
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 2 (2018), Article ID: JPHIP-118
https://doi.org/10.33790/jphip1100118Research Article
Trends in Substance Use Treatment Admissions among the Homeless in the United States: 2005-2015
Olubusayo Daniel Famutimi*, Kip R. Thompson
Master of Public Health Program, McQueary Family Health Science Hall, Suite 112, Office 118, 901 South National, Springfield MO 65897, USA.
Corresponding Author Details: Olubusayo Daniel Famutimi, Master of Public Health Program, McQueary Family Health Science Hall, Suite 112, Office 118, 901 South National, Springfield MO 65897, USA. E-mail: Famutimi82@live.missouristate.edu
Received date: 14th January, 2018
Accepted date: 17th July, 2018
Published date: 31st August, 2018
Citation: Famutimi OD, Thompson KR (2018) Trends in substance use treatment admissions among the homeless in the United States: 2005 -2015. J Pub Health Issue Pract 2: 118.
Copyright: ©2018, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Substance abuse is a significant public health problem among the homeless population in the United States. In this study, we sought to investigate the recent patterns of substance abuse among homeless people in the United States and estimate the prevalence of co-occurring mental illness in this population, using the substance use treatment episode data set for admissions (TEDS-A) during 2005 through 2015. Males and non-Hispanic Black Americans constituted a disproportionately high percentage of the admissions. Five substance groups accounted for 98.1% of primary substances reported between 2005 and 2015: alcohol (46%), opiates (24.6%), cocaine/crack (13%), methamphetamine (MA) (8.5%) and marijuana/hashish (6%). Though there was a decline in the proportion of admissions that reported alcohol abuse, alcohol was the most frequently reported substance of abuse at admission, while opioids (heroin and non-heroin opiates) were the most common illicit drug reported. Admissions due to opioid abuse showed a rising trend during the study period, increasing from 19.8% in 2005 to 30.3% in 2015. The proportion of admissions that reported current intravenous drug use also showed a marked increase from 17.4% in 2005 to 28.7% in 2015. The age of initiation to substance use reported for most admissions was 12- 17 years and the most common primary substance reported in this age group was marijuana. We observed certain age effects on the type of substance abused in chi square analysis that was statistically significant (p < 0.0001). Our result suggests that marijuana was the preferred substance of abuse among adolescents aged 12-17 years, and with a transition from adolescence to adulthood, young people (18-34 years old) preferred to abuse other illicit drugs, notably opioids. As individuals moved into middle age andolder, alcohol became the most commonly abused substance. Approximately onethird of admissions of homeless people had a diagnosis of a mental illness in addition to a substance use problem.
Substance abuse remains a significant problem among the homeless population in the United States. The changing pattern of substance abuse implies that more psychosocial and healthcare needs may arise. This has important implications in policy and service delivery designs to meet the growing needs of the homeless population. Healthcare service delivery design must inculcate a coordinated and integrated approach that emphasizes treatment of homeless people with substance abuse disordersand co-occurring mental illness in order to halt this growing menace.
Keywords: Substance Abuse, Mental Illness,Homeless, Initiation to Substance Use, Opioids, Marijuana, Alcohol, Methamphetamine, Cocaine, TEDS-A.
Introduction
Substance abuse is an issue of great concern in the United States and has been a central topic of national discussion in the public health arena within the past few years. The rate of substance use overdose and deaths (especially opioid) has reached epidemic proportions in the United States. The unprecedented scope of the opioid crisis led to its declaration as a national public health emergency by the United States President in 2017.
Substance abuse in the United States appears to impact every segment of the population. Nevertheless, homeless people are the most vulnerable population group affected [1]. The prevalence of substance abuse among the homeless is well reported in the literature. Substance abuse has been regarded as both a cause and a consequence of homelessness [2]. Addiction may cause people to lose their jobs and therefore, income and ability to afford housing [2, 3]. On the other hand, people who become homeless see substance use as way of coping with the stress of street life [3]. Substance use and abuse is the most common cause of homelessness in United States [4]. In numerous studies, over two-thirds of homeless people have cited alcohol abuse and illicit drug use as the major reason they became homeless [3-7]. In some situations, however, substance abuse could be a consequence of homelessness rather than a cause [2]. Homeless individuals often depend on alcohol and/or illicit drugs in order to cope with the stress and challenges of street life. This can potentially give rise to a new substance abuse problem or exacerbate an existing one. Drug overdose death is also a significant problem among homeless populations. A Boston cohort study of 28,033 homeless adults revealed that drug overdose death was the most common cause of death among a homeless population studied from 2003 to 2008, accounting for 17% of deaths. Of those overdose deaths, opioid overdose accounted for more than 80% [8].
