
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 3 (2019), Article ID: JPHIP-155
https://doi.org/10.33790/jphip1100155Review Article
Policies and Practices Affecting Adolescent Sexual Health in Mississippi
Joyee L. E. Washington, MS, MPH1*, Susan Hrostowski, PhD2 , Amy Arrington, JD3 , Olivia Ismail, LMSW4 , Morgan W. Bradwell, LMSW5 , Selena Frederick, MPH6 Jerome R. Kolbo, PhD7
1School of Education, The University of Southern Mississippi, 118 College Drive, Hattiesburg, MS, 39406; USA.
2,4,5,7School of Social Work, The University of Southern Mississippi, 118 College Drive, Hattiesburg, MS, 39406, USA.
3,6Department of Public Health, The University of Southern Mississippi, 118 College Drive, Hattiesburg, MS, 39406, USA.
Corresponding Author Details: Joyee L. E. Washington, School of Education, The University of Southern Mississippi, 118 College Drive, Hattiesburg, MS, 39406; USA. E-mail: Joyee.Esters@usm.edu
Received date: 26th November, 2019
Accepted date: 26th December, 2019
Published date: 30th December, 2019
Citation: Washington, J.L.E., Hrostowski, S., Arrington, A., Ismail, O., Bradwell, M.W., Frederick, S., & Kolbo, J.R. (2019). Policies and Practices Affecting Adolescent Sexual Health in Mississippi. J Pub Health Issue Pract 3(2):155.
Copyright: ©2019, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
The purpose of this study was to examine policies and practices that affect the sexual health of adolescents in Forrest County, a southeast Mississippi community. Community members participating in a series of community conversations shared perspectives on needs and problems related to adolescent sexual health; policies and practices affecting adolescent sexual health; and their own roles in, and contributions toward, improving adolescent sexual health. Qualitative analysis of conversations yielded five overarching themes related directly to: education, health, environment, communication, and parental involvement. Community members expressed a strong desire to improve adolescent sexual health by offering specific recommendations and action plans.
Key words: Adolescent, Sexual Health, Policies, Practices
Policies and Practices Affecting Adolescent Sexual Health in Mississippi
Public health challenges related to sexual health are among the most significant public health issues facing the United States, with adolescents recognized as a population group with disparately high rates of negative sexual health outcomes [1]. Nationally, the United States is experiencing alarming rates of sexually transmitted infections, teen and unintended pregnancy, and sexual violence.2 Recognizing the severity of the problem, the U.S. Surgeon General identified sexual health as one of the seven strategic priorities in the National Prevention Strategy [2]. The U.S. Department of Health and Human Services has included sexual health and prevention of sexually transmitted diseases (STD) as priorities for Healthy People 2020, with a particular focus on Chlamydia trachomatis among adolescents and young adults. Transmission of STDs is much more prevalent among adolescents in the African-American, Hispanic, and American Indian/Alaska Native populations than in the Caucasian, non-Hispanic population. Additionally, STD prevalence is higher among economically disadvantaged populations. Other objectives set by Healthy People 2020 related to adolescent sexual health include reducing unintended pregnancy, increasing access to health services, and increasing contraceptive use [3].
On the state level, Mississippi also struggles with the issue of sexual health, particularly in regard to adolescents. Mississippi consistently has among the highest STD and teen pregnancy rates for high school students in the country [4-6].Young adults in Mississippi represent 30% of the state’s new HIV infections; however, students in Mississippi are second-to-last in the nation in receiving HIV/AIDS education [5]. According to more recent reports, in 2015, Mississippi was ranked second in the nation for teen birth rates and third in the nation for gonorrhea and chlamydia among teens aged 15-19 [6]. In 2010, Forrest County had the third highest rates of chlamydia and syphilis cases in Mississippi and was one of five Mississippi counties with the highest rates of gonorrhea [7]. In 2012, infection rates for chlamydia, gonorrhea, and HIV in Forrest County were more than double the national averages [7].
