
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 2 (2018), Article ID: JPHIP-108
https://doi.org/10.33790/jphip1100108Research Article
Hospital-affiliated Medical Fitness Center Usage: Findings from a 12-week Weight Management Program
Matthew Nichols1*, Sonia Alemagno1, Peggy C. Stephens1, Chelsey Jackson2
1The College of Public Health, Kent State University, Lowry Hall, 750 Hilltop Drive, Kent, United States
2Cleveland Clinic Akron General Health and Wellness Center, Bath, 4125, Medina Road, Akron, United States
Corresponding Author Details: Matthew Nichols, The College of Public Health, Kent State University, Lowry Hall, 750 Hilltop Drive, Kent, United States. E-mail: mnicho22@kent.edu
Received date: 12th November, 2017
Accepted date: 08th January, 2018
Published date: 05th February, 2018
Citation: Nichols M, Alemagno S, Stephens PC, Jackson C (2018) Hospital-affiliated Medical Fitness Center Usage: Findings from a 12-week Weight Management Program. J Pub Health Issue Pract 2: 108.
Copyright: ©2018, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
The extent of obesity and over weightness in the United States, as well as the comorbidity and chronic disease that accompany them, are preventable. While evidence to support retail and commercial weight management programs is conflicted, hospital-affiliated medical fitness centers present a promising alternative. This study examined health outcomes associated with participation in a 12- week weight management program, sponsored by three hospitalaffiliated medical fitness centers..
Participants consisted of 13 male and 77 female participants, and mean age was 49.3 years. Participants reported increased health status (p<0.001), and reductions in unhealthy days in the past month (p<0.001), weight (p<0.001), and chronic pain (p=0.021). Participation was influenced by facility characteristics, such as staff knowledge (p<0.001), staff helpfulness (p<0.001), staff friendliness (p<0.001), facility location (p=0.002), and an on-site emergency room (p=0.002).These findings suggest that participants’ physical and mental health improved over the 12-week program, and that the addition of hospital-affiliated medical fitness centers amongst existing hospitals systems warrants consideration..
Keywords: Hospital-affilated medical fitness center, LifeStyles®, Health, Quality of life, Weight
Introduction
The extent of obesity and overweightness in the United States has been well-documented [1]. Classified as an individual with a body mass index (BMI) of 30 or greater, obesity has doubled since the 1970s, and current prevalence rates suggest that 36% of adults and 17% of youth are obese [1]. The inclusion of those considered overweight (BMI of 25 to 29.9) increases these figures considerably. Significant health risks are produced by both overweightness and obesity, as metabolic syndrome, type-II diabetes, hypertension, coronary artery disease, stroke, various cancers, poor reproductive function, osteoarthritis, and liver and gall bladder disease can all be linked to an elevated BMI [2]. Additionally, increases in comorbidity translate into increased medical spending; roughly $147 billion dollars in direct healthcare costs are attributed to obesity each year [3].
Despite the alarming proportion of overweight and obese individuals in the United States, these conditions are preventable. The adoption of a lifestyle rich in regular exercise, decreased sedentary activity, and a wholesome diet have the ability to both attenuate and prevent the poor health outcomes associated with overweightness and obesity [3]. Findings from a number of clinical and research-based weight management programs have affirmed the beneficial effects of exercise and a healthy diet in adults, highlighting improved healthrelated quality of life [4], enhanced physical function [5], improved cardio-metabolic condition [6], weight loss [4-7], and improvements in strength, balance, and gait [7]. Inversely, deteriorating strength, balance, and gait are associated with greater risk for fall and decline in physical function in adults 65 years of age and older [8].
Clinical and research-based weight management programs have illustrated a number of positive health out- comes [2], and evidence to support retail and commercial weight management programs remain unclear. While conflicting reports have both provided evidence against [9] and attesting to [10] the efficacy of commercial weight loss plans, they commonly display limited dietary adherence [11]; high costs, high attrition rates, minimal weight loss (3.2% over two years), a likelihood of participants regaining the weight lost, and limited measure- ment of health outcomes aside from weight are also associated with commercial weight loss plans [12]. Moreover, certain populations, such as those characterized by obesity [9], or elderly individuals who exercise with the attenuation of chronic conditions, loss of independence, and/or medication management in mind [13], report preferences to clinical and non-commercial weight loss settings.
