
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 2 (2018), Article ID: JPHIP-124
https://doi.org/10.33790/jphip1100124Research Article
Context of Breastfeeding among Latina Mothers using a Social-ecological Approach: An Exploratory Study
Alice Ma1, Elisa A. Merçon-Vargas2, Brittany D. Chambers3, Monde Nyambe1, Tiffany A. Williams1
1Department of Applied Health, Southern Illinois University Edwardsville, Edwardsville, IL, 62025-1126, USA
22Department of Social and Developmental Psychology, Federal University of Espírito Santo, Vitória, Espírito Santo, 29075-073, Brazil.
33Department of Epidemiology and Biostatistics, UCSF Preterm Birth Initiative, University of California San Francisco, San Francisco, CA, 94158, USA
Corresponding Author Details: Alice Ma, Department of Applied Health, Southern Illinois University Edwardsville, Edwardsville, IL, 62025-1126, USA. E-mail: ama@siue.edu
Received date: 13th July, 2018
Accepted date: 16th November, 2018
Published date: 23rd November, 2018
Citation: Ma A, Merçon-Vargas EA, Chambers BD, Nyambe M, Williams TA (2018) Context of breastfeeding among Latina mothers using a social-ecological approach: An exploratory study. J Pub Health Issue Pract 2: 124.
Copyright: ©2018, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Background: Emerging research has begun to examine the breastfeeding experiences among racial/ethnic minority women. However, limited research to date has explored the potential factors that impact Latina mothers’ breastfeeding through a multi-level lens. We examined the context of breastfeeding among Latina mothers in an exploratory study.
Methods: We conducted semi-structured interviews with a convenience sample of 9 Latina mothers. Guided by the socialecological model, thematic content analysis was used.
Results: Latina mothers described individual- (e.g., knowledge of breastfeeding), interpersonal- (e.g., social support and norms), institutional- (e.g., healthcare system), and community-level (e.g., cultural norms) influences on their breastfeeding. Mothers recommended provision of bilingual and bicultural health professionals, information on US breastfeeding norms, and Latinofriendly informational materials in other languages.
Conclusions: Considering the multi-level factors that shape Latina mothers’ breastfeeding is essential to develop and implement culturally tailored initiatives and facilitate access to breastfeeding support to improve maternal and infant health.
Key Words: breastfeeding, Latina mothers, culture, qualitative, social-ecological model
Abbreviations: US = United States
Introduction
In accordance with recommendations from the Global Strategy on Infant and Young Child Feeding [1] and the American Academy of Pediatrics [2], breastfeeding is the optimal feeding standard for infant nutrition [3]. Despite the benefits of breastfeeding (e.g., reduced risk of post-partum hemorrhage) and high initiation rates (76.5%) among new mothers in the United States (US), overall rates for continued breastfeeding remain low (49.0% at 6 months versus 27.0% at 12 months), particularly for certain racial/ethnic groups [4,5]. Although Latina mothers’ breastfeeding initiation rates are typically higher compared to other racial/ethnic groups (80.0% versus 75.2% among White and 58.9% among Black/African American mothers) [6], their exclusive breastfeeding rates tend to be lower and formula supplementation rates higher compared to other racial/ethnic groups, which can reduce breastfeeding duration [7-9]. These rates challenge Healthy People 2020’s national goals for breastfeeding (e.g., increasing the proportion of infants who are breastfed and reducing the proportion who receive formula supplementation), which suggests barriers to breastfeeding that may be uniquely experienced by some racial/ethnic minority women (e.g., English-language abilities) [10,11]. To ensure that minority women, such as Latina mothers, are supported in their breastfeeding during this critical time, it is important to identify opportunities to reduce barriers and increase facilitators to breastfeeding.
Latina mothers’ breastfeeding practices are impacted by a variety of factors, including cultural norms, social support, and access to culturally congruent care [9,11-14]. These factors may differentially impact breastfeeding behaviors on a continuum, with some breastfeeding more due to a more supportive context (e.g., access to breastfeeding support services) and others breastfeeding less due to a more restrictive context (e.g., conflicting cultural breastfeeding norms) [9,11,13]. The interplay of these factors (e.g., culture and social support) that shape Latina mothers’ breastfeeding suggest the importance of examining them through a multi-level lens [15,16]. Although emerging research has begun to examine the breastfeeding experiences among racial/ethnic minority women [16], to our knowledge, no research has yet explored the potential factors that impact Latina mothers’ breastfeeding practices through a multilevel lens. Existing research with Latina mothers has primarily focused on individual- and interpersonal-level examinations of their breastfeeding experiences (e.g., knowledge of breastfeeding and social and cultural perceptions) [9,13,17].
