
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care
Journal of Comprehensive Nursing Research and Care Volume 11 (2026), Article ID: JCNRC-231
https://doi.org/10.33790/jcnrc1100231Review Article
Enhancing Nurse Communication Through Standardized Handoff Practices: A Practice Change Project
Neely R. Chandler, DNP, RN
Assistant Professor, Department of Nursing, Murray State University, 120 Mason Hall, Murray, Kentucky, United States.
Corresponding Author Details: Neely R. Chandler, DNP, RN, Assistant Professor, Department of Nursing, Murray State University, 120 Mason Hall, Murray, Kentucky, United States.
Received date: 26th February, 2026
Accepted date: 14th April, 2026
Published date: 16th April, 2026
Citation: Chandler, N. R., (2026). Enhancing Nurse Communication Through Standardized Handoff Practices: A Practice Change Project. J Comp Nurs Res Care 11(1):231.
Copyright: ©2026, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Effective communication during patient handoffs is essential to ensure patient safety and continuity of care. Miscommunication is a leading cause of preventable medical errors. Standardized handoff tools like I-PASS the BATON offer a structured approach to improve the transfer of information.
Problem: The project site lacked a standardized handoff process, resulting in staff dissatisfaction and frequent information gaps during transitions of care.
Methods: This practice change project utilized a pre-post design to evaluate the impact of the intervention. Patricia Benner’s Novice to Expert theoretical framework and Lewin’s Change Model guided the implementation. Nurse perceptions of handoff quality were assessed through pre- and post-intervention surveys, whereas real-time handoff quality was evaluated by direct observations.
Intervention: I-PASS the BATON was introduced as the standardized handoff tool. Staff received training through workshops and daily huddles. Implementation was supported by hospital leadership and interprofessional collaboration.
Results: Twenty-nine nurses completed the project. There was a statistically significant difference in the Handover Evaluation Scale scores before and after the intervention (p <0.05). Implementation of I-PASS the BATON improved handoff quality in terms of quality of information, interaction and support, efficiency, and patient involvement.
Conclusions: Implementing I-PASS the BATON improved the consistency and quality of handoff communication. Structured training and interprofessional collaboration were key to success. Continued use may contribute to safer patient care and increased nurse satisfaction.
Key words: I-PASS the BATON, handoff communication, transitions of care
Introduction
Ineffective communication during patient handoffs compromises patient safety and the quality of patient care. Nurses perform multiple patient handoffs daily, making precise communication essential for seamless transitions of care. Standardized handoff processes enhance patient safety and continuity of care by reducing communication errors [1]. This project concerns the implementation of I-PASS the BATON (IPB), an evidence-based intervention, to improve healthcare outcomes by enhancing patient safety and increasing the quality of nurse communication. Implementation of structured handoff tools like IPB has been shown to improve the quality of nurse communication and reduce patient harm by up to 70% [1,2]. The practice problem was the absence of a standardized handoff process, resulting in communication gaps, increased risk of errors, and disruptions in patient care. The project's aim was to enhance handoff communication among nurses through the implementation of a standardized process. This manuscript explores an assessment of the problem, the project aim and supporting objectives, the practice question, the evidence-based intervention with synthesis, methodology, theoretical framework, implementation plans, plans for sustainability, barriers, facilitators, ethical considerations, data collection, analysis plan, required resources, budget, results, conclusions, and clinical relevance.
Problem
Handoff communication failures pose a global challenge, significantly impacting patient safety and healthcare outcomes. The World Health Organization [3] indicates that miscommunication during patient handoffs contributes to 80% of serious medical errors. Healthcare organizations worldwide experience increased morbidity and mortality due to ineffective transitions of care, leading to prolonged hospitalizations, readmissions, and increased healthcare costs [3]. Economic effects are extensive with preventable medical errors to the global healthcare system exceeding $42 billion annually [3]. In resource-limited countries, communication failures further stress already resource-limited health systems [3]. Addressing this communication issue with a standardized handoff process is crucial to mitigating adverse outcomes and enhancing the quality of care worldwide.
In the United States, ineffective handoffs continue to be a leading cause of medical errors and adverse patient events. Nationally, it is estimated that 70% of serious medical errors are related to communication failures during care transitions [4]. The Joint Commission Online [5] reported failures in communication were among the top three leading causes for the 1,411 sentinel events reported during the 2023 calendar year, with 18% of these incidents resulting in patient deaths. Howick et al. [6] reported that over 160,000 avoidable deaths occur every year in the United States due to preventable medical errors. Communication failures not only contribute to patient safety events but also impose economic ramifications. Patient safety events account for 15% of hospital expenditures, with the cost of medication errors exceeding $17 billion per year [6]. Economically, these communication failures contribute to significant costs, including $1.7 billion in malpractice claims and extended hospital stays [7]. Nurses, physicians, and other healthcare professionals face heightened workloads and stress due to unclear or incomplete handoffs, impacting care quality, and contributing to burnout [7]. Addressing communication failures with a standardized handoff process is critical to improving patient outcomes and alleviating the financial burden on the healthcare system.
At the project site, the absence of a standardized handoff process was identified as a significant practice issue. Observations, staff feedback, and discussions with hospital leadership indicated frequent inaccuracies and omissions in patient information during transitions of care. Since 2006, the Joint Commission has maintained a standardized handoff protocol as a National Patient Safety Goal to promote patient safety and reduce errors [8]. Research indicates that 67% of communication errors in healthcare are attributed to deficiencies in patient handoffs [9]. The project site’s lack of a standardized approach presented a notable risk to patient safety. Unfortunately, the project site had not shown evidence of addressing this practice problem. Addressing this gap through implementing an evidence-based handoff strategy had the potential to enhance the delivery of safe patient care.
