
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 3 (2019), Article ID: JPHIP-157
https://doi.org/10.33790/jphip1100157Research Article
Missed Appointments by Hypertension Patients in Transitional Care: Race and Insurance Correlates
Hoa B. Appel, PhD, MPH1*, Amy Ai, PhD2, Seyfullah Tingir, PhD2
1*School of Nursing & Health Studies, University of Washington Bothell, 18115 Campus Way NE, Bothell, WA 98011, USA.
22College of Social Work, Florida State University, 2500 University Center Building-C, Tallahassee, FL 32306, USA.
Corresponding Author Details: Hoa B. Appel. School of Nursing & Health Studies, University of Washington Bothell, 18115 Campus Way NE, Bothell, WA 98011, USA. E-mail: hbappel@gmail.com
Received date: 30th November, 2019
Accepted date: 26th December, 2019
Published date: 31st December, 2019
Citation: Appel HB, Ai A, Tingir S. Missed appointments by hypertension patients in transitional care: Race and insurance correlates. J Pub Health Issue Pract 2019;3:157.
Copyright: ©2019, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Missed outpatient appointments represent a barrier to continuity of care. Little evidence exists on the relationship between health insurance status and missed appointments at a transitional care clinic (TCC) for underserved hypertensive patients. High blood pressure is the leading risk factor for stroke. This study examined associations between payment status and race with missed first appointments after discharge following hypertension-based hospitalization. We conducted a retrospective study using an appointment database during the first three years at a TCC that serves underserved patients. Nearly two-thirds of eligible patients (n=144) self-identified as Blacks. Three types of insurance and demographics were used to predict the missed first appointment in three two-step logistic regression models.
We also examined the interaction between race and appointment status. The role of race in appointment status varied across three models. Privately insured patients had fewer missed appointments. However, the interaction analyses showed that privately insured Black patients were more likely to miss their first appointments than patients of other races or patients with other insurance types. Black patients without insurance were more likely to appear at appointments, though neither being publicly insured nor being uninsured was independently related to missed appointments. Further investigation into vulnerable populations should address mechanisms underlying these relationships.
Key words: Transitional Care (TC); Adherence and Missed Appointments; Interprofessional collaboration; African American Health Disparity; Cardiovascular Diseases, and Hypertension
Introduction
Health disparities among the uninsured and minority populations are a major concern in health care settings and a long-standing issue for U.S. health policy. Missed appointments can be detrimental for vulnerable patients and are barriers to efficient and effective delivery of health care services [1]. Extant literature indicates approximately 50% of all patients miss appointments in community settings and general medical practices in the United States, and between 5-55% worldwide [2]. These high rates lead to increased health administrative costs, longer wait times [2], and inefficient medical services, ultimately leading to poor control of chronic diseases [1,3]. Among vulnerable patient populations, missed appointments can be especially detrimental [1]. Mitigating missed appointments could benefit both patients and health care services. The present study examined missing appointment in patients who were hospitalized due to hypertension at a regional Transitional Care Center (TCC) with a focus on race and insurance status correlates.
Race-related Health Care Disparities
Race and health insurance play key roles in obtaining timely healthcare and medical procedures. The U.S. Department of Health and Human Services estimates that racial and ethnic minority groups will increase to nearly 40% of the U.S. population by 2030 [4]. African Americans constitute the second largest minority population (40.7 million or 12.7% of the U.S. population) with 58% of them living in the South [5]. In 2017, over 25% of African Americans were living at or below the poverty level [5].
Health insurance is a significant barrier to health care appointments and access, especially for racial and ethnic minorities. Lack of health insurance for children prevents their obtaining health care and delays necessary treatment, leading to greater health problems in adulthood. The majority of Americans between the ages of 18 and 64 receive health coverage through their employers (64%) [5]. However, just over half (53%) of Black men had employment-based coverage in 2005, compared with 70% of non-Hispanic White men, 65% of Asian, and 42% of Hispanic men.5 African Americans (AA) lack health insurance and suffer poor health outcomes more than other minority groups [6]. Approximately one third of AAs aged 20-29 were uninsured in 2008 and 2009, compared with 25% of white young adults [7]. More AAs are enrolled in managed care plans, which may affect care delivery, since these plans tend to restrict access to specialists [8].
