
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care Volume 11 (2026), Article ID: JCNRC-228
https://doi.org/10.33790/jcnrc1100228Research Article
Psychometric Evaluation of the Political Self-Advocacy Instrument for nursing (PSAI‑N) as an Evidence‑Based Practice Tool
Hetal Desai1 and Brenda Marshall2*
1Professor, William Paterson University, 300 Pompton Road, Wayne, NJ, United States.
2Professor, Montclair State University, 1 Normal Ave, Montclair, NJ 07043,United States.
Corresponding Author Details: Brenda Marshall, Professor, Montclair State University, 1 Normal Ave, Montclair, NJ 07043, United States.
Received date: 17th September, 2025
Accepted date: 18th March, 2026
Published date: 20th March, 2026
Citation: Desai, H., & Marshall, B., (2026). Psychometric Evaluation of the Political Self-Advocacy Instrument for nursing (PSAI-N) as an Evidence-Based Practice Tool. J Comp Nurs Res Care 11(1):228.
Copyright: ©2026, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Nurses play a critical role as patient advocates and are increasingly expected to influence health policy and advance the profession. Effective policy advocacy requires political knowledge, skills, and confidence; however, limited research has examined nurses’ self-efficacy in political self-advocacy. Although leadership and policy engagement are emphasized in professional nursing standards, little is known about nurses’ confidence in participating in political activities that affect their practice. This gap highlights the need for a validated tool to measure political self-advocacy among nurses.
Aim: This study evaluated the effectiveness of the Political Self-Advocacy Instrument for Nurses (PSAI-N) in measuring nurses’ competency levels in political self-advocacy. By establishing the instrument’s psychometric properties, the study sought to confirm the validity and reliability of the tool. A validated PSAI-N provides an evidence-based method for assessing political self-advocacy competencies, identifying areas where nurses may benefit from targeted professional development, and ultimately strengthening nurses’ engagement in policy across all levels of practice.
Methods: A descriptive, correlational design was used. The 49‑item Political Self-Advocacy Instrument for Nursing (PSAI-N) was adapted from the American Society for Pain Management Nursing tool (ASPMN), [1]. Construct validity and reliability testing were conducted. The instrument measures nurses’ beliefs, knowledge, and skills related to political self-advocacy.
Results: Thirty-six advanced practice registered nurses (APRNs) and APRN students completed pre-tests and post-tests. The PSAI-N demonstrated strong internal consistency (Cronbach’s α = .98). Reliability across the five constructs:Personal Advocacy, Public Awareness Advocacy, Nurse Perception Advocacy, Knowledge/Skill Advocacy, and Social/Political Advocacy-ranged from .828 to .965. Knowledge/Skill Advocacy and Nurse Perception Advocacy showed weaker relationships compared to the other constructs. The results demonstrated that only 2.8% of participants reported feeling comfortable with political skills and engagement.
Conclusion: Advocacy and policy skills are essential for nurses to effectively advocate for patients, the profession, and the healthcare system. The PSAI-N shows strong psychometric potential as a standardized, evidence-based tool to measure political self-advocacy and guide targeted professional development.
Key words: Nursing Self-advocacy, Advanced Practice Registered Nurses, Political Advocacy, and Instrument Development.
Introduction
Advocacy has long been recognized as a core component of nursing practice, historically centered on protecting patients’ rights and ensuring safe, ethical, and effective care [2-4]. As the healthcare environment becomes increasingly complex, the expectations for nurses increases beyond bedside advocacy to include influencing organizational, state, and national health policy. The Future of Nursing 2020–2030 report emphasizes that strengthening the nursing workforce’s capacity to lead and advocate is essential to achieving health equity and improving population health outcomes [5]. This includes preparing nurses at all levels to participate in political processes, shape legislation, and advance the profession’s scope of practice.