Project Aim and Supporting Objectives
The primary aim of this project was to implement and evaluate the effectiveness of a standardized handoff tool in nursing shift reports to enhance the accuracy, consistency, and safety of handoff communication. The supporting objectives were: (a) assess nursing staff’s knowledge of the I-PASS the BATON handoff tool through pre- and post-training assessments administered before and immediately after structured educational sessions, with a target of achieving a post-assessment score of 90% or higher, (b) evaluate handoff quality before and after the implementation using validated measurement tools, including the Handover Evaluation Scale [10] and the Observation Tool [11] with a goal to demonstrate a 40% improvement in handoff quality scores at eight weeks post implementation, and (c) ensure at least 85% compliance of the use of IPB through systematic audits and staff self- reporting to evaluate adoption and sustainability with compliance monitored weekly over the eight week implementation period.
Practice Question
The following practice question served as the basis for the project: In nurses on a medical-surgical unit, does the implementation of the I-PASS the BATON handoff tool compared with usual practice, impact the quality of handoff communication between nurses over eight weeks?
Evidence-Based Intervention with Synthesis
Evidence-Based Intervention
I-PASS the BATON is a structured handoff tool designed to facilitate transitions of patient care by ensuring complete, consistent, and accurate transfer of information between caregivers [2,11-16]. The mnemonic I-PASS the BATON represents these key elements: I- Introduction: introduction of caregiver and their role; P – Patient: provide the patient’s name and date of birth; A- Assessment: chief complaint, diagnosis, vital signs, and pain score; S- Situation: explain the current patient status, code status, lines, tubes, level of consciousness, and any recent changes; S- Safety: allergies, alerts, critical labs, isolation precautions, fall risk, and pressure injuries; B- Background: comorbidities, current medications, family history; A- Action: orders pending, nursing interventions needed, labs to collect; T- Timing: level of urgency and prioritization of actions; O- Ownership: physician, nurse practitioner, and consulting physician assigned to the patient; and N- Next: plan for the day and for discharge [11]. The IPB handoff tool is a component of the TeamSTEPPS framework, a nationally recognized program with the AHRQ [1], designed to improve teamwork and optimize healthcare communication. Originally introduced in 2008, I-PASS was developed as an evidence-based framework to standardize the exchange of information between caregivers [1]. The tool was later expanded into I-PASS the BATON to incorporate additional components to provide a more comprehensive approach to transitions of care [1].
Evidence Synthesis
This section presents an evidence synthesis of ten research articles supporting the implementation of I-PASS the BATON. The research also highlights I-PASS, a more concise version of IPB, as an effective handoff tool. However, IPB provides a more comprehensive approach, ensuring that all aspects of patient care are thoroughly addressed [1]. The AHRQ [1] advocates for a standardized handoff protocol to ensure consistency and completeness in the transfer of patient information. Ten evidence-based, peer-reviewed research articles published within the last five years were analyzed to evaluate the effectiveness of I-PASS and IPB in improving handoff communication, nurse satisfaction, and patient safety. Two articles were evidence level II, quality A [11,17]. Three articles were evidence level II, quality B [16,18,19]. Three articles were evidence level III, quality A [13-15]. Two articles were evidence level III, quality B [12,20]. The reviewed studies provided a robust evidence base supporting the use of standardized handoff tools like IPB.
Main Themes in the Evidence
Reduction of Patient Safety Events. Structured handoff interventions such as I-PASS the BATON (IPB) significantly improve patient safety by reducing communication errors and adverse events [1,2,12,13,15,17,18,20]. Effective handoffs ensure continuity of care, minimizing information loss during transitions of care [1,12,15,17,18,20]. The standardization and structure of the IPB handoff tool promotes the accurate transfer of information, reducing medication errors, inpatient falls, and pressure injuries [2,12,15,17,18,20]. The research suggests that implementing a structured handoff tool leads to enhanced collaboration, strengthening patient safety efforts [12,14,15,17].
Enhanced Communication and High-Quality Handoffs. Enhanced communication and high-quality handoffs are critical for patient safety, as evidenced by research highlighting the effectiveness of the IPB handoff tool in facilitating an accurate, well-structured exchange of information during transitions of care [11-15]. The Joint Commission [9] and the AHRQ [1] identified communication errors in patient handoffs as a leading contributor to adverse events, underscoring the critical need for standardized approaches such as the I-PASS the BATON handoff tool. Multiple studies highlight improvements in handoff quality, efficiency, and consistency following IPB implementation, with nurses and physicians reporting fewer errors due to omitted or incorrect information [11-17,19].
Improved Nurse Satisfaction. Implementation of the I-PASS the BATON (IPB) handoff tool has significantly enhanced nursing collaboration and teamwork, leading to an increase in job satisfaction [11-16,18]. Enhanced peer interaction and support have led to more accurate, efficient communication about patient status during handoffs [11-16]. The structured format of the IPB tool enables nurses to focus on patient needs with greater confidence, reducing omitted information and reinforcing workflow effectiveness [11-15,18].
