
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Dermatology and Advanced Clinical Care
Journal of Dermatology and Advanced Clinical Care
Journal of Dermatology and Advanced Clinical Care Volume 2 (2023), Article ID: JDACC-102
https://doi.org/10.33790/jdacc1100102Research Article
Results of Dental Implant Usage in Patients with Oral Lichen Plans: A Comparative Cohort Study at the Central Hospital of Iran Oil ministry - A Multidisciplinary Study
Sarah Karimi1, Kowsar Karimi2, and Afshin Sadighha3*
1Assistant Professor, Prosthodontist, Central hospital of oil ministry, Tehran,Iran.
2Resident of Internal medicine, Shiraz university of medical science, Shiraz,Iran.
3Assistant Professor, Department of Dermatology, Ilam university of medical science, Iran.
Corresponding Author: Afshin Sadighha, Assistant Professor, Department of Dermatology, Ilam university of medical science, Iran.
Received date: 19th December, 2023
Accepted date: 19th January, 2024
Published date: 22nd January, 2024
Citation:Karimi, S., Karimi, K., & Sadighha, A., (2024). Results of Dental Implant Usage in Patients with Oral Lichen Plans: A Comparative Cohort Study at the Central Hospital of Iran Oil ministry - A Multidisciplinary Study. J Dermatol Adv Clin Care, 2(1): 102.
Copyright: ©2024, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Objective: This study aimed to determine the success rate of dental implant usage in patients with oral lichen plans (OLP) and compare the outcomes with a control group free of the disease, matched in terms of background factors. The collaborative effort between dermatology and dental prosthetics departments at the Central Hospital of Tehran Oil Company facilitated the execution of this study.
Research Methodology: A total of 17 patients with oral lichen plans and 21 healthy individuals meeting the study criteria participated. A total of 59 implants were used in the lichen plans group, and 58 implants were employed in the control group. The study spanned from March 2018 to April 2020. Pain levels and wound healing post procedure were recorded and compared between the two groups. The follow-up period was 24.7 ± 7.3 months for the lichen plans group and 23.7 ± 8.1 months for the control group. Radiographic and clinical aspects were documented to assess implant success and relevant variables.
Results: The success rate of implant usage in the lichen plans group was 100%, while in the control group, it was 95%. Postoperative complications in both groups were recorded and compared. The frequency of peri-implant mucositis (PIM) was 43% in the lichen plans group and 56% in the control group. Peri-implantitis occurred in 15% of the control group and 23% in the lichen plans group, with no statistically significant difference observed.
Conclusion: Our results showed that dental implants could be used safely in OLP if placed and managed by experienced staff.
Key words: Dental implants, Oral lichen plans, Peri-implant mucositis, Peri-implantitis
Introduction
Lichen plans is a chronic inflammatory disease that can affect the skin and mucous membranes. Typically appearing in the fourth decade of life, it is more prevalent in women. Various classifications based on pathological findings and clinical manifestations have been established, including reticular, plaque-like, erosive, and atrophic types [1-9]. The exact cause and pathogenesis of the disease remain incompletely understood, but it is clearly an autoimmune condition involving CD8+ cells. During this process, auto antigens are recognized by the patient's immune system, and activated T cells, mediated by inflammatory cytokines, induce inflammation and destruction of the basal layer, leading to a distinctive form of degeneration known as "qualified" and hydropic degeneration [9,17]. Key cytokines involved in this process include interleukin-1, interferon-gamma, and tumour necrosis factor-alpha [18].
Oral lichen plans associated with amalgam, used for the restoration of decayed teeth, has also been identified. Additionally, systemic diseases such as hepatitis C play a role in its pathogenesis. The major complication of oral lichen plans, if left untreated, is mucosal squamous cell carcinoma (SCC) [18-23]. Treatment primarily involves immunosuppressants and corticosteroids [14]. Considering the global expansion of dental implant usage and its role in improving quality of life, particularly with the increasing average age of individuals, the incorporation of this therapeutic option has been a continual challenge [11].
