
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 5 (2021), Article ID: JPHIP-182
https://doi.org/10.33790/jphip1100182Research Article
Examining Suicide and its Warning Signs and Determinants in a County of Illinois, 2014 to 2020: Implications for Future Research and Prevention
Aly Siglock, BS, MPH, Huaibo Xin*, DrPH, MD, MPH
Department of Applied Health School of Education, Health & Human Behavior, Southern Illinois University, Edwardsville, Illinois 62026, Campus Box 1126 Office: Vadalabene Center Lukas Annex 2613 in Suite 2616, United States.
Corresponding Author Details: Huaibo Xin, DrPH, MD, MPH, Department of Applied Health School of Education, Health & Human Behavior, Southern Illinois University, Edwardsville, Illinois 62026 , Campus Box 1126 Office: Vadalabene Center Lukas Annex 2613 in Suite 2616, United States. E-mail: hxin@siue.edu
Received date: 23th June, 2021
Accepted date: 07th August, 2021
Published date: 09th July, 2021
Citation:Siglock, A. and Xin, H. (2021). Examining Suicide and its Warning Signs and Determinants in a County of Illinois, 2014 to 2020: Implications for Future Research and Prevention. J Pub Health Issue Pract 5(2): 182.
Copyright:©2021, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
This study is to examine the trend in suicide over the last 12 years in a county of IL; establish warning signs leading up to suicide; identify major risk factors of suicide among the decedents; as well as explore preventative measures for future suicide interventions. It’s a mixed-methods retrospective cross-sectional study. A total of 264 existing suicide case files between 2014 and 2020 were reviewed. Based on the current literature, the suicide data collection instrument was developed to include four sections: demographics, medical history, warning signs, and risks of suicide. A total of 96 variables were included to collect both quantitative and qualitative data. Data were analyzed both quantitatively and qualitatively. From 2014 to 2020, a total of 264 suicide deaths occurred in the county with the highest number in 2017 and lowest in 2010. Approximately 77.3% of the suicide deaths were males and 81.1% were non-veterans. About 31.4% of the cases left a suicide note; 22.1% had previously attempted suicide; and 49.2% had previous suicide ideation. About 39.4% of the deaths were caused by gunshot wounds, 39.4% were caused by suffocation, and 15.5% were caused by poisoning. More than half of the cases (58.3%) had a mental illness, including depression, anxiety, and bipolar disorder. Nearly 45.5% of the cases were taking prescription medications. Roughly 41.7% of the cases indicated they were in a troubled relationship, 33.0% indicated they could be grieving the loss of parents, significant others, children, and siblings. Only 23.9% of the cases had received suicide prevention treatment, such as hospitalization or admittance to a mental health center, prior to their suicide death. Future endeavors should consider developing suicide prevention strategies/interventions within the domains of the Social Ecological Model, including building social capital, issuing temporary firearms restraining orders, and establishing community-based suicide prevention training/screening programs.
Key Words: Suicide, Suicide Prevention, County, Social Ecological Model
Introduction
Nationally, the rate of serious consideration of suicide within the last 30 days has doubled during the COVID-19 pandemic from 4.3% to 10.7% compared to the rate collected in 2018 [1]. Although an increase in suicide deaths during the COVID-19 pandemic has not been reported, suicide remains as the 10th leading cause of death in the U.S. across all races, sexes, and ages with a total of 48,344 suicide deaths in 2018 [2]. The age-adjusted suicide mortality rate in 2018 was 14.2 deaths by suicide per 100,000 deaths in the U.S [3]. The state of Illinois reported a similar age-adjusted suicide mortality rate of 11.3 deaths by suicide per 100,000 deaths in 2018 [4]. Within Illinois, counties, reported higher rates of suicide mortality than the state’s rate – an age-adjusted rate of 14.1 deaths by suicide per 100,000 deaths throughout the years of 2008 to 2017 [5].
Nearly double the amount of people died by suicide in 2018 (48,344 total suicide deaths) than in 1999 (29,199 total suicide deaths) in the U.S [6]. The age-adjusted suicide rate in the U.S. has drastically increased by 35% between the years of 1999 to 2018, from 10.5 suicide deaths per 100,000 deaths in 1999 to 14.2 suicide deaths per 100,000 deaths in 2018 [6]. Between the years of 1999 to 2006, the average suicide death rate increased by about 1% each year, and between the years of 2006 to 2018, the average suicide rate increased by about 2% each year [6]. Dying by suicide disproportionately affects males than females in the U.S. In 2018, the national suicide death rate for males was 22.8 suicide deaths per 100,000 deaths, which was 3.7 times higher than the female suicide death rate of 6.2 suicide deaths per 100,000 deaths [6]. Of the total 48,344 suicide deaths in 2018 nationwide across all sexes, races, and ages, 50.54% of suicide deaths involved the use of a firearm, 28.63% of suicide deaths occurred by suffocation, 12.90% of suicide deaths occurred by poisoning, 2.38% of suicide deaths occurred by falling, 1.86% of suicide deaths occurred by cutting or piercing, and 1.39% of suicide deaths were due to another specification – 1.08% of suicide deaths occurred by drowning, 0.44% of suicide deaths occurred due to fire or burns, and 0.39% of suicide deaths occurred by use of transportation [7].