Weight management programs conducted under the auspices of a hospital-affiliated medical fitness center present a promising alternative to retail and commercial weight management programs. Medical fitness centers operate largely on a model to, “…support the integration of wellness promotion and programming with traditional medical care…” [13] by incorporating clinical, physician, retail health, pharmacy, and fitness services in one convenient, centralized facility [14]. Hospital-affiliated medical fitness centers are likewise structured, falling under the umbrella of a one particular hospital system.
Hospital-affiliated medical fitness centers provide for greater cooperative care opportunity, blurring the tradi- tional dichotomy between fitness programming and medical care. An example of such cooperation can be illus- trated with physician referrals for exercise. Structured physician referrals, which range from written physical activity scripts to automatic referral schemes, have noted significantly higher rates of prescribed activity uptake, as compared to passive referral types, or no referral at all [15].
In order to evaluate the outcomes associated with the use of a hospital-affiliated medical fitness center, a study was undertaken to examine health outcomes associated with participation in LiteStyle®, a 12-week weight management program, conducted across a network of three hospital-affiliated medical fitness centers. Utilizing a singlesample and pre-test/post-test design, participants in the 12-week program were asked to complete a brief questionnaire, both upon orientation and during the final week of the program, which included questions from the previously validated CDC Healthy Days quality of life measures [16,17], as well as questions concerning facilityspecific participation influences, reasons for participation, and chronic pain. The inclusion of these measures was based largely upon previous findings regarding the age and health status of those utilizing hospital-affiliated medical fitness center facilities and programs [13].
Methods
Study Participants
Participants were included in the study if they were 18 years of age and older, had enrolled in the program, and were willing to complete both a pre- and post-program questionnaire. The program consisted of pre- and post-program fitness assessments and weekly group nutritional workshops administered by a registered dietician, addressing areas such as meal planning, dining out, and methods for boosting metabolism, as well as weekly dietician-graded participant food logs, bi-weekly personal training sessions (60 minutes), and meal planning.
Study Procedure
The study was approved by the Cleveland Clinic Akron General Institutional Review Board, and thereafter approved by Kent State University’s Institutional Review Board. The questionnaires were distributed to the program director and thereafter integrated into the program’s intake information, which was completed during program orientation (week 1). The same questionnaire was again distributed and completed during the last week of the program (week 12). Completion of the questionnaire was voluntary and did not affect any service other- wise owed to participants.
Data Collection
Data were collected from three different 12-week programs, occurring from: (1) August 31st to November 9th 2015, (2) January 19th to March 29th, 2016, and (3) May 4th to July 27th, 2016. At the end of each 12-week program, the director assigned an identification number linking participant questionnaire and program demo- graphic data, in order to ensure participant confidentiality. Revolving to different hospital-affiliated medical fitness center locations for enhanced availability, each of the three 12-week programs was held in a different Cleveland Clinic Akron General LifeStyles® facility, under the supervision of the same director.
Measures
Program content utilized for analysis included age, sex, physician referral, current medication status, medical history, pre- and postprogram weight, and personal program goals. The supplemental questionnaire contained four questions addressing current physical and mental health status (CDC Healthy Days), eight questions pertaining to Cleveland Clinic Akron General LifeStyles® facility influences, one question regarding chronic pain, and an open-ended question asking the participant to list the top three reasons for participating in the LifeStyle® program.
Data Analysis
Means and proportions are reported for categorical and continuous measures with the McNemar Chi-Square test and Paired Samples t-test, utilized as appropriate to determine if the change from pre-test to post-test was significant, given an alpha of 0.05.
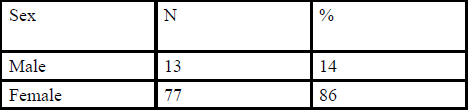
Table:1 Sex
Results
The sample consisted of 13 male and 77 female participants (Table 1), 23.3% of which were referred to the center by a physician, and mean age was 49.3 years (Table 2). Of the 90 participants, 82 (91.1%) participants were currently taking at least one medication (prescription or over-the-counter), while 19 (21.1%) were taking two to three medications, 21 (23.4%) were taking four to five medications, and 28 (29.9%) were taking six to ten medications; one individual was currently taking 15 medications (Table 2).
