
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 1 (2017), Article ID: JPHIP-106
https://doi.org/10.33790/jphip1100106Research Article
How safe is social casino gambling for elderly women?
Young Lee
Department of Mathematics and Computer Science Manchester University, USA
Corresponding Author Details: Young Lee, Department of Mathematics and Computer Science, Manchester University, USA. E-mail: yslee@manchester.edu
Received date: 16th October, 2017
Accepted date: 06th December, 2017
Published date: 08th January, 2018
Citation: Lee Y (2018) How safe is social casino gambling for elderly women? J Pub Health Issue Pract 2: 106.
Copyright: ©2018, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
We create a mathematical model with a system of nonlinear ordinary differential equations to study how safe social casino gambling is for elderly women. Older women develop gambling problems significantly faster than their male counterparts, which is a typical characteristic of electronic machine gambling. We study dynamics of the system through stability analysis and numerical simulations. We find that an exposure to a casino involves a significant risk; casino gambling is present in an endemic state; problem casino gambling among the elderly women is decreasing in the long run; the model is most sensitive to the initial exposure.
keywords: Gambling, Elderly women and casino, Prevention strategies, Mathematical modelIntroduction
Women are over-represented in the older adult population. Legalized casinos aggressively target elderly women with disposable income and time by even designing slot machines that fit the physique of elderly women [1]. Breen and Zimmerman report that machine factors have more to do with the rapid onset of problem gambling (excessive gambling that causes problems to herself and/ or others) than intrapersonal factors [2]. Casinos accommodate diverse gambling activities, of which some do not require any gaming skills, especially slot machines, which are favored by elderly women and require relatively small amounts of cash. In this study, the main electronic machine gambling is assumed as slot machine gambling, and some venues such as hotels or bars with multiple slot machines are referred to as casinos. Many elderly women start casino gambling to socialize. How healthy is social casino gambling for elderly women?
The first mathematical modeling approach to study the dynamics of gambling was done by Lee and Do [3]. They viewed gambling disorder as a communicable disease by taking the interpretation of Shaffer and Korn [4], ”exposure to gambling or activities and materials that promote it reflects a sequence of social contacts that conceptually act like germs or toxins that can lead to adverse health consequences.” We now focus on studying the effects of social casino gambling among the older female population. Women generally have less leisure time for themselves than men when children are around even when they have their own career, so many have not planned their life after retirement. Volberg [5] discusses the feminization of gambling and problem gambling, which ” refers to the idea that more women are gambling, developing problems and seeking help for problems related to gam- bling than in the past. ... [This] is linked to increased availability of gaming machines.” Many elderly women are drawn to casinos as they view them as safe spaces physically with security personnel and colorful lights and also because of incentives and conveniences that casinos provide such as free transportation and shopping malls nearby. Petry reports that older gamblers are more likely female than are the younger gamblers. Older women do not begin gambling regularly until an average age of 55 years, whereas older male gamblers with gambling disorders are generally lifelong gamblers [6]. The initial exposure to casino gambling for some elderly women could be harmful. Researchers [7,8] show that older women develop gambling problems significantly faster than their male counterparts, but theyalso recover faster, which is one of the main characteristics of electronic machine gambling. Many elderly women start casino gambling to socialize or to alleviate boredom. However, many of them also gamble to win money, about 63% according to the study by Martin et. al. [9]. I.e., the initial exposure to casino gambling for some elderly women could be harmful. Hence, one of the main goals of this study is to examine how safe social casino gambling is for elderly women.
We first derive an epidemiological model with four compartments using ordinary differentialequations. The details of stability analysis and model parameter estimations are in the Appendix section. Exploration of numerical simulations com- bined with analytical approaches conclude the discussions such as the effectiveness of education campaign, prevention vs control, the prevalence rates and the long-term prediction of the model among others.
