diagnosing dementia early enables the prompt administration of treatment interventions, such as cholinesterase inhibitors and anti-amyloid agents, when they are most effective [2]. A significant gap existed in the systematic use of such tools within primary care settings, leading to missed and delayed detection of dementia [3]. According to Hilsabeck et al. [4], primary care practitioners fail to detect up to 60% of dementia cases, highlighting a critical gap in early identification within primary care settings. While the U.S. Preventive Services Task Force [5] did not recommend routine dementia screening in primary care due to insufficient evidence on the balance of benefits and risks, it acknowledged that cognitive screening tools could help identify early-stage dementia. Early diagnosis contributed to improved management practices, enhanced patient outcomes, and reduced burdens on caregivers and healthcare systems [6]. The challenges of implementing such tools at the primary care level persist, and improvement will require continued effort.
This project was a collaborative initiative to integrate MoCA into routine primary care through a standardized process for patient screening and evaluation. By embedding MoCA into routine visits, the project focused on identifying individuals at risk early and facilitating the timely referral of MoCA-identified individuals to specialists for further evaluation and potential treatment. The first phase involved educating providers using the MOCA tool. The primary intervention was to ensure that all patients aged 55 and older were screened for dementia using the MoCA. Another critical project intervention was implementing a structured referral protocol to support appropriate follow-up. For patients with MoCA scores between 18 and 25, indicating possible mild cognitive impairment (MCI), a follow-up appointment was scheduled within four weeks for repeat testing. This step was to control for external factors, such as stress or sleep deprivation, that may influence initial results [7]. When the repeat score remained below 26, patients were referred to specialists for further assessment. Scores of 17 or below, suggestive of potential dementia, prompted direct referrals to a neurologist, geriatrician, neuropsychologist, or geriatric psychiatrist for comprehensive evaluation. The detailed referral protocol ensured that patients with cognitive concerns received timely and appropriate evaluation. By incorporating cognitive screening into routine primary care, this project shifts the focus from reactive, symptom-driven care to preventive care and early intervention. As Reiss et al. [8] emphasized, early detection and intervention improve patient outcomes and facilitate access to appropriate care and resources.
The MoCA was a 30-point cognitive screening instrument designed to identify early signs of cognitive impairment; scores of 26 or above indicated normal cognition, whereas lower scores suggested decline and warranted further evaluation. The project aimed to achieve 100% screening of adults aged 55 and older within a defined period and 100% referral of patients with abnormal MoCA results for further diagnostic evaluation and treatment.
Background and Significance
Dementia has significant health, social, and economic implications. Without timely detection, dementia could progress, leading to severe cognitive decline, functional impairments, and increased healthcare utilization [9]. This QI project is significant to healthcare because it establishes a clear and standardized protocol for cognitive screening in primary care settings. While earlier stages of this disease persisted among aging populations, the prevalence of dementia presented a significant public health challenge that seriously requires adequate methods of screening and early intervention. The choice of MOCA over other tools, such as the Mini-Mental State Examination and the Saint Louis University Mental Status Exam, was due to its greater sensitivity and specificity in detecting MCI compared to other tools. By proactively integrating MoCA into primary care workflows, healthcare professionals initiated meaningful conversations about cognitive health with patients who might otherwise have hesitated to disclose early signs of cognitive decline. This precision-driven approach enhanced patient care and optimized healthcare resources by targeting interventions for those most likely to benefit from further support or treatment. As emphasized by Harris and Kessels [10], the implementation of early cognitive impairment assessment tools, such as the MoCA, plays a critical role in the early detection of cognitive decline, thereby reducing long-term burdens on individuals and the healthcare system.
Furthermore, the project aligns with Person-Centered Care, focusing on creating a supportive environment that encourages active patient engagement in managing their cognitive health. Collaboration with healthcare providers and key stakeholders at the Family Care Clinic was crucial to implementing and sustaining the MoCA screening tool for the early detection of dementia. Staff education sessions covered dementia symptoms and the importance of early detection, empowering patients to participate in decision-making about their care [11]. By integrating MoCA into routine assessments, providers ensured that cognitive screening became systematic and tailored to each patient’s care plan, strengthening the collaborative relationship between patients and providers.