Today's homeless population appears more diverse than previously thought. This population includes families, unaccompanied children and adolescents, people of color, lesbian, gay, bisexual, and transgender (LGBT) youth, veterans, the mentally ill, and people with substance use problems.
In 2004, homeless people accounted for 9.6% of substance use treatment admissions and increased to 14.8% in 2014 [9]. Substance abuse among homeless people is higher compared to people who have stable housing [10]. In 2015, of 1,497,126 substance use treatment admissions with known living arrangement, about 16% (n= 232,797) were homeless. Similarly,in one study [11], it was estimated that at least 50% of homeless persons had a substance use problem.
A Canadian study also revealed that alcohol abuse tends to be more common among homeless adults while illicit drug use was more common among homeless youths [3]. The literature is replete with evidence that substance abuse is much more common among homeless people than in the general population. In a survey of substance abuse disorders among 428 homeless and runaway adolescents aged 16-19 in Midwestern United States [12], it wasdetermined that approximately two-thirds of homeless people had a substance use disorder. Among those that had a substance use disorder, 93% had a mental disorder, including major depressive episodes, conduct disorder and post-traumatic stress disorder.
Most studies conducted in the 1990s revealed that marijuana, followed by cocaine were the drugs of choice among homeless people in the United States. For example, a Hollywood street youth study showed that 93% of homeless youths had used marijuana, 89% had abused alcohol and 50% had used cocaine or crack within the past month [13]. Another study [14] reported similar trends in the pattern of substance use in a study of homeless youths in the Midwest. In this study, 81% of homeless youths reported using alcohol, 69% marijuana, 27% amphetamines, 26% hallucinogens, 17% inhalants, 16% methamphetamine, 15% cocaine, 9% barbiturates, 7% tranquilizers and 6% opiates in the past year. Similarly, in a study of homeless and non-homeless adolescents seeking medical care in a Hollywood outpatient clinic, homeless adolescents were four times more likely to have used illicit drugs than non-homeless counterparts [15]. According to a Homeless and Transient Population Study [16], homeless people aged 26 to 34 were more likely to use marijuana and cocaine while those aged 35 or older were more likely to abuse alcohol.Contrasting studies have shown that in some communities, cocaine or crack is the drug of choice for homeless people. In a survey of 518 homeless men who were seeking treatment in a community healthcare center in New York between 1991 and 1994, over 47% reported crack as their primary substance of use, compared to 20% who reported alcohol [17]. Among 219 homeless restaurant workers interviewed in New York regarding substance abuse, 76% reported lifetime use of cocaine, 33% reported lifetime use of opiates (including heroin), and 29% reported alcohol binge drinking [18]. In another study of 1,326 homeless people receiving treatment from 12 substance abuse treatment facilities in Chicago, in which interval interviews were conducted at baseline, and at 6, 24, and 36 months, cocaine/crack was identified as the primary substance of abuse problem, which also predicted homelessness at baseline among those not homeless, and greater homelessness at 6 months [19].
In an analysis of a nationally representative data from the Treatment Episode Data Set for Admission (TEDS-A), alcohol was the primary substance of abuse for 49% of homeless people admitted to substance use treatment facilities in 2008, followed by opiates (22%), cocaine/ crack (14%), MA(6%), and marijuana/hashish (6%) [20]. Homeless people who have had five or more treatment episodes accounted for the highest proportion (34%) of admissions with prior treatment episode(s), while only 19%of non-homeless people have hadfive or more treatment episodes. This reflects a chronic pattern of drug use that is more prevalent among homeless people. More so, about 28% of admissions of homeless people were among those with a psychiatric diagnosis in addition to a drug or alcohol problem [20].
Though the reasons for homelessness among those with mental and substance use problems are many and varied, both substance use and mental disorders have been correlated with homelessness. Homeless people suffer substance abuse problems co-occurring with a mental illness. The high prevalence of this psychiatric comorbidity among homeless persons have been reported in previous studies [12,21-23].