This study aims to investigate the success rate of dental implant usage in this patient group through a well-designed internal study. It also seeks to establish guidelines and identify suitable methods through collaborative efforts between the dermatology and dental prosthetics departments at the Central Hospital of Tehran Oil Company.
Material and Method
A total of 17 patients (11 females, 6 males) involved to oral lichen plans referred for implantation to the Dentistry Department of the Central Hospital of the Iranian Oil Company were recruited. Before referral, all patients underwent clinical and pathological assessments by a dermatologist.
Regarding the criteria for patient selection, it should be noted that all patients in the Lichen Planus group were examined by a dermatology specialist, and none of them had an active disease or were using systemic medication, despite being affected by mucosal lesions.
Various treatment options were discussed, and their consent was obtained. The study protocol was approved by the Central hospital of oil ministry university's ethics committee (Helsinki Convention on Human Experimental Studies). Inclusion criteria were the presence of oral lichen plans and being in the remission phase, with sufficient bone volume for surgery (bone length >7 mm). The study was made between March 2018 and April 2020. Types of oral lichen plans, diagnosed by the dermatologist, included reticular, erosive, and atrophic.
In five patients, cutaneous lesions were present, making oral involvement relevant for the study, especially during the remission phase. Treatment included topical steroids and oral steroids in cases with concurrent skin lesions, and chloroquine in cases with scarring alopecia. Local steroids were considered as the primary approach for oral lesions, continuing through the acute/erosive phase. No implants were placed during the erosive phase of the disease. Due to the nature of lichen planus and the Koebner phenomenon, patients were monthly examined by a dermatologist for disease activity, using corticosteroids as needed, up to twice a day. Outcome criteria included active periodontitis, history of previous radiotherapy, simultaneous immunosuppressant use, uncontrolled diabetes, and failure to record follow-up results. Demographic data and clinical findings were recorded for all patients.
The control group comprised individuals without oral lichen plans undergoing implant treatment, matched in terms of age, gender, BMI, implant length/diameter, number of fixtures, and implant location, with no statistically significant differences between the two groups. Each patient received 1-6 implants, with a diameter of 4-5 mm. Fifty nine implants were placed in the oral lichen plans group, and fifty eight implants in the control group, using the same implant type and placement method in all cases (using a general guideline and placing implants with a flap and above-bone level platform).
Amoxicillin was administered one hour before surgery (loading dose of 1 gram and then 500 mg every eight hours for seven days, the time of suture removal). Chlorhexidine mouthwash was prescribed twice daily for all cases, with complete oral hygiene instruction. Patients were provided with a brochure containing indications for consultation (presence of tissue contracture, bleeding, and pain). Patients were advised not to use removable partial dentures until the final prosthesis was fixed. Between three and six months after surgery(Maxilla and Mandible, respectively) Trans-Epithelial Abutment Attachment was used in patients.
After the final prosthesis, patients are advised to adhere to comprehensive oral hygiene, with the provision and distribution of educational brochures.
Clinical and Radiological Examination:
Bone quality at the time of implant placement was assessed using CT radiography and tactile resistance during drilling. Probing depth (PD), the distance between the implant margin mucosal prosthesis and the sulcus mucosal prosthesis, was measured during the removal of prostheses. Examinations were performed during prosthesis removal, and bleeding at that time was classified based on the following criteria:
0: absence of bleeding
1: separate points of bleeding
2: Bleeding line at mucosal margin
3: Severe bleeding
The number of exposed implant threads outside the bone (PIM) in the mesial and distal aspects of the implant was evaluated using radiography. The presence of peri-implant mucositis (BOP, PD <4mm and without bleeding)and PI (BOP or pus, bleeding during probing) was evaluated.
Postoperative Pain
Patients' postoperative pain was assessed using a modified Visual Analogue Scale (VAS), with zero( indicating no pain) and ten (indicating the most severe pain experienced by the patient). Pain during the seven days after implant placement was measured.
Soft Tissue Healing
The level of mucosal improvement around the implant was assessed during monthly follow-ups in intervals of one month after implant placement. The following criteria were considered:
0: Complete healing of mucosa around the implant without signs of inflammation
1: Mild inflammation, including redness, shape change, or non adherence of the mucosal surface around the implant(non integration).