A plethora of risk factors associated with death by suicide have been documented. Suicide is a complex issue; multiple factors can accumulate that lead to a suicide death. Suicide can be particularly related to certain populations. For example, significant associations exist between the risk factors of sleep difficulties, hopelessness, disconnection from others, and self-reported depression, and increased college student suicide risk [8]. According to the Spring 2019 American College Health Association-National College Health Assessment, within the last 12 months, 13.3% of surveyed college students reported that they had seriously considered suicide, 2.0% of surveyed college students reported that they had attempted suicide, and 8.6% of surveyed college students reported that they had self-harmed [9]. Psychiatric disorders, particularly depression, loss of independence, physical illness, bereavement, obsessional traits, and cognitive rigidity have been identified as risk factors for elderly suicide [10]. Moreover, compared to the general population, people within the LGBTQ population have a 40% increased risk of dying by suicide [11]. Although limited data regarding LGBTQ suicide death rates exist due to a lack of sexual orientation data available in death records, LGBTQ individuals have been documented to attempt suicide at elevated rates compared to the general population [12]. Transgender individuals may be at an alarmingly increased risk of dying by suicide (800 suicide deaths per 100,000 transgenders post-gender reassignment surgery) compared to the U.S. general population, but further research is needed to clarify the suicide risk of transgendered individuals [12]. In a study of veterans at a psychiatric clinic, over half (52%) reported suicidal ideation within the past week, and most (97%) displayed at least one suicide warning sign, with the most common warnings signs being agitation, sleep disturbances, desperation, anxiety, and hopelessness [13]. Veterans with post-traumatic stress disorder (PTSD) and depressive syndrome were found to display the most suicide warning signs [13]. Substance use disorder among veterans with PTSD significantly increased the risk of death by suicide [14]. Homosexual and bisexual orientation, family discord and disruption, homelessness, previous suicide attempts, loss events, and physical and sexual abuse have been identified as strong suicide risk factors for youth [10]. About 50% of adolescent suicide decedents come from a divorced family [15]. School problems and disciplinary crisis are also suicide risk factors for youth [15]. Psychiatric disorders increase the suicide risk for young people [15] by an odds ratio of 12 to 35. About 16% to 28% of youth suicides have legal problems [15]. Young people with previous suicide attempts have about a 30 times greater suicide risk compared to young people without previous suicide attempts [15]. The risk of suicide increases with alcohol intoxication, even if one does not have a substance use disorder [16]. Alcoholics who died by suicide have been found to have a more severe form of alcoholism in comparison to alcoholics who have no prior suicide attempts [16]. Alcohol use disorder was found in 56% of suicide deaths in one U.S. study [16]. In New Zealand, alcoholic suicide attempters had an increased likelihood of having anxiety disorders as well [17]. Furthermore, increased suicide deaths overall and firearm suicide deaths, but not non-firearm suicide deaths, are strongly associated with increased firearm ownership in the U.S [18]. States with 1 percent point higher firearm ownership rate have, on average, an increased suicide rate of 0.22 suicide deaths per 100,000 population [18]. Higher firearm suicide rates are observed in states with increased proportions of whites [19]. Sadly, newspaper reports of suicides with captivating headlines and photographs, especially of celebrity suicides, as well as suicide portrayed in TV dramas have also been found to influence suicide behavior of the general population [10] as elevated suicide rates are documented following highly publicized suicide stories [20].
Strategies have been employed to combat the elevating suicide rates in the U.S. Among these suicide prevention strategies are the Safety Planning Intervention, [21] gatekeeper trainings, [22] crisis self-help lines, [23] firearm restriction, [24] clinical screening, [11] and parental education [15]. However, the effectiveness of these strategies is often difficult to establish. Clearly, more work is needed to prevent suicide in the U.S. given the steadily increasing suicide mortality rate each year [6]. The purpose of this study is to determine the trend in suicide over the last 12 years in a county of Illinois; establish warning signs leading up to suicide and examine major risk factors of suicide among the decedents in the county in the past seven years; as well as explore initiatives to prevent suicide for future implication.
Materials and Methods
Study Design:
This study uses a mixed-methods retrospective cross-sectional observational study design to examine suicide in a Midwest county through the years of 2014 to 2020. A cross-sectional study is one that observes the prevalence of a health outcome during a specific timeframe [25]. A mixed-methods study design includes collection and analysis of both quantitative and qualitative data [26]. Institutional review board (IRB) approval was exempt because the current study population is comprised of deceased individuals, which does not meet the IRB approval criteria of live human subjects. To protect the privacy of the individuals studied, no data related to personal identification, such as their name, address or identification numbers, were collected.
Sampling
Utilizing secondary data, this study is rooted in extracting data from the County Coroner’s Office suicide case files between the years of 2014 to 2020. Only case files classified as suicide were used in the data collection; any case files still under investigation, incomplete, or pending were not included in the data collection. Using the data collection form, relevant information was documented from the suicide case files, including information from the certificate of death worksheet, investigative report, toxicology report, suicide notes, photographs, police reports, autopsy reports, medical records, and other information. A total of 264 suicide case files were reviewed.
