
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 3 (2019), Article ID: JPHIP-133
https://doi.org/10.33790/jphip1100133Review Article
Adenovirus Infection Rate of Chinese Children with Respiratory Diseases: A Meta-analysis
Shuting Yue1,2, Na Li1,a, Can Jian1, Xiaoxia Dai1*
1School of Public Health, Health Science Center, Xi'an Jiaotong University, Xi'an,710061, China.
2World Publishing Xi'an Corporation Ltd, Xi'an, 710003, China
Corresponding Author Details: Xiaoxia Dai, School of Public Health, Health Science Center, Xi'an Jiaotong University, Xi'an,710061, No.76 Yanta West Road, China. E-mail: xxiadai@xjtu.edu.cn
aCo-first Author: Na Li, School of Public Health, Health Science Center, Xi'an Jiaotong University, Xi'an, China.
Received date: 21st April, 2018
Accepted date: 06th December, 2018
Published date: 29th January, 2019
Citation: Yue, S., Li, N., Jian, C., & Dai, X. (2019). Adenovirus infection rate of Chinese children with respiratory diseases: A Meta- analysis. J Pub Health Issue Pract 3: 133.
Copyright: ©2019, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Objectives: To analysis the epidemiological characteristics of adenovirus infection rate of Chinese children with respiratory diseases.
Methods: Database such as PubMed, EMbase, CNKI, VIP and Wan Fang Data were searched for studies investigating adenovirus infection rate of Chinese children with respiratory diseases up to August 1st, 2018. Screened literature, exacted data, and methodological quality assessment of included studies according to the inclusion and exclusion criteria, then used the Stata11.0 for Meta-analysis.
Results: The analysis of 54 studies showed that the rate of adenovirus infection in children with respiratory diseases in China was 4.5%, and the confidence interval was 3.7% to 5.6%. Subgroup analysis indicated that the adenovirus infection rates of children with respiratory diseases in northern and southern China were 8.3% and 3.5%, respectively. The detection rate of polymerase chain reaction (PCR) was 7.8%, and the immune fluorescence and ELISA methods were 2.6% and 8.8%, respectively. The adenovirus infection rates of sample size in 1000 cases, 1000-5000 cases and more than 5000 cases were 5.8%, 4.7% and 3.1%, respectively. Adenovirus infection rates published in the 2000-2005, 2006-2010, and 2011-2018 groups were 3.5%, 1.4%, and 4.8%, respectively. The adenovirus infection rates in the 1 year, 1-3 years and 3 years were 5.3%, 4.8%, and 3.6%, respectively.
Conclusions: The adenovirus infection rate of Chinese children with respiratory diseases is different in different areas, test methods, sample size, the published time and study span.
Key words: children; adenovirus infection; respiratory diseases; meta-analysis
Introduction
Adenovirus (AdV) is a kind of double-stranded DNA virus without capsular, and as far as we know that it is one of the largest and most complex DNA virus without capsular. Adenovirus consists of seven species (A-G) and more than 67 types within these species have been identified. Adenovirus could be in tonsil, lymph and intestinal tissue of the body in a long-term latent situation, it is a common pediatric pathogen responsible for a wide variety of infection. Adenovirus often cause multiple organ damage and cause acute febrile respiratory diseases, pharyngo-conjunctival fever, pneumonia, epidemic keratitis and gastroenteritis. Adenovirus has been considered an important respiratory pathogen and may cause death. Respiratory infection caused by adenovirus in non-immuno compromised patients is usually mild and self-limited. In contrast, in immune compromised patients, adenovirus infection can be disseminated and result in a considerable mortality rate [1-3]. The studies found that adenovirus pneumonia infection were mostly children, it was more serious than ordinary pneumonia and would have sequelae such as bronchiectasis, obliterative bronchiolitis and hyperlucenct lung et al [4]. Adenovirus infections could occur as outbreaks, especially where there was a concentration of military personnel or in cities. Adenovirus type 4 infection was most common in the US military [5], type 14 outbreaks were found in Chinese schools [6]. adenovirus type 3 (AdV3) was the most common genotype of respiratory adenovirus infection in many regions. There are differences in virus types in different populations and regions.
