
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 2 (2018), Article ID: JPHIP-144
https://doi.org/10.33790/jphip1100144Research Article
Factors associated with Breast Cancer Screening among Women in the United States
Shaminul Hoque Shakib1*, Joseph Inungu2, Shayesteh Jahanfar2
1School of Health Sciences, Central Michigan University, MI, 48858, USA.
2School of Health Sciences, Central Michigan University, MI, 48858, Health Professionals 2209, USA.
Corresponding Author Details: : Shaminul Hoque Shakib, Master of Public Health, Central Michigan University, MI, 48858, USA. E-mail: Shaki1sh@cmich.edu
Received date: 08th July, 2019
Accepted date: 19th August, 2019
Published date: 22nd August, 2019
Citation: Shakib SH, Inungu J, Jahanfar S (2019) Factors associated with Breast Cancer Screening among Women in the United States. J Pub Health Issue Pract 3: 144.
Copyright: ©2019, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Background: Cancer is a major public health concern around the globe. It is the second leading cause of mortality in the United States. According to the American Cancer Society, breast cancer incidence rates for 2011-2015 was 124.7 per 100,000, placing breast cancer incidence rates at the top of the list. Breast cancer mortality rates for 2012-2016 was 20.9 people per 100,000, placing breast cancer mortality rates after Lung and bronchus cancer. Healthy People 2020 states that breast cancer is highly detectable in early stages through breast screening using mammography. Despite an increased in screening and a 10% improvement in breast cancer death rates, breast cancer remains the focus of public health prevention in the US.
Objective: To identified factors which are associated with breast cancer screening: mammography among women in the United States.
Methods: We analyzed logistic regression models using data from the 2015 National Health Interview Survey (NHIS) to evaluate factors which are associated with mammography screening among women in the United States.
Results: The most important result from the study was the association between health insurance and access to mammography screening. Women without health insurance are less likely to access mammography screening compared to women with health insurance. African American woman had slightly higher rate of recent mammogram compared to non-Hispanic White women. Women aged 51-64 reported more recent mammogram compared to women aged 40-50. Women from southern region of United States reported less recent mammogram compared to rest of the United States. Non-smokers were more likely to access mammography screening compared to smokers. Women with education attainment of bachelor's degree or higher were more likely to access mammography screening compared to women with high-school degree or less.
Conclusion: The study indicated the importance of health insurance and education attainment for the access to mammography screening. The results urge researchers and public health officials to promote health education at secondary educational institutions such as highschool because it can increase women's understanding of health messages which may result in positive health behavior. The study highlights the importance of health insurance for ensuring positive healthy behaviors such as screening.
Introduction
Cancer is a major public health concern around the globe. It is the second leading cause of mortality in the United States [1]. Although the 2018 report by the Cancer Statistics Center showed a 1.5% decline in the cancer rates for both men and women from 2006-2015, it is still estimated that in 2018 a total of 1,735,350 new cancer cases and 609,640 deaths from cancer occurred in the US [1]. Unfortunately, considering the past trend of cancer screening, much of these cases will occur in individuals from non- Hispanic black backgrounds compared to non-Hispanic whites. In 2015, the death rate from cancer was 14% higher in non-Hispanic blacks than non-Hispanic whites [1]. While cancers such as cervical cancer can be prevented by vaccination and has been at the low end among cancer incidence and death rates for the past few years, breast cancer, which is also preventable with early detection and timely screening, remains the leading type of cancer among women. According to the American Cancer Society, breast cancer incidence rates for 2011- 2015 was 124.7 per 100,000, placing breast cancer incidence rates at the top of the list [2]. Breast cancer mortality rates for 2012-2016 was 20.9 people per 100,000, placing breast cancer mortality rates after Lung and bronchus cancer [2].