Lack of health insurance coverage is associated with lower health care access and use [8]. Members of ethnic minority groups are less likely than whites to receive therapy for health care needs [9]. Some managed care plans simplify the referral process and attempt to reposition the gatekeeper function as a coordinative role in which members work with as medical concierge to facilitate referrals [10]. However, insurance coverage remains an important issue.
A men have the highest death rate among all minority groups [5], and older AAs may delay primary or preventive health care, resulting in more hospital services later in time [11]. The lack of hypertension management contributes to unfavorable relationships with managed care providers [12]. Managing patients with chronic disease is more difficult because some of these patients tend to move from one managed care plan to another [12]. This is a significant problem since nearly one-third of the adult population is believed to have hypertension with elevated blood pressure, and the prevalence of hypertension is higher in both middle-aged and older AAs compared with non- Hispanic whites [13].
Hypertension Care Disparities
Cardiovascular diseases (CVD) are the number one killer of all ethnic groups in the U.S [14]. Nearly one-third of U.S. adults ≥20 years of age had hypertension in 2009-2012 [15]. Among all racial and ethnic groups in the U.S., AAs have disproportionately greater cardiovascular morbidity and mortality, with half of the cardiovascular mortality due to hypertension [16]. AA adults present with the highest rates of hypertension in the world, with their age-adjusted prevalence at 44.9% and 46.1% for AA men and women, respectively [14]. Moreover, prevalence of hypertension has increased among AA adults, with AA women now ranked as the largest subpopulation of hypertensive patients [17].
Hypertension increases the likelihood of developing CVD. As a result of uncontrolled hypertension, AAs suffer strokes at a higher rate than white patients [14]. AAs with hypertension experience greater difficulty obtaining control over blood pressure and taking medications regularly than other Americans [15,18]. Among AAs with poorly controlled hypertension, appointment non-adherence is associated with lack of health insurance, inadequate hypertension knowledge, lack of education, medication side effects, and medication non-adherence [19]. Missed appointments, or appointment nonadherence, are obstacles to obtaining adequate and are associated with poor control of chronic health problems, including hypertension [20-22]. Missed appointments are also associated with an increased risk for hospital admissions [22].
Transitional Care
Examining the role of race in missing appointment at TC programs among hypertension patients is an important step toward improving hypertension-related health disparities and care services management. Health appointments provide an important opportunity to address health care disparities, particularly for those with hypertension. Therefore, identifying correlates of a missed appointment is a critical step in improving care quality delivered by community outpatient clinics, specifically for those caring for underserved populations such as AAs [23,24]. A recent analysis at a clinic serving low-income patients found that younger AA, Hispanic, Medicaid and self-pay individuals were less likely to appear for scheduled appointments than patients with private insurance [25]. These findings corroborate evidence from previous sentinel studies regarding the most vulnerable patients [26,27].
The 2010’s Patient Protection and Affordable Care Act addresses health disparities using interventional approaches, such as transitional care (TC). TC encompasses a multidisciplinary healthcare team offering time-limited, patient-centered services to ensure healthcare continuity, preventable poor outcomes in at-risk populations, and promote safe and timely transfer of patients from one healthcare setting to another [29]. To date, research has shown that TC programs present health care benefits, including reduced emergency room (ER) visits, lowered health care costs, and improved patient satisfaction, especially for older patients [16,30-33]. Also, research shows a community pharmacy-based TC program after discharge can considerably decrease hospital readmission rates [28]. Another study associated reduced hospital admission rates with an education intervention program as part of the transitional care plan [34] Under current managed care plans, patients should be able to take advantage of TC programs to improve their health outcomes [10]. Still, gaps remain in TC services.
