
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Multidisciplinary Clinical Case Reports
Journal of Multidisciplinary Clinical Case Reports
Journal of Multidisciplinary Clinical Case Reports Volume 1 (2021), Article ID: JMCCR-103
https://doi.org/10.33790/jmccr1100103Case Report
A Case Study of Acute Onset Obsessive-Compulsive Symptoms in a Pediatric Patient
Sydney A. Rice, MD, MSc3*, Angela J. Cabrera, MSN, CPNP1, Michael Daines, MD3, Christopher Spiekerman, DO1, Peter Klinger, MD2
1Children’s Postinfectious Autoimmune Encephalopathy Clinic, Banner Children’s, Mesa, Arizona
2Assistant Professor, Department of Psychiatry, University of Arizona College of Medicine, United States.
3Children’s Postinfectious Autoimmune Encephalopathy Center of Excellence, University of Arizona,United States.
Corresponding Author Details: Sydney A. Rice, MD, MSc, Professor of Department of Pediatrics, College of Medicine Tucson Pediatrics, University of Arizona, 1501 N. Campbell Avenue, United States. E-mail: srice@peds.arizona.edu
Received date: 09th November, 2021
Accepted date: 01st December, 2021
Published date: 03rd December, 2021
Citation: Rice, S. A., Cabrera, A. J., Daines, M., Spiekerman, C., & Klinger, P. (2021). A Case Study of Acute Onset Obsessive-Compulsive Symptoms in a Pediatric Patient. J Multidiscip Clin Case Rep, 1(1): 103. doi: https://doi.org/10.33790/ jmccr1100103.
Copyright: ©2021, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
This is a case of a 10 year old boy who was seen in a clinic that specializes in childhood postinfectious encephalopathy (CPAE). The patient presented with new onset of obsessive-compulsive behaviors, severe separation anxiety and progressive eating restriction which led to dehydration and hospitalization. His mother reported that prior to onset of symptoms two months earlier, he was a happy, playful and engaging child who enjoyed friendships, family, school and karate. Differential diagnosis in such cases focuses on identifying the most likely primary underlying cause for the presenting symptoms. This is especially challenging because there are many potential etiologies including a variety of behavioral and environmental causes. Based on patient examination, laboratory findings and psychometric tests, diagnoses considered by the clinical team included new onset or exacerbation of previously not identified obsessive compulsive disorder (OCD) or anxiety, new onset of tic disorder, new onset of eating disorder, Pediatric Autoimmune Neuropsychiatric Disorders Associated with Group A Streptococcal infection (PANDAS) and Pediatric Acute-onset Neuropsychiatric Syndrome (PANS). The presentation of OCD with an avoidant restrictive food intake disorder in combination with the acute onset of symptoms and the lack of documented strep infection led the team to a PANS diagnosis. When treated with a combination of anti-inflammatory and antibiotic medications, the patient demonstrated rapid improvement with a return to baseline functioning with resolution of OCD symptoms, separation anxiety, emotional lability, sleep disturbances and nocturnal enuresis. At 8 month follow up, school performance was reported to have returned to baseline.
Key words: Childhood Postinfectious Encephalopathy, OCD, PANDAS, PANS
The case
A10-year-old boy is seen in a clinic that specializes in childhood postinfectious encephalopathy (CPAE), with new onset of obsessive-compulsive behaviors, severe separation anxiety and progressive eating restriction which led to dehydration and hospitalization. His mother reports that prior to onset of symptoms two months earlier, he was a happy, playful and engaging child who enjoyed friendships, family, school and karate.
History and examination
In January of 2019, the patient complained of a sore throat and fatigue, with intermittent symptoms over two months. He had a history of streptococcal exposure one month prior to symptoms. Over the course of the next two months, he began having increasing fears regarding contamination, with his waking hours consumed by checking his skin for insects and scorpion stings. He also reported feeling like he was being “poked and stabbed” by invisible objects. He began to have obsessions concerning his teeth, with a fear of toothbrushes which led to refusal of dental care. He also began to have vocal stridor tics and obsessions regarding choking on food, leading to him avoiding solid foods. He lost 3 kg over two months. He also began to have secondary symptoms of nocturnal enuresis and math deterioration.