Review of Literature and synthesis
A comprehensive literature search was conducted across several databases including CINAHL, MEDLINE, PsycINFO, Scopus, PubMed, and Web of Science. Keywords were carefully selected to capture relevant research on dementia screening, early detection, cognitive assessment, and intervention strategies. Search terms included "Dementia," "Montreal Cognitive Assessment (MoCA)," "early detection of neurodegeneration," "brief cognitive tests," "primary care screening for dementia," "cognitive impairment," and "quality outcomes in dementia care.” This search strategy yielded 2,767 articles, and the following five articles were retrieved and deemed most relevant for informing the QI project, meeting the inclusion criteria. These selected articles provide a compelling evidence base, focusing on the utility, validity, and practical implications of cognitive screening tools, such as the MoCA, in primary care settings to improve early detection of dementia.
Fernandes et al. [12] conducted a systematic review examining approaches to enhance dementia diagnosis and management in primary care settings. This review highlights the importance of structured screening protocols and provider training, underscoring the necessity of standardized cognitive assessments, such as the MoCA, for accurate and timely detection. Similarly, Lei et al. [13] conducted a comprehensive review of cognitive assessment tools for detecting MCI and dementia, highlighting the utility of validated instruments, such as the MoCA, in enabling early intervention. The systematic review study by Razak et al. [14] evaluated the validity of various screening tools for dementia and MCI in primary healthcare settings. The review highlighted the MoCA as a particularly effective tool for early dementia detection due to its sensitivity and reliability in identifying cognitive impairment at earlier stages of the disease. The level III study by Bennett and Thomas [15] evaluated the barriers to timely dementia diagnosis faced by primary care physicians, identifying critical factors that impede practical assessment. Davis and Kearns [16] expanded on this theme with a survey of U.S. healthcare providers evaluating dementia assessment practices. The study uncovered significant variability in the dementia assessment protocols employed across primary care facilities. This inconsistency highlighted the critical need for standardized screening tools, such as the MoCA, to promote uniformity in dementia screening practices. These studies all underscore the effectiveness of early detection tools, such as the MoCA, in identifying individuals at risk of cognitive decline. This can significantly improve patient outcomes through timely intervention. The MoCA stands out as a sensitive, valid, and practical tool for detecting early cognitive changes that may otherwise go unnoticed. Literature synthesis highlighted the effectiveness of the MoCA as a reliable tool for early detection of neurodegeneration, particularly in primary care settings. It emphasized the importance of standardized tools and personalized care models in enhancing patient outcomes.
Theoretical Framework for the QI Project
The nursing theory that supported the project was Imogene King’s Goal Attainment, which closely aligned with the practice site’s mission, vision, and values. This theory highlighted the importance of mutual goal setting and collaboration between healthcare providers and patients in improving health outcomes [17]. Its principles were especially relevant for early dementia detection, as success depended on a partnership between healthcare professionals and patients to identify cognitive impairments promptly and implement timely interventions. Within the theory, the interpersonal system emphasized the nurse-patient relationship and effective communication, both of which proved essential for educating patients about the screening process and addressing their concerns or fears about dementia. Furthermore, the social-system element considered broader organizational and community structures, such as healthcare teams and family involvement, which played a critical role in supporting patients after the screening process.
Lewin’s change theory served as the framework for managing the change process in this project due to its adaptability and flexibility for addressing challenges in various settings, employing a staged approach to change management. Lewin’s paradigm of social change emphasized collective decision-making, group ideology, and cultural transformation [18]. His model of change consisted of three steps: unfreezing, changing, and refreezing. During the unfreezing stage, the project manager engaged clinic leadership and staff to abandon informal cognitive assessments and adopt a standardized MoCA protocol. By demonstrating how routine MoCA screening identified at-risk patients earlier, streamlined specialty referrals, and enhanced care planning, the manager highlighted clear clinical and operational benefits. In the change stage, the clinic staff implemented the MoCA tool, with all stakeholders fulfilling their roles. To dispel concerns that screening could increase visits, the project manager maintained clear and ongoing communication to support providers in completing the tool within 10 minutes, thereby avoiding disruptions to the clinic workflow. During the refreezing stage, ongoing evaluation and feedback mechanisms sustained the use of MoCA and integrated it into routine practice. The project lead held regular feedback sessions to reinforce staff confidence, address emerging challenges, celebrate accomplishments, and provide continued education for long-term implementation. By applying Lewin’s model, the project lead systematically identified and managed forces that either drove or resisted change within the clinic setting.