Derivation of the Model
Our system is composed of lonely retired women ages 65-80. Most of these are widows who live alone or in a retirement community or are care givers to spouses. These individuals are divided into four classes of our model. The susceptible class, S, in our model consists of individuals who have not visited a casino for the last 12 months although they might have played other games of chance such as lotteries or Bingo games. When individuals of the susceptible class are exposed to a casino and begin to enjoy a casino game, especially slot machines for our model populations, they transition to the sec- ond compartment, E. Members of E are exposed to slot machines and visit a casino frequently, but they are not addicted to gambling and do not gamble excessively. Since gambling disorder occurs on a continuum, regular gamblers of E are at risk of problem gambling. The A class consists of individuals with problem gambling behaviors measured by the Lie/ Bet Questionnaire, ”Have you ever felt the need to bet more and more money?” and ”Have you ever had to lie to people important to you about how much you gamble?” When individuals of E progress to intense gambling and develop problem gambling behaviors, they advance to the A class to which pathological gamblers also belong. As problems associated with gambling occur with severity, some members of the A class may seek treatment for recovery and transition to the R class. Some individuals of the R class relapse to the A class, and some succeed and join the susceptible class. It is known that even some pathological gamblers recover naturally. The members of the A class who recover without any treatment transition to the S class. The total constant population is represented by N = S + E + A + R.
We specify the rates at which members of each class transition between classes by considering the main features that trigger each transition. In our model, individuals of the S class are exposed to casinos by peers, and we assume that more exposure and more opportunities lead elderly women to become frequent gamblers. We model it by the constant rate β, which is directly proportional to the number of gamblers among the peer group, (E + A)/N, and depends on the frequency and intensity of the interaction with gamblers. All transition rates are given as per capita. Many elderly women start gambling as a recreational activity to socialize, but some of them may become a problem gambler or pathological gambler depending on many factors. According to Shaffer and Korn [4], it depends on behavior patterns, psychology, and neurobiology. Alcohol, smoking, finances and excitement, among other things, influence gamblers’ behaviors. The transition rate from an exposed-to-casinos class to an excessive-gambling class is a decreasing function of education campaigns such as informing the elderly about the danger of gambling addiction and providing routine screening tests for gambling problems. An education campaign can be carried out by social workers, primary care providers and counselors among others. Depending on the intensity and severity of problems associated with gambling, some are forced to seek help such as clinical treatment or counseling, and some recover naturally from addiction to gambling without any professional treatment [10]. The former is measured by δ and the latter is done by ρ. The rates at which individuals in the R class relapse to A and succeed to recovery are modeled by η and ρ, respectively. The parameter μ is the per capita rate at which individuals age into the S population and age out of the system. The model is summarized by Figure 1 in schematic form.

Figure 1: A schematic diagram of the model
We obtain a system of four ordinary differential equations with these assumptions. The governing compartmental model is the following:
dS⁄dt = µN − βS E + A⁄N+ΨE + ρA + ϕR − μS
dS⁄dt = βS E + A⁄N − T(0)E − ( Ψ+ μ)E
dA⁄dt = T (0)E + nR − (ρ+ δ + μ)A
dR⁄dt = δA − (n + ϕ + μ)R
N = S + E + A + R
Results from stability analysis
We first re-scale and reduce the system, and then find the basic reproductive number R0 (see Appendix), which is interpreted as a tipping point in a sociological term, i.e., it is a point at which a stable system turns into an unstable one or vice versa, which is a threshold condition. In epidemiological models, R0 is interpreted as the average number of secondary cases caused by a typical single infected individual, hence the disease spreads if R0 > 1, and it dies out if R0 < 1. R0 shows how the gambling environment contributes to the gambling problems, and describes the relationship between transition rates among classes. This measurement is crucial in developing prevention strategies or control policies to limit gambling disorder
R0 = 1⁄2 [β⁄τ(0)+ψ+µ + ηδ⁄(η+φ+µ)(δ+ρ+µ) +
√ (β⁄τ(θ)+Ψ+µ) - ηδ⁄(η+φ+µ)(δ+ρ+µ))2 + τ(θ)β⁄(τ(θ)+Ψ+µ)(δ+ρ+µ)]
In order to interpret R0 in our model, we observe each term of R0 . The first term β⁄τ(θ)+ψ+µ expresses that individuals become casino gamblers at a rate of β and leave E after an average time of 1⁄τ(θ)+ψ+µ. The second term represents the fraction of excessive gamblers who seek treatment, δ⁄δ+ρ+µ, and then relapse to A,η⁄η+φµ before aging out of the system. R0 has to be greater than the max of these two, which is easily seen algebraically. Since the gambling disorder in our model is a progressive one, the square root rises from the two stages required for a susceptible person to become an excessive gambler. Observe the inequality:

The first term on the right side of (3) is the reproductive number for the at-risk class. The expressions in the radical of (3) represent the proportion of susceptible individuals who become frequent gamblers and then begin to show problem gambling behaviors (from S to E to A). I.e., the second term on the right of (3) is a reproductive number for the class with excessive gambling problems. R0 is less than the sum of these two because of the overlap from S to E in the two stages.