Contrasting Elements in the Research
While all the studies acknowledged the benefits of a standardized handoff tool such as IPB, notable variations of the research methodologies were worth highlighting. Some studies were conducted over three to six months to evaluate the immediate effects on communication efficiency and nurse satisfaction [11, 14, 16,18] others were conducted up to three years to identify the long term impact and sustained improvements to patient safety [12,13,15,19]. While some studies included a broad population of nurses across multiple settings [13,15,17,19,20] others focused on specific hospital units [11,12,14,16,18]. Additionally, some studies measured the effectiveness of the intervention through self reports and direct observational audits [11,14,16], others relied solely on self-reports [12,13,15], and others relied solely on direct observations [18,19].
Support for the Evidence-Based Intervention
Extensive research supports the effectiveness of the IPB handoff tool in improving patient safety, communication, the quality of handoffs, and nurse satisfaction, with studies ranging from Level II to Level III [11-20]. Findings consistently demonstrated that a structured handoff protocol such as IPB reduces errors, strengthens teamwork, enhances communication, and improves nurse satisfaction, reinforcing the need for standardized handoff communication in the healthcare setting [11-20]. The extensive research underscored the IPB as a fundamental tool for optimizing nurse communication to improve the quality of patient care.
Methodology
The methodology section of the manuscript contains the essential components that shape the practicum project's foundation. The methodology provides a comprehensive review of the organizational setting, population, translational science model, project management plan, project implementation plan, and plans for sustainability.
Organizational Setting
The project site was a 28-bed medical-surgical unit within a non-profit community hospital in the southeastern United States. The hospital serves a mid-sized rural population and functions as a regional healthcare provider, offering comprehensive services including inpatient and outpatient care, emergency services, oncology, and inpatient hospice care. The patient population spans all age groups and presents with diverse medical needs, including primary care, surgical interventions, chronic disease management, and emergency services. Common diagnoses include diabetes, asthma, chronic obstructive pulmonary disease, hypertension, congestive heart failure, myocardial infarctions, orthopedic injuries, joint replacements, and general surgical conditions.
Each month, the medical-surgical unit accommodates approximately 130 patients, with an average length of stay of 4.36 days. A dedicated interdisciplinary team including physicians, nurses, physical therapists, pharmacists, and social workers collaborates to deliver high-quality, patient-centered care. The interdisciplinary team develops individualized treatment plans aimed at optimizing health outcomes.
Population
The project population included nurses employed in a medical surgical unit at the practicum site. A total of 35 nurses participated in the project's initiation; 29 remained active participants at the project's conclusion. Inclusion criteria for participation required that nurses actively work on the medical-surgical unit and regularly participate in shift handoffs. Exclusion criteria included nurses hired after the start of the implementation process, nurses not actively working on the medical-surgical unit at time of implementation, and nurses who do not regularly participate in shift handoffs. As the IPB handoff tool was considered a standard of care, all nurses assigned to the unit were automatically included in its implementation; informed consent was not required. Enrollment was coordinated with the unit Nurse Director to confirm that all nurses were informed about the project and attended a scheduled educational session.
Translation Science, Nursing Theory, and Project Management Plan
Theoretical Framework
Patricia Benner’s Novice to Expert theoretical framework and Lewin’s Change Model were used to guide the implementation of the I-PASS the BATON handoff tool. Benner’s model outlines five stages of nursing competence novice, advanced beginner, competent, proficient, and expert which ensures nurses receive appropriate support at their respective competency levels as they adopt the new handoff tool [21]. Lewin’s model employs three phases unfreezing, moving, and refreezing that facilitate change through stakeholder engagement, education, implementation, and reinforcement for sustainability [22]. Together, these models provided a structured framework for the successful adoption and implementation of the I-PASS the BATON handoff tool.
Project Implementation Plan
Week 1 Project Implementation Began- Lewin's Unfreezing Phase & Benner’s Novice to Advanced Beginner Stages. One week before the intervention implementation, the project lead promoted the upcoming educational sessions to generate interest and familiarize staff with the IPB handoff tool (see Appendix A). The project lead was present at the unit staff meetings where the Nurse Director introduced the project intervention as a new standard of care. In week one, the project lead conducted comprehensive educational sessions designed to familiarize nursing staff with the purpose and significance of the IPB handoff tool. Educational sessions addressed common handoff challenges, including incomplete information transfer, errors resulting from communication failures, and the benefits of standardized handoff practices. The sessions provided instructions on the steps of the IPB handoff tool (see Appendix B). To accommodate all nursing staff, 60-minute sessions were held at 7:00 am and 7:00 pm on five separate days in the unit’s conference room.
To evaluate the effectiveness of the training, participants completed paper-based pre- and post- education quizzes (see Appendix C), with a target of achieving a score of 90% or higher on the post- assessment administered immediately following the training. For structured pre-implementation data collection, each nurse completed the Handover Evaluation Scale (HES) on paper [10] (see Appendix D). Concurrently, the Nurse Director used a paper-based handoff observation tool [11] (see Appendix E) to document observations during morning and evening handoffs prior to the educational sessions in week one. Permission to use both instruments was obtained from the original authors (see Appendices F and G).