This study analyzed adenovirus infection rate of Chinese children with respiratory diseases by Meta-analysis method, and our results can be used for preventive measures, diagnosis and treatment work.
Materials and methods
Inclusion and exclusion criteria
Literature: The studies which were related to adenovirus infection rate of Chinese children with respiratory diseases were included. The studies must be written in either Chinese or English.
Study subjects: The study subjects are patients aged 0-18 years with adenovirus infection respiratory diseases. The diagnosis of respiratory disease according to WHO diagnostic criterion.
Outcome: Adenovirus infection rate.
Exclusion criteria: 1. Epidemic or pandemic outbreak; 2. Immuno compromised population; 3. The studies only involved in upper or lower respiratory tract infection.
Search strategy for study identification: Database such as PubMed, EMbase, CNKI, VIP and Wan Fang Data were searched for studies investigating adenovirus infection rate of Chinese children with respiratory diseases up to March 1st, 2018. Search terms are children, adenovirus infection, respiratory disease. The search strategy for PubMed is#1 children AND #2 adenovirus infection AND #3 respiratory diseases
Study selection, data extraction and Quality assessment: Study selection was performed following the removal of duplicates in Endnote X7 software. Titles and abstracts shall then be screened following inclusion criteria, following which the full texts of potentially eligible articles will be obtained. These full texts will be screened using a standard and pre-tested form to include eligible studies. Data will include the geographic region where study was conducted, the year study was carried out and the year of publication, study design, sample size, age, season, adenovirus infection rate and detection method. The study quality evaluated by the evaluation criteria for observational study from Agency for Healthcare Research and Quality (AHRQ). The poor quality of studies will not be included to further analysis.
Statistical analysis: All identified data will be entered into Stata11.0 software for statistical analysis. Heterogeneity across studies was determined for choosing different analysis model and heterogeneity was assessed using the I2 values, assuming that I2 values of 25%, 50% and 75% represent low, medium and high heterogeneity, respectively. The subgroup analysis is used to analysis the different types of adenovirus infection rate of Chinese children with respiratory diseases and explore the source of heterogeneity. Sensitivity analysis is done to the results and the publication bias is evaluated by Egger, s Test.
]Results
Study selection result
This analysis was carried out using the PRISMA. Fifty-four studies meeting the inclusion criteria were included in this study, including 309149 patients. Details of the study selection process (Figure 1).
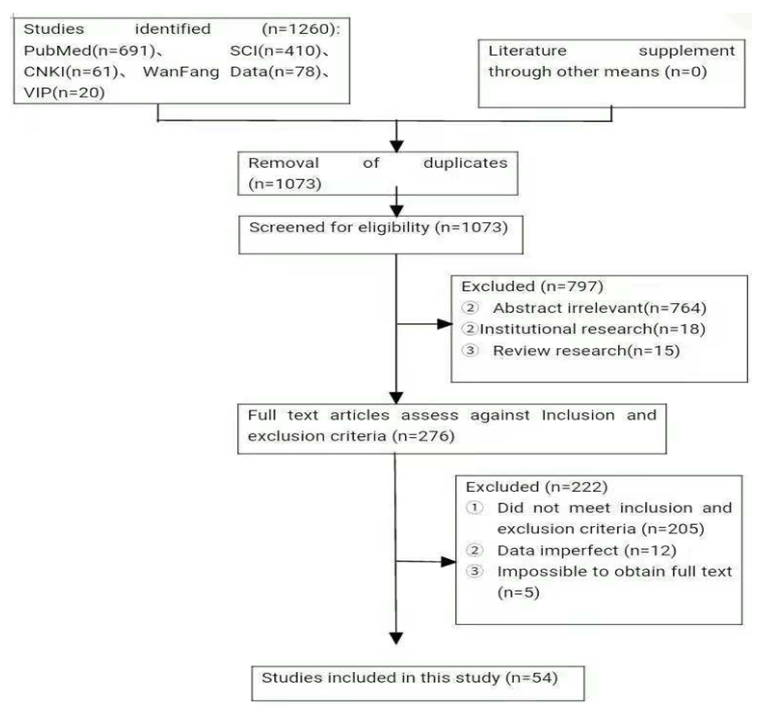
Figure: 1 Details of the study selection process.