A needs assessment at the practice site revealed inconsistencies in the early detection and management of dementia, as providers used various approaches and tools. This lack of standardization led to gaps in identifying cognitive impairment, potentially delaying timely interventions. Approximately 40% of the target population, adults aged 55 and older, stood to benefit from regular dementia screening. The implementation of the MOCA aligned with the clinic's mission to provide high-quality, comprehensive, and personalized medical care focused on the health and well-being of our community [19]. The facility was dedicated to managing chronic and complex issues while facilitating necessary specialty referrals, underscoring the critical importance of standardized screening and diagnosis of cognitive impairment. This integration of the MoCA into primary practice aimed to enhance early identification and promote timely, guidelinedirected care, thereby supporting improved patient outcomes.
Materials and Methods
This QI project focused on implementing the MoCA screening tool (Appendix 1) to detect dementia early in adults aged 55 and older. The project aimed to introduce MoCA as a routine screening measure in the primary care setting, enabling healthcare providers to detect cognitive impairment in its early stages. Implementing the MoCA screening tool in the primary care clinic lasted 12 weeks. The MoCA tool implementation began by recruiting the clinic’s two nurse practitioners to participate in the project. Then, informed consent was secured from all participants to confirm their voluntary involvement. Phase one began with comprehensive training sessions for providers, focusing on the use of the MoCA tool, scoring protocols, and associated procedures (Appendix 2). An educational handout (Appendix 3) was distributed to support implementation. Before recruitment and training, the project manager had secured the Institutional Review Board approval to ensure full ethical compliance. To ensure adherence to ethical standards, the project coordinator maintained rigorous safeguards to protect human subjects throughout the implementation period. All patients meeting the inclusion criteria were eligible to participate, with no exclusions based on race, gender, ethnicity, or medical diagnosis. The project lead ensured that patient privacy and confidentiality were maintained throughout the project. The team did not collect personally identifiable information such as names, dates of birth, or protected health information beyond MoCA scores and referral actions. Data was collected and securely stored in compliance with HIPAA regulations and the institution’s security policies, ensuring strict patient confidentiality and privacy.
Project Timeline
The implementation of the MoCA screening tool in the primary care clinic took 12 weeks after IRB approval. The project began with the recruitment and training of nurse practitioner providers during weeks one and two. The training emphasized the importance of early detection of dementia and proper administration of the MoCA. During the implementation phase, from week three to week ten, providers used MOCA to screen eligible patients in clinic assessments for adults aged 55 and older. The project leads visited the clinic weekly to gather data and meet with staff to assess progress in implementing the tool and address any challenges that arose. During weeks eleven and twelve, the project manager began data collection and analyzed the results to evaluate the implementation outcomes.
Data Collection
Data was collected using the MoCA, a highly validated screening tool developed by Nasreddine et al. [20] to detect MCI and dementia. The MoCA took 10 to 15 minutes to administer and evaluate critical cognitive domains, including executive function, visuospatial abilities, naming, short-term memory, attention, working memory, language, concentration, verbal abstraction, and orientation. Following administration of the MoCA, providers documented each patient's score, uploaded the completed assessment to the electronic health record (EHR), and provided referral recommendations based on the MoCA results. The project lead conducted chart reviews to collect all results of the complete MOCA assessment. All data was securely organized in a protected Excel spreadsheet stored in an encrypted thumb drive. Subsequent analysis verified that referral practices aligned with project protocols, confirming fidelity to the intervention and supporting timely, appropriate follow-up care for patients.