Instruments
By examining information regarding suicide from peer reviewed academic journals, such as the American Public Health Association (APHA) and the Archives of Suicide Research, and credible websites, such as the National Institute of Mental Health, a suicide data collection tool was produced. The suicide data collection tool included four sections and 96 variables – demographics, medical history and other characteristics, warning signs, and underlying causes of suicide. Within the demographics section, information, such as sex, race, occupation, education, and location of residency, were collected for data analysis. The medical history and other characteristics sections included information regarding health diagnosis, medications, mental illness diagnoses, clothing worn at time of death, and noted tattoos. The warning signs included the presence of a suicide note, previous suicide attempts, exposure to suicide, and threat of suicide are a few examples of data collected in the warning signs section. The underlying causes of suicide section of the data collection tool included data such as troubled relationships, job loss, loneliness, and childhood trauma. Some components of the suicide data collection tool, such as the threat of suicide section, were mimicked from Johnson’s data collection tool [27] in St. Clair County, Illinois. The suicide data collection form was created by the principal investigator and validated by the research mentor, the County Public Health Director, and the County Deputy Coroner.
Data Analysis
All quantitative data from the collection forms was entered into IMB SPSS 27.0 (Armonk, NY). Descriptive statistics were conducted to determine the suicide trend between the years 2008 to 2020 in a county, Illinois. All 96 variables were analyzed using descriptive statistics including frequencies, percentages, and Chi square tests. Qualitative data was analyzed using theme analysis.
Results
A total of 473 suicide deaths occurred in a county of IL between the years 2008 to 2020. Figure 1 illustrates the suicide mortality trend in the county between the years 2008 to 2020. During this 12- year time period, the most suicide deaths occurred in 2017, with a total of 53 suicide deaths, and the least number of suicide deaths occurred in 2010, with 25 total suicide deaths. In the last 12 years, the accumulative suicide mortality rate was 18 per 10,000 residents living in the county of IL. The highest annual suicide mortality death rate was 2 per 10,000 residents in 2017, and the lowest annual suicide mortality rate was 1 per 10,000 residents in 2010.
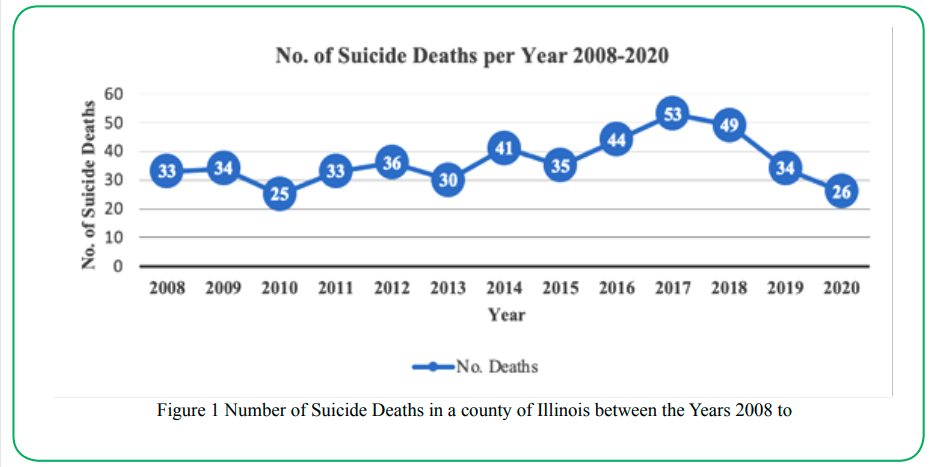
Figure 1.Number of Suicide Deaths in a county of Illinois between the Years 2008 to
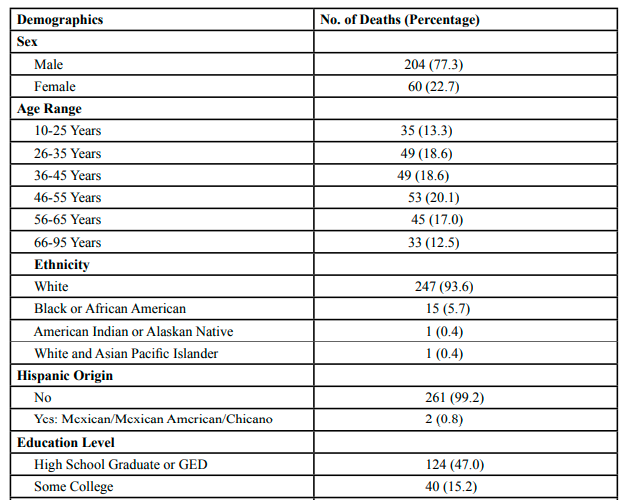
Table 1.Demographic Information About Decedents who Died by Suicide in a County of IL, 2014-2020 (N=264)
Table 1 shows that the majority (77.3%) of those who died by suicide in the county between the years 2014 to 2020 were males and 22.7% were females. The most suicide deaths (20.1%) were individuals between 46 to 55 years old. The next most prominent age groups were individuals age 26 to 35 years and 36 to 45 years with 18.6% of suicides in the county between the years 2014 to 2020 occurring in both of these age categories. The vast majority (93.6%) of suicide deaths occurred in those of White ethnicity, 5.7% of suicide deaths were Black or African American, 0.4% of suicide deaths were American Indian or Alaskan Native, and 0.4% of suicide deaths were White and Asian Pacific Islander. Only two suicide deaths were of Hispanic descent with 99.2% of decedents not of Hispanic descent. Nearly half of those who died by suicide had graduated high school or completed a GED as their highest level of education achieved. Most (81.1%) of those who died by suicide were not veterans; 15.9% of decedents were veterans. Half of those who died by suicide were not in a relationship, and 49.3% of those who died by suicide were known to be in a relationship, including having a marriage, having a fiancé/cee, or having a girlfriend/boyfriend.