The burden of adverse adolescent sexual health outcomes is evident at the state and local levels. Economically, teen pregnancy costs Mississippi taxpayers an estimated $155 million in 2009, with approximately $3.8 million of that burden being borne by the Forrest County community [8]. Since Mississippi has a high rate of child poverty, teen mothers face challenges that impact education, health, and employment. For example, teen mothers are less likely to complete high school, with only one-third of teen mothers earning a high school diploma [8]. Teen mothers are also at higher risk for having children with low birth weight. Furthermore, the children born of teenage pregnancy also face significant challenges. Sons of teen mothers are 13% more likely to end up in prison, and daughters of teen mothers are 22% more likely to become teen mothers themselves. Additionally, children of teen mothers are more likely to perform poorly in school and are at a greater risk of abuse and neglect [8].
Multiple policy interventions have attempted to address various components of sexual health. For example, on a national level, numerous legislative policies affect adolescent sexual health, including recent provisions of the Patient Protection and Affordable Care Act (PPACA) aimed at funding family planning services and statelevel sex education programs [9]. In addition, federal administrative agency policies also affect adolescent sexual health. An example is the Food and Drug Administration's decision allowing all "women of reproductive potential, "including minors, to obtain over-thecounter access to emergency contraception [10]. At the state level, Mississippi has several formal policy interventions targeting certain aspects of adolescent sexual health, including laws related to sexual offenses against minors, sex-related education, family planning, and minor access to services for sexually transmitted disease, abortion, contraception and pregnancy [11-14]. In 2011, the Mississippi Legislature mandated sex related education in all public school districts, however not all policy efforts have been sustained. For example, in 2015 the Teen Pregnancy Prevention Program, a federally funded grant program that provided sex education to schools and communities in Southeast Mississippi for five years, was not renewed and reduced the options for sex education in Forrest County.
Recognizing the importance of addressing the challenges associated with advancing sexual health, the CDC/Health Resources and Services Administration Advisory Committee on HIV, Viral Hepatitis, and STD Prevention and Treatment (CHAC) developed the following definition of sexual health for the United States in 2012:
Sexual health is a state of well-being in relation to sexuality across the life span that involves physical, emotional, mental, social and spiritual dimensions. Sexual health is an intrinsic element of human health and is based on a positive, equitable, and respectful approach to sexuality, relationships, and reproduction that is free of coercion, fear, discrimination, stigma, shame and violence. It includes: the ability to understand the benefits, risks, and responsibilities of sexual behavior; the prevention and care of disease and other adverse outcomes; and the possibility of fulfilling sexual relationships. Sexual health is impacted by socioeconomic and cultural contexts including policies, practices, and services that support health outcomes for individuals, families, and their communities [15].
As recognized by the CHAC definition, sexual health is a multifaceted health issue affected by elements at the individual, interpersonal, community and societal levels [1]. Therefore, the framework for sexual health interventions, including public health policies, must necessarily include each of these elements. However, traditional public health approaches, such as policies and practices focused on education, screening, treatment, partner notification, and preventative services, have been segmented and more narrowly focused, and therefore limited in their ability to produce positive results [1].
Recent research suggests that a more holistic and health-focused approach to advancing sexual health is needed to overcome barriers to progress in the field [1,16]. As former U.S. Surgeon General David Satcher points out, a diverse group of key partners is essential to advancing adolescent sexual health, including state and local governments, businesses, health care providers and payers, educational institutions, and community- and faith-based organizations [17]. From a policy perspective, the input of those affected by public policies is valued in the democratic system of government in the United States [18,19]. Individual stakeholders of health policies (i.e., those who have an interest in health policies relevant to their own health or the health of others) are limited in effectiveness due to individual resource constraints. However, effectiveness increases when groups of people or organizations with similar policy interests collaborate and concentrate their individual resources. Opportunities to influence health policymaking are enhanced by collective action among those with similar policy interests [20]. Each of the numerous frameworks describing the policy advocacy process recognizes active community involvement and dialogue among diverse constituencies as crucial for effecting policy change [21].
The purpose of this study was to examine how adolescent sexual health is affected by a community’s exploring the perceptions of needs and problems, identifying policies and practices, assessing implementation and outcomes, and generating recommendations for change. To accomplish this purpose, a diverse group of community stakeholders (including community partner Southeast Mississippi Rural Health Initiative also known as SeMRHI, a network of community health centers) and researchers from The University of Southern Mississippi (USM) collaborated to evaluate policies and practices that affect the sexual health of adolescents in Forrest County, Mississippi.