Statistical Analysis
Statistical analysis was performed by SPSS, All the p-values <0.05 considered statistically significant.chi square for discrete and anova for continuous variables were used.
Results
The basic demographic and clinical features of patients are presented in Table 1, statistical analysis showed no meaningful differences between the two groups based on these variables, indicating high internal validity of the study.
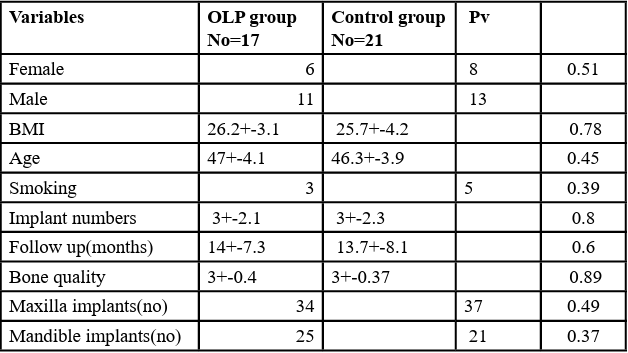
Table 1: Patients and control groups clinical and demographic features at baseline
Demographic and clinical aspects of the patients were meticulously examined and statistically compared. 64.7% of patients with oral Lichen Planus were male, while in the control group, 62% were male, indicating no significant statistical difference. Additionally, the mean age in the oral Lichen Planus group was 47±4.1 years, and in the control group, it was 46.3±3.9 years, showing no statistically significant difference. To enhance external validity, the frequency of tobacco use and BMI of the patients were calculated and statistically compared (Table 1.).
Appropriate screening resulted in only 3% implant failure rates to the control group, thus the implant successful rate in the oral lichen planus group was 100%. The minimum follow-up period was one year (24 months). Comparison of implant diameter and length between the two groups did not reveal any statistically significant differences. Bone loss levels are shown in Table 2, and their comparison did not demonstrate a statistically significant difference between the two groups (p=0.47).
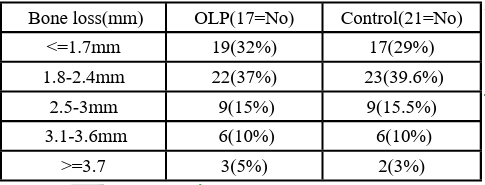
Table 2: Numbers and percentages of implants in each group based on bone loss levels
Probing depth (PD) was evaluated at the time of superstructure removal, and no meaningful difference was detected between the two groups. The frequency of PD based on the number of patients and implants is presented in Table 3.
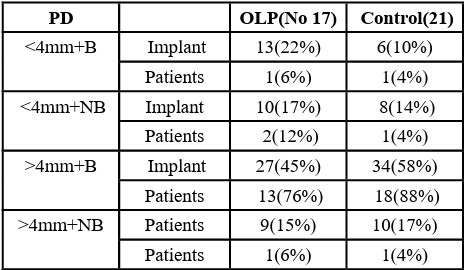
Table 3: Frequency of implants and patients according to different probing depths and the presence of bleeding in each group
(PIM) and (PI) were compared between the two groups and a summary of the results are presented in Table 4.

Table 4: Frequency of peri-implant mucositis and peri-implantitis in both groups
Patient pain, assessed using the Visual Analog Scale (VAS) with an interquartile range (IR) of 20, was examined and measured after implant placement in both groups. Statistical comparison did not reveal a significant difference between the two groups. Additionally, patients' improvement levels over time in both groups were examined and statistically compared, showing no significant differences.
Discussion
The evaluation of the effect of immediate loading on the success rate of dental implants has been studied in several research studies. However, their internal validity has been insufficient on the one hand, and the examination of this issue in Asian patients, relying on clinical information while using statistical data techniques for the first time, has been carried out in this study. Esposito [6] and Reichart [5]were the first to investigate this issue through small clinical studies and case series. Considering the increasing use of dental implants and their impact on patients' quality of life, it seems logical to pay more attention to this matter.