Weeks 2-9: Intervention Implementation Began- Lewin's Moving Stage. During weeks two-nine, the nursing staff used a paper copy of the IPB handoff tool during the morning and evening shift handoffs. The off-going nurse would introduce themselves and the patient, summarize the diagnosis and care plan, describe relevant assessment findings, list outstanding tasks, highlight safety concerns, and offer contingency plans. The process continued with the off-going nurse adding pertinent background information, urgent interventions, timing of tasks, responsible providers, and anticipated next steps. The oncoming nurse then confirmed understanding. The intervention entailed completing the IPB handoff tool in its entirety as designed. The project lead was present at the practicum site two to three times per week to monitor compliance, address staff concerns, answer questions, and offer support. The Nurse Director and charge nurses served as project champions conducting weekly formative assessments using an intervention checklist (see Appendix H). The formative assessment-intervention checklist verified that all IPB components were addressed, confirmed staff comprehension, and ensured the accurate transfer of handoff details. If intervention fidelity fell below 75%, corrective actions would have been implemented to improve IPB adherence, including targeted retraining and individual coaching for staff who need additional support. The Nurse Director and charge nurses' observation of the handoff process provided real- time insights and feedback, reinforcing structured communication, and promoting consistency in the handoff process. The project champions were restricted to supporting the project implementation team and did not serve as a replacement for the project manager. The project lead completed the formative assessment-high level implementation checklist (see Appendix I) weekly to ensure execution of data collection procedures, educational sessions, huddles, and other essential implementation steps, enabling early detection of potential fidelity gaps.
Week 10: Project Evaluation-Benner’s Expert stage and Lewin’s Refreezing phase. In week ten, post-implementation data was collected using paper-based tools: each nurse completed the Handover Evaluation Scale (HES), and the Nurse Director completed the handoff observation tool [10,11]. All pre- and post-summative data were submitted to a statistician for analysis.
Plans for Sustainability
To support sustainability of the practice change initiative, the intervention plan including implementation procedures and both formative and summative evaluation strategies were formally transitioned to key stakeholders. Pre- and post-intervention data, along with statistical analyses, were presented to show the intervention's effectiveness. Ongoing stakeholder engagement and the strategic use of project champions will be critical to fostering continuous improvement and ensuring long-term sustainability.
Barriers, Facilitators, Ethical Considerations
Implementation of the IPB handoff tool required careful planning and strategic execution, as changes within the clinical environment were challenging and met with resistance. The process involved addressing potential barriers, leveraging organizational facilitators, and ensuring adherence to ethical standards to support successful, sustainable project execution [23]. Barriers included staff resistance to change and workflow disruption. Some nursing staff were hesitant to adopt a new handoff tool because it was perceived as time consuming with no added value [24]. Early stakeholder engagement and educational sessions addressed these concerns by emphasizing evidence-based outcomes, improvements in patient safety, and increased nurse satisfaction [11]. To mitigate potential workflow challenges, the project lead and project champions were readily available to support staff, answer questions, and receive feedback from staff.
Facilitators at the project site offered dedicated support for implementing the IPB handoff tool. Key leaders including the Chief Nursing Officer, Director of Quality, and Nurse Director consistently endorsed the structured communication tool, as it aligns with institutional goals and national patient safety initiatives. Leadership remained unchanged since the project’s inception, providing continuity, reliability, and sustained engagement throughout the planning and implementation process. Regular communication and progress updates reinforced transparency and sustained stakeholder engagement throughout the implementation period.
Ethical considerations, including protection of privacy, confidentiality, and data integrity, were foundational to the project [25]. No patient-level identifiable data was collected, and all evaluation metrics were aggregated and de-identified to uphold participant's anonymity. Collected data will be securely stored for seven years on a password-protected computer, to ensure confidentiality and data integrity. These safeguards reinforced the ethical integrity of the project and ensured that the participants’ rights were fully protected. A letter of support was obtained from the project site, affirming that Institutional Review Board (IRB) approval was not required. As the IPB handoff tool is considered a standard of care, informed consent was not required.
Data Collection and Analysis Plan
This project used a pre-post intervention design over an eight-week intervention implementation period to evaluate the effectiveness of the I-PASS the BATON handoff tool in improving the quality of handoff communication between nurses. Data was collected from the nurses on the designated unit before and after the intervention using two instruments: the Handover Evaluation Scale (HES) [10] and the Observation Tool [11]. The HES (see Appendix D), a self-report survey, evaluated the effectiveness of handoff and contains seventeen questions in four subscales including the quality of information, interaction and support, efficiency, and patient involvement. Each survey item was scored on a seven-point Likert scale with higher scores indicating better perceptions of the handover process. The construct validity was confirmed by O’Connell et al. [10]. The researchers first performed exploratory factor analysis (EFA) to examine whether the items formed the intended structure and thereby the construct validity of the tool [10]. Then, O’Connell et al. [10] performed two competing nested models of confirmatory analysis (CFA) to confirm the structure of the subscales and to determine whether the subscales generated using EFA measured one latent construct. The reliability of the tool was confirmed using Cronbach’s alpha analysis with α = 0.80 for quality of information, α = 0.86 for interaction and support, α = 0.67 for efficiency, and α = 0.69 for patient involvement [10].
The Nurse Director collected observational data pre- and post intervention using the Observation Tool [11] (see Appendix E) to evaluate real-time adherence to the I-PASS the BATON elements. The instrument consisted of eleven questions with each item scored on a six-point Likert scale. A higher score indicated a higher quality of handoff. Nemati et al. [11] reported that to determine the validity of the observation instrument, ten nursing instructors approved its construct validity and its reliability was assessed using inter-rater reliability. The Observation Tool was used in the quasi-experimental study by Nemati et al. [11], demonstrating effective application in structured communication evaluations. Permission to use each tool was obtained from the original authors and is included in Appendices F and G.
