
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 2 (2018), Article ID: JPHIP-113
https://doi.org/10.33790/jphip1100113Review Article
The Effects of Body weight on Sleep Quantity and Quality in College Students
Jason D. Wagganer*, Kylie A. Williamson, Lucas K. Shrum, Jeremy T. Barnes
Department of Health, Human Performance and Recreation, Southeast Missouri State University, Cape Girardeau, MO 63701, United States.
Corresponding Author Details: Jason D Wagganer, Department of Health, Human Performance and Recreation, Southeast Missouri State University, Cape Girardeau, MO 63701, United States. E-mail: jwagganer@semo.edu
Received date: 12th June, 2018
Accepted date: 15th March, 2018
Published date: 12th April, 2018
Citation: Wagganer JD, Wiloliamson KA, Shrum LK, Barnes JT (2018) The Effects of Body weight on Sleep Quantity and Quality in College Students. J Pub Health Issue Pract 2: 113.
Copyright: ©2018, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
The underlying factors which contribute to being overweight and/or obese are not fully understood. The pur- pose of this study was to assess the relationship between sleep patterns and body mass index (BMI) in American college students. The sample population (n=150, age=21.4±2.2 yr) at Southeast Missouri State University com- pleted a validated questionnaire. For the sample, 59.3% slept seven or more hours; 29.3% slept seven hours; and 40.7% slept less than seven hours. Twenty percent had a Pittsburgh Sleep Quality Index (PSQI) global score of less than five, while 80% had a global PSQI score of five or higher. Overall, as PSQI increased, sleep quantity decreased (p<0.001) and BMI increased (p=0.024). Moreover, as sleep quantity increased, eating out decreased (p=0.035) and days of eating breakfast increased (p=0.006). These findings suggest that both sleep quality and quantity are important factors in the contribution to lifestyle behaviors that may increase BMI overtime.
Key Words:Sleep quantity, Sleep quality, Obesity, Body mass index, Overweight
Introduction
The underlying factors which contribute to being overweight and/or obese are not fully understood. The purpose of this study was to assess the relationship between sleep patterns and body mass index (BMI) in American college students. The sample population (n=150, age=21.4±2.2 yr) at Southeast Missouri State University completed a validated questionnaire. For the sample, 59.3% slept seven or more hours; 29.3% slept seven hours; and 40.7% slept less than seven hours. Twenty percent had a Pittsburgh Sleep Quality Index (PSQI) global score of less than five, while 80% had a global PSQI score of five or higher. Overall, as PSQI increased, sleep quantity decreased (p<0.001) and BMI increased (p=0.024). Moreover, as sleep quantity increased, eating out decreased (p=0.035) and days of eating breakfast increased (p=0.006). These findings suggest that both sleep quality and quantity are important factors in the contribution to lifestyle behaviors that may increase BMI overtime.
Several factors contribute to being overweight and/or obese, and sleep problems may be one of the more significant. Lack of sleep has shown an association with obesity in both children and adults [3]. Sleep patterns (i.e., quantity and quality) can be evaluated through different instruments such as surveys or sleep monitors.
Many studies have used the validated Pittsburgh Sleep Quality Index (PSQI) survey to measure sleep patterns, as it is a convenient tool. According to the Sleep Health Index (SHI), Americans, aged 18 years and older, have reported sleeping an average of seven hours and 36 minutes per night [7]. Therefore, while Americans are obtaining the NSF recommended seven to nine hours of sleep per night, it is viewed as the low end of the range. Additionally, the SHI indicated that 35% of Americans reported sleep quality as “poor” or “only fair,” and 20% felt they did not wake up feeling refreshed during the prior seven days [7]. Individuals experiencing poor sleep quality include college-aged young adults. The NSF reported young adults, aged 18 to 29 years old, stay up later, and sleep longer, than older adults [7].
Going to bed later and sleeping longer into the next day is termed sleep phase delay. Most research suggests no change in sleep quantity or quality in younger [8]. and younger-middle aged [9]. individuals, who typically exhibit sleep phase delay. However, the majority of research does indicate that sleep phase delay does cause metabolic (i.e., glucose-insulin) disturbances, which can ultimately lead to an increased risk for carrying excess body weight.
The impact of inadequate sleep patterns on overweightness and obesity are well established. It has been suggested that very short sleep (<5 hours) and short sleep (5-6 hours) may be independent risk factors for becoming overweight or obese [10].. Moreover, in a survey study consisting of 3,927 American participants aged birth to 13 years, short sleep duration was significantly associated with an increased risk being overweight or obese [11]. Similar results were found in three to four year olds (n=1,311) from a survey which directly measured height and weight [12]. in three to seven year olds (n=244) with accelerometry measured sleep duration, and bioelectrical impedance (BIA) to measure BMI [13].. In European adolescents, aged 12.5 to 17.5 years (n=3,311), shorter duration of sleep resulted in significantly higher BMI values [14].. A survey study, involving direct measurement of height and weight, on 10 to 19 year olds (n=5,877) in Saudi Arabia, reported that short sleep duration and obesity were significantly associated with obesity [15]. Using various methodologies and conducting studies on a variety of ethnicities, research has indicated similar results regarding the correlation between sleep quantity and quality and BMI in children and adolescents.
