
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 2 (2018), Article ID: JPHIP-129
https://doi.org/10.33790/jphip1100129Research Article
Examining the Concerns of Low-income, African American Postpartum Mothers in Order to Create Effective Health and Weight-related Programs
Riley A. Dodson, Bailey K. Allen, Jennifer L. Zuercher*
Department of Applied Health, Southern Illinois University Edwardsville, Campus Box 1126, Edwardsville, IL 62026, USA
Corresponding Author Details: Jennifer L. Zuercher, Department of Applied Health, Southern Illinois University Edwardsville, Campus Box 1126, Edwardsville, IL 62026 , Phone: 618-650-5801, Fax: 618-650-3719, USA. E-mail: jzuerch@siue.edu
Received date: 25th September, 2018
Accepted date: 26th November, 2018
Published date: 20th December, 2018
Citation: Zuercher JL, Dodson RA, Allen BK (2018) Examining the Concerns of Low-income, African American postpartum mothers in order to create effective health and weight-related programs. J Pub Health Issue Pract 2: 129.
Copyright: ©2018, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Objective: Returning to prepregnancy weight is important for longterm weight control as well as for ensuring healthy subsequent pregnancies. In this study, we set out to discover the health-related concerns and intervention preferences of postpartum mothers living in East St. Louis in an effort to promote a return to prepregnancy weight among women living in this community.
Methods: Twenty-eight mothers of infants participating in the Women, Infants, and Children (WIC) program in East St. Louis, IL were recruited to participate in this qualitative study. Questions and discussion focused on mothers’ health concerns and their ability to prioritize their own needs. Using Atlas.ti, researchers conducted content and thematic analysis of group transcripts.
Results: Weight in and of itself was not generally a concern unless it interfered with one’s ability to be happy and comfortable with themselves. Women were interested in addressing their health needs, but ultimately, stress and other priorities get in the way. To address their needs, group-based interventions that involve their children (i.e. child care for younger kids and educational programming for older children) would be the most useful. Additionally, support between inperson sessions would provide opportunities for additional learning and motivation to continue pursuing health goals.
Conclusions: Prioritization of one’s own health is a challenge for mothers of infants given the demands of their role as a new mother. In creating health-related interventions for this population, weightspecific programs should be avoided while facilitating balance in participants’ lives should be the priority.
Keywords: postpartum, qualitative, African American, health concerns, weight
Introduction
Obesity is an epidemic in the United States. Obesity-related diseases, such as cardiovascular disease and diabetes are among the leading causes of death [1]. Individuals aged 25-34 have the highest incidence of weight gain [2]. For women, the childbearing years are a major factor; women are twice as likely to gain weight during this period given factors such as more liberalized gestational weight gain [3].
Although a weight gain of 11-40 pounds for a single fetus [4] or 25-62 pounds for multiple fetuses [5] is usually recommended during pregnancy, with more specific recommendations based on pre-pregnancy weight, this gain can be associated with some concerns. Sixty percent of women do not return to their pre-pregnancy weight, and women who retain weight at six months postpartum are more likely to become overweight or obese later in life [6]. Low-income women, especially those who belong to a minority group, are at an even higher risk than their low-income majority counterparts, as they were more likely to be overweight or obese before pregnancy [7]. Women from minority groups also gain weight during pregnancy at disproportionate rates, up to two to three times more than non- Hispanic white women [8].
Reducing weight gain in the postpartum period is challenging. New mothers do not necessarily prioritize themselves, but rather often feel that their own health is not as important to address as the health of their children [9,10]. The newborn’s constant demand for the mother’s time and attention further contributes to mothers failing to put necessary emphasis on their own well-being [11].
Additionally, many low-income communities, such as East St. Louis, IL, have experienced a significant reduction in resources to address health-related concerns among new mothers, such as WIC and Family Case Management [12,13]. In this high needs community where obesity impacts over 60% of new mothers [14], defining the specific concerns, needs, and most effective means of intervention is paramount so that effective and efficient programs can be developed and implemented.
