
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 3 (2019), Article ID: JPHIP-134
https://doi.org/10.33790/jphip1100134Review Article
Truancy in Adolescence as a Predictor of Sexual Risk Outcomes in Young Adulthood
Maureen Muchimba
Department of Health Science, Saginaw Valley State University, University Center, USA.
Corresponding Author Details: Maureen Muchimba, Department of Health Science, Saginaw Valley State University, University Center, MI 48710, USA. E-mail: mmuchimb@svsu.edu
Received date: 24th November, 2018
Accepted date: 01st February, 2019
Published date: 05th February, 2019
Citation: Muchimba, M. (2019). Truancy in Adolescence as a Predictor of Sexual Risk Outcomes in Young Adulthood. J Pub Health Issue Pract 3: 134.
Copyright: ©2019, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Objectives: To examine the associations between truancy in adolescence and sexual risk outcomes in young adulthood.
Methods: Data were drawn from 2677 participants of the National Longitudinal Study of Adolescent to Adult Health. Assessed when participants were aged 13-18 years, truancy was categorized as no truancy, low-level truancy and high-level truancy. When participants were aged 25-31 years, age of sexual debut, number of lifetime sexual partners and having a sexually transmitted disease (STD) in the previous 12 months were assessed. Logistic regression was used to estimate the associations.
Results: Compared to non-truants, the likelihood of early sexual debut was higher among low-level truants and highest among highlevel truants. For lifetime number of sexual partners, low-level truants were more likely to have a high number of lifetime sexual partners compared to non-truants in young adulthood, while there was no relationship between high-level truancy and number of lifetime sexual partners. Low-level truants were just as likely as nontruants to report having an STD in the previous 12 months in young adulthood; however, high-level truants were more likely report having an STD in the same time period.
Conclusions: Truancy in adolescence is associated with sexual risk outcomes in adulthood. Although not a cause of risky sexual behavior, habitual truancy presents an important point of intervention and may therefore be a useful indicator for programs that aim to prevent STDs.
Introduction
Sexually transmitted diseases (STDs) are an important public health concern in the United States. According to the Centers for Disease Control and Prevention (CDC), approximately 20 million new cases of STDs occur in the United States each year [1]. Adolescents and young adults are disproportionately affected by STDs. Compared with those aged 25 and older, sexually active adolescents aged 15-19 years and young adults aged 20-24 years are at higher risk of acquiring STDs [2]. Further, even though they make up just over one quarter of the sexually active population, youth ages 15-24 account for about half of all new STD cases [3]. If left undiagnosed and untreated, STDs can have serious health consequences, including pelvic inflammatory disease, infertility, life-threatening ectopic pregnancy, stillbirth in infants [4-6]. One STD, human papillomavirus, is the primary cause of several cancers, including those of the cervix, vulva, vagina, penis, anus, and oropharynx [7]. Plus, the presence of STDs increases the likelihood of both transmitting and acquiring HIV, and increased risk for HIV transmission [8,9]. Aside from the negative health effects of these diseases, direct medical costs associated with STD diagnosis and treatment can be substantial [1]. An improved understanding of factors that contribute to STDs among young adults is important for prevention efforts.
Truancy
Truancy is a modifiable factor that has been associated with STDrelated behaviors. Generally considered as any unexcused or unverified absence from school, truancy is a serious issue that affects most school districts in the United States. For example, in 2013-14, roughly 14% of students nationwide missed 15 or more days of school [10]. Aside from impacting academic performance, truancy is of concern as it often represents unsupervised time during which health risk behaviors, such as sexual risk behavior and substance use, can occur. Research has linked truancy to problem behaviors such as substance use [11-12], juvenile delinquency [13] and adult criminal offending [14]. It has also been associated with sexual risk behavior [15].
Sexual Risk Behavior
Although there is a great deal of research on truancy and other risk behaviorssuch as substance use, there are fewer studies on truancy and sexual risk behavior. Research conducted in truant adolescent samples indicates that they report high levels of sexual risk behavior [16-17]. Findings from a sample of truant adolescents followed over 18 months revealed that they had a much higher frequency of sexual intercourse than that of the national youth population [16]. In another study of truant adolescentswho were also followed over 18 months, participants reported high rates of sexual intercourse, intercourse without using a condom, and having sex with two or more people at each follow-up time point covered by the study [17].