Previous research has also suggested a correlation between reduced sleep and higher BMIs in both young and elderly adults. An inverse linear relationship was found between sleep duration and BMI among American participants >20 years old (n=13,742) [16].. A national cohort study of Thai adults, aged 20 to 49 years (n=87,134 in 2005; n=60,569 in 2009 at follow-up), also suggested a significant correlation between short sleep duration and obesity [17].. Moreover, a significant correlation between short sleep duration and obesity was found in a random sample of middle aged (45.3 yr) Australian adults (n=1,162) [18].. Through the use of a survey and polysomnog- raphy, poor sleep quality was associated with an increased BMI in 15 to 90-year-old Canadians (n=314) [19]. A similar significant correlation in participants (n=983) from the Netherlands, aged 57 to 97 years, by directly measuring height and weight and using wrist actigraphy to assess sleep duration [19]. Additionally, BMI was greatest in those who got the least amount of sleep when studying elderly participants (n=6,102), aged 67 to 99 years [20].
There are many variables that can contribute to a high BMI. Although the relationship between sleep patterns and a high BMI is multifactorial, it appears that poor sleep quantity and/or quality may be a more significant factor in becoming overweight or obese. It has been suggested that there is a correlation between poor sleep patterns (i.e., quality) and obesity in adults and children. This correlation has also been suggested in college students, although insufficient literature exists which examines the relationship. Therefore, the purpose of this study was to examine the multifactorial relationship of sleep patterns (i.e., quality) and BMI in college students.
Methods
Participants
The sample population included 18 to 32-year-old college students (n=150) at Southeast Missouri State University. This research was approved by Southeast Missouri State University’s College of Health and Human Sciences Research Involving Human Subjects Committee. Southeast Missouri State University is considered a large rural institution, with a campus population of ~11,000 students (27.6% residential, 72.4% commuter; 57% female, 43% male).
Procedures
The PSQI was used to collect data regarding sleep [21]. Students were stratified into BMI categories and were selected at random by walking around campus (at several different times and locations). Surveys were initially distributed in person (normal=72; overweight=65; obese=84) until a total of 50 participants were reached in each BMI category. An additional questionnaire pertaining to sleep habits, basic demographics, physical activity, eating habits, and lifestyle habits were included with the PSQI.
Sleep Quality
The PSQI is a validated, 19-item, sleep quantity and quality, self-report questionnaire that estimates sleep quality within the past month utilizing seven components (scored on a 0 to 3 scale) related to sleep habits that takes 5-10 minutes to complete [21]. The component scores are then added together to give a total global score ranging from 0 to 21. A global score of greater than or equal to 5 indicates poor sleep quality whereas a score of less than 5 indicates good sleep quality.
Sleep Duration
The duration of sleep for each participant was assessed using the PSQI question, “During the past month, how many hours of actual sleep did you get at night?” Sleep recommendations were used from the National Sleep Foundation: less than seven hours of sleep was considered ‘too little’, between seven and nine hours was the recommended, and more than nine hours was ‘too much’ [7].
Eating Habits
Participants were asked how often they participate in consuming breakfast, meals out, servings of fruits, vegetables, and sweets, and if they preferred a snack between meals for both the past week and in the past month.
Physical Activity
Participants were assessed on adherence to the American College of Sports Medicine (ACSM) guidelines of minutes per week for cardiorespiratory fitness and resistance exercise in the past month and a rating of perceived exertion (RPE) scale [22] was included for the participants to accurately estimate exercise intensity. Physical activity was defined as aerobic exercise performed, as follows: Moderate - at least five days per week at an intensity of 12-13 on the RPE scale for 30-60 minutes per day; Vigorous - at least three days per week at an intensity of 14-17 on the RPE scale for 20-60 minutes per day.
Days of Not Getting Enough Sleep the Night Before
Participants were assessed on likelihood to eat out, drink caffeine, snack more, watch more television, exercise, nap, or get out of bed early on days when they did not get enough sleep the night before.
Lifestyle Behaviors
Questions in this section pertained to smoking, alcohol, caffeine, and energy drink consumption.
Data Analysis
A Pearson correlation coefficient and One-Way Analysis of Variance were utilized to assess correlations between variables and differences across BMI categories and gender. BMI was categorized in the following manner: Normal: ≥18.5 and ≤24.9, Overweight: ≥25.0 and ≤29.9, and Obese: ≥30.0 [22].. Data was analyzed using IBM SPSS Software 24.0 (International Business Machines Corporation, Armonk, NY) with an α-level of p<0.05.