The possible end state for this model is (s , e , a , r ) = (1, 0, 0, 0), which is the Casino Free Equilibrium (CFE). This state will happen if individuals age out of the system faster than being exposed to casinos and enjoying casino games. I.e., if μ > , no problem gambling state will ever develop in this population, and all solutions will approach the CFE. If the basic reproductive number R0 is less than 1, the CFE is locally asymptotically stable. If R0 > 1, there is a unique endemic equilibrium solution, and it is always locally asymptotically stable if it exists. See Appendix for the details of equililbria.
Numerical simulations and discussions
We will run numerical simulations using the parameter values that we obtained in the Appendix section.
Computing R0 using (2) provides R0≈1.7. Figure 2 shows that the endemic equilibrium exists and locally asymptotically stable, which agrees with our stability analysis. In other words, gambling problems among older women are present in an endemic state. Our model shows that problem gambling among the elderly women is decreasing. This agrees with recent studies: after initial exposures to casinos among the population, adaptation occurs. LaPlants and Shaffer [11] described this phenomenon of problem gambling in terms of infectious public health perspective: after a rapid increase in the rate of infection among the population, resistance and immunity occur resulting in less infection. The figure indicates that the equilibrium point is (e (t), a (t))≈ (0.37, 0.09). The long-term behavior of the solution to our model shows that about 37% and 9% of the system population gamble socially and excessively, respectively. Note that the data we used to approximate parameters employed the Lie/Bet Questionnaire and had a prevalence rate of 10.4%.
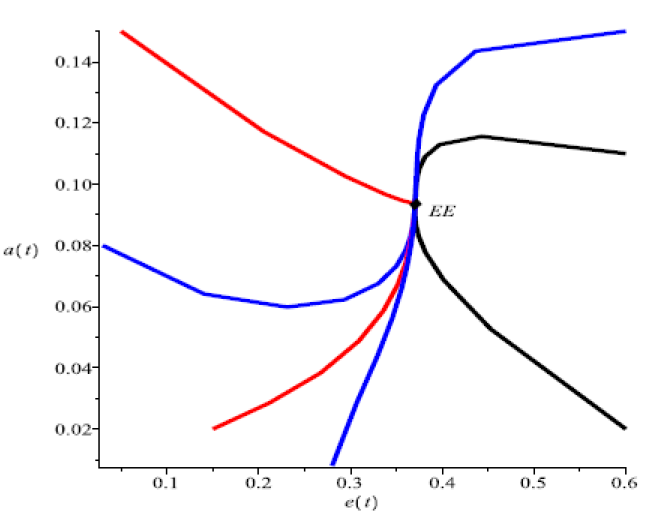
Figure 2: Stability
According to Zaranek, Chapleski and Lichtenberg[12][13], 18.2% of those who had any casino visits reported problem gambling behaviors. Figure 2 indicates that about 50% of the population are in E, A, or R, and about 10% are in A or R, which implies that about 20% of individuals who are exposed to casino gambling show gambling problems. This suggests that even social casino gambling is unsafe and often harmful.
