
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care Volume 11 (2026), Article ID: JCNRC-230
https://doi.org/10.33790/jcnrc1100230Research Article
The Efficacy of Systematic Voiding Programs to Improve Continence in Post-Stroke Adults: An Integrative Review
Kimberli Martinez, DNP, RN, CRRN, FARN
Clinical Educator, Select Medical Mechanicsburg, Pennsylvania, United States.
Corresponding Author Details: Kimberli Martinez, DNP, RN, CRRN, FARN, Clinical Educator, Select Medical Mechanicsburg, Pennsylvania, United States.
Received date: 29th December, 2025
Accepted date: 25th March, 2026
Published date: 27th March, 2026
Citation: Martinez, K., (2026). The Efficacy of Systematic Voiding Programs to Improve Continence in Post-Stroke Adults: An Integrative Review. J Comp Nurs Res Care 11(1):230.
Copyright: ©2026, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Stroke is a leading cause of disability, with many survivors’ requiring post-acute rehabilitation and experiencing post-stroke urinary incontinence. Functional incontinence is associated with increased falls, skin breakdown, rehospitalization, and mortality, and it can negatively affect mood, quality of life, and discharge destination. The purpose of this integrative review was to determine whether implementing a systematic voiding program can improve functional continence in post-stroke adults. A qualitative integrative approach was used to synthesize findings from primary qualitative research, quasi-experimental and intervention studies, randomized controlled trials, and systematic reviews examining behavioral continence interventions. Sixteen articles met the inclusion criteria. Systematic voiding programs, including timed or prompted voiding and the use of voiding diaries, emerged as first-line strategies for continence promotion compared with pharmacologic and other therapeutic interventions, as they do not confer adverse drug effects. Although systematic voiding programs appear promising, the evidence base is limited by small sample sizes, heterogeneous methods, and a lack of long-term follow-up. Further research using rigorous randomized controlled designs is recommended to confirm effectiveness and optimize implementation strategies in rehabilitation settings.
Key words: Stroke, Urinary Incontinence, Continence Promotion, Rehabilitation Nursing, Behavioral Interventions, Timed Voiding
Introduction
Stroke is a leading cause of disability in the United States, and more than half of stroke survivors require post-acute care services to support functional recovery [1]. Among those admitted to inpatient rehabilitation hospitals, many experience neurogenic bladder and new-onset urinary incontinence, which can lead to falls, urinary tract infections, skin breakdown, and prolonged hospitalizations [2,3]. Incontinence also affects discharge destination, limits the ability to return home, and contributes to depression and reduced quality of life.
Behavioral interventions, including systematic voiding programs, may offer a nonpharmacologic approach to improving continence and safety outcomes in this population [4-6]. However, translation of evidence into practice remains inconsistent and influenced by institutional barriers, staff perceptions, and competing clinical priorities.
A systematic voiding program refers to a structured behavioral continence intervention designed to reduce urinary incontinence through structured toileting and monitoring of voiding programs [5-7]. The purpose of this integrative review was to determine whether implementing systematic voiding programs with behavioral interventions can improve continence in post-stroke adults prior to discharge from post-acute care settings.
Significance of the Practice Problem
Stroke is a leading cause of disability, with more than 50% of survivors requiring inpatient rehabilitation [1]. Post-stroke bladder dysfunction occurs in approximately 30–75% of adults and is frequently under recognized despite its significant impact on patient outcomes [4]. Urinary incontinence is associated with urinary tract infections, falls, skin breakdown, sepsis, rehospitalization, depression, and mortality [3]. Staff burden of care may also increase when continence is not addressed, limiting rehabilitation-focused care and education [5]. Functional outcomes, including bowel and bladder function, are monitored at admission and discharge, and discharge disposition is linked to reimbursement and organizational performance [8]. Continence promotion is therefore a critical component of stroke rehabilitation.
Theoretical Framework
The Knowledge-to-Action Framework guided this review, supporting translation of research into practice through seven cyclical phases addressing problem identification, knowledge adaptation, barrier assessment, intervention implementation, monitoring, evaluation, and sustainability. This framework supports interdisciplinary collaboration, sustained knowledge use, and leadership support to maintain continence initiatives [2,9-11].