Results
Of the 150 college students who completed the survey and met participant guidelines [age=21.4±2.2 yr, ht=1.73±0.11 m, wt=85.9±25.5 kg (self-reported), and BMI=28.8±7.0 kg/m2], 45.3% were males (n = 68) and 54.7% were females (n = 82). The majority of the sample population (59.3%) reported getting seven or more hours of sleep, while 29.3% obtained an average of seven hours, and 40.7% slept less than seven hours. Twenty percent had a PSQI score of less than five (good sleep quality), while 80% had a PSQI score of five or higher (poor sleep quality). Descriptive data (Table 1), shows significant Pearson correlations between PSQI (Table 2), sleep quantity (Table 3), and BMI (Table 4) across various factors, are presented. Results from the One-way ANOVA are presented in Table 5-7. The BMI categories did not produce significant differences across PSQI (i.e., sleep quality) or sleep quantity across all participants or based upon gender.
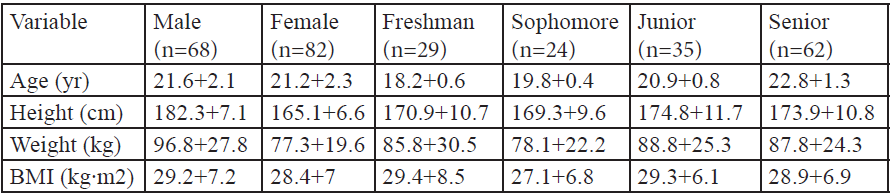
Table:1 Descriptive Characteristics.
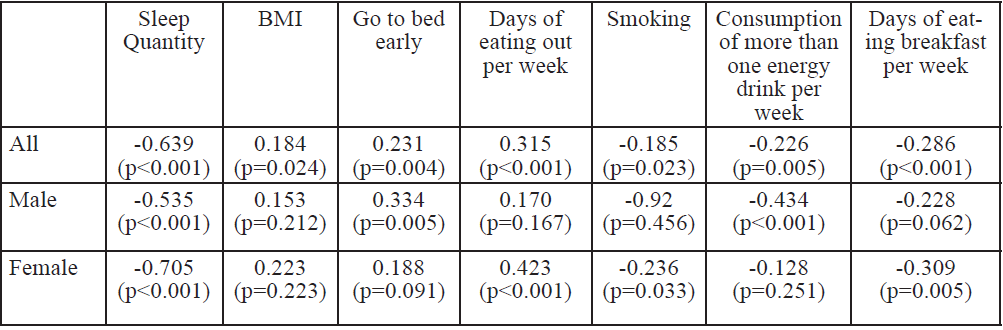
Table:2 PSQI Pearson Correlations.
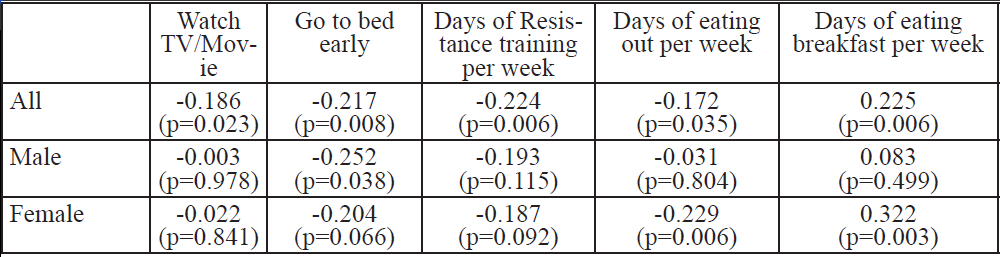
Table:3 Sleep Quantity Pearson Correlations.
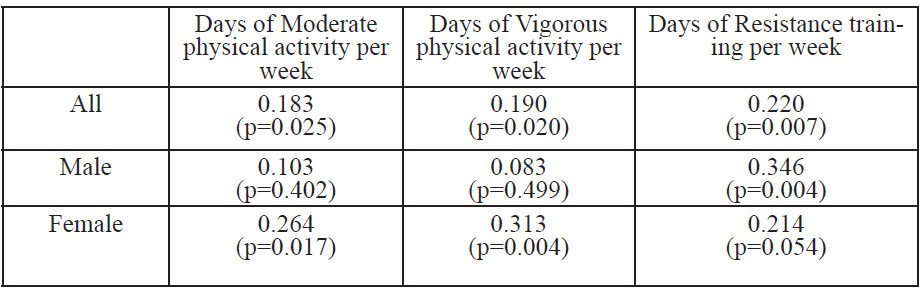
Table:4 BMI Pearson Correlations.