Despite these expectations, evidence suggests that many nurses lack confidence, preparation, and self‑efficacy in political engagement. Studies show that advocacy skills improve when nurses are exposed to advocacy experiences during their education, yet political participation remains limited across the profession [6]. Nurses with advanced degrees are more likely to engage in political activities, but overall political involvement among nurses remains low [7]. This gap is concerning given that nursing practice is regulated at the state level, where political decisions directly influence scope of practice, workplace conditions, and patient care delivery.
Advocacy has evolved from an individual-level activity to a broader professional responsibility that includes influencing systems, organizations, and public policy [8]. The American Nurses Association [9], identifies advocacy as a professional duty, and the International Council of Nurses recognizes it as a guiding principle of nursing practice [10]. As healthcare systems shift and the roles of Advanced Practice Registered Nurses (APRNs) expand, political self-advocacy becomes increasingly important for ensuring that nurses can effectively shape policies that impact their practice, their patients, and the healthcare system as a whole [11].
However, while the importance of political advocacy is well established, there is limited empirical research examining nurses’ political self-efficacy; their confidence in their ability to engage in political action. Without a clear understanding of nurses’ strengths and gaps in political self-advocacy, it is difficult for educators, organizations, and policymakers to design targeted interventions that build these competencies. A major barrier to advancing this area of research has been the absence of a validated, nursing-specific instrument to measure political self-advocacy.
Political advocacy
For the purpose of this study, political advocacy is defined as the actions nurses (RNs and APRNs) take to influence policies, legislation, and regulatory decisions that affect nursing practice and patient care [12,13]. It encompasses the skills required to navigate political systems, engage with policymakers, and participate in decisions that shape the conditions under which nurses practice.
Although policy engagement is embedded in professional nursing standards, research consistently shows that nurses are often not adequately prepared to possess the political knowledge, skills, and confidence needed for effective participation [4,8]. Contemporary studies highlight that political advocacy is essential for advancing equitable health policies, improving workplace conditions, and addressing systemic barriers that impact patient outcomes [3]. Effective political advocacy also relies on interdisciplinary collaboration and collective action, enabling nurses to contribute meaningfully to policy development at local, state, and national levels [14].
Political Self-Advocacy
Political self-advocacy refers to a nurse’s ability and confidence to influence policies, legislation, and organizational decisions that shape nursing practice and patient care. It involves recognizing one’s professional voice, understanding the political landscape, and taking action to advance the interests of nurses and the populations they serve. As healthcare systems evolve, political self-advocacy has become essential in the advocacy role, enabling nurses to address structural barriers, promote equitable policies, and strengthen the profession’s influence in decision-making [4,13]. Strengthening nurses’ political self-advocacy is therefore critical to advancing the profession and shaping the future of healthcare.
Political Advocacy in Nursing for APRNs
A fundamental aspect of the APRN’s role: is to gain knowledge of patients, promote self-determination and improve patient self-care through advocacy [8]. While most research has emphasized advocacy for patient rights, comparatively little attention has been directed toward policy-level advocacy or the development of nurses capacity for self-advocacy [8,12,15]. Advocacy is defined as the promotion of change, enabling practitioners to highlight areas of need, address gaps in health care and contribute to improved health outcomes. Chiu et al [8], identifies much of the literature examining policy advocacy of organizations, however little has been devoted to nurses’ involvement in the social-political advocacy among APRNs.
The scope of nursing practice is determined by state Legislatures. At this time, thirty states/territories and the District of Columbia have full practice, fifteen states have reduced autonomy meaning nurse practitioners can perform some of their scope of practice without physician supervision and eleven states have restricted practice, which require physician supervision under restricted practice authority [16,17]. Nursing advocacy reflects nursing empowerment, and especially since COVID-19, this need for empowerment and a voice in policy decisions has become imperative [14]. Unfortunately, many nurses still lack knowledge and skills related to effective advocacy, hindering their efforts to implement change [8]. Unfortunately, there still remain barriers to nurse involvement in advocacy, barriers that discourage nurses from realizing their power to bring about the professional change they desire.
