
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 2 (2018), Article ID: JPHIP-127
https://doi.org/10.33790/jphip1100127Research Article
Teen Pregnancy Prevention and African American Faith-Based Organizations: Lessons Learned from the Southern Nevada Teen Pregnancy Prevention Project
Melva Thompson-Robinson1*, Pamelia Atkins-Girouard2, Johanna Andrews3, Marya L. Shegog4, Crystal Lee5
1Professor, UNLV School of Community Health Sciences & Director, Center for Health Disparities Research, United States.
2UNLV Medicine Maternal Child Wellness, University Nevada Las Vegas, United States.
3Center for Health Disparities Research, School of Community Health Sciences, University of Nevada, Las Vegas, United States.
4The Lincy Institute and School of Community Health Sciences, Social and Behavioral Program, University of Nevada, Las Vegas, United States.
55Department of Public Health, Usha Kundu, MD College of Health, University of West Florida, United states.
States.Corresponding Author Details: Melva Thompson-Robinson, Professor, UNLV School of Community Health Sciences & Director, Center for Health Disparities Research, United States. E-mail: melva.thompson-robinson@unlv.edu
Received date: 07th April, 2018
Accepted date: 16th November, 2018
Published date: 10th December, 2018
Citation: Robinson MT, Atkins-Girouard P, Andrews J, Shegog ML, Lee C (2018) Teen Pregnancy Prevention and African American Faith-Based Organizations: Lessons Learned from the Southern Nevada Teen Pregnancy Prevention Project. J Pub Health Issue Pract 2: 127.
Copyright: ©2018, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
African American faith-based organizations have long been recognized as vital resources in the African American community. Within the Social Determinants of Health Framework, various barriers and facilitators to implementing HIV and STI prevention activities within these faith-based organizations have been identified. The Southern Nevada Teen Pregnancy Prevention project implemented an evidence-based teen pregnancy prevention intervention targeting African American youth ages 14-19 years in African American faithbased organizations in Clark County, NV. This manuscript presents the lessons learned from this project. In addition to confirming some of the barriers and facilitators previously identified in the literature, this manuscript also identifies additional barriers and facilitators based on the experiences of this project, which can further enhance future work with these organizations.
Introduction
African American faith-based organizations (FBOs) are cornerstones of and respected institutionswithin the community in which they are located. Often, these FBOs are not only a place of worship, but serve as a collective voice for change, advocate for social justice and human rights,serve as a meeting place for social action organizations, and provide education and information, including health education to its members [1-3]. As such, these FBOs represent a potentially underutilized partner for public health programming,addressing health disparities, and providing a targeted audience with.
Despite human immunodeficiency virus (HIV), sexually transmitted infections (STIs), and teen pregnancy rates disproportionately affecting African American communities, their FBOs have been hesitant to engage in providing comprehensive sexuality education and/or HIV prevention services and activities within their organizations for their members and the larger community [4,5]. According to the literature, among the identified barriers to engaging African American FBOs in the provision of comprehensive sexuality education and/or HIV prevention services are:
* The doctrine of the FBOs may vary across denomination, such that certain denominations may be more accepting of issues related to sexuality and religion than others [3,5].
* Addressing reproductive health issues can conflict with the religious doctrine [3,4,7].
* Evidence-based strategies and interventions are not congruent with the beliefs and culture of the FBO [2].
* Unwillingness of or lack of interested by FBO leadership to provide comprehensive sexuality education and/or HIV prevention services [1,6].
* Promoting condoms can be viewed as condoning sex [2].
* FBOs face financial and resource constraints that inhibit ability to provide comprehensive sexuality education and/or HIV prevention services [7,8].
* Stigma and homophobia may exist among FBO leadership and/ or congregation [3,7].
* FBOs may want to emphasize abstinence instead of comprehensive sexuality education [1].
* Congregation and/or leadership may not think that the youth affiliated with their FBO are at risk for HIV/AIDS, STIs, and/ or teen pregnancy [1].
* Lack of knowledge by FBO leadership about the severity of the local issues related to HIV/AIDS, STIs, and/or teen pregnancy [7].