Methods
A comprehensive literature search was conducted using PubMed, CINAHL, MEDLINE, and the Cochrane Database of Systematic Reviews to identify studies examining continence promotion interventions for post-stroke urinary incontinence. Boolean search strategies were applied using combinations of the following keywords: continence, continence promotion, systematic voiding, timed voiding, neurogenic bladder, bladder management, urinary incontinence, stroke, and behavioral interventions.
The search initially yielded approximately 100 records across the selected databases. After removal of duplicate records, titles and abstracts were screened for relevance. Studies were excluded if they involved pediatric populations, chronic urinary incontinence unrelated to neurological injury, catheter-dependent populations, non–peer-reviewed literature, or studies not published in English.
Full-text articles were then assessed for eligibility based on predefined inclusion criteria, which included primary research studies, quasi-experimental designs, randomized controlled trials, qualitative studies, and systematic reviews examining behavioral continence interventions in adults following stroke or neurological injury. Studies also required Level II–III evidence with A/B quality ratings and publication within the past five years.
Following full-text review and application of inclusion and exclusion criteria, 16 studies met the final eligibility criteria and were included in the integrative review. The study selection process is illustrated in Figure 1 using the PRISMA 2020 flow diagram.
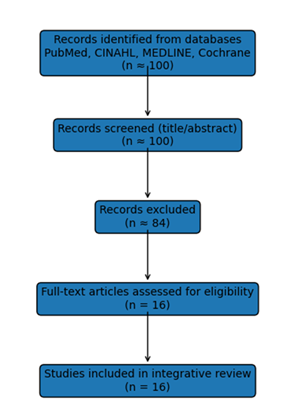
Figure 1
Results: Characterization of the Literature
To evaluate the methodological quality of the included studies, the Johns Hopkins Nursing Evidence-Based Practice (JHNEBP) appraisal tool was used. This tool categorizes evidence based on both level of evidence and quality rating, allowing systematic evaluation of research strength and rigor. Evidence levels were classified according to the JHNEBP hierarchy, with Level I representing experimental or randomized controlled trials, Level II representing quasi-experimental studies, and Level III representing non-experimental or qualitative studies.
Each study was also assigned a quality rating of A (high quality), B (good quality), or C (low quality) based on criteria including study design, sample size, methodological rigor, clarity of results, and consistency with existing evidence. Studies included in this review were limited to those demonstrating Level II or Level III evidence with A or B quality ratings to ensure methodological reliability and relevance to clinical practice.
Following appraisal, 16 studies met the inclusion criteria and were retained for analysis. These studies included qualitative research, systematic reviews, quasi-experimental studies, randomized controlled trials, and intervention studies examining behavioral continence interventions and continence promotion strategies in individuals recovering from stroke or other neurological conditions.
Effectiveness of Interventions
Common interventions included timed or prompted voids, pelvic floor muscle training, behavioral strategies, and pharmacologic options. Systematic voiding programs are consistently identified as foundational, first-line continence strategies due to safety, low cost, and absence of medication side effects [2,4-7]. Programs typically begin with staff education and appropriate patient selection, followed by completion of voiding diaries and initiation of timed voiding every two hours, with gradual interval extension as continence improves [7,12,13].
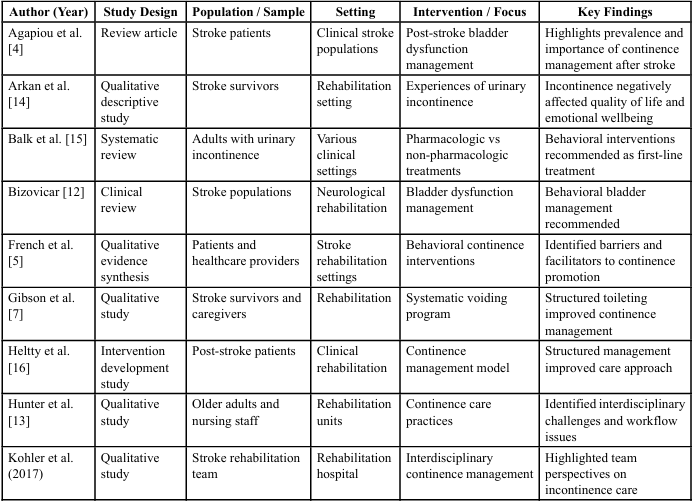
Table 1.