This study adapted the American Society for Pain Management Nursing Survey (ASPMN) “Advocacy Survey Instrument” [1] to develop the Political Self-Advocacy Instrument-Nursing (PSAI-N), a tool designed to measure nurses’ beliefs, knowledge, and skills related to political self-advocacy. The PSAI-N was constructed to align political self-advocacy competencies with Benner’s “From Novice-To-Expert” framework, offering a structured way to understand how these competencies develop across a nursing career. Evaluating the reliability and validity of the instrument addresses a significant gap in the literature by ensuring that the PSAI-N provides an accurate, standardized, and evidence-based method for assessing political self-advocacy within the profession. Establishing strong psychometric properties is essential to ensure the tool can generate meaningful data to guide curricular decisions, target professional development initiatives, and strengthen nurses’ capacity for effective policy engagement. The purpose of this study was to validate the PSAI-N as a rigorous tool for examining nurses’ perceived confidence in political self-advocacy, identifying specific areas requiring strengthening, and informing interventions that build a more politically empowered nursing workforce capable of shaping the future of healthcare.
Methods
Design
A descriptive, correlational design was utilized to determine the psychometric properties of the PSAI-N. The research design included reliability calculations with examination of content validity.
Development of the PSAI-N Instrument
The PSAI-N instrument was adapted from the American Society for Pain Management Nursing Survey (ASPMN) Advocacy Survey Instrument (AASI) with a written permission from the authors: Ware, Bruckenthal, Davis, and O’Conner-Von [1]. In each area that referred to patient’ pain, the concept of political self-advocacy was inserted. The newly developed tool Political Self-Advocacy Instrument-Nursing (PSAI-N) like the AASI, measured five constructs of advocacy: personal advocacy, public awareness advocacy, nurse’s perception about advocacy, knowledge/skills related to advocacy and social/political advocacy.
The PSAI-N questionnaire included 49 items: 9 demographic items, 38 political self advocacy items, and 2 self-identification items; study was conducted twice via pre-test and post test within a two-week interval. The PSAI-N items within the questionnaire were scored on a five-point Likert scale to identify levels of belief, knowledge and skills towards political self advocacy. The Likert scale is a five-level scale that ranges from “strongly agree” to “strongly disagree”. The instrument examined five constructs which included: personal advocacy, public awareness advocacy, nurse’s perceptions about advocacy, knowledge/skills related to advocacy, and social/political advocacy.
Procedure-Data Collection/ Participant Protection
Prior to collecting data, institutional review board approval was granted from a North Eastern Public University in New Jersey. The study participants consisted of the students enrolled in an advanced nurse practitioner (APRN) program and nurses with advanced nurse practitioner (APRN) degrees. Informed consent was emailed to participants and verbally provided in the classroom setting. The PSAI-N surveys were distributed via an online database (Survey Monkey) and by pen and paper in the classroom setting. Completed online surveys were password protected, and paper surveys were locked in a cabinet accessible only by the researcher. All responses were aggregated for evaluation.
Data Analysis
Responses were entered into Statistical Package for the Social Science (SPSS) Statistics for Windows version 21 (IBM corps). The descriptive statistics of the sample analyzed the frequency distributions of the demographic variables such as: gender, age, ethnicity, years of experience as a registered nurse, years of experience as APRN, type of practice setting, practice specialty, and education preparation such as the highest level of education. The psychometric properties of the instrument were examined; specifically, the content validity and measures of reliability: Cronbach Alpha Coefficient, Inter-Item correlation coefficient, and test-retest reliability. This study also identified the Benner stages (novice to expert) of the participants by examining a frequency distribution of item 8 examining the level of experience in politics. The content validity of the instrument was examined by two experts who hold increased experience within the discipline of political advocacy.