Our model also corresponds to the studies[9][12][13][14]: a decrease of prevalence rates from 2002 to 2004 is shown in Figure 3; Figure 4 depicts the increase of susceptibles, 83% of those who reported visiting a casino in 2002 reported never visiting a casino in 2004. In our model, the transition rate from recreational gambling to problem gambling is actually a function of , where denotes the effect of an education campaign, although we could not approximate a function T(0) due to no data available. increases when we educate the elderly who enjoy social gambling, for example, informing the danger of gambling addiction and providing screening tests for gambling problems routinely as part of regular physicals, so is a decreasing function of . As stated by Zaranek, Chapleski and Lichtenberg [12,13], 18.2% of those who had any casino visits reported problem gambling behaviors. This strongly indicates that decent prevention should reduce social gambling, and this equates reducing the value of in the model. To see which is more effective to control gambling among older women, we apply sensitivity analysis to the basic reproduction number R0. Defining the sensitivity index of a threshold condition R for a parameter q by Sq = əR/əq q/R, we find the sensitivity indices of R0 for T and β. Using the parameter values we obtain ST≈ 0.037 and Sβ≈ 0.883, and find that the system is most sensitive to β. This is also shown by Figure 6. We varied T, .06, .048, .036, 20% less each time in Figure 5 and β, 1.029, .823, .617, similarly in Figure 6. They clearly show that reducing is more effective than reducing T, which displays that prevention should be stressed. For example, any retirement home should restrict the frequencies of buses to a casino. This confirms that an exposure to a casino involves a significant risk, which corresponds to the following among others: machine factors contribute to the development technological addictions; the effect of gambling settings, i.e., casinos; a complex interaction of individual and social factors such as a lack of leisure alternatives; gaming industry marketing strategies that target them including slot machine design factors; 80% of the 248 respondents of the follow-up study gambled for entertainment, 63% of them also gambled to win money; gambling disorder occurs on a continuum [8,9,15]. Women are over-represented in the older adult population, and elderly lonely women with disposable income are the most vulnerable population to electronic machine gambling. After all, for some elderly women, visiting a casino for fun with friends initially could be harmful.
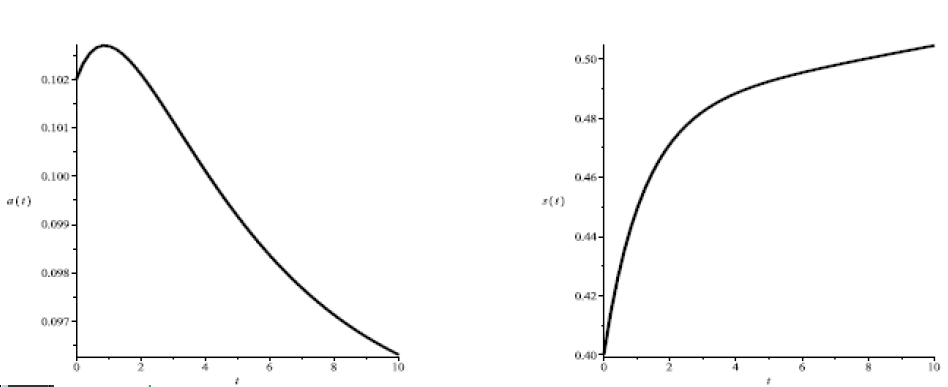
Figure 3 & 4: Decrease of prevalence rates, Increase of susceptible individuals

Figure 5 & 6: Varying : 0.06, 0.048, 0.036, Varying : 1.029, 0.823, 0.617
Appendix
Stability Anaysis
We first rescale the system (1) with the dimensionless variables s = S/N, e = E/N, a = A/N, and τ = R/N, then the model can be reduced to a system of three equations:
a' = τ(θ) + ητ - (ρ+δ+µ)a, (5)
τ' = δa - (η-φ+µ)τ, (6)
In order to calculate R0, we use the next generation operator method in Diekerman, Heesterbeek, and Metz [16]. We first solve for the equilibrium value τ* δa⁄η+φ+µ by setting Eq. (6) equal to zero, τ0 = 0, and substitute it in Eq.s (4) and (5). Then use two compartments, e and a, that gamble. Finding the Jacobian J of e and a evaluated at the CFE, and rewriting J in the form J = F −W, where all elements of F are positive and W is a diagonal matrix, provides R0. R0 is the dominant eigenvalue of FW−1. We state a few propositions omitting proofs.
Proposition 1 If β < μ, the CFE is globally stable.
Proposition 2 If R0 > 1, there is a unique endemic equilibrium solution, and it is always locally asymptotically stable if it exists. Summarizing, if R0 > 1, elderly women gambling is endemic, and the endemic state is locally
Parameter values
In order to establish model predictions, we estimate values for model parameter. Since there is very little data on older women and gambling specifically, some values are crude estimates. Therefore, our main objective is to see how closely model behavior corresponds to empirical observations, and to address that longitudinal study is needed for data-gathering.