Data Analysis and Results
Before the implementation of the MoCA tool, cognitive screening within the clinic was inconsistent and lacked structure. Fewer than 8% of eligible patients aged 55 and older received formal cognitive assessments, resulting in missed or delayed identification of cognitive impairment. In cases where cognitive impairment was suspected, specialists were often inconsistent and significantly delayed due to the absence of a standardized protocol. This workflow gap contributed to prolonged diagnostic timelines, delayed interventions, and increased frustration among both providers and patients. The preimplementation workflow lacked a standardized screening process, resulting in missed opportunities for early detection and a critical barrier to timely referral for further evaluation.
During the 12-week implementation period, the project manager evaluated both effectiveness and protocol adherence by conducting systematic chart reviews. Among the targeted population of patients aged 55 years and older seen in the clinic during the implementation period, 178 patients underwent screening. 112(62.9 %) scored in the normal range (26–30); 49 patients (27.5%) scored 18–25, suggestive of MCI; and 17 patients (9.5%) scored below 17, indicating probable dementia. Consistent, all 49 patients with scores in the 18–25 range were scheduled for a repeat MoCA within four to six weeks. At follow-up, 100% of those 49 patients maintained similar scores, and all were subsequently referred for further evaluation. Likewise, 100% of the 17 patients who initially scored below 17 were promptly referred to specialists for further diagnostic assessment. These outcomes reflect full adherence to the established protocol and reinforce the MoCA tool's effectiveness in identifying patients who require further cognitive evaluation.
Provider feedback captured a dramatic shift in comfort and confidence with the MOCA tool following implementation. Confidence in administering, scoring, and integrating the MOCA into routine primary care increased markedly from 15% prior to the rollout to 95% post-implementation (Appendix 4). Clinicians agreed that the assessment still averaged about 10 minutes, remained practical for most appointments, and praised its ability to identify early cognitive impairment, facilitating prompt referrals. Moreover, providers were able to identify cognitive issues early and initiate appropriate referrals. Feedback from the survey included suggestions for improvement, such as allocating a few extra minutes per visit and incorporating the tool into the EHR template. Despite these challenges, all clinicians endorsed continuing the MoCA and proposed raising the screening age to 65 and above, as the data showed that most patients with abnormal results were 65 and older. The providers endorsed continuing to use the MoCA at the facility to screen patients suspected of cognitive impairment.
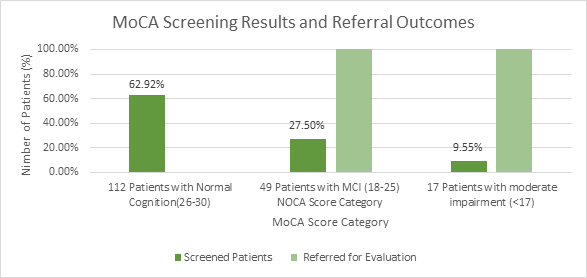
Figure 1: Graph showing total patients screened and MOCA score.
The project's sustainability beyond the 12-week rollout was reinforced by comprehensive provider training, which increased providers' confidence in using the tool. The project manager routinely audited MoCA utilization rates and assessed usability by reviewing weekly reports and provider feedback. The project provided clinicians with easy, consistent access and embedded the MoCA as a standard element of the dementia screening workflow. Because the assessment was user-friendly, took about 10 minutes to complete, and caused minimal disruption, providers felt confident using it to screen for cognitive impairment. The MoCA tool was cost-free, making it a cost-effective and sustainable solution for early dementia detection, ensuring it remains an integral part of routine clinical care. The provider satisfaction survey (Appendix 5) validated its ease of use, clinical relevance, utility, and minor workflow. Clinicians then reported more efficient handoffs, quicker decision-making, and timely specialist referrals, demonstrating that the MoCA was successful when integrated into the workflow and implemented in primary care practice.