According to Healthy People 2020, breast cancer is highly detectable in early stages through breast screening using mammography. Despite an increased in screening and a 10% improvement in breast cancer death rates, breast cancer remains the focus of public health prevention in the US. One of the objectives of the Healthy People 2020 is to reduce the female breast cancer death rate, reduce latestage female breast cancer, and increase the proportion of women who receive breast cancer screening based on the most recent guidelines [3]. Because of the effectiveness of breast cancer screening to detect this cancer early and save the life of many women, it is critical to identify factors associated with breast cancer screening among women. A good understanding of these factors will inform the development of effective interventions to increase the uptake of the breast cancer screening among non-Hispanic black women.
Methods
Data Source and Study Population
The 2015 National Health Interview Survey (NHIS) data was analyzed. The NHIS is one of the major data collection programs on the health of the civilian noninstitutionalized population of the U.S. The NHIS is operated and conducted by the National Center for Health Statistics (NCHS), which is part of the Centers for Disease Control and Prevention(CDC) [22]. Estimates on health indicators, health care utilization and access, and health-related behaviors can be obtained through the NHIS survey data. NHIS used a complex sampling design involving stratification, clustering, and multistage sampling. For each household, a family member was interviewed face to face each week throughout the year. To increase precision of the estimates, the NHIS survey design oversampled Black persons, Hispanic persons, and Asian persons [22]. This study analyzed data from the adult prevention supplement to the NHIS [22].
Sampling Methods
A subset of the NHIS data was selected for this study. The study was restricted to female respondents aged 40 to 64 years old. Mammogram recommendations for cancer screening guidelines as a part of routine preventive care begins at the age of 40 [23]. Therefore, the study focused on women aged 40 to 64 years who are particularly at risk of breast cancer. This resulted in a total sample of 12713 individuals. Women aged 65 years or older were excluded due to the differences in insurance coverage that occurs between the age group of 65 or older and younger than 65 years (i.e., the possibility of having Medicare coverage among 65 or old). Due to the insignificant sample size of other races such as Native American and Alaska Natives, Asian and etc., only Non-Hispanic White and Black/African Americans were included for the study.
Outcome Variables
Recent mammography, the outcome for the study, was defined as having had a mammogram within the 2 years preceding the interview. The comparison group consisted of women who never had a mammogram screening in their lifetime or reported having had a mammogram before the last 2 years.
Independent Variables
The following independent variables or predictors of recent mammogram screening was included for analysis: age (40-50, 51- 64), race (White, Black/African American), income (less than, greater than, or equal to 200% of the federal poverty threshold), education attainment (high school graduate or equivalent, Bachelor’s degree or higher), marital status (married or not married), health insurance coverage (private/other insurance, Medicaid, or no insurance coverage), self-reported health status (excellent/very good/ good or fair/poor), cigarette smoking (current smoker or former/ never) and region (Northeast, Midwest, South, West).
Analysis
Descriptive analyses were carried out to examine the respondents’ demographic characteristics. A bivariate analysis was conducted to assess the association between independent variables and the outcome of interest. A Chi-Square test with a significance level of 5% (P<0.05) was performed between dependent variable and independent variables. Variables found to be significantly associated with the outcome of interest were entered into the Univariate Regression model. Multivariate logistic regression models were run to assess the independent association between these independent variables and the outcome of interest (mammogram screening). Another logistic regression model including all the independent variables regardless of their significance from the Chi-Square analysis was run. The Hosmer and Lemeshow test was used to assess the models goodness of fit. The Logistic regression model with all the variables had a higher goodness of fit. All these analyses were conducted using SPSS version 25. For the multivariate logistic model, odds ratios (OR) and their 95% confidence intervals (CIs) were used to identify significant variables.
Results
Participant characteristics
Overall, a total of 2407 women aged 40 to 64 years old were selected for this study. Table 1 summarizes their sociodemographic characteristics. Most respondents were white (83.2%). 52.31% (1259) of the respondents consisted of the age group 51-64. About 69.6% (n=1673) of the respondents had a high school/Technical degree level of education. About 1293 respondents (53.9%) were not married, and 1940 (80.6%) perceived themselves to be in excellent health status. An estimated 522 (21.7%) respondents out of 2407 reported having had a mammogram test in the past 2 years. 420 White women (80.4%) and 102 African (19.5%) reported to have had a recent mammogram. African American women seem to have undergone more recent mammogram test when compared to White women.
