
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 3 (2019), Article ID: JPHIP-138
https://doi.org/10.33790/jphip1100138Research Article
A Rapid Assessment of the Impacts of Gold Mining on Women’s Health and Quality of Life in Ashanti Region, Ghana
Baraka Muvuka*, Muriel J. Harris
1Department of Health Promotion and Behavioral Sciences, School of Public Health and Information Sciences, University of Louisville, 485 East Gray Street Louisville, Kentucky 40202, USA.
Corresponding Author Details: Baraka Muvuka, Department of Health Promotion and Behavioral Sciences, School of Public Health and Information Sciences, University of Louisville, 485 East Gray Street, Louisville, Kentucky 40202, USA. E-mail: baraka.muvuka@louisville.edu
Received date: 26th November, 2018
Accepted date: 21st March, 2019
Published date: 23rd March, 2019
Citation: Muvuka, B., & Harris, M.J. (2019). A Rapid Assessment of the Impacts of Gold Mining on Women’s Health and Quality of Life in Ashanti Region, Ghana. J Pub Health Issue Pract 3: 138.
Copyright: ©2019, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Introduction: Gold mining is crucial to economic growth and development in several countries including Ghana. It accounts for 40% of Ghana's export earnings and 5.7% of Ghana's GDP. While gold mining yields substantial economic benefits, substandard mining operations have been associated with adverse health, environmental, and social impacts. Exposures to high concentrations of toxic metals (e.g. mercury, lead, arsenic) in water, food, air, and soil have been documented among mine workers and residents of mining communities. Women and children in mining communities are particularly vulnerable; however, the impacts of mining practices on their health and quality of life remain understudied.
Methods: This study explored women's perceptions of the impacts of gold mining on their health and quality of life in a community bordering the Obuasi gold mine in Ghana. A qualitative research design was employed, consisting of in depth semi-structured interviews. Participants also completed short socio-demographic surveys. Interviews were audio-recorded, transcribed verbatim, and imported into Dedoose for analysis. Thematic analysis was conducted to group codes into conceptual themes. Descriptive statistics were generated in SPSS.
Results: A total of 15 women were interviewed, about half (53%) of whom had a primary education and were married (57%). A majority (83.3%) had children under 5 years old. Participants revealed that while the mining industry provided indirect socio-economic benefits to women, it was associated with environmental degradation, a range of health issues, lack of access to farmlands, and limited sustainable income-generating activities for women, all of which negatively impacted their quality of life. Participants provided specific recommendations to improve health and quality of life of women residing in the mining community.
Conclusions: Women in mining communities face unique social, health, and safety concerns related to mining activities. There is an urgent need for gender sensitive policies that promote environmentally and economically sustainable, centered and socially responsible mining practices that improve women’s social-economic and health status.
Key Words: Gold mining; Women’s health; Environmental degradation; Advocacy; Mining policies; Ghana
Introduction
Gold mining is vital to socio-economic development in Ghana [1], accounting for 40% of Ghana’s total export earnings and 5.7% of its gross domestic product [2,3]. Ghana ranks second in Africa and ninth globally for gold production [2,3]. Over 60% of Ghana’s gold was extracted from the Obuasi gold mine, the oldest (since 1890) and largest in Ghana [2,5] prior to temporary closure in 2014 for redevelopment purposes [6]. The hike in gold prices, coupled with growing socio-economic demands have generated a rapid expansion of artisanal and small-scale gold mining in Ghana [3,7].
Despite the economic benefits associated with gold mining, substandard mining operations in both small and large-scale gold mines have been associated with adverse health outcomes, environmental degradation, food insecurity, and socio-economic deprivation in adjacent communities [1,3,4,7,8]. Mining operations involve processes such as excavation, blasting, ore processing using chemicals, and dumping of waste materials, which collectively release toxic chemicals (e.g. mercury, lead, arsenic, iron, manganese, and cadmium) into water, soil, air, and food in surrounding communities [1,4,7,9,10]. Exposure to these chemicals is associated with an increased prevalence of chronic conditions such as cancer, cardiovascular diseases,and renal diseases [7,8]. For instance, a cross-sectional study on women (N=8790) in Mongolia found an association between exposure to lower concentrations of arsenic (20– 50 μg/L) in drinking water and increases in systolic blood pressure (1.29 mmHg; 95% CI 0.82, 1.75) [11]. Additionally, occupational (miners) and environmental (residents) exposures to mercury have been associated with early signs of kidney damage (r = 0.404, p < 0.01) [12], neurological conditions (e.g. tremors, memory issues), and immune or autoimmune conditions (e.g. allergies,thyroiditis, systemic lupus erythematosus) [13,14].