The objectives of this research were four fold; to: 1) discover the health-related concerns as well as the barriers to addressing such concerns among postpartum mothers living in East St. Louis; 2) determine the breadth of knowledge related to weight, specifically the importance and methods of returning to pre-pregnancy weight; 3) examine methods to increase prioritization of personal health among new mothers living in this area; and 4) examine preferred intervention methods to promote health behavior change. Specifically, we set out to conduct focus groups discussions with postpartum women in East St. Louis to determine the health and weight-related issues, as well as the barriers that exist/need to be overcome in order for them to become involved in programs promoting a return to their prepregnancy weight. Further, we aimed to characterize new mothers’ knowledge and recognition of the importance of returning to prepregnancy weight as well as the life demands that might limit their ability to attend to their own health and weight-related concerns.
Methods
Qualitative research provides meaningful answers and is often the basis for designing future interventions within specific populations [15]. Focus group discussions are one method of qualitative research that allows us to obtain information and insight through the group interaction of individuals who are representative of the project’s target population. The purpose of this exploratory research program was to gain perspective on the specific knowledge, preferences, and barriers to positive health behaviors experienced by new mothers living in East St. Louis. To this end, five discussion groups were conducted in June and July, 2016 with women who had given birth within the last year. The study was approved by Southern Illinois University Edwardsville’s Institutional Review Board.
Recruitment
Mothers over 18 years of age, with infants (12 months and younger) who were participating in the Women, Infants, and Children (WIC) program in East St. Louis, IL were invited to take part in the discussions. Participants were informed about the study and invited to participate in the discussions by their nutritionist during scheduled clinic appointments. Exclusion criteria included an inability to speak English fluently and age (of the mother) at the time of the study being less than 18 years. The population of East St. Louis is 97.3% African American or Black [16]. Therefore, though there was no exclusion criteria based on race or ethnicity, participants were assumed to likely be a part of this group.
Focus group discussion protocol
All discussions were conducted in English and were held at the WIC facility. Sessions, led by a trained moderator, were expected to last between 1.5 and 2 hours. They began with participants providing informed consent and completing a brief survey, including information related to demographics, perceptions of the relationship between health and weight, and intervention modality preferences. A semi-structured interview guide was used to facilitate conversations (Appendix). The discussion began with the question “What are some of your own health concerns, being a mom of a new baby?” before getting to the key question of this segment of the discussion, “How has having a child influenced how you prioritize yourself and your health?”The conversation continued with discussion regarding perceptions and concerns related to weight and weight loss. Also, in order to learn more about participants’ knowledge of the relationship between breastfeeding and weight loss [17,18], participants were asked, “What have you been told about breastfeeding?”, followed by the probing question, “What have you been told about breastfeeding as it relates to weight loss?”In order to shift the discussion to possible solutions, a “miracle question”, a technique in which participants are asked to envision the perfect scenario for success, was used [19]; participants were asked, “If you could design the perfect program to help you return to your pre-pregnancy weight, what would it look like?”The discussion ended with a question about specific factors that would facilitate participation in a health-related intervention. A light dinner was provided and childcare was available. Participants received a $25 gift card in appreciation for their participation.
Analysis
Demographic and other survey data were analyzed using descriptive statistics. Each focus group discussion was recorded, transcribed, and checked for accuracy. Content and thematic analysis of the transcripts was conducted using qualitative analysis software (Atlas. ti, version 7.5.11, 2016, ATLAS. ti GmbH, Berlin, Germany).Three trained independent coders began analysis by reading transcripts without a pre-determined set of codes, allowing codes to evolve as they became more familiar with the subject matter. An initial codebook was developed, capturing relevant themes from the discussions. The transcripts were independently reviewed by the three coders and the most significant themes were determined. The three independent coders discussed the grouped quotes to determine the relevance of individual statements to both the category to which they were assigned and to each other. This procedure continued until consensus was reached on the correct placement of each statement.