The United States Department of Housing and Urban Development reported that 549,928 people were homeless on a night in 2016 [24]. Among these, 107,801 people had a severe mental illness and 94,496 people had a chronic substance use problem. This means one in five homeless persons either had a chronic substance abuse problem or a serious mental illness. The presence of co-occurring mental illness poses additional barriers to treatment and recovery, as there are only a few programs for the homeless that accept individuals with substance use problems co-occurring with mental illness. For example, some communities have treatment programs for homeless people with substance abuse problems but no program for those with psychiatric co-morbidities, others have programs for mental illness focused only on the homeless people without a substance abuse problem [25]. The lack of integration of these programs continue to present daunting challenges for various communities with such needs.
Over the past two decades, some efforts have been made to understand the pattern of drug use progression. A gateway hypothesis wasput forward to explain this pattern. This hypothesis suggests that individuals start with marijuana before progressing to use other illicit drugs [26,27]. The result of a national epidemiological survey of young people who started with marijuana, showed that about 45% progressed to use other illicit drugs later in life [28]. Multiple studies have also reported the gateway effect in the past, explaining how young people started with marijuana and later progressed to use other illicit drugs such as cocaine and heroin [29-32].
Substance abuse problems among homeless people in the United States have significant economic costs. On average, $40,500 of tax dollars are spent per homeless person per year. These costs include jail, shelter, emergency room visits and psychiatric services [33]. Homelessness and substance abuse are two complicated issues of great public health concern. Successful prevention and control require deeper insights into the pattern and trends of substance abuse over the years. The magnitude of thesubstance abuse among homeless personsmay outstretch the limit and capacity of healthcare and social services available for this vulnerable population group in many communities.
Substanceabuse among the homeless population constitutes a major public health issue in the United States. However, without understanding the pattern of the problem, it will be difficult to effectively halt the growing menace among this vulnerable population. A significant challenge of substance abuse in the United States is its potentially changing pattern [34]. However, only a few studies have examined recent patterns among homeless individuals in United States.The purpose of the present study is to investigate the recent patterns of substance abuse among homeless people and estimate the prevalence of co-occurring mental illness in this population, using national level data from TEDS-A during 2005 through2015. Specifically, we sought to estimate the percentage of admissions with known psychiatric diagnosis in addition to an alcohol or drug problem and also determine changes in the pattern of substance abuse among homeless people, the effect of age on the pattern of substance abuse and the critical age of initiation to substance use among homeless individuals.
Methodology
Data were obtained from a publicly available data set, TEDS-A. TEDS-A is a de-identified data set that is provided for public use by the Center for Behavioral Health Statistics and Quality under the auspices of the Substance Abuse and Mental Health Services Administration (SAMHSA). As TEDS-A is publicly available with subject de-identification; the Missouri State University Institutional Review Board exempted this study from review. TEDS-A provides demographic, substance abuse and treatment characteristics of admissions to alcohol or drug treatment in facilities that report to individual state administrative data systems. Demographic and substance abuse characteristics are self-reported.
Demographic characteristics include age, sex at birth, race, ethnicity, marital status, educational and employment status, source of income, living arrangement, geographic information (region and division) veteran status, health insurance and criminal history. Substance abuse characteristics include primary, secondary, and tertiary substances abused by the subject, and their route of administration, frequency of use, age at first use, source of referral to treatment, number of prior treatment episodes, number of substances reported at admission, presence of psychiatric diagnosis, where services were received, and planned use of medication assisted opioid therapy.
Data were analyzed with IBM® SPSS® Statistics 24. The present study is a descriptive analysis of substance use treatmentadmissions reported to the SAMHSAin TEDS-Afrom 2005 through 2015 for homeless people aged 12 years or older at the time of admission. This represents a total sample size of 2,594,317 admissions. The unit of our analysis was admissions rather than an individual. This is because an individual can have multiple admissions within the reporting year.
To examine if there were changing patterns, a descriptive analysis of substance abuse characteristics of admitted homeless people was done and compared for trends in admissions for the following primary substances abused: alcohol, marijuana/hashish, cocaine/crack, MA, other stimulants, heroin and other opiates (synthetic opiates and methadone), hallucinogens (phencyclidine and other hallucinogens), sedatives (benzodiazepines, other non-benzodiazepine tranquilizers, barbiturates and other barbiturate sedatives or hypnotics) and other drugs (inhalants and over-the-counter medications).