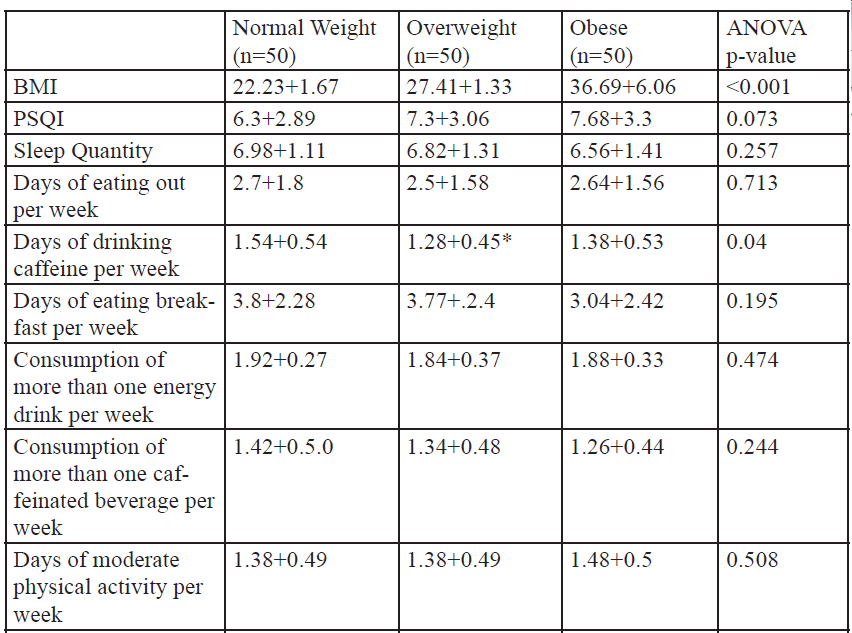
Table:5 One-way Analysis of Variance for BMI Categories.
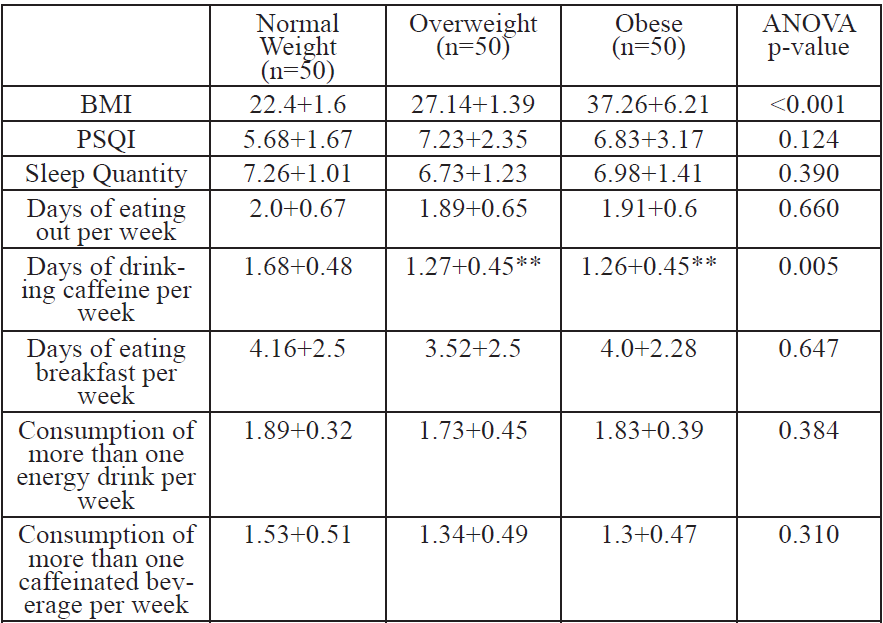
Table:6 One-way Analysis of Variance for BMI Categories for Males.