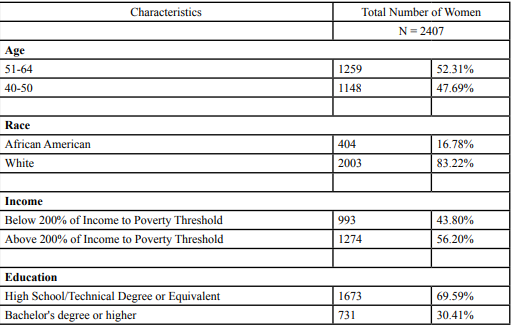
Table: 1 Socio-demographic characteristics of sample population
Tables 2 summarizes the results of the unadjusted analysis between the history of recent mammography and the independent variables.
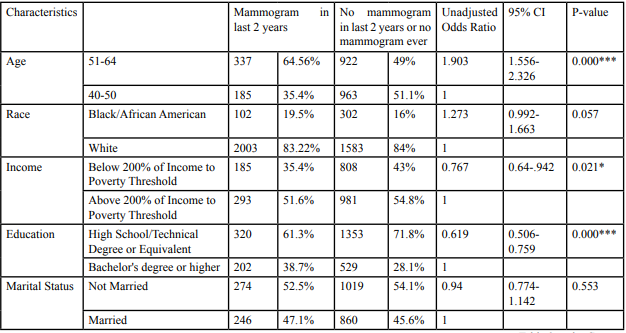
Table: 2 Unadjusted odds ratio of having Mammogram test performed in last 2 years among *p<0.05 **p<0.01 ***P<0.001.
Women with the age group 51-64 were significantly more likely to report having had a mammogram test compared to women with the age group 40-50 [OR: 1.903; 95% (CI): 1.556- 2.326]. Compared to White women, Black women were more likely to report having had a mammogram test, but the difference was not statistically significant [OR: 1.273; 95% (CI): 0.992-1.663]. Participants who reported income below 200% of income to poverty threshold [0R:0.76; [95% (CI):0.54-0.94]. Participants with a High school/ Technical degree or equivalent were significantly less likely to report having had a mammogram test compared with those with a bachelor’s degree or higher [OR:0.61; 95%CI: 0.51-0.76]. Respondents who have no health insurance coverage [OR:0.194; 95%CI 0.107-0.352], use Medicaid [OR:0.58; 95%CI: 0.53- 0.87], and who are former smokers or never smoked [OR:1.8; 95%CI: 1.43- 2.38] were significantly likely to report having had a mammogram test compared to their counterparts.
Table 3 shows the association between recent mammography for breast cancer and selected independent variable after controlling for the others. P-value and 95% confidence intervals were used to assess the level of significance.
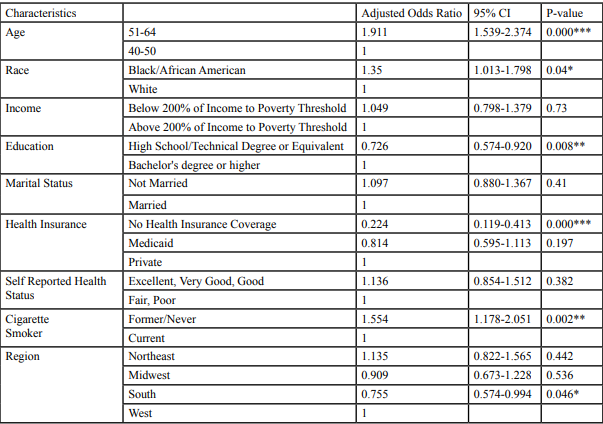
Table: 3 Adjusted odds ratio of having Mammogram test performed in last 2 years among, *p<0.05 **p<0.01 ***P<0.001.
After controlling for the other independent variables, having health insurance was strongly associated with the history of having had a recent mammography. Women who reported of having No Health Insurance Coverage were less likely to have reported a recent mammogram test compared to women who had private health insurance [OR:0.224; 95%CI: 0.11-0.41].