* Discussing human sexuality in faith settings is considered to be inappropriate [7].
* Age, lack of experience, and experience of pastor may make an FBO less likely to participate [7].
In spite of the barriers that may prevent the participation of FBOs in comprehensive sexuality education and/or HIV prevention services, the National HIV/AIDS Strategy (NHAS) indicates that faith-based organizations need to be involved [9]. NHAS outlines recommended actions for FBOs to address HIV/AIDS in their communities.
The literature also identifies facilitators of African American FBOs participation in comprehensive sexuality education and/or HIV prevention services are needed. The following facilitators and considerations have been identified that can support the successful establishment of an effective sexual health and risk reduction program within FBOs.
* Having congregational and leadership support for comprehensive sexuality education and/or HIV prevention services [3,10-13].
* Having access to culturally sensitive HIV prevention materials and culturally appropriate programs [1,3].
* Providing training and support for FBOs’ efforts for comprehensive sexuality education and/or HIV prevention services [3].
* FBO leadership recognizing HIV as an issue in the community [3].
* FBO leadership knowing someone who has HIV [3].
* Having other health/welfare/support ministries within the FBO [11].
* Having HIV-related activities already in FBOs [11,13].
* Involving the FBO and target population in the design, implementation, and program evaluation [1,10].
* Having a liaison from the FBO for HIV activities [1].
* Incorporating spirituality and compassion into prevention efforts instead of authoritarian and judgmental opinions and attitudes [1].
* Creating a sense of ownership of the program by the FBO to ensure wider program distribution and participation [1].
* Carefully selecting FBOs and HIV service organizations for partnership [10,12].
* Turning conflict with religious doctrine into an advantage for building relationships and partnerships [12].
* Choosing appropriate delivery of services [12].
* Using existing infrastructure, resources, and influence of the church and its leadership [10].
* Including simple learner evaluation tools to determine whether the program is effective and how it might be improved [10].
* Having financial and human resources for HIV activities [13].
Even with the abundance of literature regarding implementing HIV prevention activities in African American FBOs, the literature regarding the implementation of teen pregnancy prevention interventions in African American FBOs is scarce. The purpose of this manuscript is to describe the lessons that can be learned from the implementation of an evidence-based teen pregnancy prevention intervention in African American FBOs.
Methods
The Center for Health Disparities Research (CHDR) at the University of Nevada Las Vegas (UNLV) along with its partners received funding for the Southern Nevada Teen Pregnancy Prevention Project (SN-TPPP) from the Office of Adolescent Health (OAH) at the US Department of Health and Human Services to implement an evidence-based teen pregnancy prevention intervention. The purpose of SN-TPPP was to implement the evidence-based teen pregnancy prevention intervention, Becoming a Responsible Teen (BART), with African American youth between the ages of 14 and 19 years in African American FBOs in Clark County, Nevada. In order to participate in the project and receive the intervention, parents/legal guardians completed a registration packet that included an informed consent form.
BART was developed for use with African American youth, optimized contact time into 8 intervention sessions, and was designed to be implemented in community settings [14]. BART has been shown to be effective in HIV prevention intervention, as well as reducing rates of and behaviors associated with teen pregnancy, as well [14]. Table 1 outlines the BART curriculum.
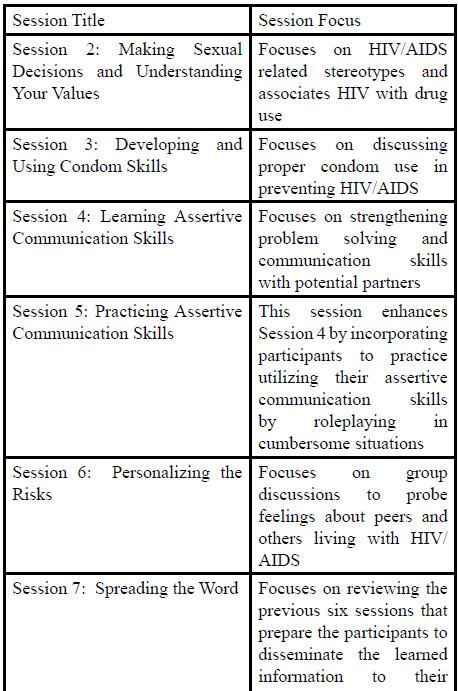
Table:1 Overview of BART Curriculum.