The patient’s medical history included controlled asthma and a history of severe food allergies, including coconut oil, eggs, peanuts and tree nuts. He had no surgeries. At sixteen months he was hospitalized for an anaphylactic food reaction. He was born at term by spontaneous vaginal delivery without complications, with normal growth and development. His family history was negative for chronic infections, autoimmune disorders, neurodevelopmental disorders, movement disorders or anxiety/mood disorders. He currently was living with his stepfather and biological mother and four siblings in a stable home environment. He was in the fourth grade and successfully home schooled with no academic problems until 2019.
The patient was evaluated by a primary care physician for fatigue and sore throat in March of 2019. Due to increasing concern over his behavior, he was referred to a local neurologist who prescribed daily ibuprofen. When his condition had not improved in May, the patient was referred to the emergency department for possible admission for dehydration. He received IV hydration and lab work and was sent home for follow up with our clinic due to concerns for autoimmune encephalopathy.
At his first appointment at our clinic, the patient was ill appearing, mildly dehydrated with dry cracked lips and mucous membranes, tachycardic, and pale. He was slow to respond to examiner history questions. His cranial nerve exam and overall gait was normal, but he presented with neurological subtle signs of dysrhythmia, mirroring and slowing of rapid sequential movements with hand pronation/ supination and heel-toe tapping. He was easily fatigued during balance, gait, and motor coordination testing.
The patient and his mother completed an initial psychometric screening which revealed significant patient concerns for anxiety (Screen for Child Anxiety Related Disorders/SCARED [1] parent score 39), affective lability (Children's Affective Lability Scale/ CALS [2] parent score 35, child score 37), obsessive compulsive symptoms (Obsessive Compulsive Inventory-Child Version/OCI-CV [3] child score 10), and restricted eating (Nine Item Avoidant/ Restrictive Food Intake disorder screen/NIAS [4] 42, child and parent). All of these scores are consistent with significant concerns in each of the related areas.
Laboratory testing
In the three months prior to his presentation at our clinic, the patient was evaluated by a primary care physician who ordered a complete blood count (CBC) and Epstein Barr virus (EBV) titers, all normal. He was referred to a local neurologist who ordered a CBC, complete metabolic panel (CMP), CD57, Lyme titers, ferritin, ceruloplasmin, anti-streptolysin O (ASO) titer, c-reactive protein (CRP), thyroglobulin antibodies, adenovirus IgG, cytomegalovirus (CMV) IgM, human herpes virus (HHV) 6 IgM, copper levels, bartonella antibody panel, and influenza IgM. All labs were essentially normal, with the exception of a mildly elevated creatinine at 0.78.mg/dl. Mycoplasma IgG and IgM levels and West Nile IgG levels were also negative. Coxsackie IgG levels were positive indicating prior exposure, but IgM levels were negative. Emergency department lab results revealed a normal CBC, a normal CMP with the exception of mildly elevated anion gap (17), calcium (10.6 mg/dL), protein (8.1 g/dL) and albumin (5.4 g/dL). Urinalysis was normal with the exception of mild ketonuria (20mg/dL).
Differential Diagnosis
This is a 10 year old boy who presented with abrupt onset of severe obsessive-compulsive behaviors, separation anxiety, phonic tics and restricted eating patterns. Refusal to take food or liquids resulted in hospitalization for dehydration.
Differential diagnosis in such cases focuses on identifying the most likely primary underlying cause for the presenting symptoms. This is especially challenging because there are many potential etiologies including a variety of behavioral and environmental causes. A range of common diagnoses that may be considered in a case similar to the one described here are shown in Table 1.
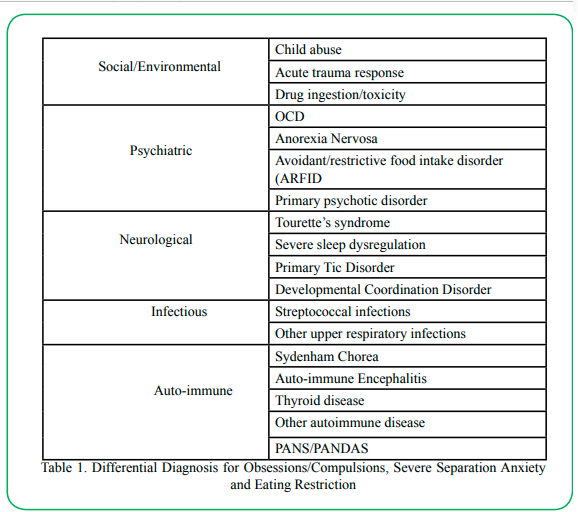
Table 1: Differential Diagnosis for Obsessions/Compulsions, Severe Separation Anxiety and Eating Restriction
Diagnoses considered in discussion with the clinic team included new onset or exacerbation of previously not identified obsessive compulsive disorder (OCD) or anxiety, new onset of tic disorder, new onset of eating disorder, Pediatric Autoimmune Neuropsychiatric Disorders Associated with Group A Streptococcal infection (PANDAS) and Pediatric Acute-onset Neuropsychiatric Syndrome (PANS). These conditions and the distinguishing characteristics among them are discussed below.