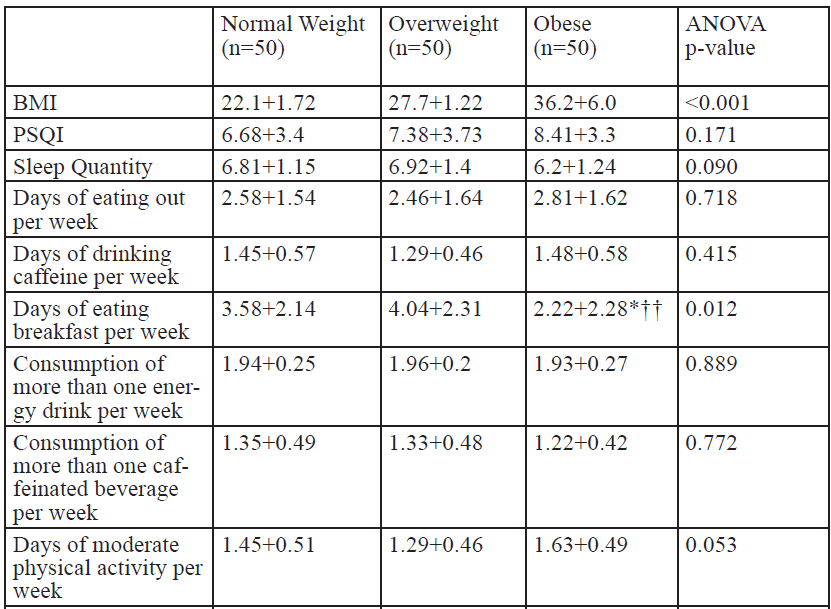
Table:7 One-way Analysis of Variance for BMI Categories for Females
Discussion
Much of the research previously conducted on sleep and obesity has found a significant negative relationship between BMI and quantity/quality of sleep in children, adolescents, adults, and the elderly [3,15,23]. Limited research has examined this relationship in college students in America and many studies fail to assess the influence of a larger number of variables associated with sleep quantity/quality and high BMI values. Therefore, this study targeted a specific population and attempted to assess the impact of lifestyle factors on BMI and quantity and quality of sleep. In support of our study, the majority (80%) of Patagonian, Chilean college students (n=832) did not receive good quality of sleep [24]. However, the majority of students (59.3%) in the current study obtained enough sleep (i.e. seven or more hours) which is in contrast to a study on Thai college students, which found 38.9% slept < six hours per day [25]. The reason for this contrast may be due the small sample size of the current study compared to 2,854 Thai college students [25]. Additionally, the ethnicity of the current study’s sample may account for, at least some of, the difference.
Eating Habits and Quantity/Quality of Sleep
The findings of this study showed that as sleep quantity increased, days of eating out decreased. This suggests that students who sleep longer are more likely to cook food for themselves whereas, students who do not sleep as much are more likely to eat out. Research has shown that foods eaten outside of the home are more likely to be high in total energy, total fat, saturated fat, cholesterol, and sodium [26]. Eating out can potentially lead to weight gain depending on food selection and quantity consumed. Therefore, the current study’s results were consistent with a study of pre-adolescent Canadians (n=56), in finding a correlation between poor sleep quantity/quality and poor eating habits [27]. The current study found no correlation among eating habits and BMI, which is not supported by a review article conducted over an 11 year time period on Middle Eastern children [26]. Additionally, the current study showed no significant relationships between sleep quantity/quality and fruit servings, vegetable servings, sweets/desserts servings, or snacks preferred, which conflicts with the findings on American college students (n=2,026) [28]. It is most likely the small sample size of the current study may explain the contrasting findings related to eating habits and sleep quantity/quality
Daily Physical Activity, Quantity/Quality of Sleep and BMI
An increased BMI being correlated with a decrease in moderate and vigorous physical activity, and resistance training is supported studies on Australian adults (n=1,162) [18]. and American college students (n=159) [29]. This suggests that college students with a higher BMI are less likely to participate in physical activity. An interesting finding of the current study was the positive correlation between BMI and moderate and vigorous physical activity for all participants. This finding was primarily due to females reporting more days per week of moderate physical activity and significantly more days per week of vigorous physical activity as BMI increased (Table 7). It is also possible this finding was due to the small sample size or lack of understanding/misreporting of physical activity levels when answering the survey. However, this finding is not supported by past research. There was a negative correlation between sleep quantity and resistance training (Table 3) (i.e., those who participated in more resistance training were likely to experience better sleep quantity). These results are similar a study on French adolescents (n=40) [30]. Therefore, these results suggest that resistance training may be an effective way to increase sleep duration in college students.
The Relationship between Days of Not Getting Enough Sleep the Night Before and Certain Activities (naps, television, drinking caffeine, etc.)
On days when participants did not get enough sleep the night before and felt tired, the majority indicated be- ing more likely to drink caffeine (61.3%), watch more television or movies (53.3%), not exercise (67.3%), nap (74%), and go to bed early (50%). These findings support a study that found shorter sleep was associated with increased screen time (i.e. television, computer, etc.) in European adults (n=6,037) [31]. These results suggest that adults who do not get enough sleep are at a higher risk for gaining weight due to an increase in sedentary behaviors.
Lifestyle Behaviors (smoking, alcohol, caffeinated drinks, and stimulant beverages) Effects on Quantity/ Quality of Sleep
Lifestyle behaviors such as smoking and consuming alcohol, caffeinated drinks, and energy drinks have also been shown to affect sleep patterns. In the current study, smokers had higher levels of poor sleep quality (i.e., high PSQI numbers) as compared to non-smokers, which is similar to a study conducted on Ethiopian college students (n=2,551) [32]. The findings of [24], who reported consumption of stimulant beverages (i.e., caffeine and energy drinks) was associated with poor sleep quality in Patagonian Chilean college students (n=994), support the findings of this study which showed poor sleep quality was associated consuming more than one energy drink per week. Interestingly, this study found no significant relationship between alcohol and sleep quantity/quality, which is not supported by [25], utilizing Thai college students (n=451 men/940 women) and American adults [33].. Again, the difference between the sample sizes in these studies and the current study may be the contributing factor for this contrast although nationality and/or ethnic differences may also play a role.