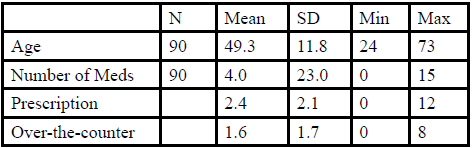
Table:2 Sample Characteristics
Table 3 contains the pre-test and post-test summary of those questions pertaining to participants’ reported health status. At pretest, participants were asked to rate their overall health, on a five point scale, from “poor” [1] to “excellent” [5]. On average, participants reported their overall health as “good” (mean = 3.0; SD = 0.9). Their reported health status increased at post-test to “very good” (mean = 3.4; SD = 0.7; p < 0.001).
At pre-test, participants reported an average of 3.1 (SD = 5.8) of the past 30 days were days that their physical health was not good, and this mean decreased significantly at post-test to 1.3 days (SD = 2.9; p = 0.003) (Table 3). Similarly, at pre-test, participants reported an average of 4.2 (SD = 7.1) of the past 30 days that their mental health was not good; this mean decreased at post-test to 1.5 days (SD = 4.4; p < 0.001) (Table 3). Respondents also reported a decrease in the mean number of days per month where poor physical or mental health kept them from their usual activities, from 1.4 days at pre-test (SD = 3.5) to 0.6 days at post-test (SD = 1.6; p = 0.030) (Table 3).
Overall, participants reported a significant reduction (p < 0.001) in the total number of unhealthy days in the past 30 days, from a pre-test mean of 6.7 (SD = 9.1) days to a post-test mean of 2.8 (SD = 5.3) days (Table 3). Moreover, there was a corresponding significant increase (p < 0.001) in the number of healthy days in the last month, from the pre-test mean of 23.3 (SD = 9.1) to a post-test mean of 27.3 (SD = 5.3) (Table 3).
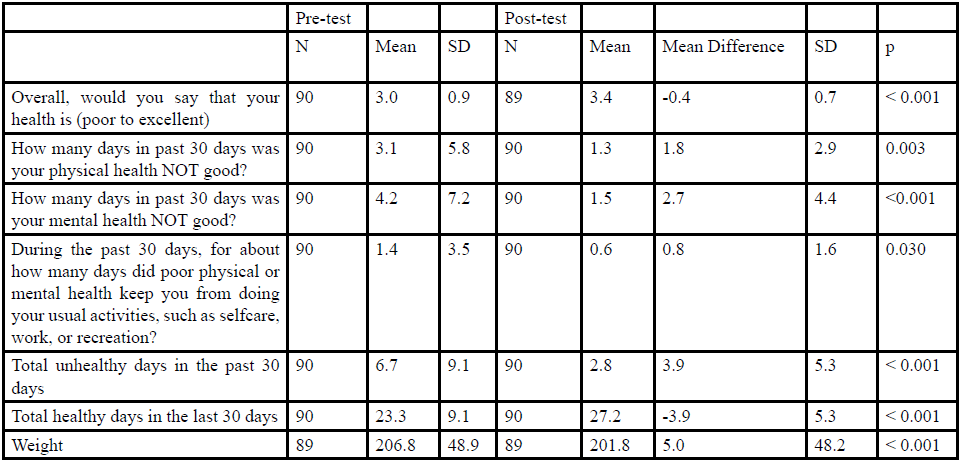
Table:3 Overall Health
Participants also demonstrated a significant (p < 0.001) reduction in weight over the program duration, from a pre-test mean weight of 206.8 lbs (SD = 48.9) to post-test mean weight of 201.8 lbs (SD 48.2) (Table 3). There was a significant decrease in the number of participants who reported having chronic pain, with 9 individuals reporting the attenuation of chronic pain from pre-test to post-test (p = 0.021) (Table 4).

