
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 2 (2018), Article ID: JPHIP-110
https://doi.org/10.33790/jphip1100110Research Article
The Relationship Between Sense of Coherence and Rumination
Christine Williams1*, Matin Katirai2
Department of Health, West Chester University, West Chester, PA 19383, USA
Department of Geography & Planning, West Chester University, West Chester, PA 19383, USA
Corresponding Author Details: Christine Williams, Department of Health, West Chester University, West Chester, PA 19383, USA. E-mail: cwilliams3@wcupa.edu
Received date: 03rd November, 2017
Accepted date: 12th February, 2018
Published date: 09th March, 2018
Citation: Williams C, Katirai M (2018) The Relationship Between Sense of Coherence and Rumination. J Pub Health Issue Pract 2: 110.
Copyright: ©2018, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Background: Ineffective coping skills and rumination can worsen existing health conditions and contribute to disease and illness. Sense of coherence (SOC) positively influences coping and is one’s belief that life is meaningful, manageable, and understandable. People with higher rumination are much less likely to offer problem solving coping skills. The purpose of the study is to determine the relationship between SOC and rumination. Survey questionnaires were administered to 211 participants concerning sense of coherence (SOC), demographics and rumination. Linear regression was used to assess the association between SOC and rumination while controlling for gender, race, age and marital status. The model was found to be significant with a R2 value of 0.30. Results indicated that SOC has an inverse relationship with rumination, with a β coefficient of 0.38. Females are also much more likely to ruminate compared to males, with a β coefficient of 4.17. It is important to understand the relationship between SOC, a variable that can improve health, and rumination, a variable that can decrease health so that health educators and therapists can offer improved skills and techniques to improve thinking patterns, resilience and stress management..
Keywords: Rumination, Sense of coherence, Stress, Coping
Introduction
Hans Selye [1] was the first to document that stress increases the risk of morbidities and mortality (1956). Researchers indicate 75 – 90% of all visits to primary care physicians are due to stress related problems [2]. A plethora of research [3,4] continues to indicate deleterious health effects of stress such as increasing the risk of disease and/or worsening existing diseases. It is important to measure the relationship of stress with other negative cognitive behavioral patterns in order to create effective coping mechanisms to decrease stress and improve health. One variable to measure stress is using sense of coherence developed by Aaron Antonovksy using his Theory of Salutagenesis [5].
The Theory of Salutogenesis has been used previously to measure health because it offers insight into the origins of health, and why some people remain healthy while others do not [6]. The theory states health is a continuum; people are not in perfect health, but are on a health ease/dis-ease continuum [5,7] and that stressors are everywhere. The Theory of Salutogenesis incorporates components that support how humans can move towards health and manage stress and one main component is sense of coherence (SOC).
Sense of coherence (SOC) is the belief that one can manage in any situation regardless of what else is occurring and encompasses meaningfulness, comprehensibility and manageability. SOC is a resource that offers people the ability to manage tension, to self-reflect on their resources and use them [6]. SOC promotes effective coping, i.e., acknowledging solutions and resolving problems and develops through childhood and adolescence. By age 30, SOC is relatively stable and a skill that is set in place [8]. While SOC has been widely researched with response to physical, emotional, spiritual and mental health [6,9-11], no studies have conducted analysis on rumination.
Rumination is the behavior of reflecting on past distressful events or worrying about future events [12]. Rumination prevents problem solving thinking to remedy problems and is considered unproductive. Rumination has been found to negatively impact health such as increasing depression, anger and anxiety [13,14]. Research indicates rumination is considered a stable, individual trait [15] and is also known to have a direct relationship with stress [16-18]. Higher levels of rumination are associated with higher levels of stress. However, studies have shown that by adopting stress management skills, rumination decreases [19] despite rumination being a stable trait. A study on mindfulness demonstrated a negative correlation with rumination [20]. Positive stress management skills can improve rumination and thus improve overall health and wellbeing.
Researchers must consider targeting rumination when studying sense of coherence because rumination has been found to negatively impact health. Sense of coherence is the ability to manage stress and a higher sense of coherence is related to better health. To date, no studies have been published researching the relationship between sense of coherence and rumination. The aim of this study was therefore, to determine the relationship between SOC and rumination.
Methods
The purpose of this study was to determine the relationship between SOC and rumination using the Theory of Salutogenesis as the framework. A snowball sampling method yielded 211 surveys. The survey contained a scale to measure SOC names The Orientation to Life Questionnaire (OLQ) and created by Antonovsky [5] in 1987. The survey also contained a rumination scale, and demographics.
The OLQ contains 13 questions with a choice of seven Likerttype responses measuring 3 factors of SOC: manageability, comprehensibility and meaningfulness. Responses vary based on each question. An example of the responses for one question ranged from 1 (“never happened”) to 7 (“always happened”). The scoring is determined by summating all scores and averaging the summation by 13.