3.2.Characteristics and quality assessment
Results of the 54 literatures enrolled, half were published in Chinese, the others were English literatures. The year of publication concentrated in between 2011 and 2018 (n=50, 93%). Most of studies used PCR (Polymerase Chain Reaction) methods (n=23, 43%), 27 studies used immunofluorescence method and 4 studies chose ELISA method. A total of 15 studies were from northern (28%), and 38 studies were from southern (70%). Summer is the season with high rate of adenovirus infection in the southern and it mostly occurred in spring and winter in the north. Among these studies, most of the patients were infants less than 5 years old. However, only nine studies had pointed out the classification of adenovirus, in which adenovirus typing was mainly type 3, followed by type 7 and type 4. In the results of quality evaluation, the scores of most studies are more than or equal to 6 points (n=29, 54%), only one study (Wang, M. 2001) scored 5 points. Table 1 presents their basic characteristics and the score of quality evaluation.
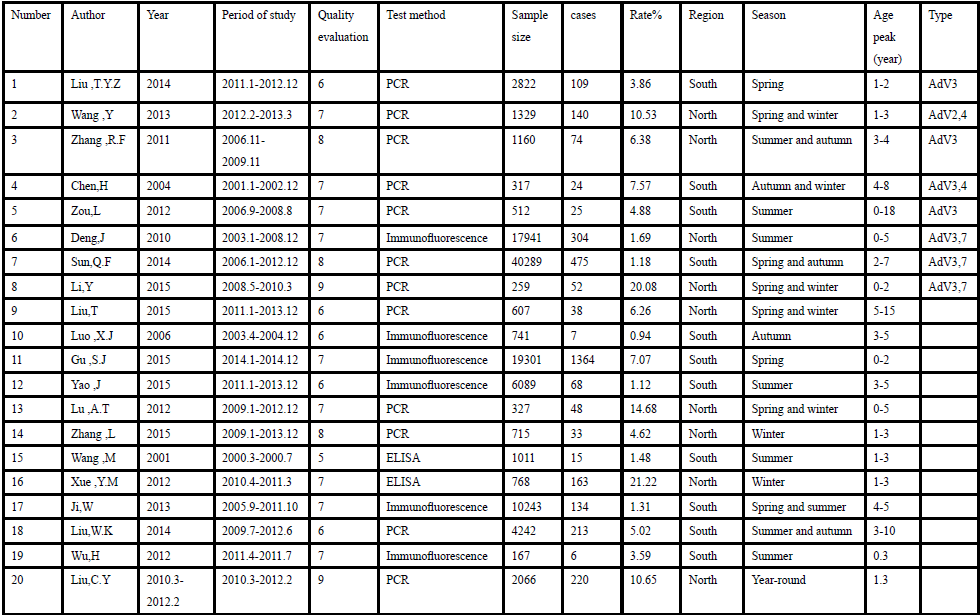
Table: 1 Basic characteristics.
3.3. Sensitivity analysis
After deleted with one-way research in turn, then observed the influence. of the combined effect variable for sensitivity analysis. Figure 2 shows the result of sensitivity analysis.