Women with a high school/technical degree level of education were less likely to have reported a recent mammogram compared to women who have a bachelor’s degree or higher [OR:0.72; 95%CI: 0.57-0.92]. In addition, women who formerly or never smoked were more likely to have reported a recent mammogram than women who smoke [OR:1.55; 95%CI: 1.17-2.05]. Women consisting from the age group 51-64 were more likely to have had a recent mammography compared to women from the age group 40-50 [OR:1.991; 95%CI: 1.539-2.374]. African American women were more likely to have had a recent mammography compared to White woman [OR:1.35; 95%CI: 1.013-1.798]. Woman living in the South were less likely to have had a recent mammography compared to woman from the West for region [OR:0.75; 95%CI: 0.57-0.99]. Income and selfreported health status and marital health status were not significantly associated with the outcome of interest.
Discussion
The purpose of this study was to assess factors associated with recent mammography among eligible women in the United States. Breast cancer is highly detectable in early stages through breast screening using mammography.
Nearly 22% of the women aged 40-64 in the sample reported having had a mammogram in the past 2 years. African American women had a slightly higher rate of recent mammography (25.2%) over NonHispanic White women (21%). The difference for mammography screening among both races was supported by a previous study [24]. Our study supports the finding as well. Our findings indicate that Non-Hispanic White women are less likely to access mammogram screening compared to African Americans. An additional explanation to the different rates of mammography screening among the races could be that Medicaid (23%) recipients from the study participants were significantly higher compared to the participants with no health insurance (8%) in the sample. Therefore, the difference could have resulted from the efforts of breast cancer screening programs which are targeted towards low-income women, especially Medicaid recipients [25]. 64.56% of the women aged 51-64 reported recent mammography which was much higher compared to the group of women aged 40-50 who reported only 35.4% recent mammography. A previous study conducted by [26] found that African American woman aged 51 or more were more adherent to mammography screening compared to African American women aged 50 or less. Another study by [5] found that as age increases among woman, there seems to be a decline in breast and cervical cancer screening and increase in morbidity/mortality from the cancer. Both of the findings do not support our finding for age. Only 16.78% of our respondent were African American. In addition to that, we found that women aged 51-64 were more likely to report a recent mammography compared to women who are aged 40-50. This finding does raise a concern. The American Cancer society recommends annual mammography screening for women who are aged 45-54 [4]. This finding can help health practitioners to emphasize on the necessity of mammography screening to women aged 40-50.
Region was a key indicator in our study for recent mammography. 36.98% of the women in our sample was from southern region of the U.S. 63.02% accounted for West, Midwest and Northeast being the rest of the sample. A previous study done by [4] found that women from states located in the south had higher breast cancer incident rate compared to women from the rest of the U.S.. We found that women from the southern region in the U.S were less likely to report a recent mammogram compared to the other regions. Mammograms have the potential to detect early stages of breast cancer. Therefore, the less access to mammogram as a form of screening should result in a higher incident rate. Although, further studies evaluating the stage of the breast cancer incidence and usage of mammogram in the southern region of the U.S could explain the contradictory finding.
Smoking was also an important finding for our study. There was a strong association between being a former smoker/nonsmoker and accessing recent mammogram by the women in our study. [5] found similar results in their study, where nonsmokers were more prone to undergo Breast and Cervical Cancer Screening behaviors. This persistent positive association between non-smokers and openness to health screening can help practitioners identify those patients who are more likely to receive screening.
Two underlying indicators in our study which evaluate the relationship between socioeconomic status and recent mammogram were income and education. While there seemed to be no significant association between income and recent mammograms from our results, the relationship between education and recent mammogram exhibited otherwise. Our study found that women who have a high school degree or equivalent are less likely to report recent mammogram compared to their counterparts, women with a bachelor’s or higher degree. A study by [5] found that higher levels of education correlates with positive health behavior such as screening among individuals. In addition to that, [4] found that lower levels of education attainment are associated with lower breast cancer survival. These results emphasize the significance of education on the likeliness of women having a mammogram as a form of preventative care. Therefore, more public health interventions tailored to communicate the importance of mammography screening are needed for women with lower levels of education.