Few studies have examined the performance of TC programs serving underserved and minority patients, who are more likely to use costly in-patient services [33]. A recent report has shown evidence that TC programs benefit Medicaid patients [33]. However, disease-specific regarding missed TC appointments in this vulnerable population is not well understood. A better understanding could help in term of minimizing the unnecessary use of expensive medical care. While federal law focuses on reducing thirty-day readmissions for specific conditions, most studies on TC programs have only offered information on the general populations [35].
The Present Study
A notable gap in the literature is the lack of information on how health insurance contributes to missed appointments at TC clinics by underserved hypertensive patients. Using the electronic records of all hypertensive patients of a northern Florida clinic, we conducted a retrospective analysis. Our research question was: Besides the evident race role, which payment status was most closely associated to missed appointments for patients hospitalized with a primary diagnosis of hypertension?
We investigated three insurance statuses: private insurance, public insurance, and self-pay/uninsured. Influences of race, healthinsurance types, and the interaction between the two variables on missed appointments were examined first before other controlled factors were entered into analyses. We hypothesized that having health insurance could improve attendance at appointments for African American patients.
Methods
Data Source and Procedure
Opened in 2011, the regional hospital’s TCC ensures outpatient follow-up for African Americans and poor populations in establishing a clinic close to their homes. Within this setting, nursing and social work staff collaboratively address patients’ barriers to accessing care, such as a lack of transportation. Many uninsured, middle-aged minority patients with multiple chronic diseases make frequent use of the ER and inpatient services. Despite the TCC’s mission for care continuity, an internal report shows an estimated 60% of patients miss appointments. Our research variables in the TCC database included: 1) demographics (age, gender, race/ethnicity, and marital status); 2) health insurance status; 3) 1st hospital discharge date when referred to the TCC initially; 4) 1st hospital discharge diagnosis and priority diagnosis number designation; 5) TCC visit dates seen; and 6) TCC visit dates missed.
Participants
All patients referred to the TCC between February, 2011(the onset of TCC), and February, 2014, were included in the initial sample. The criteria for referral included: 1) no medical insurance; 2) 3 or more hospital admissions in one year; 3) no primary care provider; and 4) patients with a primary care provider with/without insurance, but who cannot obtain a follow-up appointment within 7 days of discharge. The three-year TCC appointment database holds 6,000 patient cases referred for TCC services. Of those referred for TCC care, 144 unique cases had a primary diagnosis of hypertension at the time of their hospital admission. Among hypertension patients, 50% were female, and the average age was 49.6 (range, 24-81).
Measures
The primary outcome variable was missed first appointment (0=kept,1=missed) with respect to the first appointment referral after hospital discharge of hypetensive patients. Demographic control variables were coded as: age (1=18-35, =2=36-49, 3=50-58, 4=59+), gender (1=male, 2=female), and marital status (1=married, 2=not married, 3= unknown). Independent variables of major interests were: race (1=African American, 2=other, 3=unknown, 4= European American) and health insurance status (I.0=others,1=private; II.0=others,1=public; and II.0=others,1=self-pay). Public health insurance referred to Medicare, Medicaid, or the Veterans Health Administration. Private health insurance included managed care with public and private insurance companies. Self-pay indicated insured status with public or private insurance coverage. To examine the buffer effect of each payment status in a potential association between race and missed appointments, we created interaction variables between dummy race (others=0, African American=1) and dummy insurance types (i.e., private vs. others, public vs. others, and self-pay vs. others; coded with 1 and 0).
Data Analysis
Statistical analyses were performed using SPSS software (version 22). Three logistic regression models were performed on appointment status to reveal the significant effect of factors of major interest following preplanned two steps: 1) race, insurance type, and interaction of the two, and 2) variables in 1) and controls. All omnibus tests that is considered statistically significant if p<.05 (twotailed test).