Results
A total of 172 survey instruments were distributed to APRN students and faculty from a university in the North-eastern region of the United States of America. Respondents who met the inclusion criteria had their surveys included in the PSAI–N pilot study. Fifty-one participants responded to the pre-test via the online invitation, and twenty-one responded to the pre-test via the pen/paper method, totaling 72 respondents. After a two-week period, the surveys were redistributed for post-testing. Thirty three subjects responded to the post-test online, while twenty-one completed the pen/paper post-test, resulting in 54 responses. Thirteen participants who took the survey online did not complete both the pre-test and post-test, and five pen/ paper respondents also failed to complete both. In total, 36 subjects (n=36) met the inclusion criteria for the pilot study and completed both pre and post-tests.
Sample Demographics
The majority of the respondents were females 83.3% (n=30). The participant’s ages ranged between 18 and 64. Participants age 35 to 44 category comprised the largest group 30.6% (n=11) and fewer respondents were in the 18 to 24 age group 5.6% (n=2) (Table 1). The years of RN experience ranged from less than 5 years to greater than 31 years. 25% (n=9) of participants reported more than 11 to 20 years of RN experience, and 16.7% (n=6), which yielded equivocal in more than 21 to 30 years and more than 31 years of RN experience group (Table 1). The years of APRN experience ranged from fewer than 5 years to more than 31 years. The majority of the participants had less than 5 years of APRN experience which yielded 38.9% (n= 14). The highest level of education was at the rate of 38.9% (n=14) had a master’s degree (Table 1). The type of practice setting ranged from hospital setting, own private practice, physician owned practice and retail setting. The majority of respondents were employed in hospital settings 52.8% (n=19) (Table 1). Specialty certification consisted of family, acute care, geriatric, psychiatry, adult, pediatric, and nurse anesthesia. The majority of twenty-five percent (n=9), were Adult certified APRN (Table 1).
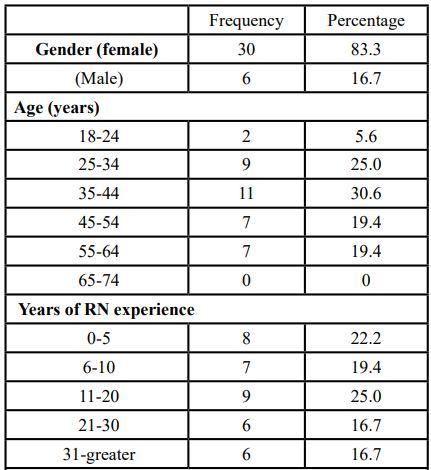
Table 1: Demographics-Sample Description (n = 36) Characteristic
Test-retest Reliability Correlation-Pre/Post-test
A Pearson correlation coefficient was calculated demonstrating the relationship between test results from the two test administrations (pre/post-test) with an interval of two weeks. The test-retest reliability was calculated to examine if the two tests (pre/post-test) remained constant over time, a coefficient reliability of .883 was obtained (Table 2). A moderate statistically significant positive correlation was found between pre and post-test responses (r (34) = .883, p < .001).
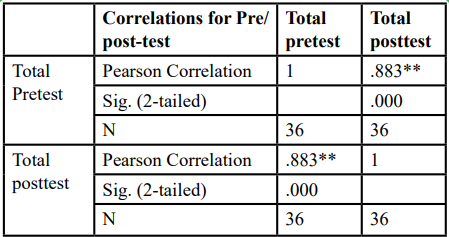
Table 2: Test-retest Reliability
Instrument Reliability Results
The PSAI-N demonstrated a strong reliability, A Cronbach’s Alpha Coefficient was calculated at .98 for the PSAI-N tool. The 5 constructs used to develop to define APRN Political Self Advocacy are: Construct 1: Personal Advocacy, Construct 2: Public Awareness about Advocacy, Construct 3: Nurse Perception about Advocacy; Construct 4: Current Knowledge/Skill about Advocacy, and Construct 5: Social/Political Advocacy. The reliability coefficient for all five constructs for pre-test/post-test ranged from .828 to .965 (Table 3).