Methods
In order to better identify and understand the impact of policies and practices on adolescent sexual health from the community perspective, the decision was made to form an academic-community partnership. As the academic partner, USM had a track record of community-based research relationships with communities in Mississippi. Additionally, university team members provided the expertise to conduct research and data analysis. As the community partner, SeMRHI, a Federally Qualified Health Center (FQHC), is widely known to provide high quality medical and dental services throughout a five-county service area in Mississippi, including Forrest County. SeMRHI had established and maintained effective partnerships with local school districts, as well as with many local faith and community-based organizations.
In past years, SeMRHI and USM had repeatedly and successfully collaborated to develop and maintain public health programs. By continually striving for equitable participation, open channels of communication, and transparency at all levels, this partnership developed a project that would build the capacity of the community and positively affect policy and practice. The ultimate goal was to achieve improved health outcomes among adolescents and other vulnerable populations. Support and approval for this study were first obtained from the community partner, SEMRHI in April 2014. The study received Institutional Review Board approval through the Human Subjects Committee at The University of Southern Mississippi in October 2014. Data collection occurred between March 2015 and August 2016.
Participants
Several groups of community participants were engaged throughout the research project. At the beginning of the project, university researchers and SeMRHI collaborated and formed a Community University Research Team (C-URT). The C-URT then identified community leaders to serve as a Community Advisory Team (CAT). With the help of the CAT, several different Culture Sharing Groups (CSG) were created to represent community stakeholder groups interested in or impacting adolescent sexual health (see Figure 1 Community-Academic Partnership Organization).
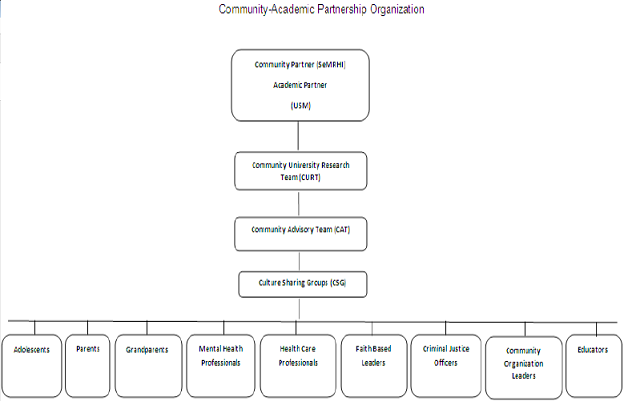
Figure: 1 Participant organization for community academic partnership.
Community – University Research Team (C-URT)
Several community stakeholders and administrators of SeMRHI were first engaged by the university researchers to form the CURT. The C-URT engaged several other community stakeholders from SeMRHI’s Teen Pregnancy Prevention (TPP) Coalition to discuss their questions and concerns related to adolescent sexual health. The TPP Coalition had been in place for over three years and was comprised of over 50 members, including individuals and representatives of local agencies and organizations. Several of these community stakeholders from the TPP Coalition were asked by the C-URT to participate on a Community Advisory Team (CAT).
Community Advisory Team (CAT)
CAT participants, who lived or worked in the Forrest County community, consisted of educators, health care professionals, faithbased leaders, mental health professionals, community organization leaders, criminal justice officers, adolescents, grandparents, and parents. CAT participants were recruited based on their concern and commitment to improving adolescent sexual health.
The purpose of the CAT was to make decisions regarding definitions of adolescent sexual health as well as developing instruments and procedures for collection of data through consensus-building processes that were facilitated by the C-URT and coordinators. To aid in the development of instruments that were both methodologically sound and representative of community questions and concerns, the C-URT established a broad methodological framework while the CAT determined specific items within the instrument, particularly questions to guide community conversations. Community conversations were designed to be one hour meetings for participants of the Culture Sharing Groups to discuss various topics related to adolescent sexual health in the Forrest County community. Once the C-URT and CAT agreed upon instruments and procedures for data collection, the CAT members were asked to individually complete (pilot test) each of the instruments to be used in the study. Recommended changes were made prior to use in the remainder of the study with participants of community conversations.