Intervention fidelity was monitored through formative assessment- intervention checklists completed by the Nurse Director. These checklists verified that all IPB components were addressed, confirmed staff comprehension, and ensured accurate transfer of handoff details. Formative assessment-high level checklists were completed weekly to ensure execution of data collection procedures, educational sessions, huddles, and other essential implementation steps, enabling early detection of potential fidelity gaps.
To assess the effectiveness of the I-PASS the BATON intervention, a statistician conducted data analysis to ensure validity and methodological rigor. The statistician performed Mann Whitney U tests to compare the pre-intervention and post-intervention scores on the HES and Observation Tool. This statistical test was appropriate, as it analyzed two independent groups when the assumption of normality was not met.
Comparison of pre- and post-intervention data from the HES and Observation Tool was used to determine whether the implementation of the IPB handoff tool improved the quality of nurse-to-nurse handoff communication. The statistically significant increase in post-intervention scores indicated an improvement in the quality of handoff communication. These results provided direct evidence of practice improvement and supported the effectiveness of the IPB intervention. These positive findings justified the broader implementation of the IPB handoff tool within the practicum site.
Required Resources and Budget
For the implementation of the I-PASS the BATON handoff tool, several essential resources were required to support successful planning, training, data collection, and evaluation. Education time for nursing staff represented a significant portion of the budget, with one hour of education provided to 32 nurses, calculated at an average hourly wage of $32.00 including benefits, totaling $1024. To support daily use of the tool, printed IPB worksheets were used during the intervention period. Additional materials such as posters and flyers were developed for visual reinforcement, with printing completed by the practicum site’s printshop. A professional statistician was contracted for data analysis to ensure accurate interpretation of the results. Finally, refreshments for the nursing staff during training sessions were provided to support engagement and participation. Each resource is itemized in the budget table (see Table 1), with corresponding revenue support aligned to each expense. This structure ensured that the budget remained balanced and sustainable, yielding a net zero balance.
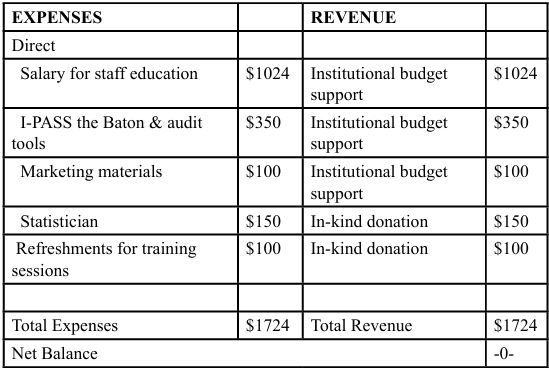
Table 1. Budget
Results
Data was compiled for analysis in a Microsoft Excel™ database after securing site authorization and institutional board review. During the implementation of IPB, the nursing staff used the IPB tool during morning and evening handoffs. The scores for the pre- and post-implementation survey instruments (HES and Observation Tool) were calculated using their associated scoring rubrics. After the subscale and total scores were calculated, the statistical assumption of each score was tested using Shapiro-Wilk tests. When the assumption was violated, non-parametric Mann-Whitney U tests were performed to compare the pre-intervention and post-intervention groups on each subscale and total score [26]. Medians (Mdn) and interquartile ranges (IQR) were reported for each group, per analysis. Statistical significance was assumed at a two-sided alpha value of 0.05, and all analyses were performed using SPSS Version 29 [27].
For the HES total and subscales, the post-intervention group had significantly higher median values versus the pre-intervention group for the HES total score (pre-intervention, Mdn = 4.88, IQR 4.21 – 5.15 vs. post-intervention, Mdn = 6.41, IQR 6.18 – 6.71, p < 0.001), HES – Quality of Information (pre-intervention, Mdn = 5.00, IQR 4.67 – 5.58 vs. post-intervention, Mdn = 6.50, IQR 6.17 – 6.83, p < 0.001), HES – Interaction and Support (pre-intervention Mdn = 5.60, IQR 5.10 – 6.00 vs. post-intervention, Mdn = 6.40, IQR 6.00 – 6.808, p < 0.001), HES – Efficiency (pre-intervention, Mdn = 4.00, IQR 3.33 – 5.00 vs. post-intervention, Mdn = 6.67, IQR 6.00 – 7.00, p < 0.001), and HES – Patient Involvement (pre- intervention, Mdn = 3.33, IQR 2.67 – 4.67 vs. post-intervention, Mdn = 6.33, IQR 6.00 – 6.67, p < 0.001).
Similarly, there were significant increases in the Observation Tool subscales including Introduction (pre-intervention, Mdn = 2.50, IQR 1.00 – 4.75 vs. post-intervention Mdn = 6.00, IQR 6.00 – 6.00, p < 0.001), Patient (pre-intervention, Mdn = 4.00, IQR 3.50 – 4.75 vs. post-intervention, Mdn = 5.50, IQR 5.00 – 6.00, p < 0.001), Action (pre-intervention, Mdn = 3.50, IQR 2.75 – 4.75 vs. post-intervention, Mdn = 5.50, IQR 5.00 – 6.00, p < 0.001), Situation (pre-intervention, Mdn = 4.00, IQR 3.00 – 5.00 vs. post-intervention, Mdn = 5.50, IQR = 5.00 – 5.00, p < 0.001), Safety (pre-intervention, Mdn = 3.50, IQR 2.00 – 5.00 vs. post-intervention, Mdn = 5.50, IQR 5.00 – 6.00, p < 0.001), and The Baton (pre-intervention, Mdn = 4.00, IQR 2.50 – 5.00 vs. post-intervention, Mdn = 6.00, IQR 6.00 – 6.00, p < 0.001). See Table 2 for the descriptive statistics associated with each analysis and Figures 1-11 for graphical depictions of the differences between the groups.