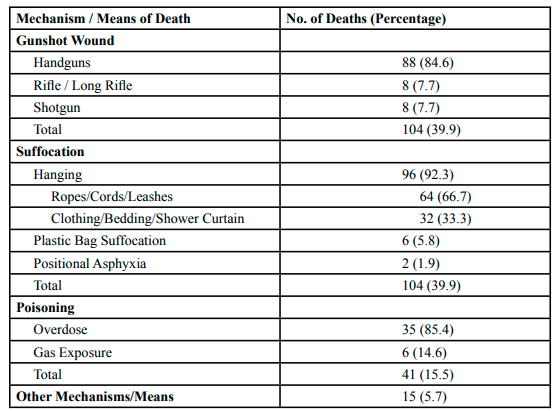
Table 2.Mechanisms and Weapons/Means of Suicide Deaths in a County of IL, 2014-2020
As indicated in Table 2, of the total 264 suicide deaths that occurred in the county between the years 2014 to 2020, both suffocation and gunshot wounds accounted for 104 (39.4%) suicide death mechanisms each. Of the suicide deaths that occurred from gunshot wounds (104 deaths), a handgun was used in 88 deaths (84.6%), and both shotguns and rifles were used in 8 deaths (7.7%) each. A third (33.3%) of the suicide decedents used a handgun to end their life, making handguns the most frequently used item by suicide decedents. Of the 104 suffocation deaths, hanging accounted for most (92.3%) suicide death mechanisms, with ropes, cords, or leashes used in 64 deaths (66.7%), and clothing, bedding, or shower curtains used in 32 deaths (33.3%). Of the 41 poisoning suicide deaths, 35 deaths (85.4%) occurred by use of prescription, over the counter, or illegal drug(s), and 6 deaths (14.6%) occurred by gas exposure, such as carbon monoxide. A limited number of suicide deaths (15 deaths) occurred by other mechanisms, such as blunt impact trauma (5 deaths), cutting or stabbing (4 deaths) and drowning (3 deaths). In about 15% (40 deaths) of the suicide deaths, pharmaceuticals were listed as contributing to the cause of death, including prescription medications, over the counter medications, and/or illegal drugs.
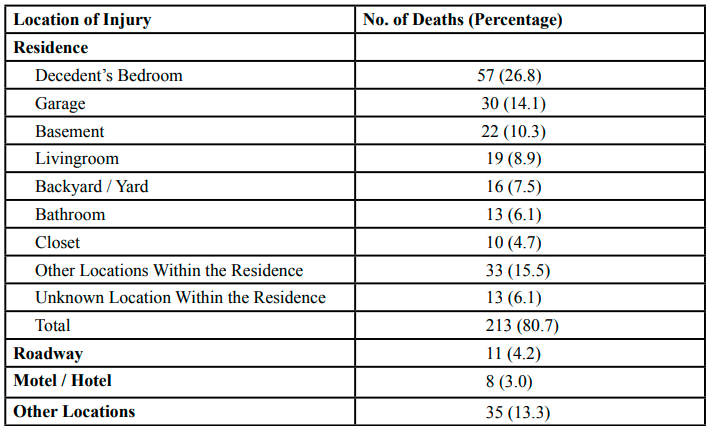
Table 3.Location of Suicide Deaths in a County of IL, 2014-2020 (N=264)
Table 3 presents the location of the suicide deaths that occurred between the years 2014 to 2020 in the County, IL. The vast majority of suicide deaths (80.7%) occurred within a residence, usually the decedent’s residence, as only 7 deaths (2.7%) occurred at a residence that was not the decedent’s home. Roadways, hotels, and motels were also common locations where suicide death occurred. Parking lots (6 deaths), rivers (4 deaths), wooded areas (4 deaths), and commercial buildings (3 deaths) were other locations where suicide deaths occurred.