Demographic characteristics by age, sex, race/ethnicity and education level were compared. The primary substance of abuse was compared across six age groups: 12 to 17; 18 to 24; 25 to 34; 35 to 44; 45 to 54; and 55 years or older. Trends in admissions for alcohol, cocaine, marijuana, opiates and stimulants, were compared over time to identify key patterns. Substance abuse characteristics were analyzed including frequency of use by age of initiation, percentage of admissions with multiple drug use (defined as the use of more than one drug in addition to alcohol), percentage of admissions with prior substance use treatment episode, and the proportion of admissions with co-occurring mental illness. In addition, the proportion of admissions that included medication assisted opioid therapy (MAT) among those that reported opioid use was estimated over time. Finally, chi squared tests (alpha = 0.05) were used to determine the significance of association between age groups and substance abuse characteristics, as well as age of initiation, with special attention to age effects.
Results
During 2005 through 2015,there were 19,481,369 substance use treatment admissions aged 12 years or older reported. Homeless people accounted for 13.3% (N=2,594,317) of these admissions. From 2005 to 2012, reported substance use treatment admissions for homeless people varied between 12.5% and 13.5% of all substance use treatment admissions. However, it increased from 13.8% in 2013 to 15.5% of all admissions, in 2015
Males constituted majority of the admissions of homeless people, accounting for 74.2%, while females accounted for 25.8% (Table 1). Most of those admitted for treatment were aged 35-44 (28.7%) and 45-54 (27.9%) years. Homeless young people under the age of 18 years accounted for the fewest admissions (0.5%). Of the homeless people admitted for treatment, 77% were 30 years or older.NonHispanic Whites accounted for most of the admissions (51.7%) followed by Non-Hispanic Blacks (27.8%) and Hispanics (14.9%) (Table 1). Self or individual referrals were responsible for 46.1% of admission to treatment, while court/criminal justice system and community referrals constituted 16.5% and 14.4% of cases, respectively.
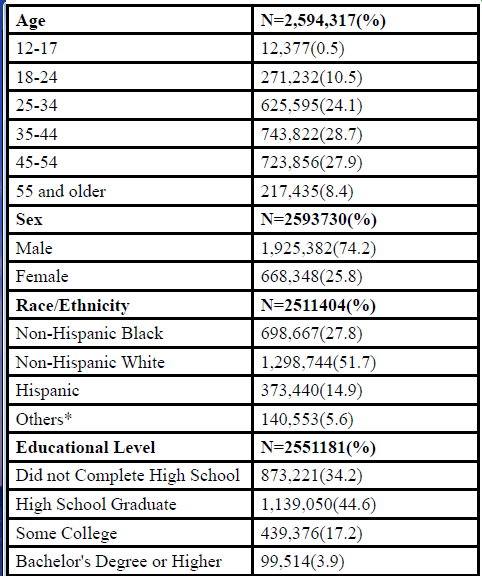
Table:1 Demographic characteristics of homeless people reporting any substance abuse at treatment admission, TEDS-A, 2005 to 2015
*Includes Native American and Alaska Native, Asian American, Native Hawaiian and Other Pacific Islander, and people of two or more races
Five substance groups accounted for 98.1% of primary substances of abuse reported from 2005 through 2015: alcohol (46%), opiates (24.6%), cocaine/crack (13%), MA (8.5%) and marijuana/hashish (6%). A downward trend was observed for primary alcohol land cocaine/crack abuse among admissions of homeless people from 2005 through 2015 (Figure 1). However, there was a marked increase in the proportion of admissions that reported primary abuse of opiates and MA (19.8% to 30.3%; and 5.4% to 12.7%, respectively). A moderate increase was also found in the proportion of admissions that reported marijuana abuse from 5.4% in 2005 to 6.1% in 2015. Approximately 45% of primary (illicit) drug use reported at admission between 2005 and 2015 were opioids (heroin and non-heroin opiates). The proportion of heroin admissions with treatment plans that included receiving medication assisted opioid therapy increased gradually from 12.1% in 2005 to 20.7% in 2015. This represents an average increase of 15.9% in this 11-year period.
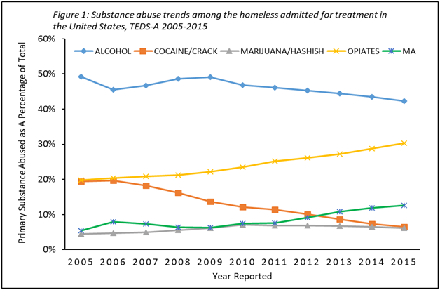
Figure: 1 Substance abuse trends among the homeless admitted for treatment in the United States, TEDS-A 2005-2015
Intravenous and/or intramuscular injection was the usual route of administration in 71.9% of admissions that reported heroin use. Meanwhile, for admissions that reported marijuana and cocaine, smoking was the usual route of administration in 96.7% and 82.9% of cases respectively.The proportion of admissions that reported current intravenous drug use also showed a marked increase from 17.4% in 2005 to 28.7% in 2015 (Figure 2).