Culture Sharing Groups (CSG)
CAT members were also asked to identify between eight to ten other individuals that they believed best represent their community sub-system. These additional stakeholders were asked to participate in one of nine CSG during community conversations. While the CAT identified possible members for the CSGs, the C-URT and community coordinators identified other possible members with a goal of each CSG being broad, diverse, and inclusive. The nine CSGs were separated into groups of parents, adolescents, educators, faithbased leaders, grandparents, health care professionals, mental health professionals, community organization leaders, and criminal justice officers. In total, these CSGs included approximately 95 participants. In regard to gender, the CSGs were 73% female and 27% male. In regard to race and ethnicity, the CSGs were 70% African American/ Black, 28% Caucasian/ White, 1% Asian, and 1% Hispanic/Latino.
Data Collection
Prior to each community conversation, participants were provided discussion questions and asked to submit written responses if they could not attend the meeting. Each participant was asked to attend three group meetings as well as an all-inclusive meeting towards the conclusion of the project where preliminary results were disseminated and discussed.
In the community conversations, participants were divided into their respective CSG’s. Each group held discussions focused on identifying needs and problems that affect adolescent sexual health. CSG participants were provided the definition of adolescent sexual health agreed upon by the CAT which stated the following: Adolescent sexual health is defined as a positive and respectful approach to sexuality that involves physical, emotional, mental, social and spiritual levels. During one’s lifetime, sexual maturity develops across these five levels to strengthen the process of self-identification.
In the first community conversation, based on the definition provided by the CAT, CSG participants were asked to identify needs and problems based on physical, emotional, mental, social, and spiritual dimensions. For the second community conversation, CSG participants were asked to identify policies and practices that affect adolescent sexual health based on the previously mentioned dimensions. The third community conversation involved more of a process of self-reflection by asking CSG members to define their role and contribution in improving adolescent sexual health, challenges to fulfilling that role, and what was needed to fulfill that role. Community members were also asked to provide any recommendations and action plans they would like to see implemented.Responses from all community conversations were compiled and disseminated at a final all-inclusive meeting. The all-inclusive meeting involved all CSG and CAT participants from all subsystems. At that time, all members received a copy of preliminary data that contained a synopsis of the responses from each group. Participants from various subsystems were able to intermingle and provide their feedback and reactions to the responses from each subsystem.
Results
Data Analysis
Audio recordings of the community conversations were transcribed and reviewed to get a broad perspective of the data. Then, summaries were created and categorized by CSGs and by objectives. The software, NVivo 2.5 was used to expedite this process [21]. This software allows the researcher to store, manage, and manipulate qualitative data by creating categories or "nodes" and then find relationships between and among those nodes [22]. The transcripts were loaded into the NVivo and carefully read to obtain a broad perspective of the participants’ input. Next, the researchers reviewed the text to discern concepts common within all the collected data. Paying particular attention to each participant's perspective, the researchers looked for patterns of thoughts and opinions. These patterns are deemed “meaning units” [23]. Next, the researchers developed conceptual themes that encapsulated the essence of the shared experiences and the meanings given to them by the participants. Finally, the researchers developed a description of the themes common among the participants’ responses. The results of the analysis were shared with the C-URT for review and discussion of the process and conceptual themes. These themes were then shared with all community members at the final all-inclusive community conversation meeting, and at the final meeting with the CAT.
Findings
Responses obtained through the community conversations coalesced around five major themes including education, health, environment, parental involvement, and communication. Each theme was supported by relevant quotes from participants (see Table 1 Quotes From Participants). Findings from this thematic analysis are explicated below:
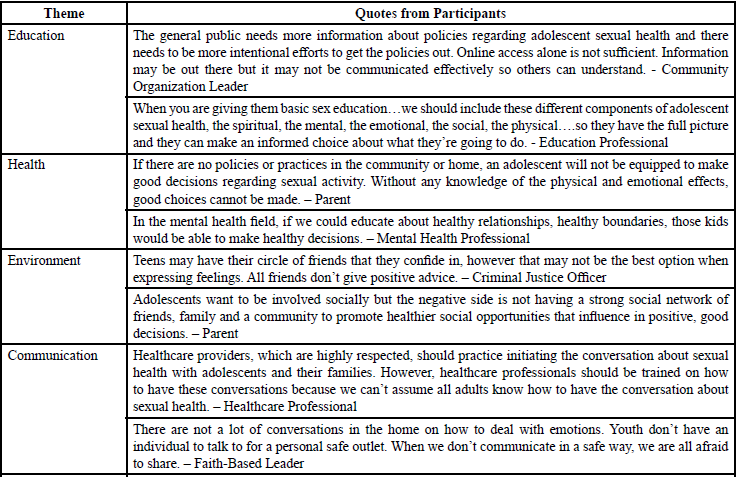
Table: 1 Quotes from participants related to various themes.