Accordingly, we examined the context of breastfeeding among a small sample of Latina mothers using the social-ecological model in an exploratory study.
Materials and Methods
Participants and data collection
We conducted an exploratory study with nine Latina mothers who resided in a diverse, mid-sized city located in the southeastern US. Inclusion criteria included: (1) self-identified as Latina or Hispanic; (2) age 18 years or older; (3) have at least one child of any age; (4) have initiated breastfeeding at any time (i.e., feeding breast milk via the breast directly and/or expressing milk); (5) be able to speak English; and (6) willingness to share their breastfeeding experiences. After each interview, we asked the participant to suggest additional contacts who met the inclusion criteria. Data collection occurred between March and April 2014. Participants were selected via snowball and criterion sampling. We also recruited participants through flyers, personal contacts, social media posts to local groups, e-mails, and phone calls. Recruitment ceased when similar themes emerged in the interviews and a variety of nationalities were represented. The research team determined this point to be data and sampling saturation. The Institutional Review Boards at the University of North Carolina at Greensboro and Southern Illinois University Edwardsville provided human subject review and study oversight (#14-0097 and #18-0122-1C).
We maintained a detailed audit trail to document our study procedures. After participants gave informed consent, we conducted interviews using a semi-structured guide in a setting and time convenient for them. We used open-ended questions to elicit participants’ breastfeeding experiences and probes to prompt elaboration. All interviews were audio-recorded and transcribed verbatim by the researcher present for the interview. The average interview length was approximately 25 minutes. Table 1 presents sample interview questions. No compensation was provided to participants.
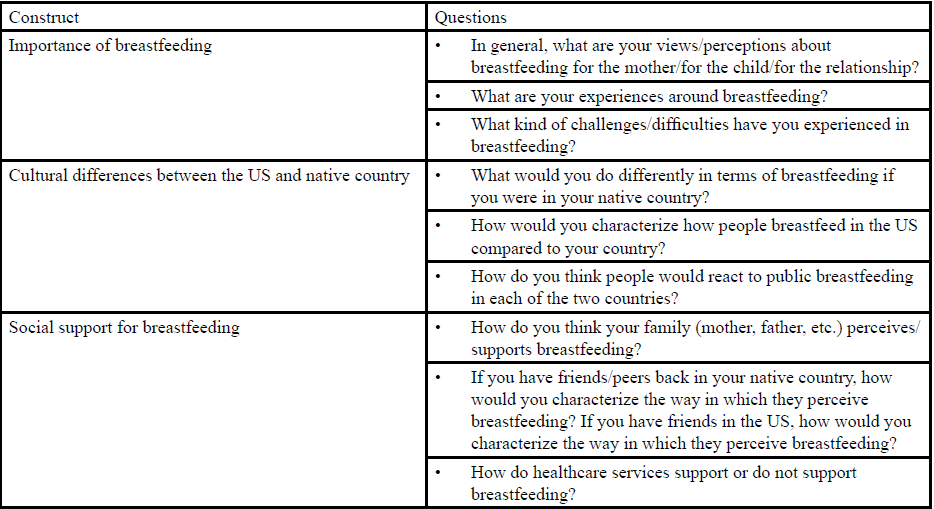
Table:1 Sample interview questions.
Analysis
Guided by the social-ecological model [18] and interview questions, we used content analysis to interpret the breastfeeding experiences described by Latina mothers [19]. We developed a priori codes (e.g., social support) based on the literature. We added and compared emergent codes (e.g., healthcare) based on the interview transcripts. The finalized coding structure was then applied to the interview transcripts; a coding glossary and hierarchical coding chart facilitated this process. Coding discrepancies were resolved by discussion. Exemplar quotations were used from each participant to identify patterns, then common themes were generated based on these codes and patterns. We analyzed and discussed interviews as they occurred, individually and in groups, and compared them to confirm or disconfirm emerging themes. The quotations presented reflect main themes from the participants. Participant information was deidentified with pseudonyms; the first letter of each pseudonym coincides with the first letter of her self-identified native country (e.g., Barbara’s native country is Brazil). Data were entered and managed using Microsoft Word.
Results
Nine Latina mothers participated in the study; their demographic characteristics are presented in Table 2. They identified with a variety of nationalities, including Brazil (n=3), the Dominican Republic (n=1), Mexico (n=3), and Puerto Rico (n=2). The average age was 36 years (range: 22–49 years). Slightly more mothers reported a long breastfeeding duration (n=4) than those who reported a short duration (n=3).
Table:2 Demographic characteristics of Latina mothers (N = 9).