Skipping Breakfast, BMI, and Sleep Quantity/Quality
The findings that as sleep quality decreased the days of eating breakfast decrease are supported by research on Japanese adults (n=603) [34]. and Chinese college students (n=4,318) [35]. Another significant finding was that as sleep quantity increased, days of eating breakfast increased which was similar to a study reporting American college students (n=1,257) skipped breakfast were more likely to sleep <5.5 hours compared to those you ate breakfast [36].. These results suggest that sleep quality and quantity can both be a contributing factor to whether or not college students skip breakfast. Finally, in contrast to a study utilizing Malaysian college students (n=240) [37]., there was no relationship between BMI and days of skipping breakfast. Differences in nationality may be the reason for the contrasting findings in these two studies since [37] also used a survey to obtain information and had a similar sample size comparable to the current study.
Another inconsistency of studies regarding sleep and overweight/obesity is the utilization of BMI as the main anthropometric measurement, leaving other potentially more accurate anthropometric measurements (i.e., waist to hip ratio and skinfolds) unexplained [38]. While there are varied results in regards to the correlation between sleep quantity/quality and BMI, the majority of studies suggest that a correlation is present. However, it is not clear whether people who weigh more sleep less due to comorbidities associated with obesity or lack of sleep quality, or if lack of sleep causes weight gain due to increased hunger or late-night eating. It has also been sug- gested that there may be some unidentified confounding variable instead of there being a causal relationship in either direction. Another study found shorter sleep duration was associated with increased BMI and increased genetic influences on BMI in middle-aged American twins (n=1,088) [39]. These findings suggest that shorter sleep duration increases the expression of genetic risks for higher body weight later in life.
While the majority of studies have established the correlation between lack of sleep and an increased BMI, there are some inconsistencies. For example, no relationship was found between sleep duration and BMI in a longitudinal study of 723 American adolescents, where total sleep duration was self-reported and BMI was objectively measured [40].. This was one of the first studies to examine how change in sleep duration over time may relate to changes in body weight whereas, previous longitudinal studies examined how baseline sleep predicted future risk of obesity. With similar methods, no relationship between BMI and sleep quantity in Nepalese (n=241; 18 to 60 year olds) participants was reported [41]. These findings are particularly interesting, because the incidence of overweight (32.9-37.3%) [42] and obesity (7.2-8%) [44] is fairly high in Nepal. The findings of [41] may be due to the small sample size or possibly because the population included more active individuals since it was conducted in a busy mid-city location. However, a cross sectional study that directly measured height and weight and used a survey to obtain sleep duration found an inverse relationship (i.e., as BMI increased sleep quantity decreased) among 18 to 21 year old Karachi students (n=192) [44]. In contrast, a study using polysomnography and reports on sleep habits through surveys and sleep dairies found a U-shaped curvilinear relationship (i.e., <7.7 and >7.7 hours of sleep were associated with increased BMI whereas 7.7 hours of sleep was associated with lower BMI) between sleep duration and BMI among 30 to 60 year old American participants (n=1,024) [45]. This further supports the relationship between sleep duration and BMI is apparent, but the exact shape is not fully confirmed.
Although not many studies regarding the relationship between poor sleep quantity/quality and overweight/obe- sity have been conducted on college students in America, there have been several studies that have conducted research on this topic in other countries. The majority of these studies on Americans and other countries suggest that there is a correlation between poor sleep quantity/quality and overweight/obesity. This study has several potential limitations, the first of which is the utilization of a self-reporting questionnaire. Past research has found women are more likely to under report body weight [46]. Secondly, the study recruited more males (n=68) than females (n=82). However, past research has utilized unmatched gender pools with similar and larger sample sizes to this study, with supportive and opposing results. Thirdly, psychosocial stress (i.e., perceived and life event based) as it relates to BMI was not assessed. Past research has suggested stressful life events have an impact on the risk of weight gain in younger people [47,48] and stress (both perceived and life events) were associated with weight gain over a five year period [49]. Overall, the findings of the current study suggest that multiple variables are connected to an increase in BMI in college students. Factors such as sleep quality and/or quantity, physical activity, eating habits, and lifestyle habits are important in relation to the BMI of a college student. In this study, sleep quantity and quality were associated with different variables studied, in their own diverse ways; therefore suggesting that both sleep quality and quantity may uniquely contribute to an increase in BMI overtime. More research needs to be conducted on American college students in order to better understand the complex relationship between sleep, physical activity, eating habits, lifestyle habits, and BMI in this population.