There have also been some cross-sectional examinationswhere outcomes intruant and non-truant adolescents were compared. In a study of 12- to 14-year-old adolescents with mental health symptoms, teens with a history of truancy were more likely than non-truant teens to report greater frequency of having ever engaged in oral, vaginal, and anal sex, and in non-intercourse sexual behaviors [15]. An investigation among high school students by Eaton, Brener and Kann [18] revealed an association between truancy and sexual risk behavior, including sexual intercourse before age 13 years and having had sexual intercourse with more than 4 persons during their life. In that study, the odds of sexual risk behavior were lowest among students who were never absent, higher among students who were absent with permission, and highest among students who were absent without permission, indicating that the probability of sexual risk behavior differs depending on the type of truancy. In studies among Pacific Island and Caribbean adolescentstruant adolescents were more likely to ever had sex, to have early sexual debut and to have multiple sexual partners [19-20].
Theoretical Underpinnings
Truancy tends to co-occur with other problem behaviors such as substance use and delinquency [21]. Some theories postulate common causes for multiple problem behaviors among youth, leading to covariation of risk behaviors, for example, Jessor’s Problem Behavior Theory [22-23]. According to this view, engaging in a form of problem behavior is a symptom of the larger “general syndrome” of deviance, such that young people who engage in a certain problem behavior(e.g., substance use) are significantly more likely to engage in other problem behaviors.This general syndrome is commonly referred to as problem behavior syndrome [22], and these behaviors are seen to reflect a general disposition towards problem behavior. From the perspective of the Problem Behavior Theory, those who tend toward truancy are more likely to engage in behaviors that are not considered typically acceptable.
Other models, rooted in routine activities theory [24], posit that periods of unstructured and unsupervised socializing with peers increase the likelihood that problem behaviors will occur [25-27]. Some authors [26] argue that in the absence of adult authority figures, adolescents are less likely to respond to pressure by social normsto behave in a prosocial manner, and if the adult absence is coupled with exposure to delinquent peers, delinquent acts are easier to carry out. When students are truant from school, they are much more likely to be unsupervised and to engage in non-prosocial behaviors.
Present Study
This study explored the relationship between truancy in adolescence and sexual risk behavior in young adulthood. It adds to the literature in two ways. First, the research on truancy and sexual risk behavior has been focused on adolescents. Less is known about outcomes in young adulthood. By investigating young adults, the present study picks up where the extant research on school-age adolescents leaves off; it extends the adolescent health literature by examining whether the sexual risk behavior outcomes of truancy observed among adolescents would be observed in young adults. The CDC reports that STD rates have been consistently highest among young adults, the highest rates being in the20–29 age group [2]. This makes young adults an important population from the STD prevention perspective. Second, there is a dearth of longitudinal studies on truancy and sexual risk behavior. As informative as cross-sectional studies are, longitudinal studies are better able to provide information about the temporal order of the events underlying the associationsbetween truancy and sexual risk behavior. A greater understanding of factors that influence sexual behavior among young adults would inform programs aimed at reducing STD-related sexual behaviors in this population, which in turn could reduce the incidence of STDs.
The question the present study sought to answer was, is truancy in adolescence associated with sexual risk behavior in young adulthood? The overarching hypothesis of the present study was that adolescents with a history of truancy would be more likely to report sexual risk outcomes in young adulthood.
Method
The present study was a secondary analysis of data from the National Longitudinal Study on Adolescent Health (Add Health) [28]. Add Health is a comprehensive, nationally representative, survey that launched in 1994 and has followed adolescents into adulthood for over two decades. Eighty U.S. high schools and their corresponding middle schools were selected with a probability proportional to size. Approximately 90,000 students in grades 7–12 completed in-school questionnaires, of which a sample of 20,475 adolescents completed a Wave I home interview. A parent, usually the resident mother, also completed a 30-minute interviewer-assisted interview at Wave I. Adolescents interviewed in Wave I were then followed up in 1996 (Wave II), 2001–2002 (Wave III), and 2007–2008 (Wave IV). A fifth wave of data collection has been underway since 2016. The Add Health survey includes data on respondents’ social, economic, psychological and physical well-being, their family, neighborhood, community, school, friendships, peer groups, and romantic relationships. It therefore provides unique opportunities to study how social environments and behaviors in adolescence are linked to health outcomes in young adulthood.