Mining communities also experience a high burden of water and vector-borne diseases [7]. Poor water and sanitation (e.g. toilets, sewage disposal) infrastructure coupled with overcrowding, have been linked with an increased incidence of diarrheal diseases such as cholera and typhoid in diverse mining communities [15-19]. Furthermore, stagnant water pools from mining processes are a suitable breeding ground for disease vectors, contributing to malaria and dengue out breaks and hyperendemicity in some mining communities in French Guiana [20], Columbia (36.1% of national malaria incidence) [21], Ghana [18], and the Democratic Republic of Congo [16], among others [15,17].
Women and children residing in mining communities are particularly vulnerable to the poor environmental, health, and social impacts of substandard gold mining [9,22]. Women are more likely to be exposed to high levels of water pollutants as they perform traditionally ascribed tasks such as water collection, food preparation, dishwashing, and laundry [9]. Prenatal heavy metal exposure has been associated with adverse pregnancy and birth outcomes. In a systematic review and meta-analysis of 23 studies, exposure to high concentrations of arsenic (≥ 50 μg/L) in groundwater was significantly associated with high risks of spontaneous abortion (OR = 1.98), stillbirths (OR = 1.77), and infant mortality (OR = 1.35), among others [23]. Furthermore, women in mining communities disproportionately experience unemployment and poverty as a result of gender discrimination in the mining sector (male-dominated) and limited access to traditional sources of livelihood such as subsistence farming due to land acquisition by mining companies [9,10,22,24-26]. Other studies have reported a high prevalence of domestic and sexual violence, commercial sex trade, and consequently, sexually transmitted infections (STIs) including HIV among women in mining communities [7,9,10,24,26,27].
Despite their vulnerability, there is a dearth of literature on the impacts of mining activities on women’s health and quality of life in these communities [7,27]. Much of the literature has focused on assessing the health of mineworkers and concentrations of heavy metals in mining communities [8]. This study explored women’s perceptions of the impacts of gold mining on their health and quality of life. Identifying the various socio-economic, environmental, and structural factors influencing women’s health in a mining community will potentially inform research, practice, and policies to protect women and residents of mining communities.
Methodology
Study Setting
The Ashanti Region is located in the middle belt of Ghana. It spans across 24, 389 square kilometers and is composed of onemetropolitan area, six municipalities, and 20 district assemblies, with a total population of 3,612 950 (2000 Census) [28,29]. While agriculture is the main source of livelihood in the Ashanti Region for 65% of the population [28,29], it is a mineral-rich region with large reserves of gold, diamond, and bauxite, among others [28]. This study was conducted in a small gold mining community [de-identified] bordering an underground mine in the Ashanti Region. This community is home to 3000 residents, 53.3% (1600) female and 26.7% (800) adult. Only 20% of the population completed high school. Twi is the main spoken language, however, 43% of individuals also speak English [30].
Study Design
An exploratory qualitative research design was utilized to examine the impacts of gold mining processes on women’s health and quality of life in this mining community. This design was best suited to capture the complex mechanisms through which gold mining impacts women’s health and quality of life in this community. Research activities were undertaken between May 27th and May 30th, 2017.
Sampling and Recruitment
Participants were recruited using convenience and snowball sampling. Recruitment occurred concurrently with data collection over three field trips to the community. The researchers contacted potential participants in-person to assess their interest in participating in the study. Those expressing an interest were screened to ensure that they met the following inclusion criteria: 1) 18 years or older, 2) community resident for at least 1 year, and 3) able to speak English or Twi.