Acknowledgments
The authors are not aware of any affiliations, memberships, findings or financial holdings that might be perceived as affecting the objectivity of this manuscript. This study was not supported by any funding.
Conflict of Interest
The authors declare no conflict of interest
References
National Institute of Diabetes and Digestive and Kidney Diseases (2012) Overweight and obesity statistics.View
Nieman DC (2010) Exercise testing and prescription: A health-related approach. Boston, NY: McGraw-Hill.View
Becutti G, Pannain S (2011) Sleep and obesity. Current Opinion in Clinical Nutrition & Metabolic Care 14: 402-412.View
Carter PJ, Taylor BJ, Williams SM, Taylor RW (2011) Longitudinal analysis of sleep in relation to BMI and body fat in children: the FLAME study. British Medical J 342: 1-7.
Hingorjo MR, Syed S, Qureshi MA (2009) Overweight and obesity in students of a Dental College of Karachi: lifestyle influence and measurement by an appropriate anthropometric index. J Pak Mel Assoc 59: 528-532.View
Knutson KL, Van Cauter E (2008) Associations between sleep loss and increased risk of obesity and diabetes. Annals of the New York Academy of Sciences 1129: 287-304.View
National Sleep Foundation (2014) Sleep health index.View
Gonnissen HK, Rutter F, Mazuy C, Martens EA, Adam TC, et al. (2012) Effect of a phase advance and phase delay of the 24-h cycle on energy metabolism, appetite, and related hormones. Am j Clin Nutr 96: 689-697.View
O’Reardon JP, Ringel BL, Dinges DF, Allison KC, Rogers NL et al. (2004) Circadian eating and sleeping patterns in the night eating syndrome. Obesity Research, 12: 1789-1796.View
Jean-Louis G, Williams NJ, Sarpong D, Pandey A, Youngstedt S, et al. (2014). Associations between inadequate sleep and obesity in the US adult population: analysis of the national health interview survey (1977-2009). BioMed Central Public Health 14: 290. View
Bell JF, Zimmerman FJ (2010) Shortened nighttime sleep duration in early life and subsequent childhood obesity. Archives of Pediatrics and Adolescent Medicine Journal, 164: 840-845. View
Jiang F, Zhu S, Yan C, Jin X, Bandla H et al. (2009) Sleep and obesity in preschool children. J Ped 154: 814-818. View
Carter PJ, Taylor BJ, Williams SM, Taylor RW (2011) Longitudinal analysis of sleep in relation to BMI and body fat in children: the FLAME study. View
GarauletM, Ortega FB, Ruiz JR, Rey-López JP, Béghin L, et al. (2011). Short sleep duration is associated with increased obesity markers in European adolescents: effect of physical activity and dietary habits. The HELENA study. Int J Obes 35: 1308-1317. View
Bawazeer NM, Al-Daghri NM, Valsamakis G, Al-Rubeaan KA, Sabico SL, et al. (2009) Sleep duration and quality associated with obesity among Arab children. Obesity 17: 2251-2253. View
Ford ES, Li C, Wheaton AG, Chapman DP, Perry GS, et al. (2014) Sleep duration and body mass index and waist circumference among US adults. Obesity 22: 598-607. View
Yiengprugsawan V, Banwell C, Seubsman S, Sleigh AC (2012) Short sleep and obesity in a large national cohort of Thai adults. Brit Med J Open 2. View
Milia LD, Vandelanotte C, Duncan MJ (2013) The association between short sleep and obesity after controlling for demographic, lifestyle, work and health related factors. Sleep Medicine 14: 319-323. View
Berg JF, Neven AK, Tulen JH, Hofman A, Witteman, JC, et al. (2008) Actigraphic sleep duration and fragmentation are related to obesity in the elderly: the Rotterdam study. Int J Obes 32: 1083-1090. View
Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ (1989) The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Research 28: 193-213. View
Borg G (1998) Borg’s perceived exertion and pain scales. Champaign, IL: Human Kinetics. View
Centers for Disease Control and Prevention. (2015).