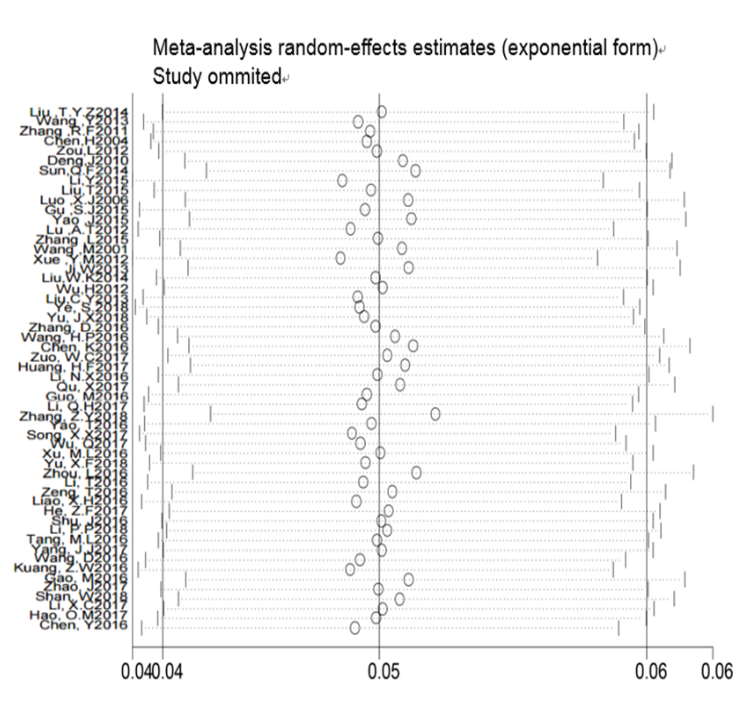
Figure: 2 Result of sensitivity analysis.
Results of Meta-analysis
Because of obvious heterogeneity among different studies, the random effect model is used for meta-analysis. 54 studies are included to further analysis.
Adenovirus infection rate of Chinese children with respiratory diseases
Table 2 shows the adenovirus infection rate of Chinese children with respiratory diseases is 4.5% [95%CI (3.7%, 5.6%)], heterogeneity is high (I2=99.2%, P<0.0001). The heterogeneity will be analyzed later. Figure 3 is the forest plots.

Table: 2 Summary of Meta-analysis of adenovirus infection rate of Chinese children with respiratory diseases.
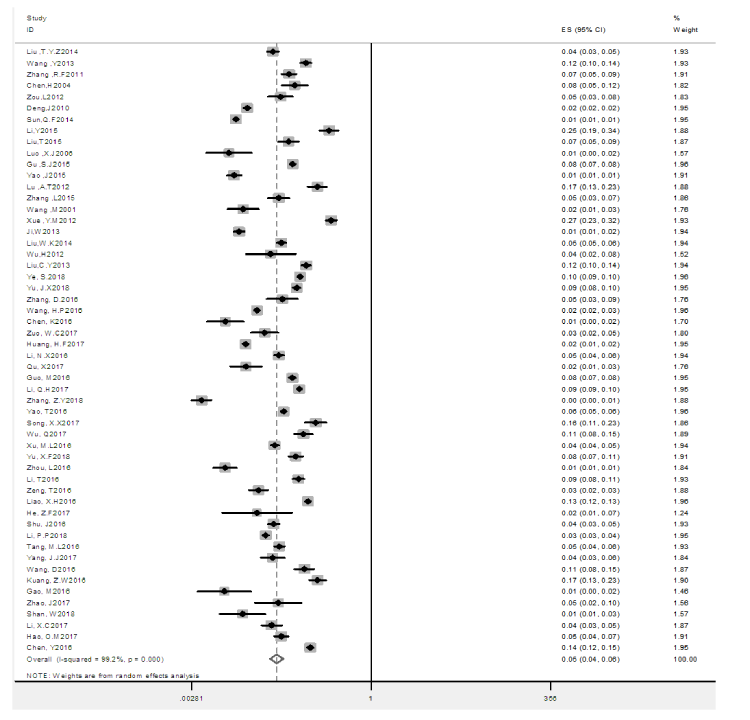
Figure: 3 Meta-analysis forest plots.
Region analysis
Table 3 shows the adenovirus infection rate of Chinese children with respiratory diseases in the north is 8.3%, and it is 3.5% in the south. The former is higher than the latter (P<0.05). This difference may be related to climate and living habits.
3.4.3. Test method analysis
Table 4 shows the adenovirus infection rate of Chinese children with respiratory diseases by PCR methods is 7.8%, 2.6% by immunofluorescence method and 8.8% by ELISA method. The PCR and ELISA method may be more sensitive than immunofluorescence method in adenovirus detection.