The current study’s sample comprised Add Health youth who had data for both waves II and IV and reported having been sexually active at Wave IV (n = 2677). Add Health participants provided written informed consent for participation in all aspects of Add Health in accordance with the University of North Carolina School of Public Health Institutional Review Board guidelines.
Measures
The present study included three outcomes, assessed at Wave IV
Early sexual debut. Early sexual debut was defines as engaging in sexual intercourse for the first time before the age of 16. Participants were asked, “How old were you the first time you had vaginal intercourse?” The responses weredichotomized to 0 = ≥16 years, 1= <16 years.
Lifetime multiple partners. Participants reported on the number of partners they had ever had vaginal sexual intercourse with. According to the CDC’s National Survey of Family Growth website [29], the median number of sexual partners reported by those aged 25-44 years was six for men and four for women. Based on that information, a variable was created, coded 0 = ≤6 (low number of partners), 1 = >6 (high number of partners) for males; and 0 = ≤4 (low number of partners), 1 = >4 (high number of partners) for females.
STD diagnosis in the previous 12 months. Participants were asked if, in the past year, they had been told by a doctor, nurse, or other health professional that they had no sexually transmitted diseases. Respondents selected 1 if the statement applied to them and 0 if it did not. For the present study, those who selected 1 were recoded as 0 (no STD diagnosis in the previous 12 months) and those who selected 0 as 1 (STD diagnosis in the previous 12 months).
Independent variable
Truancy was the independent variable of interest. Participants were asked how many times they had skipped school for a full day without an excuse during the school year. Responses ranged from 0 to 70 times. Responses were subsequently coded into 0 = non-truants (0 days), 1 = low-level truancy (1–3 days), 2 = high-level truancy (4+ days).
Control Variables
The following potential confounders were controlled for: gender, age, race, parental socioeconomic status (SES), participant SES, maternal connectedness, paternal connectedness,school connectedness andmarital history. Data for parental SESwere obtained from Wave I of Add Health, when it was assessed. A score was computed for SES by summing maternal education level (1= as less than high school, 2=high school graduate, 3=some college, 4=college graduate, 5=postgraduate) and annual household income (1=$0-$20,000, 2=$21,000-$40,000, 3=$41,000-$60,000, 4=$61,000-$80,000, 5=$81,000+). The resulting score had a range of 1-5. At Wave II, age, maternal connectedness, paternal connectedness and school connectedness were controlled for maternal connectedness was using a four-item score that included items asking participants how much they agreed with statements regarding their relationship with their mother, e.g., “Most of the time, your mother is warm and loving toward you.” Responses ranged from (1) strongly agree to (5) strongly disagree. The responses were reverse coded so that high values indicated high levels of connectedness. The resulting score ranged from 1 to 5. A corresponding score was created for paternal connectedness. School connectedness was ascore created from five items that asked how participants felt about their school, e.g., “You feel like you are part of your school.” Responses ranged from (1) strongly agree to (5) strongly disagree. Where appropriate, variables were recoded so that high values indicated high levels of school connectedness. The score created had a range of 1-5. At Wave IV, the variables controlled for were age, education level (less than high school, high school graduate, some college, college graduate, postgraduate) and marital history (ever married vs never married).
Statistical Analysis
Descriptive statistics were ascertained to characterize the sample. Crude associations between each outcome variable and all other variables were estimated. The associationsbetween truancy and sexual risk outcomes were estimated in terms of odds ratios (ORs) with 95% confidence intervals (CIs). Variables that were significant in the bivariate analysis were included as covariates were in logistic regression analyses. The multivariable logistic regression was checked for model fit and multicollinearity. Data were analyzed using IBM SPSS Statistics version 24.