The life expectancy of women in the United States is 80.6 years [17], so the average time an individual remains in the population is about 15 years, providing the rate at which an individual enters or leaves the system is μ≈1/15 yr−1.
MaKay’s paper [8] cites that less than 100 out of 12,348 older women 65 or older with gambling problems in Ontario called the Ontario Problem Gambling Helpline for assistance, only about 3% of people with gambling problems seek formal assistance, and older women are less likely to seek help than older men or younger people. Hence, we assume that about 2% of individuals of A seek help. Although the most commonly reported length of time experiencing problems with gambling is 2 to 5 years [18], Tavares et. al. showed that women had a significantly shorter duration of problem gambling than men [19]. Hence, we use 2 years for the average time that older women stay in A; we take δ≈ 0.02/2 yr−1.
In general, quitting problem gambling is easy, but staying away from gambling is a challenge. Collier says that about 90% of problem gamblers in the general population relapse [20]; however, the abstinence rate after recovery for older women is greater than younger population because of finances. One of the reasons why they started casino gambling was that it was less expansive and more affordable than other social activities [12]. Note that many gamblers think that they can still win even after some break from gambling due to a financial crisis; the combination of that thought and a convenient shuttle bus waiting for them leads them to a casino again when they have some money on hand. We take 80% for relapse and 20% for recovery within a year or so, and obtain n = 0.8 and ϕ= 0.2 yr−1.
Slutske [10] found that among individuals with a lifetime history of DSM-IV pathological gambling, about one-third recovered naturally without seeking any treatment, where the study subjects had a lifetime history of pathological gambling. Researchers speculate that whether leading older adults with gambling problem behaviors to engage in new activities is part of natural recovery [21]. Older adults who live with a fixed pension or social security fund have to stop betting when their money runs out, which is also related to a natural recovery rate. In the absence of available data on the natural recovery rate for older women with problem gambling, we take ρ≈0.33/2 yr−1 using an average of 2 years of duration in A as above.
The data from Detroit [14] in 2002 was analyzed by Zaranek, Chapleski and Lichtenberg: the studies included 1410 adults age 60 and older; 70% of them were female; the average age was 71.4 years; 66.7% either rarely or never visit casinos; 42.2% never visited a casino; 40.6% rarely to a few times a year; 17.2% monthly or more. Problem gambling behaviors yielded a prevalence of 10.4%, which was measured by the Lie/Bet Questionnaire; 18.2% of those who had any casino visitations reported problem gambling behaviors. Since the majority (70%) of 1040 older adults are female and there is no available data on gambling in older women only, we employ this set of data to estimate some transition rates between classes. There was a follow-up survey to 243 individuals chosen from those 1410 in 2004: 34% responded that they never visited a casino in the previous year; 41% reported less than monthly visits; 25% reported visiting a casino monthly or more[9]. It is unfortunate that we cannot employ this directly as a longitudinal study to measure because of two reasons: first, participants who gambled monthly or more were purposely over-sampled, resulting in 8% more problem gamblers in the final sample; second, the first frequency (to casinos) group of the three studies [12-14] above was never, never visited a casino before, which was not the same as no visit during the preceding year of the follow-up study [9]. Quantifiable correlation is obtained only from longitudinal studies with unbiased selection of subgroup and the same questionnaire over the periods.
Many researchers, Volberg [5], Tavaras [19] and Breen & Zimmerman [2] among others, agree that addiction to gambling for women is rapid, to which electronic machine gambling contributes greatly. Fowler finds that it takes about one to three years for older women to fall into excessive gambling when they gamble to relieve negative feelings of loss, isolation and boredom [22]. We will therefore use a conservative estimate of three years for the time it takes for older women to move from E to A. Since 18.2% of members of E report problems with gambling, we take T ≈ 0.182/3 yr−1. We will also simulate the model using a decreasing function of prevention factors, T(0).