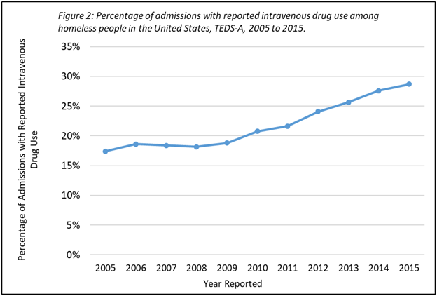
Figure: 2 Percentage of admissions with reported intravenous drug use among homeless people in the United States, TEDS-A 2005-2015
Approximately 33% of admissions had a co-occurring mental illness in addition to a substance abuse problem.Approximately 30% of admissions had no prior treatment episode, while 70% of admissions have had one or more prior treatment episode(s). Among admissions with one or more prior treatment episodes, those that have had five or more prior treatment admissions constituted the largest proportion, accounting for 25.6%. Though, the 11-year average (2005-2015) of admissions with five or more treatment episodes was 25.6%, certain changing trends were noted. From 2005 to 2008, the percentage of admissions with five or more treatment episodes showed some stability between 21% and 23%. Nonetheless, it increased from 25.6% in 2009 to 29.7% in 2015.
Findings showed that 73% of those who reported daily use of primary substance of abuse were initiated before the age of 21 years and 55.9% below the age of 18 years. Overall, more than half of homeless people admittedfor substance use treatment (56.1%) had used the primary substance of abuse before their eighteenth birthday.
The use of multiple drugs (two or more) was reported in 60% of admissions of homeless people. Similarly, homeless people aged 15-17 years old reported the highest use of multiple drugs (25.2%). Overall, 71.5% of homeless people who reported use of multiple drugs were under the age of 21 years while 54.7% were under the age of 18 years.
There was a statistically significant association (p < 0.0001) between age groups and substance use reported in chi-square analysis. Marijuana was the most frequently reported primary substance of abuse(Table 2). among admissions of homeless people aged 12-17 (63.9%), while opioids (heroin and other opiates) was most frequently reported for age groups 18-24 and 25-34 years (37.2% and 35.3% respectively). For all age groups, alcohol was the most frequent primary substance of abuse reported. Further analyses revealed that with increasing age, admission due to alcohol abuse increased, while admission due to opioid abuse decreased with age (Table 2).
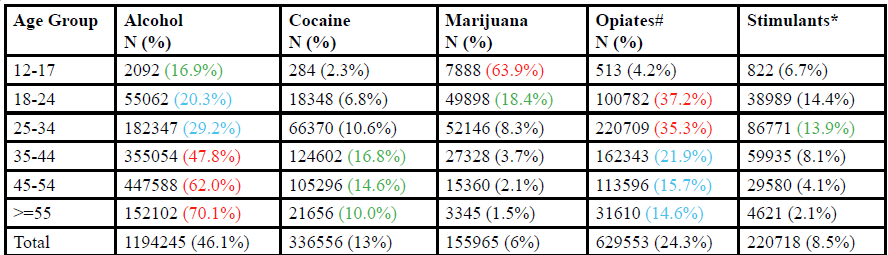
Table 2. primary substance of abuse reported by homeless people admitted for substance use treatment by age catagory, United States TEDS-A, 2005-2015.
Colors are used to demonstrate substances with high percentage of abuse within age catagories. red, blue and green indicate highest percentages in decreasing order.
#Include heroin, non-prescription methadone, other opiates and synthetics.
*Includes methamphetamine, amphetamine, phencyclidine and other stimulants
Age also affected the primary substance used. Based on chi square analysis(p < 0.0001), the most frequently reported primary substance of abuse among those aged 12-17 years was marijuana, accounting for almost two-thirds (63.9%) of primary substance reported. Among those aged 18-24 and 25-34 years, opioids (heroin and non-heroin opiates) were the most commonly reported substance of abuse (Table 2). A decrease in the proportion of admission due to primary opioid use with increasing age occurred within each age category, while the proportion of admission due to primary alcohol abuse within each age category increased with increasing age. As observed in this study, it appeared that marijuana use is a major problem of early initiates (12-17 years) while opioid use problems tend to develop with a transition from adolescence to adulthood. Though findings from this study suggests a gateway hypothesis as described in previous studies [26,27,29-32], it is not possible to infer a causal mechanism of marijuana-induced opioid sensitization due to the nature of this descriptive observational study. However, a neurobiological mechanism has been demonstrated using laboratory rats [45]. In the experiment, scientists were able to elicit behavioral sensitization to opioids after repeated exposure to delta (9)-tetra hydrocannabinol (cannabis/marijuana). This effect was nullified after administration of cannabinoid antagonists.