Theme 1: Education
Community members, as represented in the CSGs, most frequently commented on the importance of and need for information exchange among parents, students, caregivers or guardians, and other community stakeholders on adolescent sexual health. Although some may think about the words “education” and “information” in similar contexts, community members used these terms in different ways. Education was described as the process of not only receiving but also sharing information. Information was described as the substantive material used in the education process, which supported the members’ decision-making regarding adolescent sexual health. For instance, community members cannot be involved in education if they don’t have accurate information.
Theme 2: Health
During the community conversations, community members made references to various dimensions of health, including physical, social, emotional, mental, and spiritual health. These dimensions were primarily based on the CAT definition of adolescent sexual health. Community members described the importance of understanding physical health; however, more emphasis was placed on the various ways emotional and mental health can be affected and the influence of spirituality on sexual health.
Theme 3: Environment
During the community conversations, members described a number of environmental influences, including external factors that have significant effects on adolescent sexual health. For instance, they mentioned the overwhelming influence of peers in an adolescent’s environment, both positive and negative. Negative peer pressure and bullying resulted in fear and poor self-esteem, whereas the need for positive peers to serve as accountability partners was discussed as a recommendation. Additionally, social determinants (i.e., poverty, socioeconomic status), were of concern as community members stated that many of them live in low-income areas, but not low enough to qualify for health care services. Additionally, community involvement could help address the lack of resources available to youth.
Theme 4: Parental Involvement
During sharing groups, community members referenced parents as being the “key” to improving adolescent sexual health. Community members placed significant weight on the importance of parental guidance including communication, education and training, and involvement in the lives of all adolescents. Emphasis was placed on the parent’s responsibility to keep children informed about information related to sex, setting an example for their children, and working with others such as schools, churches, community organizations, and healthcare providers to support their child’s health and decision making.
Theme 5: Communication
Based on community members’ responses, communication fell into two distinct categories. First, participants described communication as a practice used in families and communities to convey information. Poor communication between adults and adolescents was identified as a result of several other problems such as age appropriateness, barriers, and lack of trust. Secondly, participants observed that communication regarding policies - or the lack thereof - affects policy implementation, families, schools, and agencies/organizations. It was most commonly stated that community members found out information about policies by “word of mouth”, which may also lead a breakdown in communication. As a result, people are not aware of policies and even if information is out there, it may not be communicated effectively so others can understand.
Discussion
Throughout the process of thematic analysis, researchers identified several overarching ideas brought by community members during the community conversations. One of the key findings was that the identified themes aligned with the holistic perspective of sexual health defined by the CHAC. The following points of discussion are organized under the five themes.
Education
Community members asserted a difference between education and information, recognizing that information is only one part of education. Education is an inclusive process consisting of accurate information. Community members recognized that education was most commonly thought of as a school-based program, but they expressed a strong desire for more sex education within a wider array of settings directed to both parents and adolescents. Community members reported that sex education could be strengthened with the provision of stronger and more consistent policies, such as allowing the discussion of safe sex practices and condom demonstrations in sex education curricula. Additionally, community members indicated the need for broader educational content for both students and parents, including aspects other than just physical health. For example, sex education must consider both the positive and negative impacts of technology. Community members also noted that current policies, such as abstinence only sex education policies, are restrictive and may influence how others carry out practices in multiple sectors. However, community members also reported that actual practices are more important than policies when improving adolescent sexual health. Community recommendations included maximizing social media, involving more outreach programs, and providing more accessible information about resources and services for parents and adolescents.