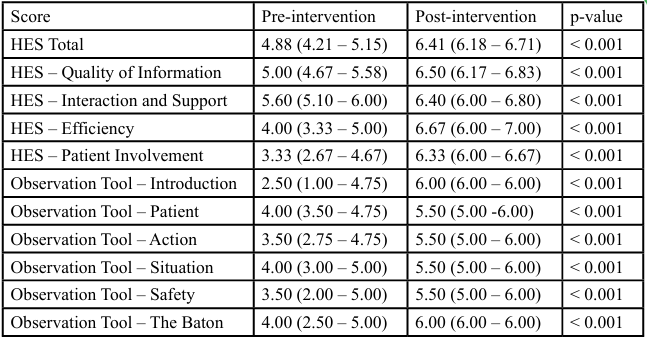
Table 2. Descriptive Statistics for Wilcoxon Signed Ranks Tests
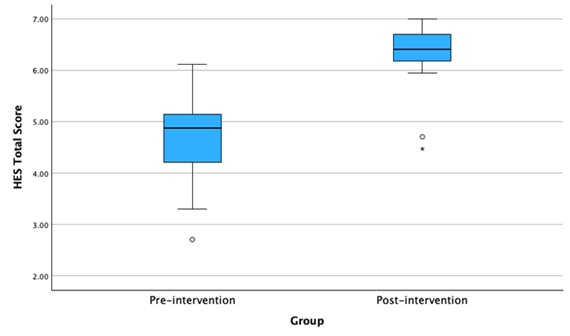
Figure 1: HES Total Score
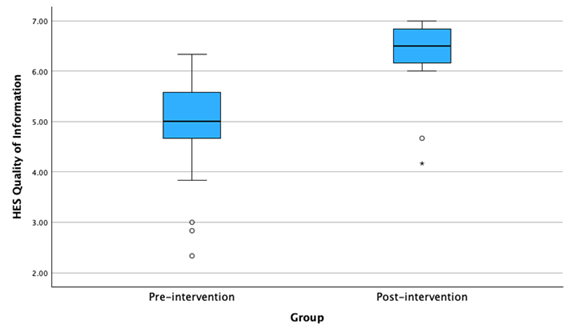
Figure 2: HES – Quality of Information
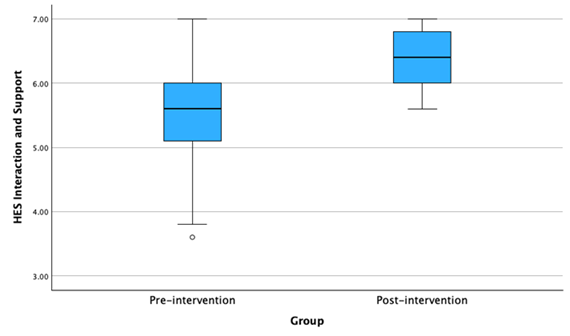
Figure 3: HES – Interaction and Support
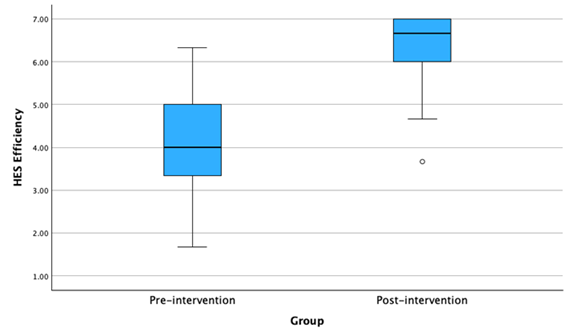
Figure 4: HES - Efficiency
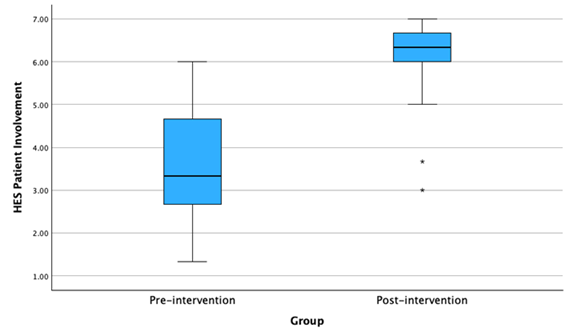
Figure 5: HES – Patient Involvement
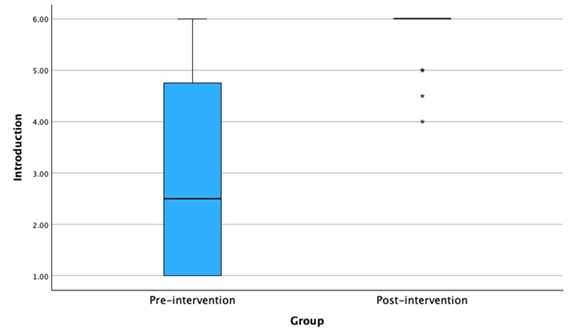
Figure 6: Observation Tool - Introduction
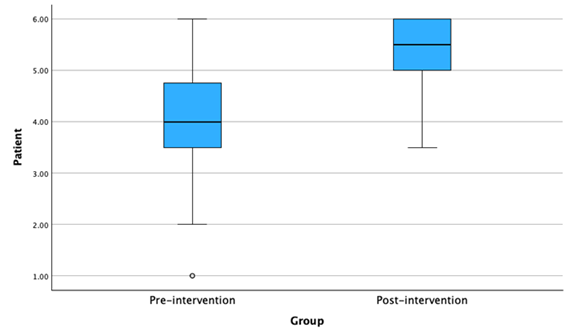
Figure 7: Observation Tool – Patient
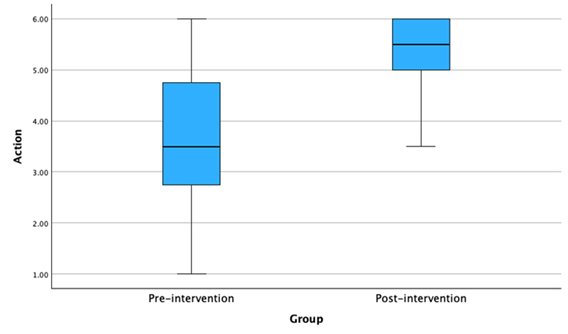
Figure 8: Observation Tool – Action
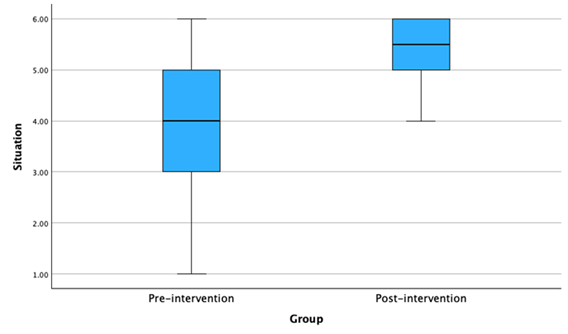
Figure 9: Observation Tool – Situation
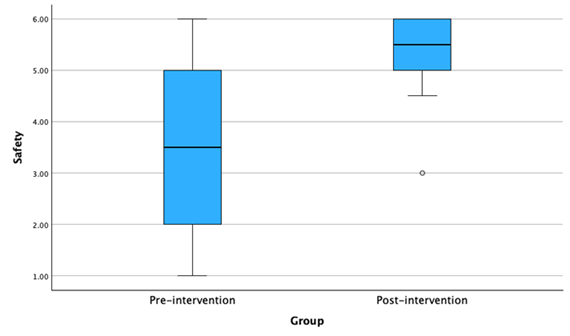
Figure 10: Observation Tool – Safety
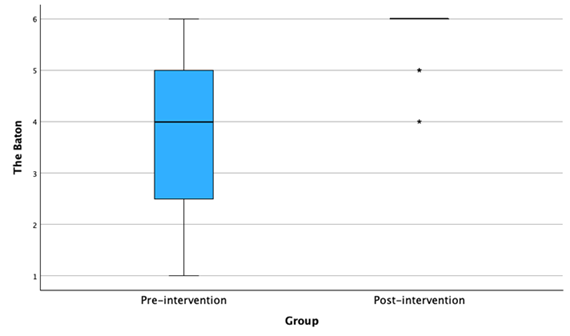
Figure 11: Observation Tool – The Baton
Conclusions
This practice change project aimed to enhance the accuracy, consistency, and safety of handoff communication through the implementation of a standardized process, I-PASS the BATON. The intervention was designed to enhance clarity, consistency, and completeness of information exchange during transitions of care. Analysis of pre- and post- implementation data from the HES and Observation Tool demonstrated a significant increase in post- implementation median scores, indicating significant improvement in handoff quality in terms of quality of information, interaction and support, efficiency, and patient involvement. These findings support the effectiveness of standardized communication tools in advancing patient safety and nurse satisfaction, reinforcing the value of this evidence-based practice change in the clinical setting.
While the results are promising, interpretation should consider several limitations, including single-site design, small sample size, short follow-up period, and potential for observer bias. Future work should explore broader implementation across multiple units or hospitals, incorporate longer evaluations periods, and examine sustainability over time.
Clinical Relevance
The implementation of I-PASS the BATON significantly improved the quality of nurse-to-nurse handoff communication at the project site, as evidenced by increased post-intervention scores on the HES and Observation Tool. These findings align with existing literature demonstrating that standardized handoff tools enhance the complete transfer of patient information, improve patient safety, and promote nurse satisfaction [11-15]. For nursing leaders, the results highlight the importance of standardized communication tools to support safer transitions of care and nurse satisfaction [11,13,18]. At the systems level, standardized handoffs can improve efficiency and support regulatory compliance, while fostering improved patient outcomes and enhancing staff satisfaction.
Recommendations include hospital-wide implementation of I-PASS the BATON with integration into the electronic medical record using the implementation procedures and both formative and summative evaluation strategies established in this project. Sustainability will be supported through weekly fidelity audits, staff huddles, leadership engagement, and continuous education. Ultimately, this practice change project reinforces the critical role of standardized communication in nursing practice.
Conflict of interest:
There are no conflicts of interest to disclose.