The Social Determinants of Health Framework as related to teen pregnancy prevention were also a key consideration when implementing and program. Clark County, Nevada is an optimal area to address a teen pregnancy [15]. Implementing BART with African American teens serves to increase knowledge, skills and access to health resources in order to further close the gap and support health equity by reducing teen pregnancy.
To implement BART, project staff recruited African American FBOs to participate in the project. FBOs served as the host site for the implementation of the project and recruited youth to participate. Project staff worked with the FBOs to schedule the onsite sessions. FBOs were asked to provide a liaison to the project. This person was responsible for reminding youth to attend the sessions and communicating information between FBO leadership and project staff. The project provided the intervention materials, a substantial snack for session participants, trained facilitators as well as monitored the implementation. FBOs that participated were compensated $500 by the project to offset expenses that may have occurred as a result of their participation.
Results
Over a 5 year period, the SN-TPPP implemented the BART intervention in 35 unduplicated African American FBOs in Clark County, NV. Five hundred (500) African American teens between the ages of 14 and 19 completed 75% or more of the intervention sessions. Over 70 persons from the community were trained as facilitators to implement the evidence-based intervention with fidelity. The results presented below reflect the experience and lessons learned from the implementation of project activities.
Lessons Learned
Numerous lessons were learned from this project. The lessons were identified as either barriers or facilitators to the implementation of the project. The facilitators are presented first followed by the barriers.
Facilitators
The following are lessons that were learned by the project, which resulted in the successful implementation of the project and intervention.
InvestedFBO Leadership
Pastors embraced the need for teen pregnancy prevention as well as HIV/STI prevention for youth. Regardless of participation in the project, pastors generally felt that that education focused on teen pregnancy prevention was needed in the community. Among those pastors whose FBOs participated in the project, those pastors reported knowing someone who was infected with HIV, having been a teen parent, teen pregnancy occurring within their FBOs, and/or recognizing that teens that attended their FBO were at high risk for HIV, STIs, and/or teen pregnancy. In some cases, pastors reported that even though they felt that a potential conflict between the project and church doctrine may exist, they felt that the need to educate their youth in a modern world, which meant that they had to confront issues associated with risky sex behavior(s).
Present the Abstinence Message
A method for addressing the potential conflict with religious doctrine was the development and implementation of a session on abstinence that was added to the beginning of the intervention as the first session. The session focused on abstinence based on information from existing sexual education resourceswas developed by SN-TPPP staff specifically for this project. This session received the approval of the Office of Adolescent Health to ensure that this adaptation did not compromise the original intent of the intervention. Pastors appreciated the recognition that their beliefs reflect abstinence and that the abstinence message was carried throughout the intervention as the only 100% method for remaining HIV-free and not pregnant.
Use Ready-Made Groups
The project had its most success when implementing the intervention with FBOs that had youth groups that met on a consistent basis. When the project was able to implement intervention sessions on the same night and at the same time that the youth group at the FBO usually met, then youth were more likely to attend the sessions. Asking youth to come on a night when they normally do not attend activities at the FBO created transportation issues for the youth. In addition, sessions followed the schedule that these groups generally had, so intervention sessions were postponed a week if the FBO had an event that conflicted with an intervention session. The school calendar was also taken into consideration. The project staff learned that if youth were not in school on a particular day, then they were generally less likely to come to intervention sessions at the FBO.
Make Participation for Youth Easy
FBOs were asked to identify a liaison from within who knew the youth, could help recruit participants, and work with project staff. The liaison was also responsible for sending out reminders about the intervention session schedule. This person could follow up with youth who did not attend a session(s) to work with them and their families to promote attendance.
Since intervention sessions lasted 1.5 to 2 hours and were held on weeknights, providing participants with a substantial snack allowed for sessions to infringe upon the evening meal time. Initially, FBOs that participated early on in the project were compensated more money to provide this snack. Over time, due to the limited space and resources that some FBOs had, the project assumed the role of providing the snackfrom local restaurants. The financial compensation that was then provided to the FBOs was reduced to reflect their reduced responsibility.