Data Collection
Data collection consisted of short socio-demographic surveys (e.g. education, employment status, income) and semi-structured interviews with eligible women. A semi-structured interview guide (Appendix A) was developed following a review of the literature on the impacts of gold mining on community health. Women were interviewed in English or in Twi (through a translator), with each interview lasting approximately 30 minutes. The interviews covered the following topics: general community health issues; women’s health issues; health-related programs and resources in the community; and the perceived impacts of gold mining on women’s health. Participants did not receive any compensation for participation. All interviews were audio-recorded, transcribed verbatim, and imported into Dedoose™, a mixed methods data management software.
Data Analysis
SPSS 24.0 was used to generate descriptive statistics (frequencies, proportions, and measures of central tendency) summarizing participants’ socio-demographic characteristics. Interview data were analyzed in Dedoose™ using an inductive, constant comparative method. This process began with an open line-by-line coding of all interview transcripts to identify initial codes that are grounded in participants’ perceptions and experiences. Next, the initial codes were examined and combined as needed, elevated into focused codes based on frequency and salience, and re-applied to all transcripts. Using thematic analysis, focused codes were grouped into conceptual categories or themes and subthemes that portrayed recurrent patterns across the data.
Ethical Approval
This study was reviewed and approved by the University of Louisville’s Institutional Review Board [IRB number: 17.0365]. Potential participants were informed about the research study and procedures, its voluntary nature, their rights to withdraw at any time, risks and benefits, protection of confidentiality, and that interviews were to be audio-recorded. All participants provided verbal consent to be interviewed (Appendix B).
Results
Socio-demographic characteristics
A total of 15 women were interviewed. Table 1 depicts participants’ socio-demographic characteristics. Participants had a mean age of 34 years old (standard deviation=9.7 years), majority of whom were married (57%) and had a primary education (53.3%). Seven (46.7%) respondents were involved in small businesses, while four (26.7%) were unemployed. None of the women were employed in the mining sector, however, eight (60%) women had male relatives who previously or currently work in the mines.
Themes
The thematic analysis revealed six major themes reflecting women’s perceptions of the impacts of gold mining on their health and quality of life: 1) environmental issues; 2) mining-related health issues; 3) the paradox of socio-economic development; 4) under-development of mining community; 5) limited decision-making power; and 6) recommendations to address mining-related issues.
Environmental issues
The adverse environmental effects of gold mining were a prominent theme across the interviews, with all participants expressing concern over water, air, and noise pollution, as well as land degradation. Participants reported large-scale contamination of surface and ground water sources by toxic chemicals from mining processes. Many noted unusual colors and metal/chemical taste and smells in drinking water. There are two main sources of drinking water in the community– piped water supplied by the mining company and water from a borehole provided by the government. While 57% of women utilized piped water from the mining company, the majority considered it unsafe for drinking given its “reddish to brownish” coloration and an increased incidence of diarrheal diseases among women and children consuming this water.
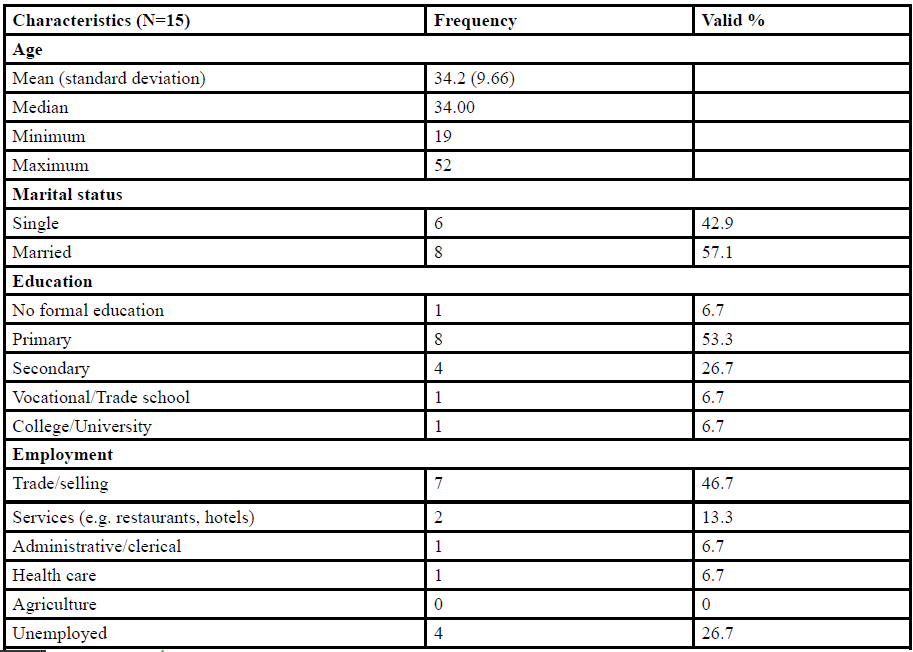
Table:1 Socio-demographic characteristics of participants.