The project lead visited the facility weekly during the 12-week implementation phase for the formative evaluation. All stakeholders were engaged throughout the implementation process, ensuring a successful evaluation. Chart review revealed that 178 of 183 eligible patients aged 55 and older were successfully screened with the MoCA tool, resulting in a 97% screening rate. This high rate reflects strong adherence to the screening protocol and effective integration into routine clinical practice. The review also showed that only five eligible patients were missing throughout the project. These missed cases occurred early in implementation and were primarily unscheduled walk-in or same-day acute visits, during which the screening workflow had not yet been fully mastered. To address this gap, the project manager collaborated with the front-desk staff to implement a reminder system, ensuring that MoCA forms were placed in the charts of all patients aged 55 and older before their appointments. As the weeks progressed, clinicians reported that once they gained confidence in administering the workflow, the time required improved to within the targeted 10 minutes. A midimplementation survey revealed that the nurse practitioner found the MoCA to be "easy" to administer and score. This formative evaluation confirmed that embedding the MoCA into clinic workflows, with stakeholder support, was essential to maintaining momentum and achieving high screening compliance throughout the remainder of the project.
At the end of the project, the project manager conducted the summative evaluation to assess the overall project. Chart reviews showed that 97 percent of eligible patients aged 55 and older had been screened during the 12 weeks. Provider surveys showed a steady rise in confidence in administering and scoring the MoCA, with a marked increase from the project's start to its completion. Weekly audits confirmed that the ten-minute, paper-based assessment had not disrupted clinic flow, and having the printed MoCA form readily available in each chart proved invaluable. Overall, the intervention met or exceeded all benchmarks for screening coverage, follow-up, and provider buy-in. By embedding MoCA into routine workflows, the clinic identified cognitive impairment earlier, positioned patients for timely therapies and preventive interventions, and set a foundation for long-term sustainability through minimal ongoing costs, regular audits, and periodic refresher sessions.
Discussion
The QI project was to enhance early identification of cognitive impairment in adults aged 55 and older by implementing the MoCA tool into routine primary care visits. Prior to this initiative, mild MCI and early dementia often went undetected in the facility, resulting in delayed referrals and missed opportunities for timely intervention. A preliminary needs assessment revealed that the clinic lacked a standardized screening tool and exhibited inconsistent follow-up practices. After securing IRB approval for quality improvement, the project manager trained two nurse practitioners to administer the MoCA. Over the 12 weeks, every patient aged 55 or older received a MoCA screen, and those who scored below 26 were referred immediately for specialist evaluation. The MoCA was chosen for its proven sensitivity in detecting MCI, which is higher than that of the Mini-Mental State Examination, and its approximate 10-minute administration time, making it feasible in the primary care setting. Chart reviews demonstrated that 93% of eligible patients received MoCA screening. Of these, 27 percent had scores suggestive of MCI and were referred for further assessment. Post-implementation surveys revealed a 95% increase in provider confidence when identifying cognitive impairment and a notable rise in perceived ease of integrating the tool into daily workflows (Appendix 4). Informal feedback underscored high provider satisfaction and requests to continue MoCA screening beyond the pilot phase. Formative and summative evaluations guided minor workflow refinements, confirming that embedding the MoCA had a minimal impact on clinic flow while significantly enhancing early detection.
Limitations
Although this quality improvement project demonstrated promising outcomes, several limitations should be acknowledged. First, the project was conducted in a single primary care clinic with a small provider group, which may limit the generalizability of findings to larger, more diverse, or multi-site practice settings. Additionally, the sample size, constrained by the 12-week project period, limited the ability to observe trends across demographic or clinical subgroups and to evaluate screening performance over an extended period. Another limitation is the absence of longitudinal follow-up. The project did not track whether patients referred for specialty evaluation ultimately received formal diagnoses of mild cognitive impairment or dementia, limiting the ability to assess the long-term clinical impact of the screening intervention. Furthermore, as a QI initiative rather than a controlled research study, there was no comparison group, limiting the ability to attribute outcomes solely to the implementation of the MoCA. Despite these limitations, the project offers valuable insights into the feasibility and effectiveness of integrating standardized cognitive screening into routine primary care, establishing a strong foundation for future initiatives focused on broader implementation and long-term outcome evaluation.
Future Recommendations
Future recommendations from this project should continue to emphasize the importance of dementia screening in primary care while ensuring that these efforts remain feasible, sustainable, and aligned with clinic workflow realities. Although universal dementia screening is not recommended due to potential concerns about overdiagnosis, unnecessary patient anxiety, and increased strain on primary care, there remains a critical need to identify cognitive impairment early enough for patients to benefit from emerging treatments. Striking an appropriate balance between early detection and workflow burden is essential.