Condom Demonstrations Can Be Done in FBOs
The condom demonstration session was treated like any other session as a part of the BART intervention. Project staff and intervention facilitators did not call attention to this session of the intervention either during discussion with FBO leadership about participation and in explaining the intervention to participants. To respect the FBO and its members, wrappers, condoms, and other trash used in the demonstration were gathered and disposed of by project staff and intervention facilitators outside of the FBO. Condoms were not readily made available for teens through the project, but were provided to those who specifically asked for them. Project staff and intervention facilitators also provided participants with referrals to local resources, including condom distribution sites and sexual health clinics, upon request.
Use Community Persons to Implement the Intervention
For this project, the intervention facilitators were community persons who were trained by the project to implement the intervention. Each facilitator completed 20 hours of training, which included 16 hours of intervention training plus an additional 4 hours of training on the project and mandatory reporting. During the training, participants were observed by project staff to determine which persons were most ready to be facilitators and which persons needed some additional support from the project before being assigned an FBO site. As new facilitators were trained over the course of the project, they were paired with facilitators who had experience with implementation of the intervention so that the newer facilitator could have additional hands on training. Additionally, to facilitate a safe and confidential environment for participants, facilitators that had any type of relationship with a specific FBO were not allowed to implement the intervention at that FBO.
In accordance with funding requirements, intervention facilitators were formally observed by project staff. This observation was guided by a checklist, based on the intervention. Where appropriate, feedback for improvement was provided. Facilitators also documented fidelity in the implementation of the intervention after each session.
Availability of Project Staff
In addition to the FBO providing a liaison, a project staff member was also onsite during the implementation of the intervention session. The role of this person was to serve as a liaison between the project, intervention facilitators, and FBO; troubleshoot problems that may arise onsite; answer questions that parents and others may have about the project; ensure that project-related materials and supplies were available; receive the delivery of the substantial snack; and ensure that intervention sessions were implemented as planned. In order to maintain the safe and confidential environment for participants, the onsite staff person did not teach intervention sessions, except in emergency situations when a facilitator was not able to attend the session.
Barriers
The following identified barriers challenged the successful implementation of the project and intervention. Where appropriate, strategies for addressing the barrier that arose are provided below. In some cases, strategies to address the barriers could not be identified and implemented; so consequently, are not presented here.
Conflict with Religious Doctrine
Project staff made sure to not discuss religious doctrine with pastors and FBO leadership, in part because project staff is not as familiar with the doctrine. Due to federal funding, project staff had to adhere to a policy in which federal funds could not be used to support religious doctrine. As such, project staff had to ensure that activities, such as having prayer at the beginning or end of a session, were done separate from the project-related activities. Pastors were encouraged to have an additional session with the participants after the project completed its implementation to discuss with the teens how what they learned through the project fit within the FBO’s doctrine.
This policy of not using federal funds to support religious doctrine also impacted those FBOs who were opposed to having the condom demonstration session taking place in their facility. Per discussions with OAH staff, project staff had to present the option of moving all of the intervention sessions out of their facility in order to not highlight the condom demonstration session. If moving all of the sessions from the facility was not feasible, then often it was determined that the FBO could not participate in the project.
Decision Making Varies by FBO
The decision to participate in the project were, in general, made by the pastor of the FBO. In some cases, decisions were made at different levels within an FBO. The level at which the decision to participate in the project was made was unique to the FBO and not consistent within or across denominations. Persons who attended the FBO and wanted their teens to participate in the intervention did not automatically translate to the leadership of the FBO agreeing to participate in the project.
FBO Having Limited Resources
FBO resources varied significantly. Some FBOs had multiple rooms available in their facility; whereas, others had just their sanctuary for meeting space. Project staff had to be creative in adapting to the available space in order to meet the requirements of the intervention. Not all FBOs have full-time office staff that could assist the project with copying project-related materials and securing of resources to provide needed supplies. Consequently, the project provided all of the materials and supplies needed for implementation of the intervention sessions.