Obsessive compulsive disorder and anxiety
According to the Diagnostic and Statistical Manual of Mental Disorders, obsessions are defined by:
1. Recurrent and persistent thoughts, urges, or images that are experienced, at some time during the disturbance, as intrusive and unwanted, and that in most individuals cause marked anxiety or distress.
2. The individual attempts to ignore or suppress such thoughts, urges, or images, or to neutralize them with some other thought or action (i.e., by performing a compulsion).
Compulsions are defined by: 1. Repetitive behaviors (e.g., hand washing, ordering, checking) or mental acts (e.g., praying, counting, repeating words silently) that the individual feels driven to perform in response to an obsession or according to rules that must be applied rigidly.
2. The behaviors or mental acts are aimed at preventing or reducing anxiety or distress, or preventing some dreaded event or situation; however, these behaviors or mental acts are not connected in a realistic way with what they are designed to neutralize or prevent, or are clearly excessive [5].
The patient met criteria for a diagnosis of OCD based on the presence of intrusive and distressing thoughts about insects and contamination, and repetitive compulsive checking and reassurance-seeking behaviors that transiently relieved his distress while negatively impacting his functioning. In this case, the child’s obsessions focused on tactile sensation, and an intrusive and functionally impairing fear of “invisible” insect bites or stings. Distinguishing his obsession from a specific insect phobia can be challenging, but in this case the intrusive obsessional concerns extended to other areas such as his teeth and fears about choking that were unrelated to insects. His OCI-CV score on screening in the clinic initially was 10, consistent with significant OCD symptoms.
The presentation of a child with OCD behaviors poses a significant challenge for the general pediatrician. The prevalence of obsessive-compulsive disorders among children and adolescents is estimated at 0.25%–4%, so perplexing symptoms such as these may been countered only occasionally, if at all, in a general pediatric practice. But left unresolved, these symptoms can become chronic and lead to impairment of the child’s functioning in multiple domains, including at home, school and socially [6].
While our patient met criteria for OCD, the lack of any previous concerns for OCD and the abrupt onset of symptoms was not consistent with a typical presentation of OCD. In general, children who develop OCD have subtle behaviors initially and the behaviors increase in intensity over months to years.
Our patient also presented with severe separation anxiety. The combination of new onset OCD and anxiety in a child with no previous psychiatric concerns brings up concern for trauma as the cause of this change. Traumatic experiences include physical abuse, psychological maltreatment, sexual abuse, or neglect. The possibility that the presenting symptoms are a response to a particular traumatic incident must also be considered. In this particular case, examination of the child showed no evidence of physical harm, there was a warm and appropriate relationship between mother and child, and the child disclosed feeling safe with in home and family, there by making abuse as a causal factor unlikely. The behavioral symptoms could also be a medication reaction or a result of illicit substance use, but the case history reveals neither of these as a potential factor.
Pediatric anxiety disorders typically begin during specific developmental phases. For example, separation anxiety usually begins during pre-school/early school age years. The acute onset of severe separation anxiety in a 10-year-old boy without a prior history, who is experiencing neither an escalation of an ongoing situation nor a new significant stressor would be atypical and would suggest evaluation for another condition.
Eating concerns
Our patient presented with food avoidance due to fear of choking. Many children develop food avoidance following aversive experiences such as choking or vomiting. Our patient’s history of anaphylaxis would certainly qualify as a frightening experience that could have primed him for an avoidant restrictive food intake disorder (ARFID). We reviewed possible traumatic experiences associated with the history of anaphylactic food allergy, and family could not identify any experiences that would have heightened either parent and child fear about eating. Anorexia nervosa (AN) diagnosis requires a preoccupation with weight and body shape, and this child shared no concerns for body dysmorphia; parents concurred that the child had not shared any concerns about weight or body image.