Health
As community members addressed varying aspects of health, there was less emphasis placed on physical health. More time was spent discussing needs, problems, policies, and practices based on mental, emotional, and spiritual health as opposed to topics related to physical health such as teen pregnancy or STDs. Additionally, the most emphasis seemed to be placed on spiritual health as community members focused on how religious or faith-based views positively and negatively impact adolescent sexual health policies and practices as well as adolescent behaviors. Some community members distinguished between what is considered spiritual, religious, and moral. For example, community members stated multiple times that, although an individual may not be religious, they could make moral decisions. Community members similarly noted that some individuals might be spiritual and not necessarily religious. Differing viewpoints on spirituality or religion may create mixed or conflicting messages, just as other messages about mental and emotional health may also have conflicting messages, be based in fear, and create double standards, which impacts how policies and practices are both perceived and implemented. Community recommendations included more access to contraceptives, more focus on healthy emotions, decision-making and self-esteem, and working with churches or religious/spiritual organizations to provide safe places for teens to discuss sexual health.
Environment
The importance of relationships and mentorship within the community was discussed as playing a role when the home or family life is lacking. Community members described the power of community as the most significant part of the environment. Community members stressed the importance of community involvement because state policies on sex education often place the responsibility on churches and community organizations to teach adolescents about sexual health. However, families, parents, and communities may have varied, and at times biased, practices to communicate with adolescents about sexual health. There was a substantial discussion among community members about the shift from adults taking responsibility for all children in the community to now having policy-based restrictions for adult interactions with minors, particularly as it relates to discussing sexual health topics in the school setting. These policies were described as barriers to the community mentality of “it takes a village.” Although community members discussed many barriers that have suppressed this power the community holds, they also expressed that this power still exists. Community members also discussed that many policies do not address the considerable influence of the environment on adolescent sexual health but focus on individual decisions instead. For example, policies may not take into consideration the negative impact of peer pressure and stigmatization. Community members suggested that organized peer mentoring could be beneficial for adolescents in making decisions about sexual health and behavior. Among the policies noted by community members, the social determinant of gender was discussed. Community members noted that many policies are femaleoriented, such as laws directed at statutory rape, incest, sexual assault, partner violence, and teen pregnancy. Community recommendations included more open communication, addressing stigmas and stereotypes, focusing on peer mentoring, and building more positive relationships.
Parental Involvement
Community members noted that many policies directed toward adolescent sexual health often assume that parents are more actively involved in the activities of their children than they actually are. In addition, policy violations (or breaking laws) are blamed solely on the child’s individual decision. As noted before, community members discussed the need to restore the “it takes a village” mentality within the community thereby encouraging adults to support and help take responsibility for children who may not be their own. Community recommendations included training for parents and other interested adults on health and well-being, developmental changes during adolescence, effective communication skills with adolescents, and parenting skills.
Communication
Based on analysis of the qualitative data, two processes of communication emerged. First, communication of policies or the lack thereof was a concern for community members. Community members identified “word of mouth” to be the primary method of communication for policy information. According to community members’ responses, a more effective method of communicating policies should include leveling language to increase understanding between the public and policymakers such as legislators. Community members had a strong desire to learn more about the policies that influence their everyday lives and interactions with adolescents. This leads into the second process: communication between adults and adolescents as a practice. Communication between adults and adolescents has the potential to create barriers or open doors of opportunity. One barrier identified across subsystems was the lack of trust. However, community members also expressed that opening up for conversation requires honesty and leveling language between adults and adolescents to foster understanding and rebuild trust. Community recommendations included promoting open dialogue with adolescents, involving others in policy making, and informing politicians of community concerns.
Limitations
Because community members included in the sharing groups may not be reflective of those who are most at-risk for some of the biggest issues with adolescent sexual health like teenage pregnancy and STDs, generalization is limited. The demographic composition of our sharing groups included primarily females with limited male participation. Therefore, the female perspective may have been overrepresented within the sharing groups. Additionally, data on socioeconomic status (SES) was not collected. Therefore, it cannot be determined how responses or participation varied by SES. Third, it was difficult to schedule meetings for the number of community members involved despite consistent contact by phone and email. As a result, faceto- face participation from community members was not consistent throughout for data collection. Community members needed time to build relationships and trust with other members and facilitators in order to open up about the topic of adolescent sexual health. Had the study continued longer, with more conversations, the authors believe additional insights would have been possible.