The recent availability of anti-amyloid therapies for individuals with mild cognitive impairment and early Alzheimer's disease further underscores the need for timely and structured screening in primary care [21]. Many patients are not identified until later stages of decline [22]. By the time they reach specialty clinics, they may already fall outside the eligibility window for those anti-amyloid therapies. Strengthening cognitive screening pathways in primary care is, therefore, vital to ensuring equitable and timely access to these new treatment options. Future projects should incorporate a targeted prescreening process using brief questionnaires, risk-stratification tools, or structured clinical triggers to identify patients most likely to benefit from comprehensive cognitive testing. This approach will prioritize its use for individuals at risk or showing early signs of impairment, thereby reducing unnecessary screening among lower-risk groups. In addition, future initiatives should expand standardized cognitive screening to additional primary care clinics to further validate its feasibility and effectiveness across diverse settings. Incorporating structured provider training, periodic competency refreshers, and well-defined referral pathways will be essential to sustaining workflow efficiency and ensuring accuracy over time. Additionally, incorporating a longitudinal follow-up to monitor referral outcomes and track long-term clinical benefits will provide valuable insights into the sustained impact of early screening. These recommendations support the development of a sustainable, balanced, and evidencebased approach to cognitive screening that maximizes early detection, facilitates timely intervention, and minimizes strain on primary care systems.
Conclusion
The implementation of the MoCA as a standardized screening tool within primary care demonstrated that early detection of cognitive impairment is both feasible and impactful. Dementia screening in primary care is an effective means of identifying individuals with cognitive deficits who may require further evaluation, a diagnostic workup, and timely intervention. Although universal screening is not currently recommended, the emergence of new therapies for patients with mild cognitive impairment underscores the growing importance of recognizing cognitive decline at its earliest stages. The project demonstrated that incorporating a targeted, sensitive tool, such as the MoCA, into routine primary care enhances the ability to detect early cognitive changes that might otherwise go unnoticed. High screening completion rates, improved provider confidence, and streamlined referral pathways reflect the value of a standardized approach. By identifying patients earlier and ensuring timely follow-up, primary care practices can support more effective diagnosis, intervention, and long-term management. While the project was limited by scope and duration, its outcomes highlight the significant potential of structured screening protocols to improve early identification, care coordination, and long-term health outcomes for patients at risk of dementia. Sustained screening efforts, combined with ongoing provider education and workflow refinement, have the potential to enhance patient outcomes, support emerging treatment pathways, and improve the quality of dementia care in primary care settings.
Acknowledgments
The authors express their profound gratitude to Dr. Henry Tama of Family Care and Clinic for facilitating the data used in this manuscript and to the consultant, Dr. Shirlean Pelham-Bennett of Purdue University Global, for expert guidance and supervision throughout the development of this work.
Statements and Declarations
Declaration of Conflicting Interests:
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding statement
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and informed consent statements
Purdue University Global consultants and approved by IRB (IRB Application IRB-2024-0000251) on January 14, 2025. Prior to completing the survey, all participants were directed to sign the written informed consent and complete the survey questionnaire if they were at least 18 years of age and voluntarily agreed to participate.