The population of each class in 2002 is |R| = 3, |A| = 145 and |E| = 557, where absolute values denote the population: |A + R| is about 148 [ ≈ (1410)(0.104)]; or equivalently, 815 respondents (57.8% of 1410) had a casino visit, and about 148 individuals (18.2% of 815) belong to A or R; about 3 individuals (2% of 148) out of 1410 are in the R class; since 42.2% reported no casino visits before and 40.6% rarely to a few times a year, we assume that about half of them did not visit a casino in the previous year, so |E| = 557 [ ≈ (0.5)(1410) − 148]. According to Martin, Lichenberg and Templin in the follow-up study[9], about 83% of those who reported visiting a casino in 2002 reported never visiting a casino in 2004. Hence, 83% of 815 (57.8% of 1410) transitioned from E, A or R in two years, we have ψ|E| + ρ|A| + ϕ |R| = 1410 0.578 0.83/2. By using the above values for ϕ and ρ, we solve for our unknown parameter ψ , ψ ≈ 0.563 yr−1.
In the absence of a longitudinal study to estimate the value of , we assume that the rate of change of the susceptible class is very slow, i.e., s' ≈ 0. So the first equation of the system (1) with s = 1 − e − a − r is set to zero and we solve it for using all other parameter values we obtained above: β ≈ 1.03 yr−1.
References
Rivlin G (2004) The Tug of the Newfangled Slot Machines, The New York Times Megazine.View
Breen R, Zimmerman M (2002) Rapid onset of problem gambling in machine gamblers. J Gambl Stud 18: 31-44. View
Lee Y, Do TS (2013) A mathematical modeling approach to gambling among older adults. Appl Math Comput 221: 403-410.
Shaffer HJ, Korn DA (2002) Gambling and Related Mental Disorders: A Public Health Analysis. Annu Rev Pub Health 23:171-212.View
Volberg R (2003) Has there been a ”feminization” of gambling and problem gambling in the United States? J Gambl Iss.View
Petry N (2002) A comparison of young, middle-aged, and older adult treatment-seeking pathological gamblers. Genrontologist 42: 92-99.View
Suzanne K. Eckenrode (2013) Problem Gambling and Women.
McKay C (2005) Double Jeopardy. Int J Ment Health Addict 3: 35-53.View
Martin F, Lichtenberg PA, Templin TN (2011) A Longitudinal Study: Casino Gambling Attitudes, Motivations, and Gambling Patterns Among Urban Elders. J Gambl Stud 27: 287-297.View
Slutske W (2006) Natural Recovery and Treatment-Seeking in Pathological Gambling: Results of Two U.S. National Surveys. Am J Psychiat 163: 297-302.View
LaPlante D (2007) Shaffer H. Understanding the Influence of Gambling Opportunities: Expanding Exposure Models to Include Adaptation. Am J Orthopsychiat 77: 616-623.View
Zaranek RR, Lichtenberg PA (2008) Urban elders and casino gambling: Are they at risk of a gambling problem? J Aging Stud 22: 13-22.View
Zaranek RR, Chapleski EE (2005) Casino gambling among urban elders: Just another social activity? J Gerontol Soc Sci 60: 74-81.View
Chapleski E (2002) Facing the future: 2002 city of Detroit needs assessment of older adults. A Report for the City of Detroit Department of Senior Citizens; Wayne State University.
Institute of Gerontology. Center for Urban Studies; Center for Healthcare Effectiveness.
Griffiths M (199) Gamblin gtechnologies: Prospects for problem gambling. J Gambl Stud 15: 265-285.View
Diekmann O, Heesterbeek J, Metz J (1990) On the definition and the computation of the basic reproduction ration R0 in models from infectious diseases in heterogeneous population. J Math Biol 28: 365-382. View
Centers for Disease Control and Prevention. Life expectancy. Common Wealth of Australia. Gambling - Productivity Commission Inquiry Report.
Tavares H, Zilberman ML, Beites FJ, Gentil V (2007) Gender differences in gambling progression. J Gambl Stud 17: 151-159.
Collier R (2008) Gambling treatment options: a roll of the dice. Can Med Assoc J 179: 127-128. View
Hodgins DC, el-Guebaly N (1995) Natural and treatmentassisted recovery from gambling problems: A comparison of resolved and active gamblers. Addiction 95: 777-789. View
Fowler P (1997) Addiction crisis stage comes quick for slot players. National Council on Problem Gambling. Mississippi Sun Herald.