The large sample size derived from national level population data are major strengths of this study, as they increased the power of effect observed and made the present findings nationally representative. However, several limitations exist. The limitations of this study have to do with the inherent nature of the TEDS-A. The data includes treatment admissions, and in many states, the files may include multiple admissions for the same client reported within the same year. Therefore, the unit of analysis was admissions and not persons. Though TEDS-A captures more than 80% of all treatment admissions, it does not represent all admissions to substance use treatment facilities in the United States. TEDS-A only includes admissions at centers approved by a state to provide substance use treatment or those being administratively monitored for various reasons. The demographic and substance use characteristics of persons not seeking care in these centers may be different from what was observed in our study, and this might slightly impact the generalizability of our findings. In addition, not all participating states consistently reported admissions throughout the 11-year period (2005-2015). Therefore, substance abuse patterns by state or by region were not compared. Also, the self-reported nature of TEDS-A may be subject to recall bias. Lastly, some states have no opioid treatment programs (OTPs) that provide medicationassisted therapy using methadone and/or buprenorphine. Therefore, utilization of OTPs between states was not compared.
This study has several policy implications. The magnitude of repeated treatment admissions as well as the increasing number of homeless people with substance use problems co-occurring with a mental illness calls for a review of the current service delivery model designed for homeless people. Housing first service delivery model offers permanent housing to homeless people with substance use problems and/or mental illness without any treatment precondition [46]. In contrast, treatment first approaches make it a precondition for people with substance use problems and/or mental illness to start treatment first and then show evidence that they are prepared to live in permanent housing before they are provided such [47]. The treatment first approach dominates many service delivery models and policy designs [47]. However, it has been shown in several studies [46-50] that housing first approaches yield better results compared to treatment first approaches in terms of treatment adherence, housing retention rates, utilization of crisis services, quality of life and psychosocial outcomes
To improve treatment outcomes and reduce treatment readmissions, housing first service delivery model should be reconsidered in public policy designs. More so, better utilization of MAT among homeless people may be seen with housing first service delivery models. Additionally, as more advocates push for a flexible marijuana policy across many states, it should be put into perspective that adolescents aged 12-17 years are the highest abusers of marijuana and the continued use of marijuana has been shown to trigger the abuse of other illicit drugs, especially heroin and other opioids [26,27,29-32]. Also, the high number of initiates at ages 12-17 years make this age group an important target for intervention and therefore, substance abuse prevention programs should remain a priority for this age group.
Conclusion
The proportion of admissions to substance abuse treatment programs attributable to homeless people increased during the study period. Substance abuse remains a significant problem among the homeless population in the United States. Though the proportion of substance use treatment admission that reported alcohol declined, alcohol remained the most frequent reason for the admission of homeless persons during the study period, while opioid was the most common illicit drug reported at admission.The critical age of initiation was 12-17 years and marijuana appeared to be the drug of choice for this age group. It appeared that most early initiates (12-17 years) first experimented with marijuana and then proceeded to use other illicit drugs, notably heroin during the transition from adolescence to adulthood, while alcohol became more commonly abused in the older age groups. Adolescents aged 12-17 years should be major target for substance abuse prevention programs. The increase in the proportion ofsubstance use treatment admissions for people that are homeless, the high prevalence of psychiatric co-morbidity observed, and the rising rate of intravenous drug use found in the present study, are indications that substance abuse among the homeless population is a very serious problem. The low utilization of MAT for persons with opioid abuse problems suggests a service need for the homeless. Current service delivery models for homeless people with substance use problems should be reviewed to meet this growing need. A coordinated and integrated approach that emphasizes treatment and recovery of homeless people with substance use disorder and co-occurring mental illness needs to be adopted.