Of the 239 suicide deaths that occurred at a known date, the most suicide deaths (28.9%) in the county between the years 2014 to 2020 occurred during the summer season and the least number of suicide deaths (20.9%) occurred during the winter season. About 20.1% of suicide deaths that occurred at a known date occurred at the time of the seasonal change, within seven days before or after an equinox or solstice. Of the 239 suicide deaths that occurred at a known date, the most suicide deaths (13.4%) occurred during the month of September. Viewing weeks starting on Sundays and ending on Saturdays, the most suicide deaths (61 deaths) occurred during the second week of the month. The highest number of suicide deaths (49 deaths) occurred on Mondays and the lowest number of suicide deaths (24 deaths) occurred on Saturdays. Of the 239 suicide deaths that occurred at a known date, 43 suicide deaths (18.0%) occurred within three days of a holiday. New Year’s Day (8 deaths), Labor Day (6 deaths), and Christmas (5 deaths) were the most common holidays when suicide deaths occurred. Of the 165 suicide deaths that occurred at a known time, 57.6% of these deaths occurred during the PM (Post Meridiem) hours and 42.4% of these deaths occurred during the AM (Ante Meridiem) hours. Specifically, 8.5% of suicide deaths that occurred at a known time occurred during the hour of 3PM and 6.7% of the suicide deaths that occurred at a known time occurred during the hours of both 9AM and 11PM.
Most of the people who died by suicide (20.7%) were wearing a black shirt when they died, and most of the people who died by suicide (36.2%) were wearing blue pants when they died. About 40% of those who died by suicide were wearing accessories, including rings, necklaces, and watches, at their time of death. About a third (86 deaths) of the suicide death decedents had tattoos. The most common tattoos were words or phrases (19 deaths), names (14 deaths), crosses (11 deaths), and hearts (10 deaths).
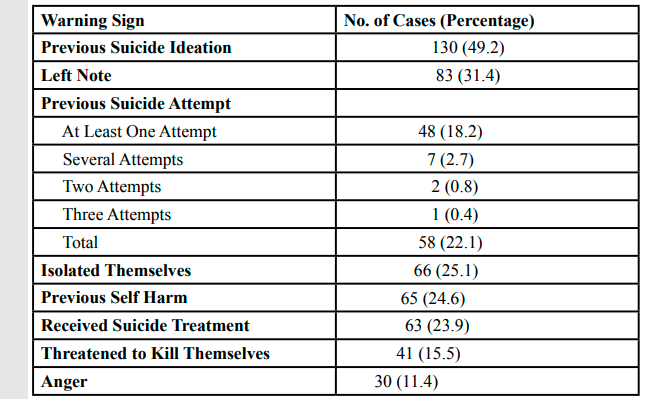
Table 4.Warning Signs of Suicide Exhibited by Suicide Decedents in a County of IL, 2014-2020 (N=264)
Table 4 shows that of the total 264 suicide deaths that occurred in the county, IL between the years 2014 to 2020, half were known to have previously had suicide ideation. Over a quarter of those who died by suicide left a note when they died. About 22% of the total 264 suicide deaths were known to have attempted suicide previously before they died. A quarter of those who died by suicide had isolated themselves prior to their death. Of the total 264 suicide deaths that occurred, 24.6% were known to have previously engaged in self-harm. About 24% of those who died by suicide were known to have receive treatment for suicidal thoughts, including hospitalization (34 deaths) and visiting a behavioral health center (13 deaths). Of the 264 total suicide deaths, 11.4% of those who died by suicide reported to be angry. A total of 21 suicide deaths that occurred had reported at least one exposure to a suicide death prior to their own death by suicide. Of the 21 suicide deaths that had reported exposure to suicide, 8 suicide exposures were documented with the most commonly reported suicide exposure (34.7%) as death of a sibling to suicide. Three (14.3%) of those who were exposed to suicide prior to their death were known to have died by the same mechanism of suicide death as the person they were previously exposed to. Of the 264 total suicide deaths, poor sleep and aggressive behavior, including yelling, hitting and threatening violence, were reported in 6.5% of the suicide death case files. Qualitative theme analysis found the following additional suicide warning signs: 21 deaths (8.0%) had been reported to miss work, school, or family events, 14 deaths (5.3%) had sent an affectionate or apologizing message or call to a loved one prior to their suicide death, and 9 deaths (3.4%) were known to recently obtain access to a gun.
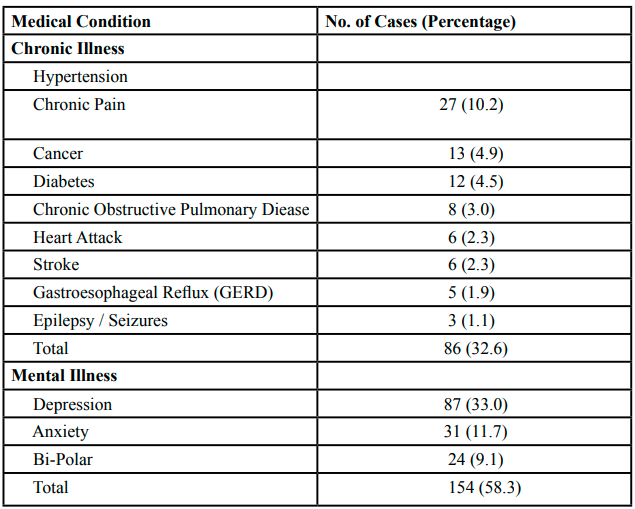
Table 5.Medical Conditions of Suicide Decedents in a County of IL, 2014 to 2020 (N=264)
Table 5 indicates that of the total 264 suicide deaths, 32.6% of those who died by suicide in the county, IL between the years 2014 to 2020, had a chronic illness. The most commonly reported chronic illness of those who died by suicide was hypertension (10.2%). Over half (58.3%) of those who died by suicide reported a mental illness, and depression was most commonly reported (33.0%). Fifteen (5.7%) of the suicide deaths were known to refuse medical intervention to treat their mental illness. Six (2.3%) of the people who died by suicide were known to recently stop taking their mental illness medications prior to their death. Five (1.9%) of those who died by suicide had mentioned to someone that their medication(s) had adversely changed them or gave them suicidal thoughts.