Results
Description of the sample
Characteristics of the study participants are shown in Table 1. A little over half of the sample was female (52.8%). Participants had a mean age of 15.8 years at Wave II and 28.2 years at Wave IV. Whites, African Americans and Hispanics comprised 72.6%, 12.6% and 10.9% of the sample, respectively. American Indians or Native Americans and Asian or Pacific Islanders fell in the “other” race category. The majority of participants (43.5%) reported having some college education. About half of the participants (51.9%) had never married. About a quarter of the sample (24.7%) reported ever being truant. Just over one third of participants (34.8%) debuted early sexually. The majority (57.0%) had a high number of sexual partners, and nearly a quarter (24.4%) reported having had an STD in the previous 12 months (Table-2).
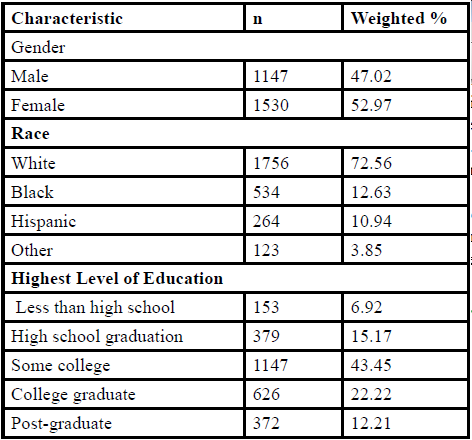
Table: 1 Characteristics of the Study Sample.
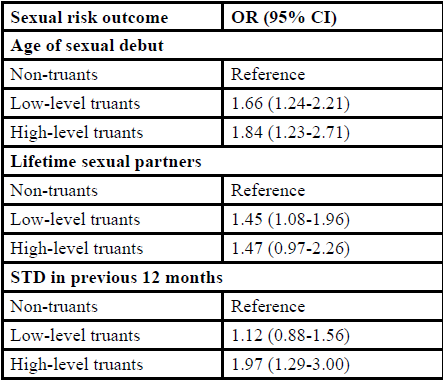
Table: 2 Relationship between Truancy and Sexual Risk Outcomes.
Associations between truancy and sexual risk behavior
Compared with non-truants, low-level truants were1.66 (95% CI = 1.24-2.21) times more likely to have early sexual debut, while highlevel truants were 1.84 (95% CI= 1.23-2.71) times more likely. For lifetime number of sexual partners, low-level truants were 1.45 (95% CI = 1.08-1.96) times more likely to have a high number of lifetime sexual partners compared to non-truants in young adulthood, while there was no relationship between high-level truancy and number of lifetime sexual partners. Low-level truants were just as likely as non-truants to report having an STD in in the previous 12 months young adulthood, however, high-level truants were 1.97 (95% CI = 1.29-3.00) times more likely report having an STD.
Discussion
This study extends the literature by longitudinally examining the relationship between truancy and sexual risk behavior. In this nationally representative sample, those who reported being truant in adolescence were more likely to engage in sexual risk behavior in young adulthood. By using a longitudinal design, the present study moved beyond correlations in adolescence and provided evidence of a temporal relationship between truancy and sexual risk behavior. The associations of truancy with early sexual debut, a high number of sexual partners and having an STD in the previous 12 months largely persisted even when pertinent confounders wereadjusted for.
The findings of the present study are consistent with cross-sectional research among adolescents, which have shown a relationship between truancy and sexual risk behavior [15,18-20]. The findings further demonstrate that the relationship between truancy and sexual risk behavior described in adolescence encompasses young adulthood. These findings suggest that adolescents who have values and behaviors that conform to conventional societal norms are less likely to engage in risk behaviors in adolescence as well as and in later life. The findings from studies among adolescents and those of the present study highlight the importance of truancy as a particularly salient predictor of sexual risk behavior in the young adulthood population.