The most important predictor in our study for recent mammograms among Non-Hispanic White and African American women was access to health insurance. Our results indicated that there was a negative association between women with no health insurance and recent mammograms when compared to women with health insurance in the sample. This finding was supported a previous research by [7] who found that health insurance provides better rate of survival among both Non-Hispanic White women and African American women when not adjusted for clinical and sociodemographic factor.
Previous studies have suggested that women with higher socioeconomic status and health insurance coverage are more likely to seek out preventative care, including breast and cervical cancer screening [27,28]. While income is an important component, socioeconomic status didn’t hold true for our results. Findings for education and health insurance in relation to recent mammograms seem to relate with previous studies. National data mirrors our findings that women with higher education and health insurance are more likely to undergo mammogram screening.
Limitations
This study has several strengths mainly resulting from the large national probability sample of women which contributes to generalizability of the findings. In addition to that, the sample contained a sufficiently large number of African American women which allowed us to factor in the problems that might be associated to the race-based communities. However, this study has several limitations. Since the survey is self-reported, there is potential for recall bias. Johnson et al. [29] have suggested that self-reported data may overestimate the prevalence of cancer screening. Also, another limitation to using self-reported survey is social desirability bias. Women might feel under pressure to report negative for recent mammogram due to social stigma around the importance for breast cancer screening for the aged group of 40-64.
Conclusion
Breast cancer is problematic among both White and African American women. Mammograms are a part of preventive care and are effective for detecting breast cancer at early stage. This study indicated the importance of health insurance and education attainment for the access to mammography screening. The results urge researchers and public health officials to promote health education at lower level educational institutions such as high schools because it can promote women’s understanding of health messages, resulting in positive health behavior. In addition, the study shed light on the importance of health insurance for ensuring positive healthy behaviors such as screening.
Recommendation
For future studies and research, it will be important to evaluate and develop breast screening programs targeted for women aged 40-50 from low socioeconomic communities with limited access to proper education and health insurance. In addition, more screening programs geared towards early stages are needed throughout the nation. Programs to prevent breast cancers need to take into account the culture of the neighborhood and all the underlying socioeconomic factors associated with low socioeconomic conditions.
Conflict of interest
The authors declare no conflict of interest.
References
Siegel RL, Miller KD, Jemal A (2018) Cancer statistics, 2018. CA: A Cancer J Clini 68: 7-30.View
American Cancer Society (2019) Cancer Facts & Statistics.
Healthy People 2020: An Opportunity to Address Societal Determinants of Health in the United States (2018).
Desantis CE, Fedewa SA, Goding SA, Kramer JL, Smith RA, et al. (2016). Breast cancer statistics, 2015: Convergence of incidence rates between black and white women. CA: A Cancer J Clini 66: 31-42.View
Welch C, Miller CW, James NT (2008) Sociodemographic and Health-Related Determinants of Breast and Cervical Cancer Screening Behavior, 2005. J Obstet Gynecol Neonatal Nurs 37: 51-57.View
Desantis CE, Siegel RL, Sauer AG, Miller KD, Fedewa SA, et al. (2016) Cancer statistics for African Americans, 2016: Progress and opportunities in reducing racial disparities. CA: A Cancer J for Clini 66: 290-308. View