References
Gomez R, Thompson SJ, Barczyk AN (2010) Factors associated with substance use among homeless young adults. Substance Abuse 31: 24-34. View
Johnson TP, Freels SA, Parsons JA, Vangeest JB (1997) Substance abuse and homelessness: social selection or social adaptation? Addiction 92: 437-445.View
Didenko E, Pankratz N (2007). Substance use: Pathways to homelessness? Or a way of adapting to street life. Visions: BC’s Mental Health and Addictions Journal 4: 9-10.View
National Coalition for Homelessness (2009) Substance abuse and homelessness.View
Glasser I, Zywiak, WH (2003) Homelessness and substance misuse: A tale of two cities. Substance Use and Misuse 38: 551-576.View
Fountain J, Howes S, Marsden J, Taylor C, Strang J (2003) Drug and alcohol use and the link with homelessness: results from a survey of homeless people in London. Addiction Research & Theory 11: 245-256.View
O'toole, TP, Gibbon JL, Hanusa BH, Freyder, PJ, Conde AM et al. (2004) Self-reported changes in drug and alcohol use after becoming homeless. American Journal of Public Health, 94, 830-835.View
Baggett TP, Hwang SW, O’Connell JJ, Porneala BC, Stringfellow EJ, et al. (2013) Mortality among homeless adults in Boston: shifts in causes of death over a 15-year period. JAMA Intern Med 173: 189–195.View
Substance Abuse and Mental Health Services Administration, Office of Applied Studies (2006) Treatment Episode Data Set (TEDS). Highlights - 2004. National Admissions to Substance Abuse Treatment Services, DASIS Series: S-31, DHHS Publication No. (SMA) 06-4140, Rockville, MD.View
Baer, JS, Peterson P L, Wells EA (2004) Rationale and design of a brief substance use intervention for homeless adolescents. Addiction Research & Theory 12: 317-334.View
Baumohl J, Huebner RB (1991) Alcohol and other drug problems among the homeless: Research, practice, and future directions. Housing Policy Debate 2: 837-866.View
Whitbeck LB, Johnson K, Hoyt DR, Cauce, AM (2004) Mental disorder and comorbidity among runaway and homeless adolescents. Journal of Adolescent Health, 35: 132–140.View
Kipke MD, Montgomery SB, Simon TR, Iverson EF (1997) “Substance abuse” disorders among runaway and homeless youth. Substance use & misuse 32: 969-986.View
Bao WN, Whitbeck LB, Hoyt DR (2000) Abuse, support, and depression among homeless and runaway adolescents. Journal of Health and Social Behavior, 408-420.View
Yates GL, Mackenzie R, Pennbridge J, Cohen E (1988) A risk profile comparison of runaway and non-runaway youth. American Journal of Public Health 78: 820–21.View
Lambert, EY, Caces, MF (1995) Correlates of drug abuse among homeless and transient people in the Washington, DC, metropolitan area in 1991. Public Health Reports 110: 455.View
Rahav M, Link BG (1995) When Social Problems Converge: Homeless, Mentally ill, Chemical Misusing Men in New York City. International Journal of the Addictions, 30: 1019-1042.View
Magura, S, Nwakeze, PC, Rosenblum A, Joseph H. (2000) Substance misuse and related infectious diseases in a soup kitchen population. Substance use & misuse 35, 551-583.View
Orwin RG, Scott CK, Arieira C (2005) Transitions through homelessness and factors that predict them: three-year treatment outcomes. Journal of Substance Abuse Treatment, 28: S23-S39.
Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality (2010) Treatment Episode Data Set (TEDS): 1998-2008. State Admissions to Substance Abuse Treatment Services, DASIS Series: S-55, HHS Publication No. (SMA) 10-4613, Rockville, MD.
Feitel B, Margetson N, Chamas J, Lipman C. (1992) Psychosocial background and behavioral and emotional disorders of homeless and runaway youths. Hospital and Community Psychiatry 43, 115–159.View
McCaskill P, Toro P, Wolfe S (1998) Homeless and matched housed adolescents: A comparative study of psychopathology. Journal of Clinical Child Psychology 27: 306–319.
Cauce AM, Paradise M, Ginzler J, Embry L, Morgan C, & Lohr Y, et al. (2000) The characteristics and mental health of homeless adolescents: Age and gender differences. Journal of Emotional and Behavioral Disorders 8: 220–239.
United States Department of Housing and Urban Development (2016). Continuum of care homeless assistance programs homeless populations and subpopulations 2016 report.