The Latina mothers identified a variety of factors as salient in their breastfeeding experiences across the social-ecological model [18]. Overall, the mothers described navigating breastfeeding in the US as “very complicated” (Barbara, Brazil), with one mother noting the continual challenges of breastfeeding in the US: “Well, I would assume here [in the US], it [breastfeeding] would be getting easier, but apparently it’s not” (Maria, Mexico).
Individual
Knowledge of breastfeeding. The Latina mothers shared basic knowledge of breastfeeding. Many highlighted the importance of breastfeeding and the benefits associated with it: “The kids will be healthier and more immune to diseases from the outside when breastfeeding” (Patricia, Puerto Rico). Several mothers stressed that breast milk provided the best nutrients (e.g., vitamins) and contributed to the immunization and protection of the child (e.g., antibodies) in the short- and long-term. Further, mothers reported that breastfeeding contributed to their physical and psychological well-being, including nurturing the bond with their child. They also noted that breastfeeding helped them lose the weight gained during pregnancy. The mothers’ knowledge of breastfeeding and its benefits are summarized by Bruna (Brazil): “So for the mother...It [breastfeeding] is good to create a bond with the child, it is good to slim, it is good to the self-esteem, it is good because it is delightful...”
Interpersonal
Social support and norms. Many Latina mothers reported having a strong support system from family members and friends. To some extent, this support influenced their decision to breastfeed. Several mothers noted that almost everyone they knew, either growing up or as adults, breastfed their children: “Culturally I was raised seeing everybody in my family or in the community breastfeeding” (Dolores, Dominican Republic). Friends and family often validated the importance of breastfeeding – many of whom shared the mothers’ cultural background and were proponents of breastfeeding. Paloma (Puerto Rico) described, “My mother-in-law and my mom were always like, ‘You’re gonna breastfeed, right? That’s important, you have to, you have to!’”
However, when some mothers experienced unsuccessful or complicated breastfeeding, they reported psychological distress, such as disappointment, sadness, and even grief. When Maria (Mexico) was not able to breastfeed due to latching difficulties, she recalled feeling “really, really, really sad and really mourned not being able to nurse him.” This internal pressure and expectation to breastfeed, and at times subsequent distress, illuminate the psychological challenges and the need for social support, particularly emotional support, when mothers breastfeed.
Institutional
Healthcare. Although breastfeeding was widely accepted across the Latina mothers, they noted a dearth of Latinofriendly resources in the healthcare system to access breastfeeding information. Despite some mothers enjoying the “many courses” (Bianca, Brazil) and other hospital support services, such as postpartum in-home support, others reported language difficulties, including issues finding bilingual health professionals. Patricia (Puerto Rico) noted, “I don’t know if they have enough material in Spanish and that would help because...they come here [US], it’s a culture mix, and they got lost in the culture and sometimes they don’t know.”
Notably, Paloma (Puerto Rico) described “a lot of prejudice” witnessed at a clinic appointment with her Latina friend. She believed her friend experienced poor quality service due to her friend’s limited English-speaking abilities: “They were nicer to me than her [my friend]. And I didn’t like that...I think the girl was a little bit rude with her. Maybe she got frustrated because she [my friend] didn’t understood her or something.”
Community
Cultural norms. The Latina mothers noted the cultural differences in breastfeeding between their native countries and the US. They emphasized breastfeeding in their culture as natural, therefore public breastfeeding was not an issue, as explained by Barbara (Brazil): “I think in Brazil, breastfeeding...it is much more necessary. We see that as, it is basic...You can breastfeed your child in public, here you cannot.” Oftentimes, the mothers perceived breastfeeding in the US as “not acceptable” (Dolores, Dominican Republic), with typically longer breastfeeding durations in their native country than in the US.
Additionally, some mothers noted the lack of information on US breastfeeding norms as a critical barrier. For instance, Bianca (Brazil) expressed it was through her friends that she was alerted to the taboos of public breastfeeding in the US: “But if my Brazilian friends had not told me, I wouldn’t know...And maybe I would get to an embarrassing situation.” In this case, friends were a more important source of information on US cultural breastfeeding practices than healthcare professionals.
Recommendations
The Latina mothers emphasized the need for more breastfeeding support services and awareness, particularly for bilingual and bicultural healthcare professionals and resources: “Maybe doing more like classes, workshops about these things [breastfeeding]...because the Hispanic—most of the time, they really don’t know. It’s not that they don’t want to, it’s that they don’t really know, they don’t have the information...So it will be more Spanish material and more maybe workshops...” (Patricia, Puerto Rico).