Komenaka IK, Martinez ME, Pennington RE, Hsu CH, Clare SE, et al. (2010) Race and ethnicity and breast cancer outcomes in an underinsured population.(Author abstract)(Report). J National Cancer Institute 102: 1178.View
Williams DR, Mohammed SA, Leavell J, Collins C (2010) Race, socioeconomic status, and health: Complexities, ongoing challenges, and research opportunities. Annals of the New York Academy of Sciences 11861: 69-101.View
Williams DR, Mohammed SA, Shields AE (2016) Understanding and effectively addressing breast cancer in African American women: Unpacking the social context 122: 2138-2149.View
Dunn B, Agurs-Collins T, Browne D, Lubet R, Johnson K et al. (2010) Health disparities in breast cancer: biology meets socioeconomic status. Breast Cancer Res Treatment, 121: 281- 292.View
Geronimus AT, Hicken M, Keene D, Bound J (2006) "Weathering" and age patterns of allostatic load scores among blacks and whites in the United States. Am J Pub Health 96: 826. View
Palmer JR, Boggs DA, Wise LA, Adams-Campbell LL, Rosenberg L (2012) Individual and Neighborhood Socioeconomic Status in Relation to Breast Cancer Incidence in African-American Women. Am J Epidemiol 176: 1141-1146. View
. Lee JM, Appugliese D, Kaciroti N, Corwyn RF, Bradley RH, et al. (2007) Weight status in young girls and the onset of puberty. Pediatrics 119: e624.View
Mervish NA, Gardiner EW, Galvez MP, Kushi LH, Windham GC, et al. (2013) Dietary flavonol intake is associated with age of puberty in a longitudinal cohort of girls. Nutri Res 33: 534-542.View
Walvoord EC (2010) The Timing of Puberty: Is It Changing? Does It Matter? J Adolescent Health 47: 433-439.View
. Behie AM, Donnell MH (2015) Prenatal smoking and age at menarche: influence of the prenatal environment on the timing of puberty. Human Reproduction 30: 957-962.View
Deardorff J, Fyfe M, Ekwaru JP, Kushi LH, Greenspan LC (2012) Does neighborhood environment influence girls' pubertal onset? findings from a cohort study. BMC pediatrics 12: 27. View
Sarkissyan M, Wu Y, Vadgama JV (2011) Obesity is associated with breast cancer in African American women but not Hispanic women in South Los Angeles. Cancer, 117: 3814-3823.View
Sexton KR, Franzini L, Day RS, Brewster A, Vernon SW, et al. (2011) A review of body size and breast cancer risk in Hispanic and African American women 117: 5271-5281. View
Bittoni MA, Wexler R, Spees CK, Clinton SK, Taylor CA, et al. (2015) Lack of private health insurance is associated with higher mortality from cancer and other chronic diseases, poor diet quality, and inflammatory biomarkers in the United States. Preven Med 81: 420-426.View
Liu Y, Colditz GA, Rosner B, Berkey CS, Collins LC, et al. (2013) Alcohol intake between menarche and first pregnancy: a prospective study of breast cancer risk. J National Cancer Institute 105: 1571.View
National Center for Health Statistics. Survey Description, National Health Interview Survey (2015).View
Oeffinger KC, Fontham ETH, Etzioni R, Herzig A, Michaelson JS, (2015) Breast Cancer Screening for Women at Average Risk: 2015 Guideline Update From the American Cancer Society. JAMA 314: 1599-1614.View
Selvin E, Brett KM (2003) Breast and cervical cancer screening: sociodemographic predictors among White, Black, and Hispanic women.(Abstract). Am J Pub Health 93: 618. View
Lawson HW, Henson R, Bobo JK, Kaeser MK (2000). Implementing recommendations for the early detection of breast and cervical cancer among low-income women. MMWR. Recommendations and reports : Morbidity and mortality weekly report. Recommendations and reports 49: 37. View
Halbert CH, Kessler L, Wileyto EP, Weathers B, Stopfer J, et al. (2006) Breast cancer screening behaviors among African American women with a strong family history of breast cancer. Preven Med 43: 385-388.
Katz S, Zemencuk J, Hofer T (2000) Breast cancer screening in the United States and Canada, 1994: socioeconomic gradients persist. Am J Pub Health 90: 799-803.View
Makuc DM, Freid VM, Parsons PE (1994) Health insurance and cancer screening among women. Advance data(254), 1.
Johnson CS, Archer J, Camposoutcalt D (1995) Accuracy of Pap smear and mammogram self-reports in a southwestern Native American tribe. Am J Preven Med 11: 360-363.