The findings of the present study are also aligned with prior research that report a positive association between truancy and delinquency, drug use, aggression, and an overall propensity toward other risk behaviors [12]. Together, these results support the notion that health-compromising behaviors are due to a common underlying construct of unconventionality related to several personality and contextual factors [22-23,30]. They support problem behavior theory, demonstrating that truant youth, who are likely to be high on externalizing behavioral traits, are also more likely than nontruants to engage in sexual risk behaviors. They also show that the relationship between truancy and sexual risk behavior observed in adolescence would most likely also be apparent in young adulthood. Although other models propose that problem behaviors, including truancy and risky sex, are most likely to occur during periods of unstructured and unsupervised time with peers [25-27], the use of longitudinal data demonstrates that the relationship between truancy and sexual risk behavior persists in young adulthood, when most young people, those were truant and those who were not, are no longer under the supervision of adults. This demonstrates that those with a higher probability of engaging in sexual risk behaviorin adolescence would still have a higher probability of engaging in suchbehavior even when not under the supervision of parents or teachers. The follow-up assessment in the present study was 12 years after the first assessment, which strengthens this argument.
Undoubtedly, truancy is not a cause of sexual risk behavior; however, it can serve as a potential marker for future healthcompromising behaviors [31], including those that increase the risk for STDs. The findings of the present study strengthen the argument for truancy as a sound indicator of the probability of later sexual risk behavior. Adolescents who are frequently truant may comprise a population that STD prevention efforts may need to target. Collecting and examining data on absenteeism could help with aptly identifying adolescents who are at increased risk for engaging in risky sexual behavior in later adolescence or adulthood, those in need of programs aimed at reducing or preventing sexual risk behaviors.
Limitations of this study need to be considered. First, there may be issues of measurement bias if there were inaccuracies in the survey responses, particularly due to respondents answering untruthfully. Second, the third outcome variables in the present study measured STD diagnosis in the previous 12 months. Some individuals might not have had an STD in the past year, but may have had over one year prior, therefore, that information was missed. Lastly, because this study used two waves of data over the period 1996-2008, results may not be generalizable to different time periods. Despite these limitations, the study’s strengths include the use of a large national dataset with rich information about youth behavior, and the use of a longitudinal design, from which temporal relationships can be inferred. Further, this study assessed outcomes in young adolescence, providing information about sexual risk behavior outcomes beyond adolescence. Truancy in adolescence is associated with the likelihood of sexual risk behavior in young adulthood. Although it should not be understood as a cause of risky sexual behaviorin a young person’s life, habitual truancy presents an important point of intervention and may therefore be a useful indicator for programs that aim to prevent risky sexual behavior. Programs aimed at preventing STD-related behaviors among young adults could use truancy to identify adolescents who have a higher probability of engaging in risky sexual behaviors. The programs could work with schools and other relevant community programs to initiate preventive efforts before adolescents begin to engage in these behaviors.
Acknowledgement
This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. Special acknowledgment is due Ronald R. Rindfuss and Barbara Entwisle for assistance in the original design. Information on how to obtain the Add Health data files is available on the Add Health website (http://www.cpc.unc.edu/ addhealth).
Conflicts of Interest Statement
The author has not conflict of interest to declare.
References
Centers for Disease Control and Prevention. Reported STDs in the United States (2016) High burden of STDs threaten millions of Americans Fact Sheet.View
Centers for Disease Control and Prevention. (2016) Sexually transmitted disease surveillance.View
Satterwhite CL, Torrone E, Meites E, Dunne EF, Mahajan R et al. (2013) Sexually transmitted infections among US women and men: prevalence and incidence estimates, 2008. Sex Transm Dis 40: 187-193.View