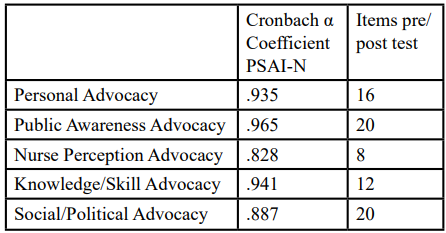
Table 3: Cronbach's Alpha Coefficient PSAI-N: 5 constructs of advocacy
Inter-Item Correlation for PSAI-N
The Inter-Item correlation examined the reliability of each item within the 5 constructs of PSAI-N tool (Construct 1: Personal Advocacy, Construct 2: Public Awareness about Advocacy, Construct 3: Nurse Perception about Advocacy, Construct 4: Current Knowledge/Skill about Advocacy, and Construct 5: Social/ Political Advocacy). This study demonstrated significant reliable relationships within constructs 1-4. It revealed nurses are capable of engaging in advocacy activities within their practice setting such as involvement in political self-advocacy activities, nurses perception related to their advocacy role and knowledge and skills related to advocacy activities. However, construct 5 which examined the level of nurses’ experience in social and political advocacy demonstrated multiple weak relationships. The results yielded APRNs had a lack of comfort in voting practices, speaking to the political leaders and understanding the disciplinary process at the workplace (Table 3).
Level of experience in politics and political advocacy
The level of nurses’ experience in politics and political advocacy was examined using Benner’s Novice to Expert Model, which outlines five progressive stages of professional development: novice, advanced beginner, competent, proficient, and expert [18]. Applying this framework to political self-advocacy provides a structured way to understand how nurses develop confidence and skill in navigating political processes.
At the novice stage, nurses typically have no political experience and rely heavily on rules, external guidance, or formal instruction. Advanced beginners may have limited exposure to political activities such as attending a legislative event or contacting a representative but often lack the deeper insight needed to identify long-term political goals and are generally hesitant to take independent action.
Nurses at the competent stage begin to demonstrate more deliberate engagement. They may participate in organizational advocacy efforts, understand basic policy issues, and feel increasingly capable of contributing to political discussions. Proficient nurses show a broader understanding of the political landscape, can anticipate policy implications, and often take initiative in advocacy activities, such as joining professional organizations or supporting legislative campaigns.
At the expert level, nurses possess a high degree of political self-efficacy. They demonstrate confidence in influencing policy, navigating complex political environments, and leading advocacy initiatives at local, state, or national levels. Expert political advocates often mentor others, contribute to policy development, and serve as influential voices within professional and legislative arenas.
Using Benner’s Novice to Expert model to conceptualize political self-advocacy highlights the developmental nature of political competence and underscores the need for tools such as the PSAI-N to assess where nurses fall along this continuum and identify opportunities for targeted growth.
The majority of respondents 36% (n=13) reported having had no experience, 28% (n=10) had exposure with little experience, 22% (n=8) had limited experience, 11% (n=4) had moderate experience, while only 2.8% (n=1) are at the expert level and is connected with political positions and skills (Table 4).
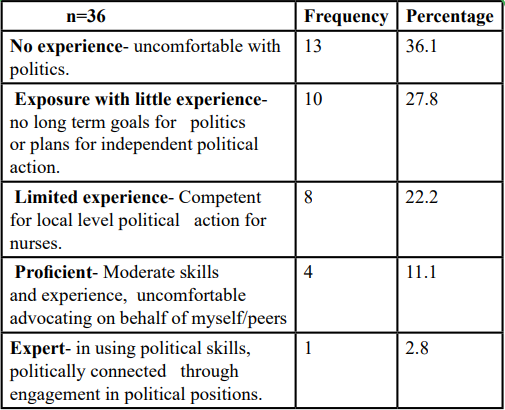
Table 4: Demographic Data-Level of experience in politics
Benner’s Novice to Expert Model and PSAI-N scores
The one-way ANOVA was conducted to compare the total score on the PSAI-N survey with the participants’ level of political advocacy experience (Benner’s five levels of experience). This test was analyzed and it revealed a significant difference in scores among the levels of experience (F(4,31) = 5.990, p=.001). One-way ANOVA revealed that the mean score indicating the participants in the novice level scored (m = 97.22, sd = 26.333), participants in the advanced beginner level scored (m = 109.412, sd = 17.038), participants in the competent level scored (m = 84.246, sd = 11.365), participants in the proficient level scored (m = 63.098, sd = 16.416) and participants in the expert level scored (m = 41.061), and were not significantly different from other three groups. A Tukey’s HSD was used to determine the nature of the differences between groups. This analysis demonstrated that the scores from participants differed according to self-identified level of experience (Table 5). The lower the score the least competent the subject was in political self-advocacy.