“It [piped water from the mining company] causes sickness– When you drink it. It gives you health problems. When you go to the hospital, they tell you it is typhoid or any stomach related problems, so you can't drink it at all” (Interviewee 6).
Some participants took measures to ensure safe drinking water in their households, while a few consumed untreated water. To avoid health issues, some participants (29%) utilized water from the borehole; others purchased sachet water (water wrapped and sold in small sachets) and bottled water; while a few practiced boiling and plain sedimentation/settling.
Women also reported the presence of stagnant water pools mixed with chemicals discharged directly from the mining concession, which they perceived as being suitable breeding grounds for mosquitoes.
Poor air quality was another critical environmental concern that participantsperceived to result from a combination of smoke, dust, and toxic fumes emitted by the mining structures within their community.
“When the [mining] company was active,…due to blasting and other mining activities in times of Harmattan or the dry season, there is this sand blowing from the highlands to this side that affects breathing and the atmosphere” (Interviewee 6).
In addition, many recounted hearing loud noises coupled with ground vibrations from blasting, an explosive technique that breaks down rocks during mining processes. Participants linked noise pollution from mine blasting with hearing loss, sleep disturbances, cracks in residential structures, and fear of physical injury.
Finally, participants highlighted the issue of land degradation from mining activities in the community. Many believed that the release of toxic chemicals into the soil coupled with deforestation for mining purposes, had depleted the soil of its natural nutrients, affecting soil fertility. Land degradation has limited women’s ability to engage in subsistence and industrial farming, thus contributing to food insecurity and poverty.
Mining-related health issues
Participants highlighted an array of mining-related health issues among women and families residing in their community, including infectious diseases, dermatologic conditions, respiratory issues, and premature death. These connections were based on their observations of decreasing trends in some health issues (dermatologic and respiratory issues) since the mine closure, although several health issues persist even after mine closure.
. Infectious diseases were the most commonly reported conditions that participants attributed to gold mining. They identified malaria as a leading cause of morbidity and mortality among women and children in their community.
“At the age of 30 or 40s women die because of the chemicals women are dying early. At times they get sick and die from malaria” (Interviewee 10).
The high malaria incidence was attributed to waste and stagnant water in their community discharged from mining concessions as these attracted mosquitoes. In addition, diarrheal diseases including typhoid and cholera were reported among women and children and were linked with the consumption of unsafe water. Two participants cited HIV as an emerging public health issue in this community due to unprotected sex and increased commercial sex trade.
In addition to infectious diseases, respiratory issues such as coughs, colds, and asthma, were common among women and children and believed to be triggered by mining-induced air pollution.
“Mining activities bring about dust and fumes into the atmosphere, so most people get these serious cough problems, people who stay close to the environment, being children or being female, they get cough problems” (Interviewee 3).
Finally, participants noted the prevalence of different types of dermatologic conditions such as rashes, white patches, and black spots, which they linked with chemicals in water and air. However, some have observed a decreasing trend in skin conditions since mine closure.
“Years ago, we were having some skin rashes but now no more. When they were having some surface mining there were skin diseases” (Interviewee 12).
A few reported the lack of knowledge of health risks associated with mining processes.
The paradox of socio-economic development
This study revealed mixed findings regarding the perceived impacts of gold mining on women’s socio-economic well-being and gender discrimination in employment in the mining sector, which is maledominated. This was compounded by their limited ability to practice subsistence farming due to land degradation coupled with the loss of farmlands to the mining company.
“Gold mining has brought problems in the community, the farming lands have been fenced, so people don’t have access to their farming lands” (Interviewee 4).