Results
A total of 27 African American mothers participated in the five focus groups. Groups ranged in size from three participants to eight participants (Table 1). Data from one mother was excluded from the analysis because after the focus group discussion was completed, it was revealed that she was younger than 18. Mean age of mothers was 26.8 years old (Range: 20– 37). Mean age of the infants was 6.1 months (Range: 2 weeks – 12 months). A detailed list of mothers’ characteristics are in Table 2.
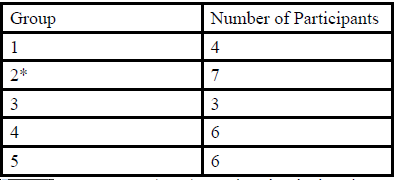
Table 1: Participants per Focus Group*
*One of the eight women who participated in Group 2 did not meet the inclusion criteria; her responses were not include in the analysis.
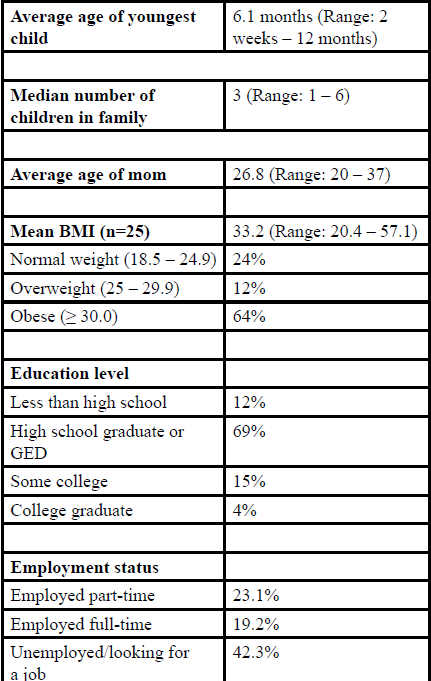
Table 2: Focus Group Demographics (N=26).
Analysis revealed two significant concerns influencing the mothers’ post-partum health: shifting priorities and stress. Additionally, while mothers’ were somewhat knowledgeable about breastfeeding, several shared incorrect information regarding the consequences and benefits to both the mom and baby. Preferences related to intervention method were discussed as well.
Significant concerns
Following an icebreaker, mothers were asked, “What are some of your own health concerns being a mom of a new baby?” While a variety of specific health issues were discussed, concerns primarily related to a change in how the mothers prioritized themselves and the stress that accompanied parenting. Direct or specific health recommendations and concerns did not necessarily arise; women were participating in health behaviors that lead to negative health consequences rather than specific disease or health related concerns.
Shifting priorities
For these new mothers, priorities shifted both when they became pregnant and when their babies arrived. They found themselves frequently putting aside activities they once enjoyed to take care of the new child. One mom in Discussion Group 3 stated, “There’s a lot of stuff, like fun stuff, that I used to do that I don't do anymore. Like go out and enjoy myself, but I can’t do it as much as I like to or used to.” For many, having a baby means putting their child before everything. All moms reported that their child was their number one priority and they put their own needs last. As stated by a mother in Discussion Group4, “I put my kids ahead of everything. Well, God come first, then my kids.”
Along with the new child, many moms reported having other children to attend to as well. Making sure all of their children were fed and taken care of was essential. When asked if their personal health was a priority, a mother from Discussion Group 4 responded, “It is not a priority to address my needs because it’s my kids I’m worried about all the time....” After their child or children were well taken care of, then the mothers would be able to focus on themselves. Unfortunately, they often do not get that time, even to do things they have to do, like “use the bathroom by myself” (Discussion Group 1). As a result, the mothers have difficulty focusing on their own needs and health concerns.
Several moms mentioned that they do not have time in the day to eat. "You’re so busy doing other things that you forget to eat," a mother from Discussion Group 1 stated. Taking kids places and doing things for them often leads mothers to reach the end of the day having forgotten or not having had time to eat, and focused solely on getting sleep. As stated by a mom in Discussion Group 2, “I work 12 hours a day, 4 days a week…when I get home, I am so tired. I give the kids their baths and sometimes I don’t feel like doing what I need to do for myself.”