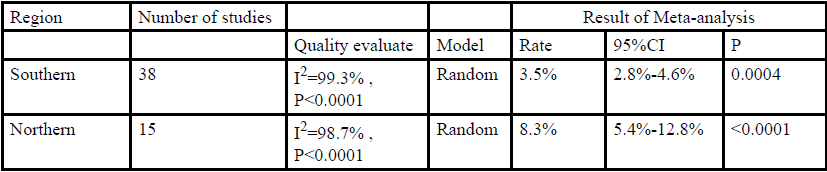
Table: 3 The adenovirus infection rates of Chinese children with respiratory diseases in different regions.
Sample size analysis
The adenovirus infection rate of Chinese children with respiratory diseases in the group within 1000 cases (including 1000 cases) is 5.8%, 1000-5000 cases is 4.7%, and the group more than 5000 cases (including 5000 cases) is 3.1%. It suggests both large sample size and small sample size may affect results of studies. The analysis of sample size described in Table 5.

Table: 4 The adenovirus infection rates of Chinese children with different testing methods.

Table: 5 The adenovirus infection rates of Chinese children with respiratory diseases in different sample size group.
Published time analysis
The adenovirus infection rate of Chinese children with respiratory diseases in the group within 2000-2005 is 3.5%, 2006-2010 is 1.4%, and the group within 2011-2018 is 4.8% (Table 6). The year of publication concentrated in between 2011 and 2018 (n=50, 93%). With the fluctuation of adenovirus infection, the attention paid to adenovirus is increasing.

Table: 6 The adenovirus infection rates of Chinese children with respiratory diseases in different published time group.
Time span analysis
The adenovirus infection rate of Chinese children with respiratory diseases in the group within one year (including one year) is 5.3%, 1-3 year (including three years) is 4.8%, and the group more than three years is 3.6% (Table 7). It suggests the time span may also be an affecting factor.

Table: 7 The adenovirus infection rates of Chinese children with respiratory diseases in different time span.
Publication bias
There are publication bias in different groups. The subgroup of southern, and group of sample size have publication bias and these factors will be analyzed in meta regression. Table 8 shows the publication bias of subgroups in our study.
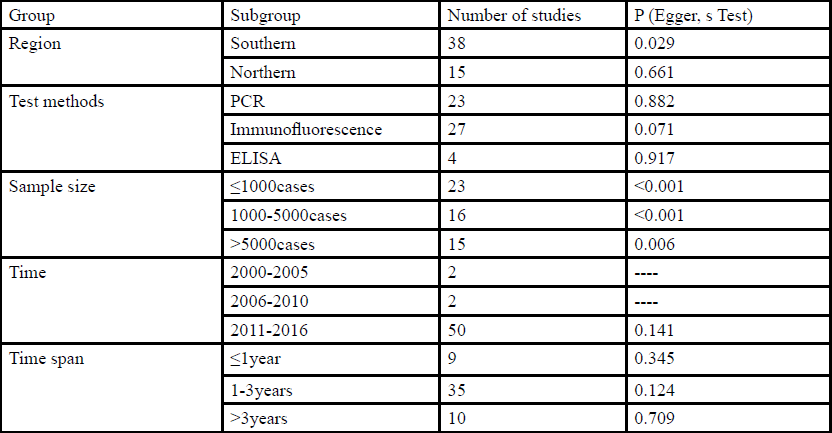
Table: 8 Result of Publication bias.
Meta regression
Meta regression has been done to explore the reason of heterogeneity. The random effect model is used for meta regression. The result of regression analysis expressed that the test methods and published time were the influencing factors, and 35.7% of heterogeneity can be explained by their difference. Table 9 shows the result of univariate analysis. effective and accurate.
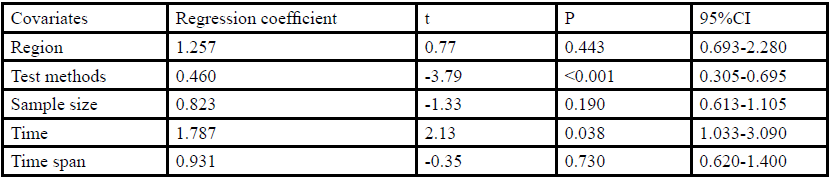
Table: 9 Result of Meta regression.