Paradoxically, despite the adverse impacts associated with gold mining, all participants perceived the mining industry as being socioeconomically beneficial to women and their families. Their narratives revealed that the advent of mining operations in this community has created a shift in occupation from agricultural activities to a direct or indirect reliance on the mining sector for livelihood. The majority of women in this study benefited indirectly from mining through 1) immediate relatives employed in this sector; and 2) through enhanced business opportunities as mining operations attracted workers into the community.Consequently, the suspension of mining operations has had a heavy toll on women’s socio-economic well-being. Left with little to no alternative sources of income, poverty, unemployment, and food insecurity have become significant issues facing women in particular, and the community in general.
“When mining work was going on, people were coming and going, doing work. But when the mines closed, all activities stopped. It affected women a lot. For example, if you have a boyfriend or husband, he don’t get money to give you—that’s one factor and you can’t get any ‘petty petty’ job to do—no job (sic). When mines were still working, women used to sell clothes, food—a lot, but now if you sell, they won’t buy it—no money” (Interviewee 1).
Participants revealed that the socio-economic challenges attributed to the mine closure have also generated a range of social issues such as prostitution, high crime rates (e.g. robbery), and population displacement/out-migration in search of employment.
“So, if you see a lady, she started befriending a man to get something to eat—it is very bad. Prostitution is common in small girls—with just 5 Cedis [1.25 USD] a man can ‘eat’ [have sex with] a woman just like that on the street.All of that because of the socio-economic issues” (Interviewee 1).
Under-development of mining community
While this community hosts a lucrative mining company, participants reported the lack of basic infrastructure in their community such as health care facilities, potable water supply, and sanitation and hygiene infrastructure.For instance, the mining hospital within the community served only mine workers and their families, with the rest of the community relying on the government hospital located downtown. For many, distance and high transportation costs to the government hospital were barriers to accessing care.
“…Usually at night when there is a medical or health challenge, they usually take the people to the city centers, sometimes there is no transportation” (Interview 3).
In addition, participants noted the limited health and social services in their community, particularly reproductive and maternal health care. They did not recall any community health programs other than the mining company’s malaria and dust control activities, the government’s community outreach to deliver child health services (e.g. immunizations, essential medications), and the communityorganized communal labor/environmental clean-up. While there is a family planning clinic in the community funded by the mining company, the services are not affordable to many.
“Even this family planning is 2 Cedis [0.5 USD] but some can’t get 2 Cedis to come for family planning” (Interviewee 1).
They also expressed frustration about the poor sanitation and hygiene infrastructure, highlighting insufficient toilet facilities as a priority issue in their community.
“The main challenge is the toilet facility, the whole community has only one small facility… so then I wish the mining agents could also bring some toilet facility or something to help community members” (Interviewee 3).
Participants reported that the mining company has failed to deliver on their promises to contribute to community development.
“Some time ago the [mining] company promised to give the toilet facilities but they couldn't get a particular time or a particular place to allocate it so it hasn't been done” (Interviewee 6).
Women’s limited decision-making power
While participants identified critical issues associated with mining, they revealed two major barriers to effective advocacy and decisionmaking in their community. First, they reported the limited political representation and participation of women in community decisionmaking. None of the women interviewed were aware of any formal women’s group or association in their community. Second, they reported minimal leadership support and power differentials between the community and this mining company, where any organized efforts to speak against irresponsible mining practices had been met with threats from the mining company or affiliated stakeholders, such as threats to cut water or electricity supply.
Women’s recommendations to address mining-related issues
Participants provided several recommendations to address the critical mining-related issues identified in this study. All advocated for investments in sustainable health and hygiene infrastructure (hospitals, toilet facilities, safe water) and improved access to maternal and reproductive health services in their community. Additionally, all participants desire to see more initiatives to elevate women’s socioeconomic status. Such initiatives include education and vocational training for women, access to farmlands, micro-credits for start-up businesses, and increased employment opportunities for women in mining and other sectors.
“Concerning unemployment, when they open the mines, they should employ more women, they should do some training for women so that they can also work” (Interview 12).
Participants called for a more active involvement of government agencies such as Ghana’s Environmental Protection Agency (EPA) to mitigate the adverse environmental effects of gold mining, protect water sources, and conduct environmental inspections.
To address mining-related issues in their community, women proposed a collaborative and participatory approach that engages the government, the mining company, community leaders, and community members. Many primarily hold the mining company accountable for ensuring safe/responsible mining practices and fulfilling their promises to the community.