Patel SR, Blackwell T, Redline S, Ancoli-Israel S, Cauley JA, et al. (2008) The association between sleep duration and obesity in older adults. Int J Obes 32: 1825-1834. View
Velez JC, Souza A, Traslavina S, Barbosa C, Wosu A, et al. (2013). The epidemiology of sleep quality and consumption of stimulant beverages among Patagonian Chilean college students. Sleep Disord 1-10. View
Lohsoonthorn V, Khidir H, Gardenia C, Lertmaharit S, Tadesse MG, et al. (2013) Sleep quality and sleep patterns in relation to consumption of energy drinks, caffeinated beverages and other stimulants among Thai college students. Sleep Breath 17: 1017-1138. View
Musaiger AO (2011) Overweight and obesity in eastern Mediterranean region: prevalence and possible causes. J Obes 1-17. View
Burt J, Dube L, Thibault L, Gruber R (2014) Sleep and eating in childhood: A potential behavioral mechanism underlying the relationship between poor sleep and obesity. Sleep Medicine 15: 71-75. View
Laska MN, Pasch KE, Lust K, Story M, Ehlinger E (2009) Latent class analysis of lifestyle characteristics and health risk behaviors among college youth. Prevention Science 10: 376-386. View
Wengreen HJ, Moncur C (2009) Change in diet, physical activity, and body weight among young-adults during the transition from high school to college. Nutrition Journal 8: 32. View
Mendelson M, Borowik A, Michallet A, Perrin C, Monneret D, et al. (2015) Sleep quality, sleep duration and physical activity in obese adolescents: effects of exercise training. Pediatric Obesity 11: 26-32. View
Lakerveld J, Mackenbach JD, Horvath E, Rutters F, Compernolle S, et al. (2016) The relation between sleep duration and sedentary behaviours in European adults. Obesity Reviews 17: 62-67. View
Lemma S, Patel SV, Tarekegn YA, Tadesse MG, Berhane Y et al. (2012) The epidemiology of sleep quality, sleep patterns, consumption of caffeinated beverages, and that use among Ethiopian college students. Sleep Disorders 1-11. View
Schoenborn CA, Adams PF (2008). Sleep duration as a correlate of smoking, alcohol use, leisure-time physical inactivity, and obesity among adults: United States, 2004-2006. CDC/NCHS, National Health Interview Survey]. View
Nishiyama M, Muto T, Minakawa T, Shibata T (2009) The combined unhealthy behaviors of breakfast skipping and smoking are associated with the prevalence of Diabetes Mellitus. Tohoku J Exp Med 218: 259-264. View
Cheng SH, Shih CC, Lee IH, Hou YW, Chen KC, et al. (2012) A study on the sleep quality of incoming university students. Psychiat Res 197: 270-274. View
Thiagarajah K, Torabi MR (2009) Irregular breakfast eating and associated health behaviors: a pilot study among college students. Health Edu 41: 1-10. View
Boo NY, Chia GJ, Wong LC, Chew RM, Chong W, et al. (2010) The prevalence of obesity among clinical students in a Malaysian medical school. Singapore Med J 51: 126-132. View
Ford ES, Li C, Wheaton AG, Chapman DP, Perry GS et al. (2014) Sleep duration and body mass index and waist circumference among US adults. Obesity 22: 598-607. View
Watson N F, Harden KP, Buchwald D, Vitiello MV, Pack AI, et al. (2012) Sleep duration and body mass index in twins: a gene-environment interaction. Sleep 35: 597-603. View
Lytle LA, Murray DM, Laska MN, Pasch KE, Anderson SE, et al. (2012) Examining the longitudinal relationship between change in sleep and obesity risk in adolescents. Health Edu Behav 40: 362-370.
Amatya M, Gorkhali B, Islam MN, Shrestha S (2014) Body mass index correlates with age but not with sleep duration in Nepalese adults. J Univer Coll Med Sci 2: 15-18. View
Vaidya A, Pokharel PK, Nagesh S, Karki P, Kumar S, et al. (2006) Association of obesity and physical activity in adult males of Dharan, Nepal. Kathmandu University Med J 5: 546-549. View
Padhye SM (2007) A study of body mass index (BMI) of Nepalese women attending gynecology clinic. J Nepal Med Assoc 46: 185-188. View
Hingorjo MR, Syed S, Qureshi MA (2009) Overweight and obesity in students of a dental college of Karachi: lifestyle influence and measurement by an appropriate anthropometric index. J Pakistan Med Asso 59: 528-532. View
Taheri S, Lin L, Austin D, Young T, Mignot E (2004) Short sleep duration is associated with reduced leptin, elevated ghrelin, and increased body mass index. PLOS Med 1: 210-217. View
Bowring AL, Peeters A, Freak-Poli R, Lim MS, Gouillou M, et al. (2012) Measuring the accuracy of self-reported height and weight in a community-based sample of young people. BMC Med Res Method 12: 175-179. View
Block JP, He Y, Zaslavky AM, Ding L, Ayanian JZ (2009) Psychosocial stress and change in weight among US adults. Am J Epidemiol 170: 181-192. View
Cameron AJ, Welborn TA, Zimmet PZ, Dunstan DW, Owen N et al. (2003). Overweight and obesity in Australia: the 1999–2000 Australian Diabetes, Obesity and Lifestyle Study (AusDiab). Med J Aust 178: 427-432. View
Harding JL, Backholer K, Williams ED, Peeters A, Cameron AJ, et al. (2014) Psychosocial stress is positively associated with body mass index gain over 5 years: Evidence from the longitudinal Aus Diab Study. Obesity 21: 277-286. View