Another area of life that falls lower on the list of priorities for new mothers is their partner. Mothers reported pushing aside relationships and spouses due to a lack of time and energy to devote to them. As stated by a mom in Discussion Group 4, “…my husband, he's at the bottom….” The mothers also cited the ability of partners to take care of themselves as a reason for how they were being prioritized. One mother(Discussion Group 4) discussed that she does, “…care about his needs…[but] if you are grown, you can take care of yourself.”
Stress
Mothers in the focus group discussions frequently brought up the topic of stress – that their lives were stressful and that they lacked effective means of dealing with the stress that they were experiencing. As previously mentioned, many of the mothers had newborns as well as other children that they needed to care for. For a mom in Discussion Group 4, even though her “…oldest helps me out with the two younger kids…”, she still struggles with the stress of taking care of everyone. Further, because her oldest is “…still a kid...,” she tries to minimize the responsibility she gives this child. Managing this type of dynamic adds its own stress.
Several mothers tied their high level of stress to their lack of sleep. The newborns’ sleeping schedule made it hard for the moms to get a good night’s sleep. "I get my sleep when they go to sleep" stated one mom from Discussion Group 1. Several mothers thought it was a good idea to take a few naps alongside their newborn, though unless they had a family member available to help out, the women were usually unable to do so. Further, as stated by a mother in DiscussionGroup4, if you do take a nap rather than working around the house while the children nap, “…your house is going to look like a mess,” adding to the stress level.
Lack of support was discussed as an additional factor impacting the stress levels among mothers in the discussions. While some moms identified having helpful family and friends nearby, who could “…take my kids for me just so I can take a bath or so I can clean…” (Discussion Group 4), most felt they did not have this type of support. Rather, mothers more frequently cited “…coming home with a newborn and you have other kids with no help. You have to be hands-on with them and the baby; you have to take all of them everywhere you go because of no help…” (Discussion Group 4).
Emotional ramifications of dealing with the stress of being a new mom were discussed as well. A mother from Discussion Group 3 stated that “...Sometimes I find myself getting sad about a lot of things that I used to do and can’t do now, or places I used to go and can’t go to now because I’ve got the kids and I have to find somebody to watch them, and it’s a lot. It’s stressful because I’ll want my own time and not have the kids all the time, but there is no way around it….” Mothers also recognized that “…you have to be mentally healthy too, because if your mind isn’t right, you won’t be worried about your body and your health” (Discussion Group 5).
Impacts of breastfeeding
In order to begin a discussion about knowledge about the association between breastfeeding and weight loss, women were asked the question “What have you been told about breastfeeding?” This led to a greater discussion regarding the challenges and complications related to whether and why mothers were choosing to or not to breastfeed.
Information
Women indicated that they obtained information regarding breastfeeding from a variety of sources including physicians, parenting classes, a peer breastfeeding advocate (from the WIC program), friends, and family. Mothers acknowledged many benefits to breastfeeding, for both their babies as well as themselves; from reducing risk for “…breast cancer…and also our pockets. We don’t have to worry about formula” (Discussion Group 1), to creating “… a stronger attachment, bigger bond” (Discussion Group 2). Additionally, women were aware of the consequences that their own lifestyle habits could have on their breastfeeding children; “Everything that you put in your body will go straight to that baby” (Discussion Group 4). Unfortunately, some mothers had inaccurate information. For instance, a mother in Discussion Group 3 stated that she “…thought it made you gain weight because the baby is gaining weight when you’re breastfeeding…”, which may have contributed to her choice to not breastfeed.
Drawbacks outweigh benefits
At least one mom in each of the five groups brought up the personal benefit of weight loss and a quicker and easier return to pre-pregnancy weight. As stated by a mother in Discussion Group 1, “It does help. I was losing so much weight. It works.” In spite of this and some other cited benefits, many mothers acknowledged that they chose to bottle feed anyway. Some chose not to breastfeed for fear of their child getting hungry at an inopportune time, causing them to have to “…take my thing out and feed them right here” (Discussion Group 4). For others, harmful lifestyle habits, such as smoking, kept them from breastfeeding. As stated by a mom in Focus Group 3, “…I smoked cigarettes, so I didn’t want to start breastfeeding my baby while I was smoking.” For yet another, “I really tried to breastfeed, but I couldn’t because I was going back to work, and when I tried it, I was so uncomfortable. I was so uncomfortable”.