Neurological and somatic concerns
This child presented with acute-onset psychiatric concerns, but also had abnormal findings on neurological examination, e.g., dysrhythmia, mirroring and slowing of rapid sequential movements with hand pronation/supination and heel-toe tapping. These findings are consistent with incoordination that could be seen in a child with developmental coordination disorder (DCD), but a child with DCD typically has been clumsy throughout childhood and this is new finding for this child. He had developed vocal tics acutely and this could be the new-onset of a tic disorder, but a tic disorder does not account for the many other symptoms in this child’s presentation. Tourette syndrome is associated with other neurobehavioral comorbidities such as OCD, ADHD and anxiety, but it does not generally present in such an acute manner and motor tics generally occur before vocal tics. Tourette syndrome also requires that the child have multiple motor tics, at least one vocal tic with these tics persisting for a year. While this child did have nocturnal enuresis after having been continent, we do not have other history of sleep concerns that would be concerning of a significant sleep disorder.
Autoimmune conditions
The presentation of illness and normal labs made many autoimmune diseases unlikely for this child; the absence of chorea or unexplained fevers, rashes, or arthritis was reassuring that this was not rheumatic fever or Sydenham Chorea. Screening labs that demonstrated a normal CBC, UA, CRP and thyroid studies also made autoimmune diseases less likely. Autoimmune encephalitis is less likely without focal CNS findings or seizures but could not be completely ruled out without CSF studies, MRI findings, and an assessment of response to immunomodulatory treatment.
PANDAS/PANS
The child’s pharyngitis and fatigue indicated the likelihood of an unidentified infection. Group A streptococcus (GAS) bacteria is known to cause a number of conditions that produce abrupt onset of neurological symptoms in children. Among these are rheumatic fever and Sydenham’schorea, both of which present with uncoordinated jerking movements involving all four limbs,which were not evident in this case. The child’s presenting symptoms were more consistent with Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infection (PANDAS), a clinical condition associated with the unusually abrupt onset of obsessive-compulsive symptoms along with other movement and behavioral abnormalities. However, PANDAS diagnostic criteria require a recent diagnosis of strep infection,which was not identified.
A more likely diagnosis was Pediatric Acute-onset Neuropsychiatric Syndrome (PANS), a clinical condition defined by the unusually abrupt onset of obsessive-compulsive symptoms A more likely diagnosis was Pediatric Acute-onset Neuropsychiatric Syndrome (PANS), a clinical condition defined by the unusually abrupt onset of obsessive-compulsive symptoms and/or severe eating restrictions and at least two concomitant cognitive, behavioral, or neurological symptoms [7]]. PANS is thought to be triggered by infections, metabolic disturbances, and other inflammatory reactions. A PANS diagnosis does not require any laboratory abnormalities and is diagnosed by an abrupt onset of obsessive compulsive-like behaviors or severely restricted food intake along with at least two additional findings: anxiety, emotional lability and or depression, irritability, aggression, and/or severe oppositional behaviors, behavioral (developmental) regression, sudden deterioration in school performance, motor or sensory abnormalities, or somatic signs and symptoms including sleep disturbances, enuresis, or urinary frequency.
Diagnosis and treatment
The presentation of OCD and ARFID in combination with lack of documented strep infection and the acute onset of symptoms led us toa PANS diagnosis. PANS is hypothesized to be the result of autoimmune antibodies mistakenly attacking the basal ganglia in the brain, frequently related to an infection. We placed the patient on amoxicillin/clavulanic acid 400mg/5ml, 7.5ml BID, naproxen sodium 125mg/5ml 10ml twice daily, and omeprazole 2mg/ml, 10ml daily for 14 days with instructions to return to the ED for worsening symptoms, and to follow up with our clinic within the next week. The rationale for treating with an antibiotic was to eliminate a possible bacterial infection that was causing our patient’s severe behavioral symptoms. In addition, we prescribed an anti-inflammatory medication to treat underlying inflammation.
At the one week follow up, the patient had improvement in appetite with a 0.5 kg weight gain, improved sleep patterns from 4-6 hours to 9 hours nightly, decreased obsessional thought patterns and separation anxiety as reported by mother and grandmother. His math difficulty persisted and nocturnal enuresis remained unchanged. He appeared more focused and attentive during evaluations. He was also willing to have a provider examine his mouth, which he was not able to do for over a month with other providers or his dentist.
Mother reported that the patient was using ibuprofen in place of naproxen and we instructed the patient to continue his antibiotics, increase his ibuprofen to three times daily, and complete a five-day course of oral prednisolone. We also recommended obtaining follow up labs (urinalysis, T3, thyroid stimulating hormone (TSH), thyroglobulin antibodies, microsomal TPO antibodies), a brain MRI, psychiatric evaluation, nutrition referral, and CBT.