Results
Descriptive and Bivariate Analyses
Table 1 presents the information for the sample of 144 hypertensive patients, of whom two-thirds self-identified as African American (AA). The gender pattern was balanced (female=50%), while the most common age group was 50-58 years (n=52, 36.1%; X=49.6, SD=11.2, and range: 24 to 82). Only slightly over one-fifth of the sample were married. The majority were uninsured (68.8%), oneeighth had private insurance, and less than one-fifth reported some type of public coverage. Over one-fifth of patients missed the first appointment. Correlations were conducted among all variables for 144 hypertensive patients with no missing values in Chi-square statistics. All three payment statuses were statistically independent. Race was significantly associated with missed appointments (X2=8.53, p=0.036).
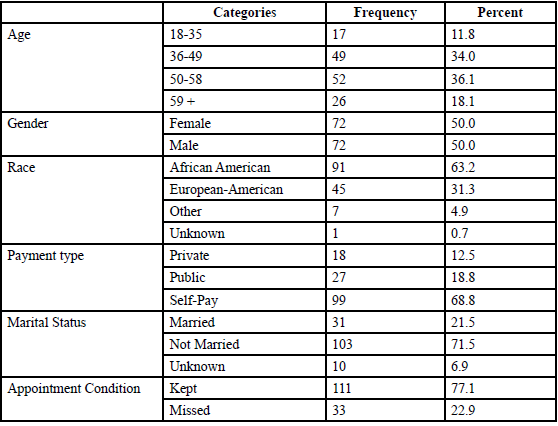
Table: 1 Frequencies and percentages of the variables for the first visit analysis for Hypertension (n=144 includes unknown values).
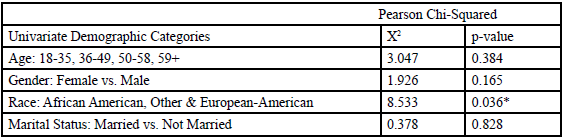
Table: 2 Bivariate Association of Independent Variables with Missed First Appointments for Hypertension Patients (n=144).
*p < .05
Logistic Regression Models
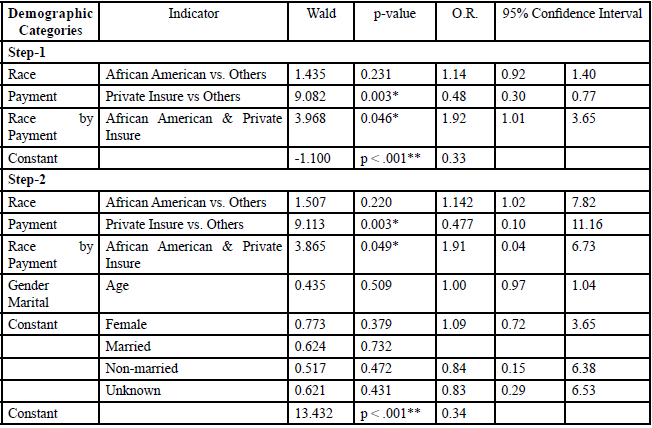
As shown in Table 3, in Step-1, Model-I, we regressed race, private insurance, and their interaction on appointment status. Interestingly, AAs were not a statistically significant predictor of missed appointments in Model-I. Both private payment and its interaction with race, however, emerged as significant predictors of missed appointments. Private payment was associated with a reduction of missed appointments by more than 50% for all hypertensive patients (OR=0.48, 95% CI: 0.30, 0.77, p=0.003). Nevertheless, interaction of race and private payment was associated with more than 90% likelihood of missing appointments (OR=1.92, 95% CI: 1.01, 2.65, p=0.046). These patterns persisted in Step 2, Model-I, after including demographic controls of which none contributed to the outcome. Specifically, privately insured minority patients were associated with a greater likelihood of failing to follow through with their referral, though private insurance was related to fewer missed appointments overall.