Conclusion
Adenovirus is one of the more common pathogens for children and adolescents respiratory diseases, and it would cause serious pneumonia or bronchitis even death in infants. Our study analyzed the adenovirus infection rates of Chinese children with respiratory diseases by meta-analysis method. The results show the adenovirus infection rate of Chinese children with respiratory diseases is 4.5% [95%CI (3.7%, 5.6%)].
The adenovirus infection rate of Chinese children with respiratory diseases in the north is 8.3%, which higher than 3.5% in the south, and the difference is statistically significant (P<0.05). The north of China is colder than the south, and the unbalance among our regional economy are obviously. These factors may lead to huge difference in medical environment between the north and the south. The result with PCR and ELISA method (7.8%, 8.8%) are higher than the result of immunofluorescence method (2.6%), and the difference is statistically significant (P<0.05). It suggests that PCR and ELISA method may be more effective than immunofluorescence method in adenovirus detection. In the clinical work, PCR method may be more effective and accurate. The analysis of sample size showed that the result in 1000 cases, 1000-5000 cases and more than 5000 cases were 5.8%, 4.7% and 3.1%, and the result of the sample size in 1000-5000 is the most close to combined rate (4.5%), It suggests that the sample size has certain influence to research. In cross-sectional survey, large sample size may lead to heavy workload and difficult standardization and affect the survey quality, and thus it is very important to select the appropriate sample size. The adenovirus infection rate of Chinese children with respiratory diseases in the group within 1-3 year (including three years) (4.8%) are closed to combined rate (4.5%). According to the published time group, the adenovirus infection rates in 2000-2005, 2006-2010 and 2011-2018 were 3.5%, 1.4% and 4.8%, respectively. According to the data characteristics, the adenovirus has an upward trend in recent years.
The results of the meta-regression analysis showed that the test method and release time had an effect on the infection rate of adenovirus. This suggests that we should try to choose a method with high sensitivity and specificity when doing the analysis, and the early research may not be as important to the adenovirus as it is now, thus affecting the infection rate of adenovirus.
The limitation of our study is the representation of the sample size. Because the difference of medical resource in regions with uneven economic level, the bias from investigation may also affect the result of analysis.
Adenovirus is not the most common pathogen in respiratory diseases, but it will cause fatal pneumonia in younger children and often coinfect with other respiratory viruses and bacteria. Our study offered the epidemiological characteristics of adenovirus infection rate of Chinese children with respiratory diseases to provide a theoretical basis for further research on prevention and treatment in the world.
Conflict of interest statement
All authors declared that there are no conflicts of interest.
Acknowledgements
This work was supported by National Natural Science Foundation of China Grants 81673117 and 81573140.
References
Mayeur N, Srairi M, Tetu L, Guilbeau FC, Fourcade O, et al. (2012) Lethal hemorrhagic alveolitis after adenovirus pneumonia in a lung transplant recipient, Heart & lung : J Critical care 41: 401-403.View
Doan ML, Mallory GB, Kaplan SL, Dishop MK, Schecter MG et al. (2007) Heinle, O. Elidemir, Treatment of adenovirus pneumonia with cidofovir in pediatric lung transplant recipients, The Journal of heart and lung transplantation : the official publication of the International Society for Heart Transplantation 26: 883-889.View
Kim SJ, Kim K, Park SB, Hong DJ, Jhun BW, et al. (2015) Outcomes of early administration of cidofovir in nonimmunocompromised patients with severe adenovirus pneumonia, PloS one 10: e0122642.View
Sun Q, Jiang W, Chen Z, Huang L, Wang Y, et al. (2014) Epidemiology and clinical features of respiratory adenoviral infections in children, Eur J Pediatric 173: 441-444.
Kajon AE, Moseley JM, Metzgar D, Huong HS, Wadleigh A, et al. (2007) Molecular epidemiology of adenovirus type 4 infections in US military recruits in the postvaccination era (1997-2003), The J Infect Disease 196: 67-75.
Huang G, Yu D, Zhu Z, Zhao H, Wang P, et al. (2013)Outbreak of febrile respiratory illness associated with human adenovirus type 14p1 in Gansu Province, China, Influenza and other respiratory viruses 7: 1048-1054.View
Chen HL, Chiou SS, Hsiao HP (2004) Respiratory adenoviral infections in children: A study of hospitalized cases in southern Taiwan in 2001-2002[J].Trop Pediatr 50: 279-284.