Federal Funding Guidance
Funding for this project was provided by the OAH in the Office of the Assistant Secretary at the US Department of Health and Human Services. As discussed earlier, based on guidance provided by the Office of Adolescent Health, the project had to ensure that federal funds were not used to support religious doctrine. For example, intervention sessions were not allowed to be implemented at the same time that FBO religious services were being conducted. Intervention sessions had to be distinct from religious services. In addition, the condom demonstration session that was part of the intervention had to be conducted in the same manner as the other sessions. FBOs that made requests that conflicted with policy and/or guidance from the OAH were not able to participate in the project.
Discussion
The Southern Nevada Teen Pregnancy Prevention Project was able to implement an evidence-based teen pregnancy prevention project in African American faith-based organizations in Clark County, NV. Through the implementation of the project, numerous lessons were learned that reflect the barriers and facilitators to the implementation of HIV prevention activities in African American FBOs previously documented in the literature.For example, as identified in the literature, having congregational and leadership support for comprehensive sexuality education and/or HIV prevention activities was a facilitator in implementing these activities in African American FBOs [3,10-13]. With this project, having invested FBO leadership was a facilitator in the implementation of the teen pregnancy prevention intervention. Often, the invested FBO leadership recognized that teen pregnancy and HIV were issues in the community as well as knew someone who had HIV and/or was a teen parent, which were also identified facilitators in the literature [3].
The project found that having a liaison from the FBO, as stated in the literature, was a key to implementing the teen pregnancy prevention intervention [1]. Since SN-TPPP was an outside entity implementing the intervention at FBOs, having a staff person from the FBO and the project onsite assisted in troubleshooting problems, as they arose, allowed for problems to be addressed immediately. The coordination of the two liaisons allowed for smooth implementation of the intervention at FBOs.
Aaron et al. [10] cited that using existing infrastructure, resources, and influence of the church and its leadership to be a facilitator in the implementation of HIV-related activities in African American FBOs. Specifically, in working with youth and teen pregnancy prevention, the use of ready-made groups and making participation for youth easy were facilitators. The project found that trying to bring youth together who did not have a relationship with the FBO or at times when the youth normally are not onsite reduced attendance, which made implementation of the intervention sessions difficult despite having a liaison from the FBO who recruited and reminded the youth of the intervention sessions.
The Southern Nevada Teen Pregnancy Prevention Project did identify additional facilitators not previously identified in the literature. Condom demonstrations can be done in FBOs is a facilitator for successfully implementing comprehensive sex education. Using community persons to implement the intervention sessions was another identified facilitator in this project. The use of community persons to implement the intervention created community capacity and promote project sustainability. Future efforts should replicate and build on the efforts of this project with these facilitators.
Some of the barriers that are cited in the literature were also found in this project. Conflict with religious doctrine was found with this project as well as in the literature [3,4,7]. The addition of a session focused on abstinence eased some of the conflict experienced with religious doctrine. Based on the experience of the project, other strategies to address and/or ease this conflict are elusive and may be non-existent, particularly when there is limited flexibility in adapting the intervention to reduce this conflict.
Limited resources remain a barrier as found by both the literature [7,8] and this project. The literature cited that FBOs may not have resources for HIV-related activities. This project eliminated that lack of resources by providing the intervention materials, supplies, and staffing, but experienced lack of resources at times in terms of space at an FBO. Creative solutions were found by project staff to address space issues. However, the use of federal funds to address the lack of resources at FBOs did create barriers as well. The intervention sessions had to be implemented in and project had to operate within federal funding guidance, which at times conflicted with the requests of the FBOS.
A barrier identified in the literature was that FBOs may want to emphasize abstinence instead of comprehensive sexuality education [1]. This project promoted abstinence along with comprehensive sexual education, which was acceptable to those African American FBOs that participated in the project. Often, leaders of these FBOs acknowledged an understanding that while abstinence is the only way to definitively prevent teen pregnancy and HIV transmission, they also understood that youth in the community and with relationships with their FBO are also engaging in sexual behaviors.