The following week, the patient was seen in clinic and continued to exhibit improvements in separation anxiety, appetite, and OCD behaviors. Parents declined the MRI due to patient’s on going improvement. On the first two days of prednisolone therapy, the patient experienced worsening OCD behaviors, but the mother noted moderate improvement in OCD, anxiety and eating restriction within one week. Handwriting, nocturnal enuresis and school performance improved. Choking fears were almost completely resolved. He began to try a variety of new food textures. Repetitive skin checking had resolved. His mother was able to leave the home and run errands without the patient experiencing separation anxiety. On exam, the patient was well appearing, with normal coordination, appropriate timing in responses to questions and a normal neurological exam. Mother noted significant improvements in mood and affect. We continued treatment with azithromycin and ibuprofen for a total of three months. We instructed the family to begin with CBT interventions.
Over the course of the next 8 months, the patient returned to baseline functioning with resolution of OCD symptoms, separation anxiety, emotional lability, sleep disturbances and nocturnal enuresis. School performance was reported to have returned to baseline. A repeat psychometric testing battery demonstrated a return to normal functioning in the areas of anxiety (SCARED parent score of 16), affective lability (CALS parent score at 0, child at 1), restricted eating (NIAS now at 16 for parent and 14 for child, with mild concerns for picky eating) and obsessive compulsive symptoms (OCI-CV child score now at 2).
Discussion
A phenomenological diagnosis is a set of clinically derived criteria that relies heavily on the subjective reports of the patient and parents, in the absence of clear and consistent biological markers. The vast majority of psychiatric disorders are diagnosed in this way and require the exclusion of other medical causes.
The National Institutes of Health first distinguished the phenomenon of strep-related PANDAS in the late 1990s, and subsequently defined PANS in 2012 to address the wider group of children who may have underlying etiologies separate from documented streptococcal infection. Research is ongoing to clarify the link between inflammation and psychiatric disorders, enhancing the ability to better diagnose and treat youth with a variety of neuropsychiatric disorders.
PANS/PANDAS, while based on a strong biological model supported by active research, does not include currently agreed upon biomarkers. As a result, it relies on phenomenological diagnosis and is a “diagnosis of exclusion” made through comprehensive clinical examination confirming that other known neurological and medical disorders do not better explain the symptoms and clinical history of the patient. The clinical symptoms overlap with a variety of psychiatric disorders; however, is the atypically rapid, severe onset of various problems that distinguishes PANS from psychiatric disorders. The manner in which PANS/PANDAS is distinguished from Pediatric OCD is summarized in Table 2.
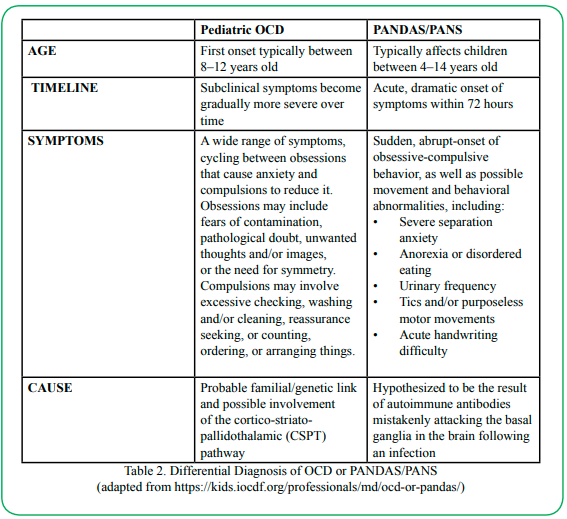
Table 2: Differential Diagnosis of OCD or PANDAS/PANS
In the time since it was first identified in 1998, PANDAS and the related PANS diagnosis have engendered some controversy, owing largely to the absence of a clear biological diagnostic marker; questions regarding the link between strep infection, OCD and the autoimmune mechanism; and the uneven results of the limited studies to date examining response to various treatments [8]. There is an urgent need for more robust research to illuminate these issues. However, there is a mounting body of evidence to support an association between infectious disease and mental disorders,and the role of inflammation in the exacerbation of symptoms.