Intervention preferences
In an effort to gain insight into intervention preferences, mothers were asked to describe the “…perfect program to help you return to your pre-pregnancy weight.” Components discussed included format, topical preferences, and participation incentives.
Format
Mothers in several groups initially brought up a traditional in-person format as the preferred means of intervention. This could be one-on-one where they would receive individualized attention and recommendations, but overwhelmingly, mothers talked about group interventions, lasting between 30 and 60 minutes, where women experiencing the same types of challenges could provide both validation and support for the situations they were experiencing; "... some people do be wanting to sit in a group and talk to people so they can learn more..." (Discussion Group 2). A smaller, more intimate group was thought to be able to provide someone to be accountable to, that “…you can talk to and get in contact with on a regular basis” (Discussion Group 5).
Mothers also expressed support for a group intervention that included some type of technology or social media component, such as Facebook. In between meeting sessions (whether they be weekly or monthly), contact with other participating mothers could provide motivation and support because “…you can jump in and put your comment, and read other people's comments” (Discussion Group 1). Text messaging or email could also provide continued support as “…you can always go back to it when you get a second and read it" (Discussion Group 1). Also, positive behaviors could be encouraged and supported. Videos, including exercise and cooking demonstrations, were also cited as desirable on several occasions.
Topics of Interest
As part of the discussion regarding intervention, mothers offered ideas of topics and activities that they would be interested in learning about and participating in, respectively. Ideas discussed included typical components of health improvement or weight-management programs, such as grocery store tours, cooking experiences, and some type of physical activity. For in person interventions, “Going out and being active” (Discussion Group 2) would be important. Further, having “…somebody around when you go to the grocery store” (Discussion Group 5) was seen as helpful for supporting healthy decisions and reducing the instances of making unhealthy choices. For asynchronous interactions, YouTube was mentioned as a favorable way to share demonstrations as, “They put everything else on YouTube” (Discussion Group 1).
Again, because women weren’t specifically concerned about weight, and most of them were feeling “…comfortable with the size that you are...”(Discussion Group 1), the pursuit of a program directly related to weight wasn’t important for them. This did not mean, though, that an intervention related to weight wasn’t warranted. Given the average BMI for participants was 33.2, a weight-related program would be relevant. Because women spoke about weight-loss being associated with disease (e.g., AIDS) or other negative concerns, creating a program that indirectly promotes healthy weight, rather than making it the focus, might be more effective.
Incentives for Participation
Location was discussed as one of the most important factors for predicting success in a face-to-face intervention. This could be “…in the middle…” (Discussion Group 5) of the community, or at a location that was visited relatively frequently, such as the WIC office where the Discussion Groups were held. Transportation, including lack of their own vehicles and dependence on public transportation, was a limiting factor to many of the mothers living in this community. Making sure the location is not off the beaten path was deemed essential.
Additionally, mothers in several groups thought it was very important to consider their children. In instances where children were not old enough to participate in activities, having childcare provided was an important element in making it possible for mothers to attend the program because “…some might have problems finding someone to watch [their] kids” (Discussion Group 4). Further, mothers would “…know that other people have their kids and they have other kids to play with….” (Discussion Group 2). Those with older children expressed great desire in both having their children nearby as well as having them learn about health and healthy behaviors. Mothers felt it would be both fun and educational for the children, and “…give the kids a chance to do something too, instead of running around outside” (Discussion Group 3).
Mothers in the Groups expressed concern for being able to get other moms to participate in an intervention. More than half of the women expressed that they would be slightly to not at all likely to participate in a group related to achieving a healthy weight after having a baby. Even as part of the group discussions, what was in it for them in the present was much more of an incentive than the longer-term impact of participation. As stated by a mom in Discussion Group 4, “If there was something in it for them. You telling us we are getting a [gift card] is why we are here today. I’m not going to lie.” Aside from monetary incentives, particularly at the end of the month when SNAP and other benefits may have run out, other enticements suggested included diapers or other tangible goods.