Subsequently, Hernandez [10], with a relatively cohesive study structure and a control group, brought this matter into focus. He conducted a study comparing these patients with a control group, revealing that the use of implants during the disease remission phase in lichen plans practically showed no significant difference in success rates. Although the study neglected various clinical factors affecting the implant deployment process, prompting us to conclusively establish this study with a stronger design. The success rate of implant use in our study was 100% in the lichen plans group, compared to 95% in the control group without lichen plans, as observed in their study. An interesting point is that it seems, due to the high precision and meticulousness in the selection and implant deployment process in the case group, to indicate a positive selection bias, which is unavoidable given the nature of the study. The level of bone loss is an important and noteworthy concept in the implant discussion, and in this study, it has been meticulously addressed. It should be noted that the presence of the inflammatory process, where CD8 cytotoxic cells induce apoptosis of basal layer cells and the occurrence of the liquefaction degeneration process, can affect bone loss.
The pathogenesis of oral Lichen Planus involves both specific and nonspecific antigenic mechanisms. Specific antigenic mechanisms in oral Lichen Planus include antigen presentation by basal keratinocytes and antigen-specific cytotoxic T-cell activity. Nonspecific mechanisms involve mast cell degranulation and matrix metalloproteinase activity in oral Lichen Planus lesions. The initial event in the formation of oral Lichen Planus lesions and factors indicating susceptibility to oral Lichen Planus are not yet clearly defined.
Several specific antigens and, of course, non-specific inflammatory mechanisms have been highlighted in this process. The presence of inflammation and mucositis can significantly impact bone loss. Standard assessment of bone loss is performed by evaluating the fixture-abutment junction point. The accepted range for bone loss is between 0.6-1.9 millimetres. The study has ambiguously shown that the use of appropriate techniques and loading does not significantly alter the meaning in patients with lichen plans. This issue has been addressed in other studies, including those by Czerninski [9] and Meijer (2009) [22], and the present study, with high precision, reinforces their findings. Although the level of bone loss is dependent on the follow-up period, gradual bone reabsorption increases over time [23]. Peri implant infections such as PIM and PI are important concepts in implantology.
In addressing peri-implantitis and Lichen Planus, it is essential to consider other variables and distinguish less effective factors. Dermatological lesions that visually resemble Lichen Planus may exhibit distinct pathology. Pathologically, Lichen Planus lesions manifest hyperkeratosis, hypergranulosis, and irregular acanthosis (sawtooth pattern). The lesions also display lymphocytic infiltration at the dermo-epidermal junction. Histologically, drug-induced and non-primary Lichen Planus lesions resemble primary cases, except for eosinophilic infiltration and prominent parakeratosis present in secondary cases.
Mucosal diseases such as lichen plans, from a theoretical standpoint, can affect the adhesion ability of epithelium to titanium surfaces (Esposito1998) [6] and lead to higher levels of peri-implant infections, along with a greater inclination toward bone loss.
Given the heterogeneous nature of oral Lichen Planus, it is evident that there is a need for larger studies with a more diverse cohort and accompanied by higher follow-up rates. Although this study can contribute within its appropriate framework, it can lay the groundwork for such comprehensive investigations.
Conclusion
Considering the coherent and high quality methodological structure of our study, this is the first study that, by taking into account all clinical and technical variables in Asian patients, clearly indicates that with appropriate attention and academic consideration, implants can be used in patients suffering from oral lichen plans. These results can definitively be cited, given its high internal validity.