References
World Health Organization. (2023, March 15). Dementia. View
Hafiz, R., Alajlani, L., Ali, A., Algarni, G. A., Aljurfi, H., Alammar, O. A. M., Ashqan, M. Y., & Alkhashan, A. (2023). The latest advances in the diagnosis and treatment of dementia. Cureus, 15(3), e50522. View
Power, M. C., Willens, V., Prather, C., Moghtaderi, A., Chen, Y., Gianattasio, K. Z., Grodstein, F., Shah, R. C., & James, B. D. (2023). Risks and benefits of clinical diagnosis around the time of dementia onset. Gerontology and Geriatric Medicine, 9, 1–10. View
Hilsabeck, R. C., Perry, W., Lacritz, L., Arnett, P. A., Shah, R. C., Borson, S., Galvin, J. E., Roaten, K., Daven, M., Hwang, U., Ivey, L., Joshi, P., Parish, A. L., Wood, J., Woodhouse, J., Tsai, J., Sorweid, M., & Subramanian, U. (2024). Improving early detection of cognitive impairment in older adults in primary care clinics: Recommendations from an interdisciplinary geriatrics summit. The Annals of Family Medicine, 22(6), 543– 549. View
U.S. Preventive Services Task Force. (2020, February 25). Cognitive impairment in older adults: Screening. View
Heintz, H., Monette, P., Epstein-Lubow, G, Smith, L., Rowlett, S., & Forester, B. P. (2019). Emerging collaborative care models for dementia care in the primary care setting: A narrative review. American Journal of Geriatric Psychiatry, 28(3), 320–330. View
McCollum, L., & Karlawish, J. (2020). Cognitive impairment evaluation and management. Medical Clinics of North America, 104(5), 807–825. View
Reiss, A. B., De Levante Raphael, D., Chin, N. A., & Sinha, V. (2022). The physician’s Alzheimer’s disease management guide: Early detection and diagnosis of cognitive impairment, Alzheimer’s disease, and related dementia. AIMS Public Health, 9(4), 661–689. View
Porsteinsson, A. P., Isaacson, R. S., Knox, S., Sabbagh, M. N., & Rubino, I. (2021). Diagnosis of early Alzheimer’s disease: Clinical practice in 2021. The Journal of Prevention of Alzheimer’s Disease, 8(3), 371–386. View
Harris, P., & Kessels, R. (2019). Dementia: Issues in early recognition and intervention in primary care. Age and Ageing, 48(5), 721–725.
American Association of Colleges of Nursing (2021). The essentials: Core competencies for professional nursing education. View
Fernandes, B., Goodarzi, Z., & Holroyd-Leduc, J. M. (2021). Optimizing the diagnosis and management of dementia within primary care: A systematic review of systematic reviews. BMC Family Practice, 22(1). View
Lei, Z., Yang, Y., & Gao, J. (2019). Cognitive assessment tools for mild cognitive impairment screening. Journal of Neurology, 268(5), 1615–1622. View
Razak, M., Ahmad, N., Chan, Y., Kasim, N., Yusof, M., Ghani, M., Omar, M., Aziz, F., & Jamaluddin, R. (2019). Validity of screening tools for dementia and mild cognitive impairment among the elderly in primary health care: A systematic review. Public Health, 169, 84–92. View
Bennett, S., & Thomas, J. (2019). Addressing the challenges of dementia diagnosis in primary care: Perspectives from family physicians and geriatricians. Journal of the American Board of Family Medicine, 31(5), 683-692.
Davis, K., & Kearns, P. (2020). Dementia assessment and management in primary care settings: A survey of current provider practices in the United States. BMC Health Services Research, 19(1), 460.
Park, B. (2021). Effects of nurse-led intervention programs based on goal attainment theory: A systematic review and meta-analysis. Healthcare, 9(6), 699. View
Barrow, J. M., Annamaraju, P., & Toney-Butler, T. J. (2022, September 18). Change management. StatPearls. View
Elite Family Care and Clinic. (2023). Elite Family Care and Clinic. View
Nasreddine, Z. S., Phillips, N. A., Bédirian, V., Charbonneau, S., Whitehead, V., Collin, I., Cummings, J. L., & Chertkow, H. (2005). The Montreal Cognitive Assessment (MoCA): A brief screening tool for mild cognitive impairment. Journal of the American Geriatrics Society, 53(4), 695–699. View
Foley, T., Perry, M., & Robinson, D. L. (2025). Dementia, more than a diagnosis and drugs: perspectives from primary care on the new therapeutic era for Alzheimer’s disease. The Lancet Primary Care, 1(5), 100061. View
Mielke, M. M., Kurzman, H. R., Hu, Y. H., Cho, M., Liss, J., Burns, J. M., Obisesan, T. O., Hornbecker, M., Pallay, A. I., Smith, S. R., Honig, L. S., Parker, M. W., Bell, J., & Hampel, H. (2025b). Advancing early detection of Alzheimer disease in the primary care setting in the United States. Neurology Clinical Practice, 16(1), e200568. View