The Rumination-Reflection Questionnaire (RRQ) was used to measure rumination [21]. It is a two- section questionnaire; the first twelve questions are on rumination and the latter twelve questions are on reflection (not used in this study). The questionnaire has a 5-point Likert scale ranging from 1 (“strongly disagree) to 5 (“strongly agree).
The survey also included a demographic questionnaire consisting of age, gender and marital status questions were used. Approval for the study was obtained by the Internal Review Board of the University The majority of those who participated in the survey where from the Eastern United Sates, refer to figure 1, which displays the distribution of survey participants. The top three states where survey participants came from where Tennessee (63), Delaware (36) and Alabama (32). Participants needed to be 30 years of age or older. Approximately 50 % of the survey participants were in their thirties, 30% were in their forties and about 19% were over the age of fifty. Over 92% of the participants were non-Hispanic-white. Close to 65% of the survey participants were female and approximately 72% were married.
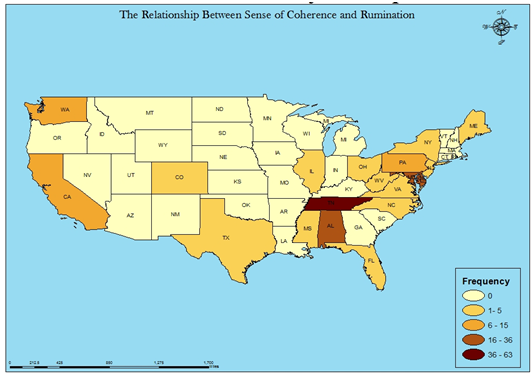
Figure:1 Distribution of Survey Participants
Linear regression was used to assess the association between SOC and rumination while controlling for gender, race, age and marital status. The outcomes of the liner regression included the unstandardized coefficients along with the significance values and the model summary R squared values.
Results
Participants scored on the upper end of SOC scores with M = 66.15, SD = 12.26. Scores ranged from 16 to 88 (n = 13) and were not normally distributed, refer to Table 1. No significant differences existed with descriptive variables and SOC.

Table.1 Table of Descriptive Statistics
Rumination scores averaged on the higher end of ruminating, M = 37.20, SD = 9.55, and were not normally distributed. Rumination scores for men were lower, M = 34.56, SD = 8.87, as compared to women, M = 38.66, SD = 9.63.
The model was found to be significant with a R2 value of 0.30 indicting that our model captures 30% of the variation of the rumination score, refer to Table 2. Results from the analysis indicate that SOC has an inverse relationship with rumination, with a β coefficient of -0.38. This means that for every one unit increase in the sense of coherence score we can expected the rumination score to decrease by 0.38 units, while controlling for gender, marital status, and age. Males were also more likely to have a rumination score that was 4.17 units lower when compared to females indicating that females tend to ruminate more. Marital status, race and age were not significant at the 95%, however marital status and age were significant at the 90% level. Descriptive variables were tested including age, gender, marriage status, race, pregnancy, BMI.
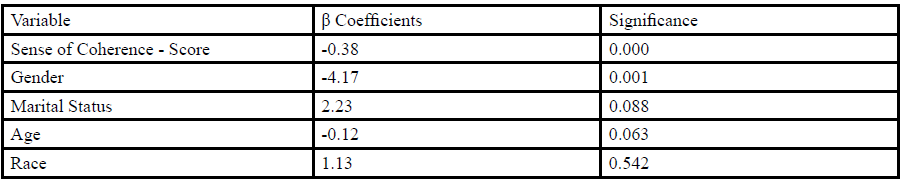
Table.2 Table of Linear Regression Results for Rumination and Sense of Coherence Dependent Variable: Rumination Score, R2 = 0.30
Discussion
This study expands the body of knowledge that one’s belief structure on meaningfulness, comprehensibility and manageability has a direct relationship with ruminative thoughts. Discerning the underlying relationship among stress and negative thought patterns is a meaningful endeavor to determine how beliefs impact physical and mental health. The purpose of this study was to assess the relationship between SOC and rumination.
Ample research indicates stress and the negative effects on health. SOC has been used as a measure for stress because the three components of SOC, meaningfulness, manageability and comprehensibility are central determinants in how we assess stressful encounters. Furthermore, SOC has a main, moderating and mediating effect on health and thus a stronger SOC is related to a better perception of overall health and particularly mental health. SOC is considered to be a health promoting resource. Although SOC has not been researched with rumination in previous studies results indicate similar findings that SOC predicts mental health status [6]. Results of this study indicate a negative relationship between SOC and rumination; rumination is lower if SOC is higher. Rumination negatively impacts mental health; research on rumination has been shown to predict depression and even posttraumatic stress disorder [22]. This study supports the existing body of research that negative thoughts and lack of ability to reframe and/or use effective coping techniques negatively impact one’s health.
Findings in this study indicate a gender difference with rumination. Previous research indicates women experience more rumination than men [12,17]. This study confirms a significant difference between gender and rumination. Because rumination involves people focusing on their problems and distress, rumination is a predictor of depression. Depression is the leading cause of disease-related disability in women [23]. Researchers must continue to examine the relationship between thought patterns, gender and mental health so that practitioners and researchers can create innovative and effective behavior modification techniques to mitigate suffering mentally and also prevent physical ailment manifestations as the link between mental and physical health is well published in medical and psychological journals.