Although healthcare clinics provided some Latino-friendly informational materials (e.g., pamphlets), Maria (Mexico) noted the dearth of Spanish-speaking local healthcare professionals – “There’s just not very many bilingual health professionals here” – which can challenge connection to a healthcare provider and limit breastfeeding education for Latina mothers. Dolores (Dominican Republic) also recommended the inclusion of health educational materials in Spanish and other languages. One recommendation to help disseminate breastfeeding information to Latina families (not only mothers) was to implement a community breastfeeding event: “I think it would be awesome if...[there is] a breastfeeding day and kind-of do like an education or awareness...that help people in the community to become interested and have more information out, so it doesn’t become so much it’s just—like a women thing” (Dolores, Dominican Republic).
Discussion
The findings from this exploratory study highlight the breastfeeding practices of a small sample of Latina mothers residing in the southeastern US. Guided by the social-ecological model [18], the mothers identified multi-level factors salient in their breastfeeding experiences, including knowledge of breastfeeding, social support and norms, the healthcare system, and cultural norms. Despite the limited sample, our findings identified common themes related to the importance of breastfeeding that emphasized personal and social aspects, including the benefits for the infant and mother. Their breastfeeding knowledge aligns with established literature on the benefits of breastfeeding, including bonding opportunities and reduced infant health risks [20]. However, given the lower rates of exclusive breastfeeding and higher rates of formula supplementation compared to other racial/ethnic groups [7-9], knowledge of breastfeeding alone may be insufficient to encourage breastfeeding among Latina mothers [13]. Our findings support emerging research that considers multi-level factors that impact breastfeeding; this approach can aid in comprehensively understanding Latina mothers’ breastfeeding behaviors and identifying opportunities for solutions to support them [15,21].
The Latina mothers often situated their breastfeeding practices in terms of their culture [9,11,22,23]. The mothers’ support system shared similar perspectives with them on the importance of breastfeeding, yet their cultural beliefs – and thereby pressures – to breastfeed were at times challenging. Although a supportive environment is critical to mothers’ relationship with breastfeeding [23-25], they may also need to be supported when breastfeeding difficulties arise. These mothers tended to experience psychological distress, suggesting a need for comprehensive support systems that are culturally congruent, particularly for those who may experience multiple, co-occurring difficulties [26,27].
Notably, our findings illuminate a potential dearth in healthcare support for Latina mothers. Some mothers described challenges in navigating the US healthcare system, such as language barriers and discrimination, which may suggest critical issues in accessing some breastfeeding support services [28]. Some mothers noted the lack of information on US cultural norms, which suggests the need for more Latino-friendly informational support on cultural norms. Developing culturally tailored efforts and enhancing diversity training among healthcare professionals may be critical to support care for Latina mothers [17]. Given that racial/ethnic disparities remain in breastfeeding rates and practices [11], it is essential to understand and enhance culturally congruent care to ensure high quality services for vulnerable mothers [29].
Although this study included participants from a variety of nationalities, our small sample is unlikely to represent all Latina mothers’ breastfeeding experiences. Further investigation with larger samples of mothers living in other parts of the US is warranted to gain insights through each unique lens. Future work should continue examining breastfeeding through a multi-level lens and consider social determinants of breastfeeding (e.g., poverty) to enhance health equity for Latino families [30].
Conclusion
To meet the goals of the Global Strategy on Infant and Young Child Feeding [1], the American Academy of Pediatrics [2], and Healthy People 2020 [10], breastfeeding promotion efforts should work to understand the context of breastfeeding for Latina mothers, as well as other racial/ethnic minority women. Considering the multilevel factors that shape Latina mothers’ breastfeeding is essential to develop and implement culturally tailored initiatives and facilitate access to breastfeeding support to improve maternal and infant health.
Acknowledgments
The authors thank the participants for their time and dedication. The authors also thank Terra McKee, MS, for her project support; Kimberly Kappler Hewitt, PhD, of the Department of Educational Leadership and Cultural Foundations and Paige Hall Smith, PhD, of the Department of Public Health Education at the University of North Carolina at Greensboro; and Wendasha Jenkins Hall, PhD, MS, of the Georgia Health Policy Center for their formative feedback and editorial assistance.
Conflict of Interest Statement
The authors report no potential conflict of interests.
Participant Consent Statement
Informed consent was obtained from all participants included in the study as approved by the university ethics review committee where the data were collected.