Simms I, Stephenson JM (2000) Pelvic inflammatory disease epidemiology: what do we know and what do we need to know? Sex Transm Infect 76: 80-87.View
Westrom L (1980) Incidence, prevalence and trends of acute pelvic inflammatory disease and its consequences in industrialized countries. Am J Obstet Gynecol 138: 880-892.View
Liu B, Roberts CL, Clarke M, Jorm L, Hunt J et al. (2013) Chlamydia and gonorrhoea infections and the risk of adverse obstetric outcomes: a retrospective cohort study. Sex Transm Infect 89: 672-678.View
Viens LJ (2016) Human papillomavirus–associated cancers— United States, 2008–2012. MMWR Morb Mortal Wkly Rep 8: 661-666.View
Pathela P, Braunstein SL, Blank S, Schillinger JA (2013) HIV incidence among men with and those without sexually transmitted rectal infections: estimates from matching against an HIV case registry. Clin Infect Dis 57: 1203-1209.View
Peterman TA, Newman DR, Maddox L, Schmitt K, Shiver S et al. (2014) High risk for HIV following syphilis diagnosis among men in Florida, 2000-2011. Public Health Rep 129: 164-169.View
US Department of Education.Chronic absenteeism in the nation's schools.View
Dembo R, Briones-Robinson R, Barrett K, Winters KC, Schmeidler J et al. (2013) The mental health, substance use, and delinquency among truant youths in a brief intervention project: A longitudinal study. J Emot Behav Disord 21: 176-192.View
Henry KL, Thornberry TP (2010) Truancy and escalation of substance use during adolescence. J Stud Alcohol Drugs 71: 115-124.View
Vaughn MG, Maynard BR, Salas-Wright CP, Perron BE, Abdon A et al. (2013) Prevalence and correlates of truancy in the US: results from a national sample. J Adolesc 36: 767-776.View
Rocque M, Jennings WG, Piquero AR, Ozkan T, Farrington DP et al. (2017) The importance of school attendance: Findings from the Cambridge Study in Delinquent Development on the Life-Course Effects of Truancy. Crime Delinquency 63: 592- 612.View
Houck CD, Hadley W, Tolou-Shams M, Brown L (2012) Truancy is associated with sexual risk among early adolescents. J Dev Behav Pediatr 33: 728-731.
Dembo R, Wareham J, Krupa J, Winters KC (2015) Sexual Risk Behavior among Male and Female Truant Youths: Exploratory, Multi-Group Latent Class Analysis. J Alcohol Drug Depend 3: 226-239.View
Dembo R, Krupa J, Wareham J, Schmeidler J, DiClemente RJ et al. (2017) A Multigroup, Longitudinal Study of Truant Youths, Marijuana Use, Depression, and STD-Associated Sexual Risk Behavior. J Child Adolesc Subst Abuse 26: 192-204.View
Eaton DK, Brener N, Kann LK (2008) Associations of health risk behaviors with school absenteeism. Does having permission for the absence make a difference? J Sch Health 78: 223-229.View
Peltzer K, Pengpid S (2015) Early Sexual Debut and Associated Factors among In-school Adolescents in Six Caribbean Countries. West Indian Med J 64: 351-356.View
Peltzer K, Pengpid S (2016) Risk and Protective Factors Affecting Sexual Risk Behavior Among School-Aged Adolescents in Fiji, Kiribati, Samoa, and Vanuatu. Asia Pac J Public Health 28: 404-415.View
Bannink R, Broeren S, Heydelberg J, van't Klooster E, Raat H et al. (2015) Depressive symptoms and clustering of risk behaviours among adolescents and young adults attending vocational education: a cross-sectional study. BMC Public Health 15: 186-194.View
Donovan JE, Jessor R (1985) Structure of problem behavior in adolescence and young adulthood. J Consult ClinPsychol 53: 890-904.View
Jessor R (1991) Risk behavior in adolescence: a psychosocial framework for understanding and action. J Adolesc Health 12: 597-605.View
Cohen L, Felson M (1979) Social change and crime rate trends: A routine activity approach. Am Sociol Rev 44: 588-608.View
Osgood DW, Anderson AL (2004) Unstructured socializing and rates of delinquency. Criminology 42: 519-550.View
Osgood DW, Wilson JK, O’Malley PM, Bachman JG, Johnston LD et al. (1996) Routine activities and individual deviant behavior. Am Sociol Rev 61: 635-655.View
Stoolmiller M (1994) Antisocial Behavior, Delinquent Peer Association, and Unsupervised Wandering for Boys: Growth and Change from Childhood to Early Adolescence. Multivariate Behav Res 29: 263-288.
Harris KM, Halpern CT, Whitsel E, Hussey J, Tabor J et al. (2009) The National Longitudinal Study of Adolescent to Adult Health.View
National Survey of Family Growth (2017).
Le Blanc M, Bouthillier C (2003) A developmental test of the general deviance syndrome with adjudicated girls and boys using hierarchical confirmatory factor analysis. Crim Behav Ment Health 13: 81-105.View
Zhou Y, Puradiredja DI, Abel G (2016) Truancy and teenage pregnancy in English adolescent girls: can we identify those at risk? J Public Health 38: 323-329.View