To counteract lack of knowledge of the extent of the problem of HIV and teen pregnancy within the community [7], project staff presented current statistics to FBO leadership as a part of the introduction to the project. This introduction reduced the impact of this barrier on this project’s activities. Other barriers identified in the literature, doctrine varying across denominations [3,6], unwillingness or lack of support to provide HIV prevention [1,8], stigma and homophobia [3,7], as well as personal characteristics of the pastor [7], were not encountered as a part of this project.
Conclusion
The Southern Nevada Teen Pregnancy Prevention Project implemented an evidence-based teen pregnancy prevention intervention, which included condom demonstration, in African American FBOs. In the implementation of the project, many lessons were learned, including that African American FBOs will allow condom demonstrations to be conducted within their facilities. Future work is needed to confirm that the barriers and facilitators identified in this manuscript are not unique to this project. The implementation of the BART intervention proved to be a strong platform to reduce teen pregnancy and help achieve health equity.
Acknowledgements
The authors would like to acknowledge all of the project staff, community-based instructors, and the faith-based organizations that participated in the Southern Nevada Teen Pregnancy Prevention Project.
Funding Acknowledgement
The Southern Nevada Teen Pregnancy Prevention Project was funded bythe Office of Adolescent Health at the US Department of Health and Human Services(TP1AH000045).
References
Francis SA, Liverpool J. (2009). A review of faith-based HIV prevention programs. J Relig Health, 48: 6-15.View
Roman Isler M, Eng E, Maman S, Adimora A, Weiner B. (2014). Public health and church-based constructions of HIV prevention: black Baptist perspective. Health Educ Res, 29: 470-484.View
Woods-Jaeger BA, Carlson M, Taggart T, Riggins L, Lightfoot AF, et al. (2015). Engaging African American Faith-Based Organizations in Adolescent HIV Prevention. J Relig Health, 54: 1358-1374.View
Cornelius JB, White AC (2013). Sexual communication needs of African American families in relation to faith-based HIV prevention. J Cult Divers, 20: 146-152.View
Coyne-Beasley T, Schoenbach VJ (2000). The African-American church: a potential forum for adolescent comprehensive sexuality education. J Adolesc Health, 26: 289-294.View
Pichon LC, Griffith DM, Campbell B, Allen JO, Williams TT. et al. (2012). Faith leaders' comfort implementing an HIV prevention curriculum in a faith setting. J Health Care Poor Underserved, 23: 1253-1265.
Moore D, Onsomu EO, Timmons SM, Abuya BA, Moore C. et al. (2012). Communicating HIV/AIDS through African American churches in North Carolina: implications and recommendations for HIV/AIDS faith-based programs. J Relig Health, 51: 865-878.View
Smith J, Simmons E, Mayer KH. (2005). HIV/AIDS and the Black Church: what are the barriers to prevention services? J Natl Med Assoc, 97: 1682-1685.View
House TW (2015). NATIONAL HIV/AIDS STRATEGY for the UNITED STATES: UPDATED TO 2020. Washington, DC.View
Aaron E, Yates L, Criniti S. (2011). A collaborative HIV prevention and education initiative in a faith-based setting. J Assoc Nurses AIDS Care, 22: 150-157.
Abara W, Coleman JD, Fairchild A, Gaddist B, White, J et al., (2015). A faith-based community partnership to address HIV/ AIDS in the southern United States: implementation, challenges, and lessons learned. J Relig Health, 54: 122-133.View
Obong'o CO, Pichon LC, Powell TW, Williams AL. (2016). Strengthening partnerships between Black Churches and HIV service providers in the United States. AIDS Care, 1-5.View
Pichon LC, Powell TW, Ogg SA, Williams AL, Becton-Odum N et al., (2016). Factors Influencing Black Churches' Readiness to Address HIV. J Relig Health, 55: 918-927.
St. Lawrence J, Brasfield T, Jefferson K, Alleyne E, O'Bannon R et al., (1995). Cognitive-behavioral intervention to reduce African-American adolescents' risk for HIV infection. Journal of Consulting and Clinical Psychology, 63: 221-237.View
U.S. Department of Health and Human Services. (2017, October 26, 2017). Social Determinants and Eliminating Teen Pregnancy.View