“The mining [company] should be concerned with the health of the people over here, so even if at least there should be regular checkups or regular screening exercises for residents to know whether they have been affected by mining activities or not so the mining industry should be also promoting health care in the community. Some time ago, they promised to do it and then now the company has collapsed” (Interviewee 5).
Participants also called on elected officials to exercise their duties as community advocates.
“It's the leaders who are supposed to come to our aid. Majority of us don’t have money to start up something. It can be the initiative of the elders or the leaders. We don’t have any strong chieftaincy system in this particular community so probably the members of parliament can advocate or speak on our behalf and you know at the government level” (Interviewee 5).
Finally, participants acknowledged the community’s role in protecting their environment through communal labor and proper waste disposal.
Discussion
This study provides insights into women’s perceptions of miningrelated health, environmental, socio-economic, and structural issues affecting their health and quality of life. Women’s narratives corroborate previous reports that women residing in mining communities are impacted through their multiple social roles as women, residents, workers, and family members [9].
Women in the present study highlighted the detrimental effects of gold mining processes on their community environment, corroborating reports of environmental degradation in other mining communities [1,7,9,10]. Hydro chemical analyses conducted in mining communities around the world have found exceedingly high levels (beyond WHO standards) of harmful metals such as arsenic, manganese, lead, and mercury in surface and groundwater [4,8]. For instance, a study in Obuasi,Ghana revealed elevated levels of arsenic and iron in groundwater, with stream water being even more polluted [4]. This evidence supports our participants’ claims of chemical contamination of drinking water sources in their community. Consistent with experiences of women in our study, residents of mining communities in other settings have had to rely on unsafe water provided by the mines, given the large-scale contamination of alternative drinking water sources in their communities [9].
The present study revealed mixed findings regarding the impacts of gold mining on women’s socio-economic well-being. Participants in this study reported limited employment opportunities for women in the mining industry, thus corroborating previous reports of maledominated mining workforces in parts of India, Indonesia, and Canada [9,22,25]. Consistent with our findings, evidence suggests that women in mining communities typically engage in service provision (e.g. restaurants, hotels, maintenance/cleaning), vocational work (e.g. tailoring), small-scale agriculture, and household tasks [3,22,25]. In many cases, these women are socio-economically disempowered and made to depend on men for income [22,25]. Interestingly, women in our study strongly perceived the mining industry as being financially beneficial to them as it increased business opportunities.
Many women in the present study expressed frustration about unemployment and poverty after the mine closure. The socioeconomic challenges experienced by women after mine closings are partly attributable to the shift in occupations brought about by the mining industry [3,25], thus the community’s economic dependence on the mining industry as reported in this study. Past studies have described this dependence on mining and the lack of sustainable livelihoods in mining communities due to the combined effects of agricultural land acquisition by mining companies, deforestation, and land degradation [3,8-10,22,24-26,31]. For instance, residents of Tarkwa mining community in Ghana have also been deprived access to their farmlands as a result of surface mining operations [8].
While the community in the present study hosts a large and lucrative mining company, women reported the lack of basic infrastructure such as potable water supply, toilet facilities, and health care facilities. Research around the world has highlighted the under development of mining communities, which are often impoverished and devoid of basic infrastructural facilities and resources [7,15-19, 25]. The lack of basic infrastructure puts a strain on women as they meet basic household needs (e.g. firewood, water) [25].The mining company has reportedly funded local initiatives, some of which include the construction of the municipal hospital, schools, and provision of water and electricity [31]. However, these limited efforts have been questioned given the under developed infrastructure and poor economic diversification in other communities in which this company operates [31].
The present study found that the compounded effects of environmental degradation, socio-economic hardships,poor sanitation and hygienein this mining community have given rise to multiple health issues among women and families [9]. Women in the present study revealed high burdens of infectious diseases, dermatologic conditions, and respiratory problems. Inadequate access to safe water and sanitation facilities in other mining communities have largely contributed to the spread of water and vector-borne diseases, to which women and children are particularly susceptible [7,9,15-19,20,21,25]. The high prevalence of dermatologic conditions described by women in the present study could be due to their exposure to heavy metals in water as they perform household tasks such as water collection, dishwashing, and laundry [9].In addition, our findings corroborate previous reports that the under employment of women in mining communities increases commercial sex work, thus the risk for HIV and other STIs [7,9,10,24,26,27].