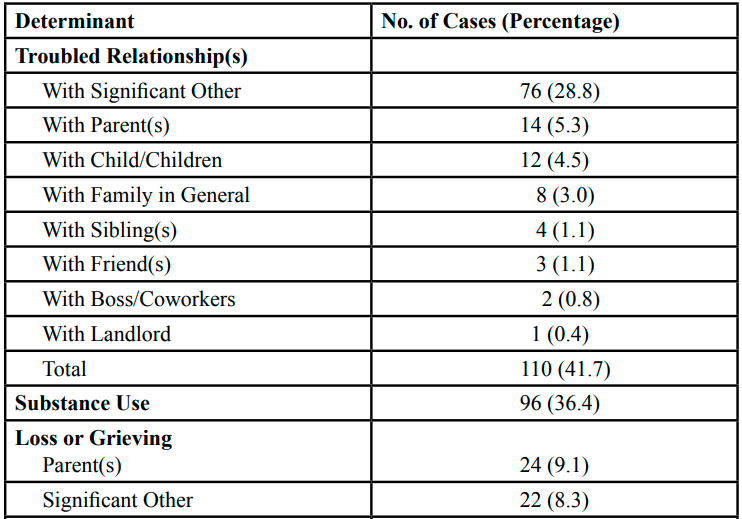
Table 6.Determinants of Suicide Deaths in a County of IL, 2014-2020 (N=264)
Table 6 indicates that of the 264 total suicide deaths that occurred in the county, 41.7% of those who died by suicide had at least one troubled relationship. About 29% of the total 264 suicide deaths had a troubled relationship with their significant other. Six of the suicide death decedents were known to be going through a divorce at their time of death, and 23 suicide death decedents were known to have had a recent breakup or separation from their partners at their time of death. Of the total 264 suicide deaths, 36.4% were known to be using substances, such as alcohol, methamphetamines, or cocaine, at their time of death. Nearly a quarter (22.7%) of suicide death decedents tested positive for alcohol in their bloodstream at their time of death. A third (33.0%) of those who died by suicide could have been grieving at their time of death. Of the 87 suicide decedents who could have been grieving, the most commonly reported losseswere parents (27.6%), significant others (25.3%), children (21.8%), and siblings (16.1%). Financial issues were reported in 18.2% of the total suicide deaths that occurred in the county with 6.1% of suicide deaths known to have recently lost their jobs. Stress was documented in 13.6% of the total suicide death case files. Living problems, including homelessness, eviction, and looking for a place to live, was documented in 10 (7.6%) of the suicide death case files between the years 2014 to 2020.
Of the 154 suicide death cases in the county, IL between the years 2014 to 2020 that indicated having a mental illness, the following indirect causes were observed: 65 cases (42.2%) had troubled relationships, 55 cases (35.7%) had a loss or were grieving, 54 cases (35.1%) used substances, 27 cases (17.5%) had psychological pain, 21 cases (13.6%) had stress, 19 cases (12.3%) had legal issues, 14 cases (9.1%) had fear, 10 cases (6.5%) reported loneliness, 10 (6.5%) cases were known to experience childhood trauma, 9 cases (5.8%) expressed burdensomeness, 9 cases (5.8%) indicated being a victim or perpetrator of sexual assault, 9 cases (5.8%) had shame, and 8 cases (5.2%) had guilt. Of the 96 suicide death cases that indicated substance use, the following indirect cases were observed: 59 cases (61.5%) had troubled relationships, 33 cases (34.4%) had a loss or were grieving, 16 cases (16.7%) had legal issues, 12 cases (12.5%) had psychological pain, 9 cases (9.4%) had a recent job loss, 8 cases (8.3%) had stress, and 7 cases (7.3%) felt burdensomeness. Of the 86 suicide death cases, the following indirect causes were observed: 52 cases (60.5%) had mental illness, 29 cases (33.7%) had troubled relationships, 26 cases (30.2%) had a loss or were grieving, 21 cases (24.4%) used substances, 14 cases (16.3%) had psychological pain, 10 cases (11.6%) had financial issues, 9 cases (10.5%) felt burdensomeness, 8 cases (9.3%) had stress, 6 cases (7.0%) felt loneliness, 5 cases (5.8%) felt fear, and 5 cases (5.8%) felt shame.