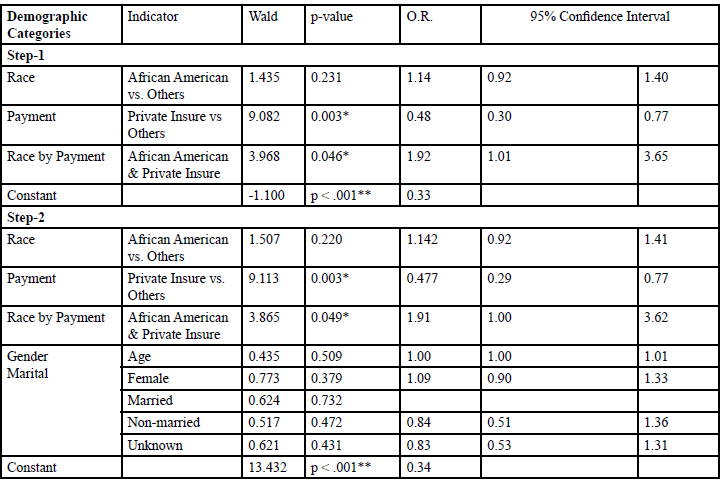
*p < .05; **p< .001
Table: 3 Model-I: Logistic Regression on Missed Appointments Concerning Private Insurance (n=144).
As shown in Table 4, in Step-1, Model-II, we regressed race, public insurance, and their interaction on appointment status. AAs were three times more likely than others to miss a first appointment (OR=2.99, 95% CI:1.11, 8.09, p=0.031). The pattern sustained in Step 2, Model-II, after entry of demographic control variables. The results indicate the publicly insured and AAs with public insurance were more likely to miss the first appointment.
*p < .05; **p< .001
Table: 4 Model-II: Logistic Regression on Missed Appointments Concerning Public Insurance (n=144).
As shown in Table 5, in Step-1, Model-III, we regressed race, outof- pocket (self) payment, and their interaction with appointment status. Similar to findings in Step-1, Model-II, AAs had a 72% higher likelihood of missing their first appointment (OR=1.72, 95% CI: 1.26, 2.35, p=0.001). Although the self-payment status had no influence, its interaction with race did. Uninsured AAs were 44% less likely to miss an appointment (OR=0.56, 95% CI: 0.37, 0.83, p=0.005). The patterns remained unchanged after introducing demographic control variables in Step-2, Model-III, revealing no new predictors. In summary, these results indicate that uninsured AAs were less likely to miss their first appointment.
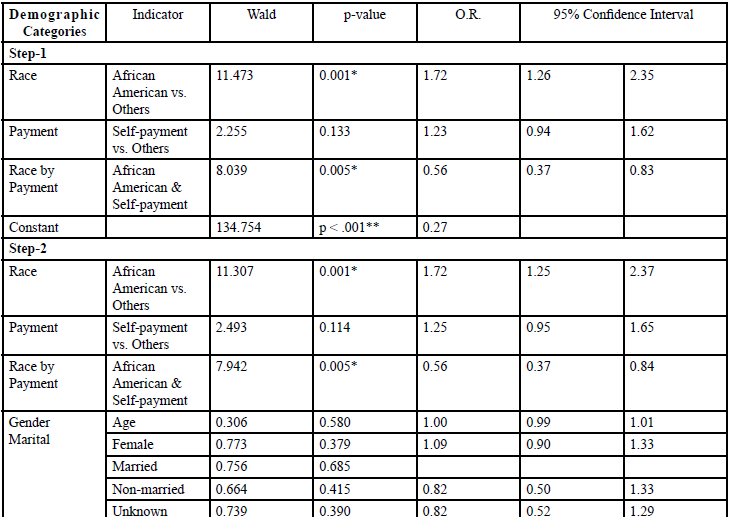
*p < .05; **p< .001
Table: 5 Model-III: Logistic Regression on Missed Appointments Concerning Self-Payment (n=144).