Pelvic floor muscle training demonstrated benefit when paired with timed voiding but was difficult for sustained patient adherence. Pharmacologic interventions demonstrated limited benefit and carried potential adverse effects [15]. Electrical stimulation showed modest benefits but required specialized resources. Overall, behavioral interventions remain the preferred first-line treatment [4,6,15,17].
Patient Perspectives
Patients frequently described embarrassment, shame, and fear of discussing incontinence [16]. Many attempted unsafe self- management strategies such as fluid restriction or limiting activities. Misconceptions existed that incontinence was permanent or unavoidable. Patients reported feeling excluded from care planning; however, when involved in structured programs, they expressed increased control, fewer accidents, and improved quality of life [2,5].
Care Provider Perspectives
Nursing staff reported feeling primary responsibility for continence but lacked interdisciplinary support [13,17]. Barriers included time constraints, staffing limitations, communication gaps, and insufficient knowledge. When interdisciplinary collaboration improved, workflow efficiency increased and continence promotion became proactive rather than reactive [2,7].
Summary of Synthesis
Urinary incontinence after stroke significantly affects quality of life, relationships, safety, and participation. It is frequently under recognized despite prevalence and clinical importance. Patients often lack knowledge and feel excluded from care decisions, while staff encounter knowledge gaps, workload pressures, and communication barriers. When interdisciplinary collaboration improves, systematic voiding programs can be implemented successfully and efficiently, improving continence outcomes.
Implications for Nursing Practice
The implementation of a systematic voiding program provides nurses with a structured, proactive approach to managing urinary incontinence in post-stroke patients. By incorporating scheduled toileting, individualized assessment, and ongoing evaluation of bladder patterns, nurses can promote continence, reduce episodes of incontinence, and enhance patient dignity and comfort. Structured voiding programs also support early identification of urinary dysfunction and allow nurses to intervene before complications such as skin breakdown, urinary tract infections, and decreased mobility occur. Conservative continence strategies including bladder training, timed voiding, and prompted voiding are recommended approaches for managing urinary incontinence following stroke and have demonstrated effectiveness in reducing incontinent episodes and improving bladder control.
In addition to nursing benefits, systematic voiding programs support interdisciplinary rehabilitation goals. Urinary incontinence is common after stroke and is associated with poorer functional outcomes and reduced independence in rehabilitation populations. Predictable toileting schedules may improve therapy participation by reducing interruptions related to urgent toileting needs or incontinence during therapy sessions. Aligning toileting schedules with rehabilitation activities may enable patients to engage more fully in physical and occupational therapy interventions focused on mobility, transfers, gait training, and activities of daily living. Furthermore, systematic continence management interventions implemented in rehabilitation settings have been associated with improvements in continence status and quality of life, highlighting the value of integrating continence management into comprehensive stroke rehabilitation care.
Limitations
This integrative review has several limitations. First, many of the included studies had small sample sizes and the evidence base consisted largely of qualitative research, which may limit the generalization of the findings. Additionally, there was an inconsistency across studies in how systematic voiding programs were defined and implemented, particularly regarding the specific behavioral interventions included. This variability may make replication of interventions and comparison across studies more difficult. Finally, a lack of long-term follow-up in many studies limits understanding of whether improvements in continence were sustained after discharge from rehabilitation settings. Future research using larger sample sizes, standardized intervention protocols, and longitudinal follow-up is needed to better evaluate the long-term effectiveness of systematic behavioral voiding programs.
Conclusions and Contributions to Nursing
Continence promotion should be prioritized in stroke rehabilitation due to its impact on patient safety, recovery, quality of life, and health system outcomes. Urinary incontinence following stroke is associated with increased risk of falls, medical complications, hospitalization, mortality, and psychological distress [2,4,12,18]. Addressing continence requires a multifaceted approach that includes patient engagement, staff education, interdisciplinary collaboration, and organizational support.
Behavioral continence interventions, such as systematic voiding programs, should be integrated into stroke care standards to support proactive continence management. Nurses play a critical role in implementing these programs and should be supported through education, structured communication processes, and leadership engagement. Collaboration between nursing and therapy teams when developing individualized voiding schedules can further enhance outcomes by aligning toileting opportunities with therapy sessions and mobility training, ultimately supporting greater therapy participation and maximizing functional independence during stroke rehabilitation.