Discussion
The suicide mortality rate in 2018 was found to be higher in the county at 1.46 suicide deaths per 10,000 residents than both the state of Illinois suicide morality rate of 1.13 suicide deaths per 10,000 deaths, [4] and the U.S. overall suicide mortality rate of 1.42 per 10,000 deaths [3]. The national suicide death rate is 3.7 times higher for males than for females [6]. Similarly, the suicide death rate for males, at a rate of 6.09 suicide deaths per 10,000 residents in the county, was 3.4 times higher than the suicide death rate for females, at a rate of 1.79 suicide deaths per 10,000 residents between the years 2014 to 2020. Looking at the means of suicide deaths, a higher percentage (50.54%) of suicide deaths occurred by use of firearms nationally in 2018 [28] than in the county (39.9%) between the years 2014 to 2020. Of the suicide cases that reported use of a specific firearm, handguns were most commonly used nationally in 2018 (26.5%) [28] and within the county (84.6%). A higher percentage of suicide deaths occurred by suffocation in the county (39.9%) than in the U.S. overall (28.63%) [7]. A similar percentage of suicide deaths occurred by poisoning at the national level (12.90%) [7] and within the county (15.5%).
The implications of the present study for future research and practice are described below through the Social Ecological Model (SEM) lens, starting with the innermost layer to the most encompassing layer: intrapersonal, interpersonal, institutional, community, and policy [29]. The suicide prevention role of the intrapersonal layer of the SEM entails empowering individuals to continue living. A top-down approach is the focus of the SEM, with an emphasis on changing the outer levels to influence the individuals’ health behavior [29]. However, in suicide prevention, modifying the lower intrapersonal and interpersonal levels tend to be more effective [30]. Self-compassion and practicing spirituality are two intrapersonal factors linked to suicide prevention. For instance, most (58.3%) of those who died by suicide in the county had a mental illness, with depression found most commonly in 33.0% of the total cases. Focusing on the heart space as an act of self-compassion minimizes the rumination of the mind, and acts as a natural antidepressant [31]. One way to activate self-compassion, self-love, and self-understanding is by placing hands on the heart space [31]. Public health initiatives, such as trainings, classes, or programs, that enable individuals to foster more compassion for themselves via simple practices, such as connecting to the heart, could be an empowering step toward suicide prevention. Initiating or strengthening an individual’s spirituality could also play a role in suicide prevention. One study found spirituality to be lower in suicidal individuals than in the general population [32]. Attendance to religious services has been found to decrease suicide ideation, [33] and reduced suicide risk is associated with religiosity, as religious countries exhibit lower suicide rates than secular countries [34]. Some (6.1%) of those who died by suicide in the county were wearing religious jewelry, including crosses and rosary bead necklaces; 4.2% of cases had tattoos of crosses at their time of death; and 0.8% of suicide decedents were known to have sought help for suicidal ideation from a pastor or a saint. Religiosity is associated with reducing levels of hostility and aggression, as well as promoting reasons for living [34]. Religious and spiritual involvement can increase the social network and support of individuals [35] and can create social identification with those of similar religious beliefs, which promotes positive social bonds [36].
Family relations are of particular importance within the interpersonal domain because these interpersonal relationships have the potential to serve as either a protective or detrimental factor related to suicide risk [37]. The present study found that the troubled relationships of those who died by suicide in the county occurred in relationships among family members and significant others. Families – particularly, siblings, children, and parents – are a target population that warrants increased suicide prevention and intervention strategies [37]. Mental health providers can empower family members of suicidal patients by providing them with education and problem-solving suicide prevention techniques, which increases the ability for families to support their relatives at elevated risk of dying by suicide [37]. Prevention initiatives linking individuals to suicide resources should target those at an elevated suicide risk within families, such as when suffering a loss or grieving, and especially, when a family member has been lost to suicide. Health care workers, such as clinicians, therapists, and social workers, can aid their patients to identify healthy, reliable family relationships and other suicide resources by utilizing the Safety Planning Intervention (SPI).21 Trainings that offer continuing education units (CEUs) to health care workers should focus on linking clients to a vast array of available resources, including family, friends, schools, housing, legal services, financial resources, jobs, religions, recreation activities, and support groups [38]. An example of support groups that assist grieving families are self-help groups for survivors of suicide loss. It is important for family survivor self-help groups to emphasize that grieving is a natural process, and that feelings of severe emotional grief are likely to occur at the anniversary date of their loved one’s suicide death [39]. Survivors of suicide loss self-help groups have the opportunity to create community bonds that expand further than the formal meetings – many of these groups sustain community connection by utilizing virtual platforms, such as online bulletin boards, blogs, social media, phone calls, text messages, and emails [39].
An institutional level prevention strategy that directly applies the Native American ancient teachings of oneness with animals [40] is for schools to utilize the animal symbolism of their mascots to create suicide prevention programs. As the tiger symbolism is rooted in protection, [41] school-wide programs teaching children and adolescents how to protect themselves from suicide could be implemented. Suicide prevention school programs embedded with the tiger protection symbolism could train students on gun safety and conflict resolution [42]. Suicide prevention programs related to school mascot symbolism could be implemented in the cities, school districts, and communities where the majority of suicide deaths occurred. Another example of a school-based suicide prevention program involves empowering parents to connect with and aid other parents, as well as cultivate healthy relationships with their children. Parent education programs given to families with adolescents in high school that focus on enhancing communication skills and relationship dynamics, are effective at strengthening protective factors related to suicide risk, such as decreasing child-parent conflicts, minimizing adolescent substance use, and decreasing adolescent delinquency [43] High school programs that empower parents with problem-solving skills have been found to not only decreased suicide risk in adolescents whose parents directly participated, but even the parental involvement of an adolescent’s best friend decreased subsequent substance use by adolescents [43].