Obstacles to Intervention
While mothers expressed that they believed that a health-related intervention providing support, encouragement, and guidance for new mothers would be beneficial, many believed that an in-person intervention, especially, would not find success in this community. They felt that conducting an intervention, in general, would be challenging in this community as people “…don't care about stuff like this” (Discussion Group 3), and only those with an inherent interest would participate in a meaningful way. Further, a few expressed that “…some might only show if they are rewarded by doing stuff” (Discussion Group 5). The strength of the behavioral risk factors available in this community, including “... half of them are out doing drugs or prostituting” (Discussion Group 5), would likely interfere as well.
Discussion
In this study, we set out to characterize the perspectives of women living in East St. Louis with regard to health and weight, and their ideas about how to best connect with other women in their community to create effective programs addressing these topics. While health promotion and weight management are topics of relevance for women in general, the difficulties these women experience, as well as the challenges of connecting with this community, were reinforced throughout this study.
Like any mom, mothers in this disadvantaged community want the best for their children and prioritize their children above themselves. They recognize the benefits of eating healthfully and taking care of themselves. Unfortunately, lack of support – financially as well as with time and individuals – cause additional burden on the moms themselves. Because other family members and friends are usually in the same situation, there are limited others that they can depend upon. Further, because of a lack of financial means, being able to hire a babysitter in order to get some “me time”, some necessary sleep, or to coordinate their households, finding adequate relief is rare.
Conversations during groups also developed around the topic of breastfeeding. Initiation of and continued breastfeeding among mothers was low, which was somewhat expected given that the rate of initiation of breastfeeding among African American women is the lowest among all races [20]. Mothers acknowledged several benefits of breastfeeding, but due to stress and failure to prioritize one’s own health, chose to continue smoking. One possible reason for this may be that these mothers have limited opportunities to do things for their own pleasure; smoking may be one area that they can do for themselves. Further, the additional stress of combating an addiction, such as nicotine, may have been more than these mothers could reasonably be expected to take on at the time. Unfortunately, while they may have felt that they were reducing their stress by continuing to smoke, they were also adding to their burden with the cost of cigarettes and the health ramifications.
Creating balance is a challenge for all families, but especially for low income and households with single parents. Several women mentioned working jobs with non-traditional (6pm to 8am) work hours. Low-income, working parents are among those most likely to be following this kind of schedule [21]. This presents an added challenge as childcare is more difficult to find, and if found, is more expensive during these non-traditional work hours. Further, this may place burden on older children. While some mothers in the discussion groups expressed getting some relief of stress due to the help of these children, they also recognized that this is not always ‘fair’ for those children. As a mom from Discussion Group 3 explained, she “…[tries] to do something fun for me and my daughter to do…”, like going to a movie together, to reward her for her help, but this is not always feasible as it costs more money and requires yet another person to be available to help watch the younger children.
While the women did discuss their ideas for intervention, they also stated that a weight-related program did not really resonate with them, and that it likely wouldn’t be important to others in their community. Only two mothers across all groups mentioned a number when asked what a healthy weight was. Instead, mothers mostly talked about how their clothes fit and how they feel about themselves. This perspective, paired with the element that others take precedence in the majority of situations, validate that women in this community need to be approached in a different manner. Addressing stress management as well as the importance of self-care, and providing a variety of supports for these moms would likely result in more effective and meaningful outcomes.
The use of technology in interventions with low-income, postpartum mothers is relatively new, but has shown promise in effecting weight loss [22,23]. Intervening with multiple strategies – including in-person groups, as well as Facebook groups, text messages, and YouTube videos that can be referred to multiple times and as convenient, would likely result in greater buy-in from this community. Creating a program focused on bringing balance and stability to women’s lives rather than strictly focusing on weight may find more success as well as help in the trust building process in this community.