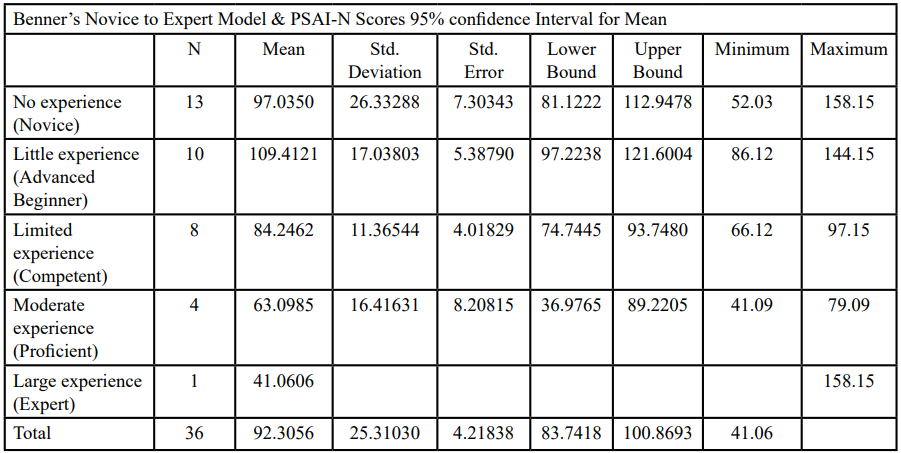
Table 5: Descriptives- One-way ANOVA
Discussion
This study developed and evaluated the Political Self-Advocacy Instrument for Nursing (PSAI-N), the first known tool designed to measure political self-advocacy at the individual nurse level. The literature review identified no existing instruments that assess nurses’ confidence, beliefs, knowledge, and skills related to political self-advocacy, highlighting a significant gap in the measurement of political competence within the profession. Although tools such as the Political Astuteness Inventory (PAI) have been used to assess political awareness and engagement [19], they do not capture nurses’ self-efficacy in advocating for themselves within political and policy-making arenas. The PSAI-N therefore fills a critical void by measuring a distinct and previously unassessed construct.
The PSAI-N consists of 49 items across five constructs Personal Advocacy, Public Awareness Advocacy, Nurse Perception Advocacy, Knowledge/Skill Advocacy, and Social/Political Advocacy. Thirty-six participants completed both pre- and post-test surveys. The sample was predominantly female, aged 35–44, with 11–20 years of RN experience; most were master’s prepared nurse practitioners with fewer than five years of APRN experience working in hospital settings.
Psychometric testing demonstrated strong reliability and validity. The PSAI-N yielded an excellent Cronbach’s alpha of .98, indicating high internal consistency. Inter-item correlations showed strong relationships among four of the five constructs, with weaker correlations in the Social/Political Advocacy domain. This suggests that while nurses may feel confident in personal and professional advocacy, they are less assured in higher-level political engagement. These findings align with prior research using the PAI, which consistently shows that nurses report low political competence and limited political participation despite recognizing its importance [19]. By measuring political self-efficacy rather than political awareness alone, the PSAI-N provides a more actionable assessment of nurses’ readiness to engage in political advocacy.