Discussion
The present study provides new information on the role of insurance types and race in missed TCC appointments for patients discharged from hypertension-based hospitalization. Consistent with previous studies [25-27], we found AAs who were hospitalized for hypertension were more likely to miss first appointments at the TCC in bivariate analysis in Models II and III. Nonetheless, when private insurance was analyzed with race, there was no association of AAs with missed appointments (Model-I). Surprisingly, findings on payment status were more complicated than we expected. Kaplan-Lewis and Percac- Lima (2013) showed that Medicaid and self-pay individuals tended to miss appointments [25]. Conversely, and contrary to our expectations, out-of-pocket payment was independently associated with a reduced odds of missed appointments, whereas public insurance and selfpayment status are unrelated to missed appointments. This finding suggests uninsured AAs place a higher value on TCC services. This may indicate the cost-effective TCC has a potential to reduce rehospitalization-based high cost because of its likelihood to address uninsured AAs who tend to use more expensive ER services. This assumption will need support from replication in larger samples of hypertensive patients.
An intriguing finding comes with interaction analyses on race and payment status. AA hypertensive patients with private insurance (Model I) were more likely to miss their first appointment at TCC after discharge than their publicly insured (Model II) or non-insured counterparts (Model-III). Also, uninsured AA hypertensive patients were less likely to miss their first appointment than their counterparts with private insurance (Model-III). Therefore, the findings did not support our hypothesis on the buffer of public insurance. More importantly, our result in Model-I suggests that the potential benefit of private payment for hypertensive patients might not apply to AAs.
In this study, PCP demographics, salary structure, history of caring for the underserved, and perceived practice capacity were all associated with continued acceptance of new Medicaid patients among PCPs who already had assigned Medicaid patients. By the same token, the ACA’s Medicaid expansion has been associated with increased access to care nationally [2,18,19,30-33,36]. Also, an increase in Medicaid acceptance among PCPs in Michigan [15,16]. It is also important to note the decrease in reducing hospital admission rates is associated with an education intervention program as part of the transitional care plan [34]. With managed care plans relaxing its restrictions, patients should be able to take advantage of TC programs to increase their health outcomes [10].
As stated above, transitional care could play a role in reducing hospital readmission rates and improve the overall outcomes of patients. Previous studies showed the decrease in hospital readmission rates resulting from transition care intervention with patient education and follow up [28,34]. Improving appointment adherence would also contribute to improved hypertension care for AAs [37]. In addition, the expansion of the ACA is associated with an increase in Medicaid usage and managed care primary care visits [38,39].
Health care providers and system factors can play a role addressing the failure to obtain adequate hypertension care, and thereby ease the disparity in care [40]. Uninsured AAs with poor controlled hypertension are more likely to miss their appointments than those with insurance [19]. Also, non-adherence to appointments is associated with medication non-compliance, especially among hypertensive patients [19]. This is important since the risk of having a stroke is nearly twice as high for AAs as for whites.
Limitations
Limitations of the present study include its cross-sectional nature and a small sample that does not permit causality and generalizability. The analysis in this study was also limited to simple regression relationships without consideration of socioeconomic status and homelessness status, or detailed behavioral health conditions, such as substance abuse, any of which could affect outcomes.
Furthermore, the study does not provide information on the mechanism underlying the association between private insurance and low rates of missed appointment. There are various barriers to patients receiving continuity of care, including forgetting, miscommunication/misunderstanding, lack of knowledge about health services [25], transportation difficulties, and patient’s belief that the appointment is unnecessary [33,35]. The study’s data did not allow us to explore why AAs with private insurance are more likely to miss appointments.
Conclusions
Our study addresses a gap in an under-investigated population with hypertension and public health impacts. The results suggest that AAs with hypertension who do not have access to health insurance could be more reliant on the services provided through TC. Without access to a stable medical home, these patients remain at risk for increases in symptom severity and preventable health problems.
Our findings are interpreted as preliminary. However, the findings suggest further investigation in the association of health insurance and minority status, with chronic illness in order to improve the quality of care for the vulnerable population through the current health care reform. Future study should include a prospective research design with a larger sample size and similar conditions and types of services. Additionally, it would be worth exploring how managed care could play a facilitating role in helping patients with lifestyle changes integrated with transitional care.