Fisher GL, Roget NA (2009) Encyclopedia of substance abuse prevention, treatment, and recovery. SAGE Publications, Thousand Oaks, California.View
Kandel DB, Yamaguchi K, Chen K (1992) Stages of progression in drug involvement from adolescence to adulthood: further evidence for the gateway theory. Journal of studies on alcohol 53: 447-457.View
Kandel DB, Yamaguchi K, Klein LC (2006) Testing the gateway hypothesis. Addiction, 101: 470-472.View
Secades-Villa R, Garcia-Rodríguez O, Jin CJ, Wang S, Blanco C (2015) Probability and predictors of the cannabis gateway effect: a national study. International Journal of Drug Policy, 26: 135-142.View
O'Donnell JA, Clayton RR (1982) The stepping-stone hypothesis—marijuana, heroin, and causality. Chemical Dependencies: Behavioral & Biomedical Issues, 3: 229–241.View
Fergusson DM, Boden JM, Horwood LJ (2006) Cannabis use and other illicit drug use: testing the cannabis gateway hypothesis. Addiction, 101(4), 556–569.View
Makanjuola VA, Oladeji BD, Gureje O (2010) The gateway hypothesis of substance abuse: an examination of its applicability in the Nigerian general population. Substance Use & Misuse, 45: 1558–1571.View
Mayet A, Legleye S, Falissard B, Chau N (2012) Cannabis use stages as predictors of subsequent initiation with other illicit drugs among French adolescents: use of a multi-state model. Addictive Behaviors, 37: 160–166.View
Culhane, DP, Metraux S, Hadley T (2002) Public service reductions associated with placement of homeless persons with severe mental illness in supportive housing. Housing policy debate, 13: 107-163.View
Sloboda Z, Kozel NJ (2004) Understanding drug trends in the role of the Community Epidemiology Work Group as part of a comprehensive drug information system. The practice of drug abuse epidemiology 55: 41.
Martin CE, Longinaker N, Terplan M (2015) Recent trends in treatment admissions for prescription opioid abuse during pregnancy. Journal of Substance Abuse Treatment, 48: 37–42.View
Aidala A, Cross JE, Stall R, Harre D, Sumartojo E (2005) Housing status and HIV risk behaviors: Implications for prevention and policy. AIDS Behav 9: 251–265.View
Bourgois P (1998) The moral economies of homeless heroin addicts: confronting ethnography, HIV risk, and everyday violence in San Francisco shooting encampments. Subst. Use Misuse 33: 2323–2351.View
Briggs D, Rhodes T, Marks D, Kimber J, Holloway G, Jones S (2009) Injecting drug use and unstable housing: scope for structural interventions in harm reduction. Drugs 16: 436–450.View
Roy E, Boivin JF, Leclerc P (2010) Initiation to drug injection among street youth: a gender-based analysis. Drug Alcohol Depend 114: 49–54.View
Song JY, Safaeian M, Strathdee SA, Vlahov D, Celentano DD (2000) The prevalence of homelessness among injection drug users with and without HIV infection. J. Urban Health 77: 678–687.View
Towey K, Fleming M (2006) Policy and Resource Guide: Alcohol Use and Adolescents. American College of Preventive Medicine and American Medical Association National Coalition for Adolescent Health, Chicago, Illinois.
Bonnie RJ, O’Connell ME (2004) Reducing Underage Drinking: A Collective Responsibility. The National Academies Press, Washington, DC.View
American Congress of Obstetricians and Gynecologists (2008) At-risk drinking and illicit drug use: Ethical Issues in Obstetric and Gynecologic Practice 422: 1-12.
National Institute on Drug Abuse. 2003. Preventing drug use among children and adolescents: a research-based guide for parents, educators, and community leaders, Second Edition. United States Department of Health and Human Services.View
Cadoni C, Pisanu A, Solinas M, Acquas E, Di Chiara G (2001) Behavioral sensitization after repeated exposure to Delta 9-tetrahydrocannabinol and cross-sensitization with morphine. Psychopharmacology 158: 259–266. 45.View
Groton D (2013) Are housing first programs effective: a research note. J. Soc. & Soc. Welfare 40:51.View
Padgett DK, Stanhope V, Henwood BF, Stefancic A (2011) Substance use outcomes among homeless clients with serious mental illness: comparing housing first with treatment first programs. Community mental health journal, 47: 227-232.View
Padgett DK, Gulcur L, Tsemberis S (2006) Housing first services for people who are homeless with co-occurring serious mental illness and substance abuse. Research on Social Work Practice, 16: 74-83.View
Tsemberis S, Gulcur L, Nakae M (2004) Housing first, consumer choice, and harm reduction for homeless individuals with a dual diagnosis. American journal of public health 94: 651-656.View
United States Interagency Council on Homelessness (2017) Housing first.