References
World Health Organization. Global Strategy for Infant and Young Child Feeding (2018).View
Gartner LM, Morton J, Lawrence RA, Naylor AJ, O’Hare D et al. (2005) Breastfeeding and the use of human milk. Pediatrics 115: 496-506.View
Eidelman AI, Schanler RJ, Johnston M, Landers S, Noble L et al. (2012) Breastfeeding and the use of human milk. Pediatrics 129.View
Centers for Disease Control and Prevention. Breastfeeding Report Card: United States (2013).View
United Nations International Children’s Emergency Fund. (2018) Improving Breastfeeding, Complementary Foods and Feeding Practices.View
United Nations International Children’s Emergency Fund. (2018) Improving Breastfeeding, Complementary Foods and Feeding Practices.View
Cartagena D, Ameringer SW, McGrath JM, Masho SW, Jallo N et al. (2015) Factors contributing to infant overfeeding in lowincome immigrant Latina mothers. Appl Nurs Res 28: 316-321.
Centers for Disease Control and Prevention. Breastfeeding Rates (2018).
Wambach K, Domian EW, Page-Goertz S, Wurtz H, Hoffman K et al. (2016) Exclusive breastfeeding experiences among Mexican American women. J Hum Lact 32: 103-111.View
Healthy People 2020. Maternal, Infant, and Child Health (2018).
Jones KM, Power ML, Queenan JT, Schulkin J (2015) Racial and ethnic disparities in breastfeeding. Breastfeed Med 10: 186- 196.View
Bai Y, Wunderlich SM, Fly AD (2011) Predicting intentions to continue exclusive breastfeeding for 6 months: A comparison among racial/ethnic groups. Matern Child Health J 15: 1257- 1264.View
Hohl S, Thompson B, Escareño M, Duggan C (2016) Cultural norms in conflict: Breastfeeding among Hispanic immigrants in rural Washington State. Matern Child Health J 20: 1549-1557.View
Insaf TZ, Fortner RT, Pekow P, Dole N, Markenson G et al. (2011) Prenatal stress, anxiety, and depressive symptoms as predictors of intention to breastfeed among Hispanic women. J Womens Health 20: 1183-1192.View
Dunn RL, Kalich KA, Fedrizzi R, Phillips S (2015) Barriers and contributors to breastfeeding in WIC mothers: A social ecological perspective. Breastfeed Med 10: 493-501.View
Reeves EA, Woods-Giscombé CL (2015) Infant-feeding practices among African American women: Social-ecological analysis and implications for practice. J Transcult Nurs 26: 219- 226.
Sloand E, Budhathoki C, Junn J, Vo D, Lowe V et al. (2016) Breastfeeding among Latino families in an urban pediatric office setting. Nurs Res Pract 2016: 1-6.View
McLeroy KR, Bibeau D, Steckler A, Glanz K (1988) An ecological perspective on health promotion programs. Health Educ Q 15: 351-377.View
Hsieh H-F, Shannon SE (2005) Three approaches to qualitative content analysis. Qual Health Res 15: 1277-1288.View
United Nations International Children’s Emergency Fund. Breastfeeding.View
Dunn RL, Kalich KA, Henning MJ, Fedrizzi R (2015) Engaging field-based professionals in a qualitative assessment of barriers and positive contributors to breastfeeding using the social ecological model. Matern Child Health J 19: 6-16.View
Barcelona de Mendoza V, Harville E, Theall K, Buekens P, Chasan-Taber L et al. (2016) Acculturation and intention to breastfeed among a population of predominantly Puerto Rican women. Birth 43: 78-85.View
Street DJ, Lewallen LP (2013) The influence of culture on breast-feeding decisions by African American and White women. J Perinat Neonatal Nurs 27: 43-51.View
Brown A, Raynor P, Lee M (2011) Young mothers who choose to breast feed: The importance of being part of a supportive breast-feeding community. Midwifery 27: 53-59.View
Demirtas B (2012) Strategies to support breastfeeding: A review. Int Nurs Rev 59: 474-481.View
Fakhrai M, Luckey DL, Hayes-Bautista TM (2016) Breastfeed today, even if you can’t tomorrow. Obstet Gynecol 127: 69S.
Feldman-Winter L (2013) Evidence-based interventions to support breastfeeding. Pediatr Clin 60: 169-187.View
González HM, Vega WA, Tarraf W (2010) Health care quality perceptions among foreign-born Latinos and the importance of speaking the same language. J Am Board Fam Med 23: 745- 752.View
Betancourt JR, Green AR, Carrillo JE, Ananeh-Firempong O (2003) Defining cultural competence: A practical framework for addressing racial/ethnic disparities in health and health care. Public Health Rep 118: 293-302.View
Waldherr R (2015) Integrating social determinants of breastfeeding into guidelines: An approach to enhance health equity in infants. Int J Integr Care 15: 19-21.View