Conflicts of Interest (COI) Statement
The authors have declared no conflict of interest.
References
Nguyen, D.L., Dejesus, R.S., Wieland, M.L. (2011). Missed appointments in resident continuity clinic: Patient characteristics and health care outcomes. J Grad Med Ed 3:350-55.View
Perron, N.J., Dao, M.D., Kossovsky, M.P., Miserez, V., Chuard, C., et al. (2010). Reduction of missed appointments at an urban primary care clinic: A randomised controlled study. BMC Fam Pract 11:79.View
Colubi, M.M., Pérez-Elías, M.J., Elías, L., Pumares, M., & Muriel, A., et al. (2012). Missing scheduled visits in the outpatient clinic as a marker of short-term admissions and death. HIV Clin Trials 13:289-95.View
U.S. Department of Health and Human Services. NIH strategic plan to reduce the ultimately eliminate health disparities. 2000; Rockville, MD: U.S. Department of Health and Human Services, National Institutes of Health, Office of Minority Health.
Race, ethnicity, and health care. The Health Status of African American Men in the United States. Henry J. Kaiser Family Foundation.View
Lucas, J.W., Barr-Anderson, D.J., & Kington, R.S. (2003). Health status, health insurance, and health care utilization patterns of immigrant black men. Am J Pub Health 93:1740-47.View
Bloom, B., & Cohen, R.A. (2011). Young adults seeking medical care: do race and ethnicity matter? NCHS Data Brief 55:1-8.View
Hargraves, J.L., & Hadley, J. (2003). The contribution of insurance coverage and community resources to reducing racial-ethnic disparities in access to care. Health Svc Res 38:809-29.View
Monheit, A.C., & Vistnes, J.P. (2000). Race/ethnicity and health insurance status: 1987 and 1996. Med Care Res Rev 57:11-35.View
Draper, D.A., Hurley, R.E., Lesser, C.S., & Strunk, B.C. (2002). The changing face of managed care. Health Affairs 21.View
Dunlop, D.D., Manheim, L.M., Song, J., & Chang, R.W. (2002). Gender and ethnic/racial disparities in health care utilization among older adults. Journal Ger: Psych Sci Soc Sci 57:S221.View
McBride, W., Ferrario, C., & Lyle, P.A. (2003). Hypertension and medical informatics. J Natl Med Assoc 95:1048-1056.View
Hertz, R.P., Unger, A.N., Cornell, J.A., & Saunders, E. (2005). Racial disparities in hypertension prevalence, awareness, and management. Arch Intern Med 165:2098–2104.View
Mozaffarian, D., Benjamin, E., Go, A., Arnett, D.K., & Blaha, M.J., et al. (2016). Heart disease and stroke Statistics—2016 update: A report from the American Heart Association. Circul 133:e360.View
Thomas, S.J., Booth, S.N., Dai, C., Li, X., & Allen, N., et al. (2018). Cumulative Incidence of Hypertension by 55 Years of Age in Blacks and Whites: The CARDIA Study. J Am Heart Assoc 7:e007988.View
Wong, M.D., Shapiro, M.F., Boscardin, W.J., & Etter, S.L. (2002). Contribution of major diseases to disparities in mortality. New Engl J Med 347:1585-92.
Ndumele, C.D., Shaykevich, S., Williams, D., & Hicks, L.S. (2010). Disparities in adherence to hypertensive care in urban ambulatory settings. J Health Care Poor Under 21:132-43.View
Bosworth, H.B., Powers, B., Grubber, J.M., Thorpe, C.T., & Olsen, M.K., et al. (2008). Racial differences in blood pressure control: potential explanatory factors. J Gen Int Med 23:692-98.View
Nwabuo, C.C., Dy, S.M., Weeks, K., & Young, H. (2014). Factors associated with appointment non-adherence among African-Americans with severe, poorly controlled hypertension. PLOS ONE 9(8):e103090.View
Capko, J. (2007). The price you pay for missed appointments. J Med Prac Man, 22:368.