References
Chrcanovic, B.R., Kisch, J., Albrektsson, T., & Wennerberg, A. A., (2018). Retrospective study on clinical and radiological outcomes of oral implants in patients followed up for a minimum of 20 years. Clin. Implant Dent. Relat. Res, 20, 199 207, doi:10.1111/cid.12571.View
Zhang, Q., Chen, B., Yan, F., Guo, J., Zhu, X., Ma, S., & Yang, W., (2014). Interleukin-10 Inhibits Bone Resorption: A Potential Therapeutic Strategy in Periodontitis and Other Bone Loss Diseases. BioMed Res. Int, 1–5.View
Sugerman, P. B., & Barber, M. T., (2002). Patient selection for endosseous dental implants: oral and systemic considerations. Int J Oral Maxillofac Implants;17:191-201.View
Fu, L., Liu, Y., Zhou, J., & Zhou, Y., (2019). Implant-retained overdenture for a patient with severe lichen planus: a case report with 3 years’ follow-up and a systematic review. J Oral Maxillofac Surg, 77:59-69.View
Reichart, P. A. (2006). Oral lichen planus and dental implants. Report of 3 cases. Int J Oral Maxillofac Surg;35:237-240. View
Esposito, S. J., Camisa, C., & Morgan, M., (2003). Implant retained overdentures for two patients with severe lichen planus: a clinical report. J Prosthet Dent;89:6-10.View
López-Jornet, P., Camacho-Alonso, F., & Sánchez-Siles, M., (2014). Dental i plants in patients with oral lichen planus: a cross-sectional study. Clin Implant Dent Relat Res;16:107-115.View
Aboushelib, M. N., & Elsafi, M. H., (2017). Clinical management protocol for dental implants inserted in patients with active lichen planus. J Prosthodont; 26:29-33.View
Czerninski, R., Eliezer, M., Wilensky, A., Soskolne, A., (2013). Oral lichen p nus and dental implants--a retrospective study. Clin Implant Dent Relat Res;15:234-242.View
Hernández, G., Lopez-Pintor, R. M., Arriba, L., Torres, J., & de Vicente, J. C., (2012). Implant treatment in patients with oral lichen planus: a prospective-controlled study. Clin Oral Implants Res; 23:726-732.View
Khamis, A. K., Aboushelib, M.N., & Helal, M. H., (2019). Clinical management protocol for dental implants inserted in patients with active lichen planus. Part II 4-year follow-up. J Prosthodont; 28:519-525.View
Sugerman, P. B., Savage, N. W., & Walsh, L. J., et al. (2002). The pathogenesis of oral lichen planus. Crit Rev Oral Biol Med; 13:350-365.View
Sciubba, J. J., (2011). Autoimmune oral mucosal diseases: clinical, etiologic, diagnostic, and treatment considerations. Dent Clin North Am; 55:89-103.View
Scully, C., & Carrozzo, M., (2008). Oral mucosal disease: Lichen planus. Br J Oral Maxillofac Surg; 46:15-21.View
Camacho-Alonso, F., López-Jornet, P., & Bermejo-Fenoll, A., (2007). Gingival involvement of oral lichen planus. J Periodontol; 78:640-644View
Mignogna, M. D., Lo Russo, L., & Fedele, S., (2005). Gingival involvement of oral lichen planus in a series of 700 patients. J Clin Periodontol; 32:1029-1033.View
Azizi, A., & Rezaee, M., (2012). Comparison of periodontal status in gingival oral lichen planus patients and healthy subjects. Dermatol Res Pract. View
Ramón-Fluixá, C., Bagán-Sebastián, J., Milián-Masanet, M., & Scully, C., (1999). Periodontal status in patients with oral lichen planus: a study of 90 cases. Oral Dis;5:303-306.View
Lo Russo, L., Guiglia, R., & Pizzo, G., et al. (2010). Effect of desquamative g givitis on periodontal status: a pilot study. Oral Dis;16:102-107 View
Lo Russo, L., Gallo, C., & Pellegrino, G., et al. (2014). Periodontal clinical and microbiological data in desquamative gingivitis patients. Clin Oral Investig;18:917-925.View
Adler, L., Buhlin, K., & Jansson, L., (2019). Survival and complications: A 9- to 15-year retrospective follow-up of dental implant therapy. J Oral Rehabil. doi: 10.1111/joor.12866.View
Meijer, H. J., Raghoebar, G. M., & Batenburg, R. H.,et al., (2009). Mandibularover dentures supported by two Branemark, IMZ or ITI implants: A ten-year prospective randomized study. J Clin Periodontol 36:799.View
Roos-Jansåker, A. M., Lindahl, C., Renvert, H., & Renvert, S., (2006). Nine- to fourteen-year follow-up of implant treatment. Part II: presence of peri-implant lesions. J Clin Periodontol; 33:290-295.View