Conclusions
This study highlights women’s perceptions of the impacts of gold mining on their health and quality of life. Overall, women perceived gold mining processes as being detrimental to their health and community environment. While the mining industry provided indirect socio-economic benefits to women, there was limited economic diversification, leaving many with no alternative sources of income after the mines closed. Women in this study experienced financial hardships, limited access to agricultural lands, lack of access to basic infrastructure, as well as an added burden of disease.Improving women’s health and quality of life in mining communities ultimately requires enforcing responsible and sustainable mining policies, while empowering women through sustainable employment opportunities, education, and political representation. Given the multifactorial nature of issues experienced by women in this mining community, there is a need for collaborative efforts involving the government, the mining company, policy makers, community leaders, and women themselves.
Practice, Research, and Policy Implications
This study has revealed issues of environmental and social injustice with important implications for public health practice, research, and policy. Women’s recommendations should be taken into consideration when addressing the issues identified in this study. More stringent policies and enforcement mechanisms are needed at the local, national, regional, and global levels to promote responsible, sustainable, and environmentally friendly mining practices. For instance, comprehensive environmental, social, health, and gender impact assessments should be required to examine the potential impacts of mining operations on the community in general and on women in particular. Ghana’s EPA should conduct regular inspections in mining communities, drawing from both quantitative studies (monitoring levels of chemicals in water, air, and soil) and qualitative input from community members. In addition, mining companies should be required to implement and periodically report social/community development projects. Similarly, the government should increase its involvement in the mining community to meet their public health and health care needs, with a focus on addressing gaps in health service delivery for women. To ensure accountability, it is important to educate the community and women about the adverse impacts of mining, existing policies, and appropriate mechanisms for reporting adverse effects. Lastly, there is a need for an equitable representation or involvement of women in decision-making about gold mining operations and other community issues.
Limitations
This study had several limitations. Findings do not represent perspectives of all women in this community given the study design and the sampling methods used (convenience and snowball). Future studies may corroborate these findings in larger and more diverse samples, using other research designs such as quantitative and mixed methods. It is important that perspectives of local health care providers and public health professionals are captured in subsequent investigations, considering their expertise and experiences serving residents.
Acknowledgements
The authors received travel funding from the Roberson Fund for African Studies, University of Louisville Graduate Student Council, and various donors through the University of Louisville School of Public Health and Information Sciences. We also acknowledge our partners at Kwame Nkrumah University of Science and Technology [KNUST] School of Public Health, KNUST Department of Theoretical andApplied Biology, KNUST Rotaract Club, as well as the community leadership and residents for their support during data collection, analysis, and dissemination.
Conflict of Interest Statement
The authors declare no competing interests.
References
Obiri S, Dodoo DK, Armah FA, Essumang DK, Cobbina SJ et al. (2010) Evaluation of lead and mercury neurotoxic health risk by resident children in the Obuasi Municipality, Ghana. Environ Toxicol Pharmacol 29: 209–212.
Mensah AK, Mahiri IO, Owusu O, Mireku OD, Wireko I et al. (2015) Environmental impacts of mining: A study of mining communities in Ghana. Applied Ecology and Environmental Sciences 3:81-94.View
Tschakert P, Singha K (2007) Contaminated identities: Mercury and marginalization in Ghana’s artisanal mining sector. Geoforum 38: 1304–1321.View
Akabzaa TM, Banoeng-Yakubo BK, Seyire JS (2007) Impact of mining activities on water resources in the vicinity of the Obuasi mine. West Afr J Appl Ecol 11: 23–34.View
Obuasi Municipal Assembly (2014) The composite budget of the Obuasi Municipal Assembly for the fiscal year 2014.
AngloGold Ashanti Limited. About Obuasi: History of Obuasi.