There are a few important limitations to this study. First, as is the case with most qualitative work, this study was based on a convenience sample of mothers in a WIC program serving one community. Also, because mothers were recruited only from this one particular WIC clinic in East St. Louis, IL, it is possible that other groups, including those in need of but not signed up for WIC benefits, were not represented by this work. That said, recruitment occurred over a period of approximately six weeks, allowing for a relatively large pool of mothers to be reached. Further, mothers were told during recruitment that they could share information about the discussion group with friends and family, and that they could bring them to participate if they fit the eligibility criteria as well, which occurred in at least two cases.
To be culturally sensitive, it is usually recommended that Focus Group leaders be of the same race, or at least from the same community, as participants [24]. Unfortunately, due to delays in scheduling discussions and personnel changes, a race-matched leader was not available at the time groups were being run. This may have contributed to mother’s perceptions and responses. That said, clinic staff, whom mothers were very familiar and comfortable with, were available and supportive of the discussions, and encouraged participants to be open and honest so that their needs could be heard and addressed.
Strengths of this study include efforts to create a thorough perspective of the needs and desires of mothers living in this community, which is frequently described as a challenging place to work. While this low-income, underserved population would benefit from additional health outreach, there are often other issues that need to be addressed first; the hardships these mothers face often overshadow health improvement. This likely contributed to some mothers’ feelings that their community was ‘not right’ for a post-partum weight-related intervention. Using this guidance on how to better intervene in this complicated community will create perspective for creating effective interventions in which postpartum mothers may be more willing to participate.
Acknowledgements
The Institute for Urban Research Scholar program at Southern Illinois University Edwardsville provided funding for this study. Additionally, the Undergraduate Research and Creative Activities (URCA) program provided funding assistance for undergraduate students working on this project. The authors would like to thank the staff and clients at the East Side Health District, Onikia Brown, PhD, RD, and David Cluphf, PhD for their support of this project.
Conflict of Interest Disclosure
The authors have no conflicts of interest.
Participant Consent Statement
Informed consent was obtained from participants of this study as approved by the university’s Institutional Review Board.
References
National Center for Health Statistics. Health, United States, 2016: With Chartbook on Long-Term Trends in Health. (DHS Pub. no. 2017-1232.) Hyattsville, MD, 2017.View
Sheehan TJ, DuBrava S, DeChello LM, Fang Z (2003) Rates of weight change for black and white Americans over a twenty year period. Int J Obes 27: 498-504.View
Yi-Li K, Chi-Li Y, Chin-Lung F, Lee MF, Lin PC et al. (2013) Community-based postpartum exercise program. J Clin Nurs 22: 2122-2131.View
Abrams B, Heggeseth B, Rehkopf D, Davis E (2013) Parity and body mass index in U.S. women: a prospective 25-year study. Obesity 21: 1514-1518.View
Luke B, Hediger M, Nugent C, Newman RB, Mauldin JG et al. (2003) Body Mass Index--Specific Weight Gains Associated with Optimal Birth Weights in Twin Pregnancies. Vol 48.; 2003.View
Rooney BL, Schauberger CW (2002) Excess pregnancy weight gain and long-term obesity: one decade later. Obstet Gynecol. 100: 245-252.View
Ogden CL, Carroll MD, Kit BK, Flegal KM (2014) Prevalence of Childhood and Adult Obesity in the United States, 2011– 2012. JAMA 311: 806-814.View
Gore SA, Brown DM, West DS (2003) The role of postpartum weight retention in obesity among women: A review of the evidence. Ann Behav Med 26: 149.View
Carter-Edwards L, Østbye T, Bastian LA, Yarnall KSH, Krause KM et al. (2009)Barriers to adopting a healthy lifestyle: insight from postpartum women. BMC Res Notes 2: 161.View
Barkin JL, Wisner KL (2013) The role of maternal self-care in new motherhood. Midwifery 29: 1050-1055.View