In cases of acute onset of symptoms that meet the PANS/PANDAS criteria, identification and intervention early in the disease cycle is critical for returning affected children to baseline functioning. General pediatricians, as the ones most likely to see these children first, play a key role in initial case finding and early treatment. The diagnostic elements for assessing a potential case of PANS/PANDAS are outlined in Table 3.
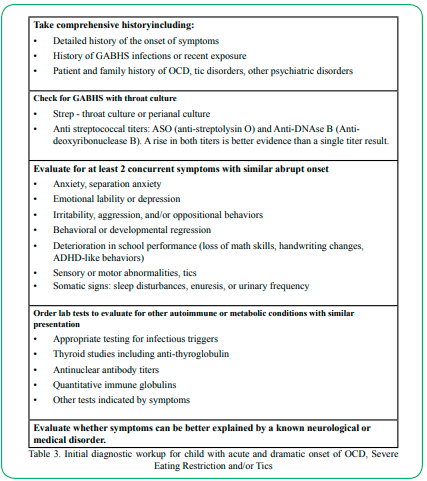
Table 3: Initial diagnostic workup for child with acute and dramatic onset of OCD, Severe Eating Restriction and/or Tics
Where there is a high index of suspicion of PANS or PANDAS based on the clinical findings, a trial antibiotic and NSAID course of treatment has the value of potentially being both diagnostic and therapeutic. Follow-up examination will reveal the efficacy of the intervention.
If the result is unremitting and worsening symptoms, referral is warranted for further investigation and treatment. Recommended treatment for more complex cases calls for a multi-disciplinary approach encompassing psychiatry and behavioral interventions [9] and immunomodulatory therapy [10]. Clinical consultation is available and ongoing investigational research is being conducted at various sites nationally and internationally.
Competing interests:
The authors declare that they have no competing interests.
References
Caporino, N.E., Sakolsky, D., Brodman, D.M., et al. (2017). Establishing Clinical Cutoffs for Response and Remission on the Screen for Child Anxiety Related Emotional Disorders (SCARED). J Am Acad Child Adolesc Psychiatry. 56(8):696- 702. doi:10.1016/j.jaac.2017.05.018View
Van Liefferinge, D., Sonuga-Barke, E., Danckaerts, M., Fayn, K., Van Broeck, N., van der Oord, S. (2018). Measuring child and adolescent emotional lability: How do questionnaire-based ratings relate to experienced and observed emotion in everyday life and experimental settings?. Int J Methods Psychiatr Res. 27(3):e1720. doi:10.1002/mpr.1720View
Jones, A.M., De Nadai, A.S., Arnold, E.B., et al. (2013). Psychometric properties of the obsessive compulsive inventory: child version in children and adolescents with obsessive-compulsive disorder. Child Psychiatry Hum Dev. 2013;44(1):137-151. doi:10.1007/s10578-012-0315-0View
Brigham KS, Manzo LD, Eddy KT, Thomas JJ. (2018). Evaluation and Treatment of Avoidant/Restrictive Food Intake Disorder (ARFID) in Adolescents. Curr Pediatr Rep, 6(2):107- 113. doi:10.1007/s40124-018-0162-y View
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association:237. doi.org/10.1176/appi. books.9780890425596View
Krebs, G., Heyman, I. (2015). Obsessive-compulsive disorder in children and adolescents. Arch Dis Child. 100(5):495-499. doi:10.1136/archdischild-2014-306934View
Swedo, S.E., Frankovich, J., Murphy, T.K. (2017). Overview of Treatment of Pediatric Acute-Onset Neuropsychiatric Syndrome. J Child Adolesc Psychopharmacol;27(7):562-565. doi:10.1089/cap.2017.0042View
Hyman, S. (2021). PANDAS: Too Narrow a View of the Neuroimmune Landscape. Am J Psychiatry.178:5–7. doi: 10.1176/appi.ajp.2020.20111598View
Thienemann, M., Murphy, T., Leckman, J., et al. (2017). Clinical Management of Pediatric Acute-Onset Neuropsychiatric Syndrome: Part I-Psychiatric and Behavioral Interventions. J Child Adolesc Psychopharmacol.27(7):566-573. doi:10.1089/ cap.2016.0145View
Frankovich, J., Swedo, S.E., Murphy, T., et al. (2017). Clinical Management of Pediatric Acute-OnsetNeuropsychiatric Syndrome: Part II-Use of Immunomodulatory Therapies. J Child AdolescPsychopharmacol.27(7):574-593. doi.org/10.1089/ cap.2016.0148View