Karter, A.J., Parker, M.M., & Moffett, H.H. (2004). Missed appointments and poor glycemic control: an opportunity to identify high-risk diabetic patients. Med Care 42:110-15.
Nuti, L.A., Lawley, M., Turkcan, A., Tian, Z., & Zhang, L., et al. (2012). Noshows to primary care appointments: subsequent acute care utilization among diabetic patients. BMC Health Svc Res 12:304.View
Majeroni, B.A., Cowan, T., Osborne, J., & Graham, R.P. (1996). Missed appointments and Medicaid managed care. Arch Fam Med 5:507-11.View
Sharp, D.J., & Hamilton, W. (2001). Non-attendance at general practices and outpatient clinics: Local systems are needed to address local problems. Brit Med J 323:1081-82.View
Kaplan-Lewis, E., & Percac-Lima, S. (2013). No-show to primary care appointments. J Prim Care Comm Health 4:251-55.View
Lacy, N.L., Paulman, A., Reuter, M.D., & Lovejoy, B. (2004). Why we don't come: Patient perceptions on no-shows. Ann Fam Med 2:541-45.View
Smith, C.M., Yawn, B.P. (1994). Factors associated with appointment keeping in a family practice residency clinic. J Fam Prac 38:25.View
Ni, W., Colayco, D., Hashimoto, J., Komoto, K., Gowda, C., Wearda, B., McCombs, J. (2017). Impact of pharmacy-based transitional care program on hospital readmissions. Am J Manag Care 23:170-176.View
Coleman, E.A., & Boult, C. (2003). Improving the quality of transitional care for persons with complex care needs. J Am Ger Soc 51:556-57.View
Chapman, E., Eastman, A., Gilmore-Bykovskyi, A., Vogelman, B., Kind, A.J., et al. (2016). Development and preliminary evaluation of the resident coordinated-transitional care (RC-TraC) program: A sustainable option for transitional care education. Geron Ger Ed 1-10.View
Elliott, K.W., Klein, J., Basu, A., & Sabbatini, A. K. (2016). Transitional care clinics for follow-up and primary care linkage for patients discharged from the ED. Am J Emerg Med 34:230-35.View
McDonagh, J.E., & Kelly, D.A. (2010). The challenges and opportunities for transitional care research. Ped Transplant 14:688-700.View
Naylor, M., & Keating, S.A. (2008). Transitional care. J Soc Work Ed 44(suppl 3):65-73.View
Li, F., Guo, J., Suga-Nakagawa, A., Takahashi, L.K., Renaud, J. (2015). The impact of Kaua'i Care Transition Intervention on hospital readmission rates. Am J Manag Care 21:e560-e566.View
Naylor, M.D., Aiken, L.H., Kurtzman, E.T., Olds, D.M., Hirschman, K.B, et al. (2011). The importance of transitional care in achieving health reform. Health Affairs 2011;30:746-54.View
Hewner, S., Casucci, S., Castner, J. (2016). The roles of chronic disease complexity, health system integration, and care management in post-discharge healthcare utilization in a low-income population. Res Nurs Health 39:215-28.View
Kawasaki, L., Munter, P., Hyre, A.D., Hampton, K., DeSalvo, K.N., et al. (2007). Willingness to attend group visits for hypertension treatment. Am J Manag Care 13:257-62.View
Coleman, E.A., Parry, C., Chalmers, S., & Min, S.J. (2006). The care transitions intervention: results of a randomized controlled trial. Arch Intern Med 166:1822-1828.View
Shu, C.C., Hsu, N.C., Lin, Y.F., Wang, J.Y., & Lin, J.W, et al. (2011). Integrated postdischarge transitional care in a hospitalist system to improve discharge outcome: an experimental study. BMC Med 9:96.View
Bosworth, H.B., Oddone, E.Z. (2002). A model of psychosocial and cultural antecedents of blood pressure control. J Nat Med Assoc 94:236-48.View