To contextualize political experience, Benner’s Novice to Expert Model [18] was applied. Most participants fell within the novice stage, indicating minimal exposure to political processes or advocacy activities. This is notable given that many had more than twenty years of nursing experience yet reported limited political efficacy. A one‑way ANOVA comparing Benner’s stages with PSAI-N scores revealed significant differences across experience levels, and Tukey’s HSD confirmed meaningful variation in political self-advocacy based on political experience.
Collectively, these findings highlight a substantial gap in nurses’ political self-advocacy and underscore the need for targeted professional development. The PSAI-N offers a validated, reliable, and nursing-specific tool that can be used alongside broader measures such as the Political Astuteness Inventory (PAI) to more fully assess nurses’ political capacity. By capturing political self-efficacy an essential precursor to political action the PSAI-N provides a foundation for identifying educational needs, designing interventions, and strengthening the nursing profession’s influence on health policy.
Limitations of Study
The limitations of this pilot study included the small convenience sample, which is sufficient for instrument testing but not for participant evaluation and results may not be generalizable. The study was limited to nurses’ either enrolled in a nurse practitioner program or who were already nurse practitioners affiliated within one medium-sized public university in the northeastern region of the United States. The large dropout rate between the pre-test and post-test of 9.2% reduced the final number of participants for evaluation purposes.
Recommendation for Future Research
Political self-advocacy is critical at all levels of nursing practice and education. Nurses who are academically prepared with the skills for political advocacy gain self-efficacy, which translates into improved confidence in engagement in the advocate role [20,21]. When nurses don’t perceive they have political advocacy skills, they will not connect in political engagement and feel uncomfortable advocating on behalf of self and peers. Utilizing the PSAI-N tool to assess nurse’s level of self-efficacy in political engagement can assist academic programs in curriculum development and assessment, organizational identification of gaps in knowledge, beliefs and behaviors, and explore methods to improve political self-efficacy among nursing professionals. Future research can utilize this tool with a larger nursing population to assess the level of political self-advocacy and engage in program development that encourages the voices of nursing in the attainment of the IOM’s mandate of practice to the full extent of nursing education and training.
Conclusion
This study set out to address a critical gap in nursing research: the absence of a validated instrument to measure nurses’ political self-advocacy. By developing and evaluating the Political Self-Advocacy Instrument for Nursing (PSAI-N), this study provides the first evidence-based tool designed to assess nurses’ beliefs, knowledge, skills, and confidence related to political self-advocacy. The PSAI-N demonstrated strong psychometric performance, including excellent internal consistency and construct validity across its five domains, confirming that it is a reliable and valid measure of political self-efficacy.
The study’s findings revealed that despite many participants having extensive clinical experience, most fell within the novice stage of political engagement, highlighting a substantial gap between professional expectations for policy involvement and nurses’ actual preparedness. This reinforces the broader concern identified in the literature: nurses recognize the importance of political engagement but often lack the confidence, skills, and experience to participate effectively.
By providing a standardized method to measure political self-advocacy, the PSAI-N offers a foundational tool for educators, organizations, and policymakers to identify strengths and gaps in nurses’ political competence. The instrument can guide the development of targeted educational programs, leadership initiatives, and professional development strategies aimed at strengthening nurses’ political capacity. Ultimately, enhancing political self-advocacy is essential for empowering nurses to influence health policy, shape the conditions of their practice, and advance the profession’s role in improving healthcare systems.
Utilization of the PSAI-N therefore represents an important step toward building a more politically empowered nursing workforce: one equipped with the confidence and skills necessary to lead, advocate, and shape the future of healthcare at local, state, and national levels.
Competing interests:
All authors have no competing interests when completing this article.