Table:4 Chronic Pain (McNemar)
When asked to list the top three reasons for participating in the program, participants indicated desires to lose weight (53.3%), to achieve better health (15.6%), and to improve fitness (5.6%). Other frequently reported re- sponses included: to get stronger, to gain knowledge of nutrition and to develop better eating habits, and to have access to a personal trainer. The influence of Cleveland Clinic Akron General LifeStyles® facility characteristics also increased from pre-test to post-test, including staff knowledge (p < 0.001), staff helpfulness (p < 0.001), staff friendliness (p < 0.001), facility location (p = 0.002), and the presence of an on-site emergency room, or ER (p = 0.002) (Table 5).
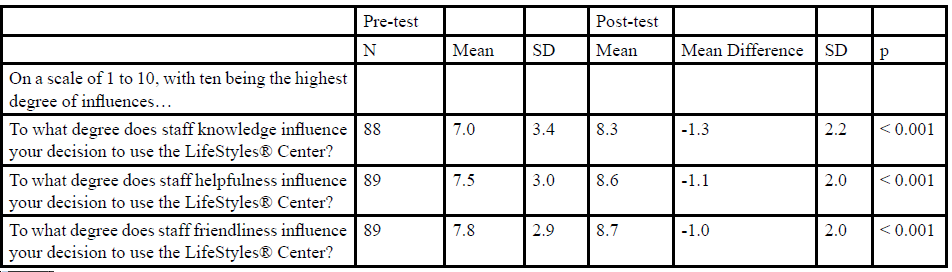
Table:5 Facility Influence
Discussion
Summary
This study examined the effects of a 12-week weight-loss program on self-reported health, including chronic pain, administered by Cleveland Clinic Akron General LifeStyles®, a hospital-affiliated medical fitness center program. Participants were surveyed before and after the program with regard to their overall health during the past 30 days, as well as their reasons for participation in the program.
Findings suggest that participants’ reported physical and mental health improved over the 12-week program, and these findings are consistent with previous findings surrounding the triadic relationship between exercise, physical health, and mental health [18]. Participants were intrinsically motivated to participate in the program, citing their own health as the strongest influence on participation.
Staff knowledge, helpfulness, and friendliness were also significant participation influences, as well as the facility location and the availability of ER services, all of which align with previous findings regarding the im- portance of staffing, convenience, and facility amenities [13]. More specifically, the relevance of ER services, which has been previously documented as a hospital-affiliated medical fitness center usage facilitator in elderly adults 65 years of age and older [13], may reflect the mean age of participants (49.3 years old), in addition to their intrinsic motivation for better health. The onset of chronic disease has been noted to develop at this age, with the potential for comorbidity advancing linearly with age [19].
Several study limitations should be noted. The sample includes all participants during the study time period who agreed to participate, but might not be generalizable to the overall profile of those participating in programs conducted in hospital-affiliated medical fitness centers. The measures, with the exception of weight, are based on self-report. Outcomes are limited to the results at the end of the 12-week program, and do not necessarily reflect potential outcomes sustained over time.
Overall, the health benefits associated with participation in a 12-week weight-loss program, conducted under the auspices of Cleveland Clinic Akron General LifeStyles®, a hospital-affiliated medical fitness center, appear to have provided notable physical and mental dividends to those who participated. Further investigation would do well to include direct comparisons to commercial health and wellness facilities, utilizing the same intervention across various age ranges, and providing for increased recruitment of male participants.
Acknowledgements
The authors would like to thank Cleveland Clinic/Akron General for facilitating the con- duction of this study across their three LifeStyles® centers.
Author Contributions
Matthew Nichols and Sonia Alemagno designed the study, developed the survey instru- ment, participated in data analysis, and wrote the manuscript. Margaret Stephens conducted data analysis, and provided several revisions to the manuscript. Chelsey Jackson conducted data collection and provided revisions to the manuscript. All authors read and approved the final manuscript.
Conflicts of Interest
The authors declare no conflicts of interest and do not have any financial disclosures.
Consent Statement
The authors declare that consent was obtained prior to participant involvement in this study. Participation in this study was voluntary, and did not affect services or membership otherwise owed to participants.