Herring SJ, Cruice JF, Bennett GG, Davey A, Foster GD et al. (2014) Using technology to promote postpartum weight loss in urban, low-income mothers: a pilot randomized controlled trial. J Nutr Educ Behav 46: 610-615.View
Smith CP (2015) Lack of state budget threatens cuts to East St. Louis Health District. Metro-East News.View
District ESH. Family Case Management (2018).View
St. Clair County Community Health Needs Assessment (2015).View
Fern EF (2001) Advanced Focus Group Research. Thousand Oaks, CA: SAGE Publications.View
Bureau USC (2012-2016) American Community Survey 5-Year Estimates.View
Dewey KG, Heinig MJ, Nommsen LA (1993) Maternal weightloss patterns during prolonged lactation. Am J Clin Nutr. 58: 162-166.View
Krause KM, Lovelady CA, Peterson BL, Chowdhury N, Østbye T et al. (2010) Effect of breast-feeding on weight retention at 3 and 6 months postpartum: data from the North Carolina WIC Programme. Public Health Nutr 13: 2019-2026.View
Berg IK, Szabo P (2005) Brief Coaching for Lasting Solutions. New York: ww Norton; 2005.View
Jones KM, Power ML, Queenan JT, Schulkin J (2015) Racial and Ethnic Disparities in Breastfeeding. Breastfeed Med. 10: 186-196.View
Enchautegui ME, Johnson M, Gelatt J (2015) Who Minds the Kids When Mom Works a Nonstandard Schedule? Washington, D.C.View
Gilmore LA, Klempel MC, Martin CK, et al. (2017) Personalized Mobile Health Intervention for Health and Weight Loss in Postpartum Women Receiving Women, Infants, and Children Benefit: A Randomized Controlled Pilot Study. J Women’s Heal. 26: 719-727.
Phelan S, Hagobian T, Brannen A, Hatley KE, Schaffner A et al. (2017) Effect of an Internet-Based Program on Weight Loss for Low-Income Postpartum Women: A Randomized Clinical Trial. Obstet Gynecol Surv 72.View
Stewart DW, Shamdasani PN (2015) Focus Groups: Theory and Practice, 3rd. Edition. Washington, D.C.: SAGE Publications.
Supplementary File
Journal of Public Health Issues and Practices
East St. Louis Post Partum Moms Focus Group Guide
Introduction
This is a discussion group to talk about being a new mom, and taking care of your own health needs and weight. We are interested in learning from you, to hear about how new mothers here in East St. Louis feel about these things.
Let’s begin by going around the room quickly. Please tell us your name and what food you craved most often when you were pregnant.
- New moms often talk about how having a baby changes their priorities, specifically related to themselves. What are some of your own health concerns, being a mom of a new baby?
- How has having a child influenced how you prioritize yourself and your health? Probes:
Who else’s needs do you put before your own?
What did you used to do for yourself that you no longer do (i.e. walks)?
Transitional statement:
Up to now, we’ve been talking about your personal health priorities, having a young child. Now we’d like to shift direction a little bit and talk about how the relationship between health and body weight.
3. What does being at a healthy weight mean to you?
Probes:
. What is a healthy weight?
. Is being at a healthy weight a concern for you?
. If it is a concern, what are some steps that you’ve taken to reach it?
. If it is not a concern, why not?
. If you were not successful, why do you think you weren’t?
4. Have you ever reached out for help with weight loss or maintaining a healthy weight?
Probe:
• If you did, was that person(s)/program successful in helping you? Why or why not?
5. How would you addressing your health concerns impact your family?
Probe:
• What kind of support would you look for?
6. What have you been told about breastfeeding?
Probe:
• What have you been told about breastfeeding as it relates to weight loss?
If we focus only on problems, we can get to feeling stuck and frustrated. Let us take time out now and use our imaginations, and think about the situation in a different way. We call this the “miracle question.”
7. If you could design the perfect program to help you return to your pre-pregnancy weight, what would it look like?
• Groups
• One-on-one contact in person
• Phone – calls, text messages
• Computer/internet
• TV/video
8. If the program were to be implemented, what are some other factors that would make you want to attend (other than your desire)?
• Childcare
• Food
• Convenient location