References
Agency for Healthcare Research and Quality. (2023). Tool: I-PASS. View
I-PASS Patient Safety Institute. (January 11, 2025). I-PASS institute for better handoffs and safer patient care. View
World Health Organization. (2024). Global patient safety 2024. View
Freel, J. & Fleharty, B. (2021). Standardizing handoff communication. American Nurse, 3, View
Joint Commission Online. (May 15, 2024). 2023 sentinel event data annual report. View
Howick J., Bennett-Weston, A., Solomon, J., Nockels, K., Bostock, J., & Keshtkar, L. (2024). How does communication affect patient safety? Protocol for a systematic review and logic model. BMJ Open, 14, e085312. View
The HIPAA Journal. (January 2, 2025). Effects of poor communication in healthcare. View
Joint Commission. (January 10, 2025). National patient safety goals. View
Joint Commission. (August 22, 2024). Handoff communication failures. View
O’Connell, B., Ockerby, C., & Hawkins, M. (2014). Construct validity and reliability of the Handover Evaluation Scale. Journal of Clinical Nursing, 3(3-4), 560-570. View
Nemati, S. M., Fathi, M., Nouri, B., & Vailee. (2022). Effects of a specific methodology (I Pass the Baton) on quality of handoff information among nurses: A comparative study. Journal of Healthcare Quality Research, 37(5), 268-274. View
Blazin, L. J., Sitthi-Amorn, J., Hoffman, J. M., & Burlison, J. D. (2020). Improving patient handoffs and transitions through adaptation and implementation of I-PASS across multiple handoff settings. Pediatric Quality Safety, 4(5), e423. View
Stenquist, D. S., Yeung, C. M., Szapary, H. J., Rossi, L., Chen, A. F., & Harris, M. B. (2022). Sustained improvement in quality of patient handoffs after orthopaedic surgery I-PASS intervention. Journal of the AAOS Global Research & Reviews, 6(9), 1-9. View
Truong, A., Nguyen, A., Pham, H., Nguyen, A., Pham, P., Tran, L., & Thai, T. (2020). The effectiveness of “I PASS the BATON” model in improving nursing handover at a university hospital in Vietnam. MedPharmRes, 4(3). View
Vega, M., Aiss, M., George, M., Day, L., Mbadugha, A., Owens, K., Sweeney, C., Chau, S., Escalante, C., & Bocurka, D. (2024). Enhancing implementation of the I-PASS handoff tool using a provider handoff task force at a comprehensive cancer center. The Joint Commission Journal on Quality and Patient Safety, 50(8), 560-568. View
Yanni, E., Calaman, S., Wiener, E., Fine, J. S., & Sagalowsky, S. T. (2023). Implementation of ED I-PASS as a standardized handoff tool in the pediatric emergency department. Journal for Healthcare Quality, 45(3), 140-147. View
Bukoh, M. X. & Siah, C. R. (2020). A systematic review on the structured handover interventions between nurses in improving patient safety outcomes. Journal of Nursing Management, 28, 744-755. View
Hada, A, Jones, L. V., Jack, L. C., Coyer, F. (2021). Translating evidence-based nursing clinical handover practice in an acute care setting : A quasi-experimental study. Nursing & Health Sciences, 23, 466-476. View
Jorro-Barón, F., Suarez-Anzorena, I., Burgos-Pratx, R., De Maio, N., Penazzi, M., Rodriguez, A. P., Rodriguez, G., Velardez, D., Gibbons, L., Ábalos, S., Lardone, S., Gallagher, R., Olivieri, J., Rodriguez, R., Vassallo, J. C., Landry, L. M., & García-Elorrio, E. (2021). Handoff improvement and adverse event reduction programme implementation in paediatric intensive care units in Argentina: A stepped-wedge trial. BMJ Quality & Safety, 30(10), 782–791. View
Hada, A. & Coyer, F. (2021). Shift-to-shift nursing handover interventions associated with improved inpatient outcomes Falls, pressure injuries, and medication administration errors: An integrative review. Nursing & Health Sciences, 23, 337-351. View
Benner, P. (1984). From novice to expert: Excellence and power in clinical nursing practice. Prentice Hall. View
Lewin, K. (1951). Field theory in social science: Selected theoretical papers (D. Cartwright, Ed.). Harper & Brothers. View
McNett, M., Tucker, S., Zadvinskis, I., Tolles, D., Thomas, B., Gorsuch, P., & Gallagher-Ford, L. (2022). A qualitative force field analysis of facilitators and barriers to evidence-based practice in healthcare using an implementation framework. Global Implementation Research and Applications, 2, 195-208. View
McCarthy, S., Motala, A., Lawson, E., & Shekelle, P. G. (2025). Use of structured handoff protocols for within-hospital unit transitions: A systematic review from Making Healthcare Safer IV. BMJ Quality & Safety, (4), 1-11. View
Adeniyi, A. O., Arowoogun, J. O., Okolo, C. A., Chidi, R., & Babawarun, O. (2024). Ethical considerations in healthcare IT: A review of data privacy and patient consent issues. World Journal of Advanced Research and Reviews, 21(2), 1660-1668. View
Chicco, D., Sichenze, A., & Jurman, G. (2025). A simple guide to the use of student’s t-test, Mann-Whitney U test, Chi-squared test, and Kruskal-Wallis test in biostatistics. BioData Mining, 18(56). View
IBM Corporation. (2022). IBM SPSS statistics for Window, version 29.0. Armonk, NY: IBM Corporation. View