This study had a small pool of participants that mainly inhabited the south, central and north east states of the US. Study participants mainly consisted of non-Hispanic-white females. A study that comprises a more inclusive and generalizable audience of the American public is recommended for future research. SOC and rumination are variables that impact all races and ethnicities and gender. Thus it is important to study participants with a wider variety of demographics. More research is needed on sense of coherence and rumination to better understand what behavior change techniques are effective and useful and how individuals can improve SOC to improve physical and mental health.
Conclusion
It is important to understand the relationship between SOC, a variable that can improve health, and rumination, a variable that can decrease health [24]. Health educators and mental health practitioners can offer improved skills and techniques to improve thinking patterns, resilience and stress management. In doing so, not only will physical health improve but mental and emotional health will enhance leading to potentially a longer life with a high quality of life. More research is needed on sense of coherence and rumination to better understand what behavior change techniques are effective and useful.
Conflict of Interest
All the authors declare no conflicts of interest.
References
Selye H (1958) The Stress of Life. New York: McGraw-Hill; 1958.View
Simmons SP, Simmons JC (1997) Measuring emotional intelligence. New York: Summit Publishing Group.
Hafen BQ, Frandsen KJ, Karren K, Hooker KR (1991) The health effects of attitudes, emotions and relationship. Provo UT: EMS Associates.
Segerstrom SC, Miller GE (2004) Psychological stress and the human immune system: A meta-analytic study of 30 years of inquiry. Psychol Bull 130: 601-630.View
Antonovsky A (1987) Unraveling the mystery of health: How people manage stress and stay well. Jossey-Bass.View
Eriksson M, Lindström B (2006) Antonovsky’s sense of coherence scale and the relation with health: a systematic review. J Epidemiol Commun Health 60: 376-381.View
Antonovsky A (1979) Health, stress, and coping.View
Antonovsky A (1993) Complexity, conflict, chaos, coherence, coercion and civility. Social Sci Med 37: 969-974.View
Eriksson M, Lindström B (2007) Antonovsky’s sense of coherence scale and its relation with quality of life: a systematic review. J Epidemiol Community Health 61: 938-944.View
Løvlien M, Mundal L, Hall-Lord ML (2016) Health-related quality of life, sense of coherence and leisure-time physical activity in women after an acute myocardial infarction. J Clinical Nurs.View
Surtees PG, Wainwright NW, Khaw KT (2006) Resilience, misfortune, and mortality: evidence that sense of coherence is a marker of social stress adaptive capacity. J Psychosomatic Res 61: 221-227.View
Nolen-Hoeksema S (1987) Sex differences in unipolar depression: evidence and theory. Psychological bulletin 101: 259.View
Modini M, Abbott MJ (2016) Negative rumination in social anxiety: A randomized trial investigating the effects of a brief intervention on cognitive processes before, during and after a social situation. J Behav Ther Exp Psychiatry 55: 73-80.View
Nolen-Hoeksema S (2000) The role of rumination in depressive disorders and mixed anxiety/depressive symptoms. J Abnormal psycho 109: 504.View
Smith JM, Alloy LB (2009) A roadmap to rumination: A review of the definition, assessment, and conceptualization of this multifaceted construct. Clin Psychol Review 29: 116-128.View
Marin KA, Rotondo EK (2018) Rumination and self-reflection in stress narratives and relations to psychological functioning. Memory 25: 44-56.View
Shull A, Mayer SE, McGinnis E, Geiss E, Vargas I, et al. (2016) Trait and state rumination interact to prolong cortisol activation to psychosocial stress in females. Psychoneuroendocrinol 74: 324-332.View
Willis KD, Burnett Jr HJ (2016) The Power of Stress: Perceived Stress and Its Relationship with Rumination, Self-Concept Clarity, and Resilience. North American J Psychol 18: 483.View
Querstret D, Cropley M, Fife-Schaw C (2018) Internet-based instructor-led mindfulness for work-related rumination, fatigue, and sleep: Assessing facets of mindfulness as mechanisms of change. A randomized waitlist control trial. J Occupational Health Psychology 22: 153.View
Raes F, Williams JM (2010) The relationship between mindfulness and uncontrollability of ruminative thinking. Mindfulness 1: 199-203.View
Trapnell PD, Campbell JD (1999) Private self-consciousness and the five-factor model of personality: distinguishing rumination from reflection. J Personal Social Psychol 76: 284.View
Valdez CE, Lilly MM (2016) Posttraumatic rumination: content, correlates, and processes. J Clin psychol.View
Noble RE (2005) Depression in women. Metabolism 54: 49-52.View
Eriksson M, Lindström B (2006) Validity of Antonovsky’s sense of coherence scale: a systematic review. J Epidemiol Commun Health 59: 460-466.View