References
Ogden CL, Carroll MD, Fryar CD, Flegal KM (2015) Prevalence of obesity among adults and youth: United States, 2011–2014. NCHS data brief 219: 1-8.View
Franz MJ, VanWormer JJ, Crain AL, Boucher JL, Histon T, et al. (2007) Weight-loss outcomes: a systematic review and metaanalysis of weight-loss clinical trials with a minimum 1-year follow-up. J Am Dietetic Assoc 107: 1755-1767. View
Hammond RA, Levine R (2010) The economic impact of obesity in the United States. Diabetes Metab Syndr Obes. 3: 285-295.View
Williamson DA, Rejeski J, Lang W, Van Dorsten B, Fabricatore AN, et al. (2009) Impact of a weight management program on health-related quality of life in overweight adults with type 2 diabetes. Arc Internal med 169: 163-171.View
Miller GD, Nicklas BJ, Davis C, Loeser RF, Lenchik L, et al. (2006) Intensive weight loss program improves physical function in older obese adults with knee osteoarthritis. Obesity 14: 1219-30.View
Goodpaster BH, DeLany JP, Otto AD, Kuller L, Vockley J, et al. (2010) Effects of diet and physical activity interventions on weight loss and cardiometabolic risk factors in severely obese adults: a randomized trial. JAMA 304: 1795- 1802.View
Villareal DT, Chode S, Parimi N, Sinacore DR, Hilton T, et al. (2011) Weight loss, exercise, or both and physical function in obese older adults. New England J Med. 364: 1218-1229.View
Trombetti A, Hars M, Herrmann FR, Kressig RW, Ferrari S, et al. (2011) Effect of music-based multitask training on gait, balance, and fall risk in elderly people: a randomized controlled trial. Arch Internal Med 171: 525-33.View
Thomas SL, Lewis S, Hyde J, Castle D, Komesaroff P (2010) “The solution needs to be complex.” Obese adults’ attitudes about the effectiveness of individual and population based interventions for obesity. BMC Public Health 10: 420.View
Jolly K, Lewis A, Beach J, Denley J, Adab P, et al. (2011) Comparison of range of commercial or primary care led weight reduction programmes with minimal intervention control for weight loss in obesity: Lighten Up randomised controlled trial. BMJ 343: d6500.View
Dansinger ML, Gleason JA, Griffith JL, Selker HP, Schaefer EJ (2005) Comparison of the Atkins, Ornish, Weight Watchers, and Zone diets for weight loss and heart disease risk reduction: a randomized trial. JAMA 293: 43-53.View
Tsai AG, Wadden TA (2005) Systematic review: an evaluation of major commercial weight loss programs in the United States. Annals Internal Med 142: 56-66.View
Yang J, Kingsbury D, Nichols M, Grimm K, Ding K, et al. (2015) Using a qualitative approach for understanding hospitalaffiliated integrated clinical and fitness facilities: characteristics and members’ experiences. BMC Public Health 15: 567.View
Vanichkachorn G, Roy BA (2010) Health care reform and medical fitness facilities: an exciting future for wellness programs. ACSM’s Health Fitness J 14: 31-34.
Grace SL, Russell KL, Reid RD, Oh P, Anand S, Rush J, et al. (2011) Effect of cardiac rehabilitation referral strategies on utilization rates: a prospective, controlled study. Arc Internal Med 171: 235-241.View
Barile JP, Reeve BB, Smith AW, Zack MM, Mitchell SA, et al. (2013) Thompson WW. Monitoring population health for Healthy People 2020: evaluation of the NIH PROMIS® Global Health, CDC Healthy Days, and satisfaction with life instruments. Quality Life Res 22: 1201-1211.View
Moriarty DG, Zack MM, Kobau R (2003) The Centers for Disease Control and Prevention’s Healthy Days Measures– Population tracking of perceived physical and mental health over time. Health and quality of life outcomes 1: 37.View
Blair SN (2009) Physical inactivity: the biggest public health problem of the 21st century. British J Sports Med 43:1-2.View
Barnett K, Mercer SW, Norbury M, Watt G, et al. (2012) Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. The Lancet. 380: 37-43.View