Recommendations
The literature supports the implementation of systematic behavioral continence programs, staff and patient education, three-day voiding diary assessments, scheduled voiding every two hours with progressive interval increases, interdisciplinary teamwork, leadership support, and follow-up post-discharge. Additional research is recommended, including randomized controlled trials and long-term follow-up to better understand intervention sustainability and impact.
Author Declaration:
This manuscript is original, has not been published previously, and is not under consideration by another journal. All listed authors have approved the final version of the manuscript and agree with its submission to the Journal of Comprehensive Nursing Research.
References
Pucciarelli, G., Paola, R., Arisido, M., Simeone, S., Vellone, E., & Alvaro, R. (2020). Direct cost related to stroke. Journal of Cardiovascular Nursing, 35(1), 86–94. View
Kohler, M., Ott, S., Mullis, J., Mayer, H., Kesselring, J., & Saxer, S. (2022). Promoting urinary continence in stroke survivors. Nursing Open, 9(2), 1262–1275. View
Kushner, D. S., & Johnson-Greene, D. (2018). Association of urinary incontinence with cognition. Journal of Stroke and Cerebrovascular Diseases, 27(10), 2677–2682. View
Agapiou, E., Efstatios-Stylianos, P., Mavridis, N. L., Meliou, M., & Wimalachandra, W. (2024). Bladder dysfunction following stroke: An updated review on diagnosis and management. Bladder, 11(1). View
French, B., Thomas, L. H., Harrison, J., Coupe, J., Roe, B., Booth, J., Cheater, F. M., Leathley, M. J., Watkins, C. L., & Hay-Smith, E. J. (2017). Client and clinical staff perceptions of behavioral interventions. Journal of Advanced Nursing, 73(1), 21–38. View
Thomas, L. H., Coupe, J., Cross, L., Tan, A., & Watkins, C. (2019). Interventions for treating urinary incontinence after stroke. Cochrane Database of Systematic Reviews, 2. View
Gibson, J., Thomas, L., Harrison, J., & Watkins, C. (2018). Stroke survivors’ and carers’ experiences of a systematic voiding programme. Journal of Clinical Nursing, 27, e107- e116. View
Werner, R., Coe, N., & Wi, M. (2019). Patient outcomes after discharge. JAMA Internal Medicine, 179(5), 617–623. View
Duff, G. (2017). Commentary on knowledge translation: Bridging the disability research-to-practice gap. Research and Practice in Intellectual and Developmental Disabilities, 4(2), 158–163. View
Field, B., Booth, A., Ilott, I., & Gerrish, K. (2014). Using the knowledge-to-action framework in practice. Implementation Science, 9, 172. View
Graham, I. D., Logan, J., Harrison, M. B., Straus, S., Tetroe, J., Caswell, W., & Robinson, N. (2006). Lost in knowledge translation: Time for a map? Journal of Continuing Education in the Health Professions, 26(1), 13–24. View
Bizovicar, N. (2018). Managing lower urinary tract dysfunction following stroke. Current Bladder Dysfunction Reports, 13, 125–131. View
Hunter, K. F., Dahlke, S., Smith, N., Lin, A., Rajabali, S., & Wagg, A. (2021). Older persons’ and staff perspectives on continence. Rehabilitation Nursing, 46(6), 305–314. View
Arkan, G., Beser, A., & Ozturk, V. (2018). Experiences related to urinary incontinence of stroke patients: A qualitative descriptive study. Journal of Neuroscience Nursing, 50(1), 42–46. View
Balk, E. M., Rofeberg, V., Adam, G., Trikalinos, T., & Jeppson, P. C. (2019). Pharmacologic and nonpharmacologic treatments for urinary incontinence in women. Annals of Internal Medicine, 170(7), 465–479. View
Heltty, H., Sitorus, R., Nusdwinuringtyas, N., & Martha, E. (2021). Development of a management model post-stroke urinary incontinence. Pelvic Floor Dysfunction, 3(1), 1–13. View
Kohler, M., Mayer, H., Kesselring, J., & Saxer, S. (2020). Urinary incontinence in stroke survivors. Journal of Clinical Nursing, 29(15-16), 3089–3096. View
Tang, F., Cheng, Z., Wen, X., & Guan, J. (2019). Continuous care intervention. Journal of International Medical Research, 47(5), 2011–2017. View