Deng J, Qian Y, Zhao LQ (2010) Identification and typing of adenoviruses from pediatric patients with acute respiratory infections in Beijing from 2003 to 2008[J]. Zhonghua Er Ke Za Zhi 48: 739-743.View
Gu SJ (2015) Epidemic of children adenovirus respiratory infection in Macheng area of 2014[J]. J Clin Hematol (China) 28: 1057-1058.
Ji W, Chen ZR, Zhou WF (2013) Etiology of acute respiratory tract infection in hospitalized children in Suzhou from 2005 to 2011[J].Zhonghua Yu Fang Yi Xue Za Zhi 47: 497-503.
Li Y, Zhou W, Zhao Y (2015) Molecular typing and clinical epidemiological profileof human adenovirus infection among children with severe acute respiratory infection[J]. Zhonghua Yu Fang Yi Xue Za Zhi 49: 571-573.
Liu CY, Xiao Y, Xie ZD (2013) Viral etiology of acute respiratory tract infection among pediatric inpatients and outpatients from 2010 to 2012 in Beijing, China[J].Zhonghua Er Ke Za Zhi 51: 255-259.View
Liu T, Li Z, Zhang S (2015) Viral Etiology of acute respiratory tract infections in hospitalized children and adults in Shandong Province, China[J]. Virol J 12: 168.View
Liu TYZ, Lv X, Huang DN (2014) Epidemiological characteristic and molecular typing of respiratory adenovirus serotypes in Shenzhen in 2011-2012[J]. J Trop Med 14: 12-15.
Liu WK, Liu Q, Chen H (2014) Epidemiology of acute respiratory infections in children in Guangzhou: a three-year study[J]. PLoS One 9: e96674.View
Lu AT (2014) Analysis of respiratory adenovirus infection in Hohhot [J]. Chin J Health Lab Tec 24: 1785-1787.
Luo XJ (2006) Study on viral pathogen of acute respiratory infection in 741 children [J]. Acta Academiae Medicinae Militaris Tertiae 28: 266-269.
Sun YP, Chen Y, Song SL (2014) Analysis of adenovirus infection characteristics in180 clinical specimens from influenza-like cases [J]. Chin J Health Lab Tec 24: 2220-2222.
Xue YM (2012) The Detection and Clinical analyses of Common Viruses and Mycoplasma Pneumonia in Respiration Infection of Children in LanZhou(master), LanZhou University.
Wang ME (2011) Tiological detection and analysis on acute respiratory tract infection in children [J]. Sichuan Medical J 22: 923-924.
Wang Y (2013) The gene detection and clinical analysis of adenovirus in children with acute respiratory infection in 1329 cases (master), Jilin University.
Wu H, Deng J, Qian Y (2012) Viruses and clinical features associated with hospitalized children with acute respiratory infections in Lhasa, Tibet [J]. Zhonghua Er Ke Za Zhi 50: 740- 742.View
Yao J, Shen GS, Fan LH (2015) Analysis on common virus pathogens in 6089 hospitalized children with respiratory track infection [J]. Chin J Epidemiol 36: 664-666.
Zhang L, Xu J, Shi W. (2015) Viral pathogen spectrum analysis of respiratory tract disease in Xi’an [J]. Modern Preventive Medicine 42: 1099-1103.
Zhang Q, Su X, Gong S (2006) Comparative genomic analysis of two strains of human adenovirus type 3 is olated from children with acute respiratory infection in southern China [J]. J Gen Virol 87: 1531-1541.
Zhang RF (2011) Molecular epidemiological and clinical features of respirstory virus inchildren with acute respiratory track infection (doctorate), Lanzhou University.
Zou LR, Zhou J, Li H, Wu J (2012) Human adenovirus infection in children with acute respiratory tract disease in Guangzhou, China [J]. APMIS 120: 683-688. of children adenovirus respiratory infection in Macheng area of 2014[J]. J Clin Hematol(China) 28: 1057-1058.