Basu N, Clarke E, Green A, Calys-Tagoe B, Chan L et al. (2015) Integrated assessment of artisanal and small-scale gold mining in Ghana—Part 1: Human health review. Int J Environ Res and Public Health 12: 5143-5176.View
Obiri S, Mattah PAD, Mattah MM, Armah FA, Osae S et al. (2016) Assessing the environmental and socio-economic impacts of artisanal gold mining on the livelihoods of communities in the Tarkwa Nsuaem municipality in Ghana. Int J Environ Res and Public Health 13: 160.View
Kuyek JN (2003) Overburdened: Understanding the impacts of mineral extraction on women's health in mining communities. Can Woman Stud 23: 121.View
Mwakumanya MA, Maghenda M, Juma H (2016) Socioeconomic and environmental impact of mining on women in Kasigau mining zone in Taita Taveta County. J Sustain Min. 15: 197-204.View
Kwok RK, Mendola P, Liu ZY, Savitz DA, Heiss G, et al. (2007) Drinking water arsenic exposure and blood pressure in healthy women of reproductive age in Inner Mongolia, China. Toxicol Appl Pharmacol 222: 337–43.View
Tian L, Guo HF, Gao A, Lu XT, Li QY et al. (2009) Effects of mercury released from gold extraction by amalgamation on renal function and environment in Shanxi, China.Bull Environ ContamToxicol 83: 71-4.View
Gibb H, O'Leary KG (2014) Mercury exposure and health impacts among individuals in the artisanal and small-scale gold mining community: a comprehensive review. Environ Health Perspect 122: 667-72.View
Rice KM, Walker EM, Wu M, Gillette C, Blough ER et al. (2014) Environmental mercury and its toxic effects. J Prev Med Public Health 47: 74-83.View
World Health Organization ( 2016) Environmental and occupational health hazards associated with artisanal and smallscale gold mining.View
World Bank (2015) Resources and resourcefulness: gender, conflict, and artisanal mining communities in Eastern Democratic Republic of the Congo (English). Washington, D.C.: World Bank Group.View
Hinton J (2005) Communities and small scale mining: An integrated review for development planning.View
Yakovleva, N (2007) Perspectives on female participation in artisanal and small-scale mining: A case study of Birim North District of Ghana. Resour Policy 32: 29–41.View
Renne E, Basu N, Gager E, Koomson E, Lee B et al. (2011) Women’s work, health and the environment in a small-scale mining site in northeastern Ghana. Women Environ 2: 13–16.
Pommier de Santi V, Dia A, Adde A, Georges H, Julien G, et al. (2016) Malaria in French Guiana linked to illegal gold mining. Emerg Infect Dis 22: 344-6.View
Castellanos A, Chaparro-Narváez P, Morales-Plaza CD, Alzate A, Padilla J et al. (2016) Malaria in gold-mining areas in Colombia. Mem Inst Oswaldo Cruz 111: 59-66.View
Lahiri-Dutt K, Mahy Petra (2007) Impacts of mining on women and youth in Indonesia: Two mining locations.View
Quansah R, Armah FA, Essumang DK, Luginaah I, Clarke E et al. (2015) Association of arsenic with adverse pregnancy outcomes/infant mortality: A systematic review and metaanalysis. Environ Health Perspect 123: 412-21.View
Shandro JA, Veiga MM, Shoveller J, Scoble M, Koehoorn M et al. (2011) Perspectives on community health issues and the mining boom – bust cycle. Resour Policy 36: 178-186.View
D’Souza MS, Karkada SN, Somayaji G, Venkatesaperumal R (2013) Women’s well-being and reproductive health in Indian mining community: need for empowerment. Reprod Health 10: 24.View
Vélez-Torres I, Vanegas DC, McLamore ES, Hurtado D (2018) Mercury pollution and artisanal gold mining in Alto Cauca, Colombia: Woman’s perception of health and environmental impacts. J Environ Dev 27: 415-444.View
D'Souza MS, Somayaji G, SubrahmanyaNairy K (2011) Determinants of reproductive health and related quality of life among Indian women in mining communities. J Adv Nurs 67: 1963-75.View
Republic of Ghana Ministry of Food and Agriculture. Ashanti Region.
Government of Ghana. Ashanti Region.
Unpublished report from the community secretary, May 27, 2017.
Asuah AY, Anokye PA (2016) The resilience of mining communities in Obuasi, as Anglogold Ashanti shifts position. J Poverty, Investment and Development 22.