References
Ware, L. J., Bruckenthal, P., Davis, G. C., & O’Conner-Von, S. K. (2011). Factors that influence patient advocacy by pain management nurses: Results of the American Society for Pain Management Nursing survey. Pain Management Nursing, 12(1), 25–32. View
Water, T., Ford, K., Spence, D., & Rasmussen, S. (2016). Patient advocacy by nurses—Past, present, and future. Contemporary Nurse, 52(6), 696–709. View
Heck, L., Carrara, B., Mendes, I., & Ventura, C. (2022). Nursing and advocacy in health: An integrative review. Nursing Ethics, 29(4), 1014–1034. View
Ibrahim, A. M. (2024). Nurses’ ethical responsibilities: Whistleblowing and advocacy in patient safety. Nursing Ethics, 31(7), 1289–1314. View
Institute of Medicine (IOM).(2021). The Future of Nursing Focus on the Scope of Practice. Washington DC: National Academies Press. View
Thomas, T., Martsolf, G., & Puskar, K. (2020). How to engage nursing students in health policy: Results of a survey assessing students’ competencies, experiences, interests, and values. Policy, Politics, & Nursing Practice, 21(1), 12–20. View
Figueira, A., Barlem, E. L., Brum, A., Mattos, L., Barlem, J., & Toescher, A. (2020). Clustering the engagement of Brazilian nurses in political advocacy. Research Square. View
Chiu, P., Cummings, G., Thorne, S., & Makaroff, K. (2021). Policy advocacy and nursing organizations: A scoping review. Policy, Politics, & Nursing Practice, 22(4), 276–296. View
American Nurses Association. (2015). Code of ethics for nurses with interpretive statements. American Nurses Publishing. View
Gandra, E. C., & da Silva, K. L. (2023). Teaching strategies for health advocacy for undergraduate nursing students. Nursing Education Perspectives, 44(2), 92–97. View
Nesime, D., & Belgin, A. (2022). Impact of Education on Student Nurses’ Advocacy and Ethical Sensitivity. Nursing Ethics, 29(4), 899–914. View
Desai, H. (2015). Adapting, developing and testing an instrument for evaluation of psychometric properties of the Political Self-Advocacy Instrument in Nursing (PSAI-N) (Publication No. 1681371076) [Doctoral dissertation, William Paterson University]. ProQuest Dissertations & Theses Global.
Turale, S., & Kunaviktikul, W. (2019). The Contribution of Nurses to Health Policy and Advocacy Requires Leaders to Provide Training and Mentorship. International Nursing Review, 66(3), 302–304. View
Arabi, Y. M., Azoulay, E., Al-Dorzi, H. M., Phua, J., Salluh, J., Binnie, A., Hodgson, C., Angus, D. C., Cecconi, M., Du, B., Fowler, R., Gomersall, C. D., Horby, P., Juffermans, N. P., Kesecioglu, J., Kleinpell, R. M., Machado, F. R., Martin, G. S., Meyfroidt, G., & Rhodes, A. (2021). How the COVID-19 pandemic will change the future of critical care. Intensive Care Medicine, 47(3), 282–291. View
Ellenbecker, C. H., Fawcett, J., Jones, E. J., Mahoney, D., Rowlands, B., & Waddell, A. (2017). A staged approach to educating nurses in health policy. Policy, Politics, & Nursing Practice, 18(1), 44–56. View
American Association of Nurse Practitioners. (2025). State practice environment. View
Feeney, A. (2025). Nurse practitioner practice authority: A state-by-state guide. Nurse Journal.org. View
Benner, P. (1984). From Novice to expert: Excellence and Power in Clinical Nursing Practice. AJN, American Journal of Nursing, 82(3), 402–407. View
Clark, P. E. (1984). Political astuteness inventory. In M.J. Clark (Ed.); Community Nursing: Health care today and tomorrow.
Hardin-Fanning, F., Hartson, K. R., Lynette, G., Gesler, R., & Kern, N. (2023). Socioecological analysis of a nursing advocacy skills-building activity. Journal of Nursing Education, 62(9), 509–515. View
Demirören, N., & Akın, B. (2022). Impact of education on student nurses’ advocacy and ethical sensitivity. Nursing Ethics, 29(4), 899–914. View