Conclusion and Future Practice
Participants overwhelmingly viewed adolescent sexual health as an important issue in the community and demonstrated a strong desire to share information and to address the problems of adolescent sexual health. Results indicate that participants gained valuable knowledge and insight into adolescent sexual health issues. Results also indicate that the process and strategies used by research team members to involve participants in the study, build trust within participant groups, and create a respectful sharing environment were wellreceived and could be used in future projects. Furthermore, engaging community members in discussing health policy and other issues has the potential to generate momentum in eliminating health disparities and achieving health equity.
An important consideration for this and future projects is the sustainability of the project to the stage of taking the recommended actions generated by the community. Fostering active roles in identifying problems and generating recommendations through community academic partnerships can make a difference in communities. This process also allows for community members to hear different perspectives from those who are affected most by identified problems. Additionally, those who suffer from health disparities are given the opportunity to voice concerns, be heard by others, and be part of the solution in the pursuit of achieving health equity. One of our adolescent participants said it best: Don’t be silent about what’s going on and don’t let the issues die. If there is nothing behind it, then it cannot stand, and we cannot make a difference.
Conflicts of Interest (COI) Statement
The author has declared no conflict of interest.
References
Ivankovich, M., Fenton, K., & Douglas, J .(2013). Considerations for national public health leadership in advancing sexual health. Pub Health Rep 128: 102-110.View
National Prevention Council (2013) Annual Status Report.View
U.S. Department of Health and Human Services (2020) Healthy People.View
Centers for Disease Control and Prevention. National vital statistics report.View
Sexuality Information and Education Council of the United States. Sexuality education in Mississippi: Progress in the magnolia state.View
Sexuality Information and Education Council of the United States. State profiles fiscal year 2017: Mississippi.View
Mississippi Department of Health. Reported cases of chlamydia by district and county.
Women's Fund of Mississippi. Do you know what you're spending on teen pregnancy in Mississippi?View
National Partnership for Women and Families. Why the ACA matters for women: A summary of key provisions.View
Food and Drug Administration. FDA approves Plan B one-step emergency contraceptive for use without a prescription for all women of child-bearing potential.View
Miss. Code Ann. §97-3-65 (LexisNexis 2014) (statutory rape). Miss. Code Ann. §97-3-95 (LexisNexis 2014) (sexual battery).View
Miss. Code Ann. §97-5-51 (LexisNexis 2014) (mandatory reporting of sex crimes against minors). Miss. Code Ann. §37-13-171 (LexisNexis 2014) (requiring abstinence-only or abstinence plus education in public schools).
Miss. Code Ann. §41-41-13 (LexisNexis 2014) (treating minors for venereal disease).View
Miss. Code Ann. §41-42-7 (LexisNexis 2014) (furnishing contraceptive supplies and information to minors).View
Department of Health and Human Services (US); CDC/ HRSA Advisory Committee on HIV, Viral Hepatitis, and STD Prevention and Treatment. Draft record of the proceedings; 2012 May 8-9; Atlanta.View
Douglas, J., Fenton, K. Guest editorial: Understanding sexual health and its role in more effective prevention programs. Pub Health Rep 128: 1-4.View
Satcher D (2013) Addressing sexual health: Looking back, looking forward. Pub Health Reports 128: 111-114.View
Ritas, C. (2003). Speaking truth, creating power: A guide to policy work for community-based participatory research practitioners. Hunter College Center on AIDS, Drugs, and Community Health for Community-Campus Partnerships for Health.View
Longest BB (2009)Health Policy Making in the United States. 5th ed. Health Administration Press.
Israel, B.A., Schulz, A.J., Parker, E., Becker, A.B. (2001). Communitybased participatory research: Policy recommendations for promoting a partnership approach in health research. Education for Health: Change in learning & practice (Taylor & Francis Ltd) 14: 182-197.View
Moore, S.N., Murphy, S., Moore, L. (2011). Health improvement, nutrition-related behavior and the role of school meals: the usefulness of a socio-ecological perspective to inform policy design, implementation and evaluation. Crit Pub Health 21: 441-454.View
Creswell, J.W. (1998). Qualitative Inquiry and Research Design: Choosing among Five Traditions. Thousand Oaks.View
QSR NVivo (2000) Version 2.5. Melbourne, Australia: QSR International Pty Ltd.