Within communities, suicide prevention campaigns may best be initiated in pharmacies as about half (45.5%) of those who died by suicide in the present study were known to take prescription medications. Suicide prevention and intervention strategies conducted at pharmacies may have the unique potential to reach groups who are at elevated suicide risk – essential workers and caregivers. Although pharmacies can serve a key role in reaching those at risk of suicide or those able to assist someone at risk of suicide, one study among a sample of 501 community pharmacy employees found few (8.8%) staff members had training or knowledge of resources for suicide prevention, and the majority of the staff (89.6%) desired additional suicide prevention training [44]. The same study reported that about a quarter (22.4%) of pharmacy employees knew a patient who died by suicide, and 21.6% of the pharmacy staff had been asked by a patient for a lethal dose of medication [44]. Pharmacy staff may also be at elevated risk of suicide due to the exposure to suicide deaths among their patients. The role of pharmacies and pharmacy staff exhibit an opportunity to prevent suicide because pharmacies are a health care resource within communities. Pharmacies may also serve as an appropriate setting for clinical suicide risk screenings. An example of a successful pharmacy intervention that was attributed to a 25.7% statewide decrease in opioid deaths between the years 2014 to 2015 stems from New Mexico [45]. This pharmacy campaign employed their intervention simultaneously with the adoption of a statewide order to promote the awareness, distribution, and use of Naloxone, a medication that prevents death by opioid poisoning [45]. State laws can differ; however, the Illinois Substance Use Disorder Act empowers healthcare professionals, including licensed pharmacists, to dispense Naloxone and educate anyone at risk of having an opioid overdose, or anyone able to assist someone at risk of having an opioid overdose [46]. Similar community access tactics could be implemented in pharmacies to prevent suicide.
Firearms were found in the present study to contribute to 39.4% of suicide deaths in the county. Freedom to own a firearm is a U.S. constitutional right; however, an effective policy level suicide prevention approach is to issue temporary Firearm Restraining Orders (FROs) to briefly remove firearms from people at risk of suicide [47]. The civil order FRO policy in Illinois allows temporary firearm removal to be facilitated by members of the family, [47] however many states have different FRO policies that could require a criminal process to remove household firearms [48]. The authorities responsible for use of this temporary firearm removing policy includes judges when warrants are required for firearm removal, [48] and law enforcement officers, as well as trusted friends and family members [47]. FROs restrict someone at risk of suicide from purchasing or possessing firearms by temporarily withholding both the firearms owner identification (FOID) card and any household firearms [47]. An emergency FRO can extend to two weeks, or the order can be expanded and filed for 6 months and extended even further if appropriate [47]. FRO policies are made at the state level, but its effectiveness in suicide prevention largely relies upon interpersonal relationships to correctly identify and swiftly act upon those at risk of suicide [49]. Public health campaigns to increase awareness and usage of FRO policies appear to have great potential to contribute to statewide suicide prevention, however clarification of FRO policies is needed. For example, clear FRO policies should outline the liability of the firearm when it is temporarily withheld from the gun owner at risk of suicide and clarify when the appropriate time is to return the firearms to the gun owner [50]. FRO policies can successfully restrict access to the lethal means of firearms from individuals at risk of suicide – public health initiatives, such as, education and increasing awareness of FRO policies, are needed to amplify the usage of this policy level suicide prevention strategy.
Increasing funding for mental health resources is another policy level approach to prevent suicide. The National Suicide Prevention Lifeline (1-800-273-8255) is a free resource available to Americans in emotional crisis and at elevated suicide risk that connects callers to mental health crisis counselors. Of the 88,615 total calls made by Illinois callers in 2018, less than 30% were answered in one of the eight call centers located within Illinois [51]. Therefore, the majority of Illinois callers experienced prolonged wait times as the calls were directed to out-of-state call centers, which could have increased the caller’s risk of dying by suicide. Currently, there are no call centers located in Madison County; however, acquiring the funding needed to open and maintain a new National Suicide Prevention Lifeline call center within the county may be warranted. A partnership with the U.S. Postal Service (USPS) could provide an avenue to both fund new call centers and raise awareness of the Lifeline resource. Similarly to the “Healing PTSD” stamps, [52] a stamp with the National Suicide Prevention Lifeline could be created, promoted, and sold at a slightly elevated cost in order to generate funding to open additional call centers. By July 16, 2022, all calls dialed to 988 in the U.S. will be directed to the National Suicide Prevention Lifeline [53]. With the shortening of the Lifeline number to 988, an increased volume of callers is anticipated [53]. Selling stamps promoting the new National Suicide Prevention Lifeline number could be a successful strategy to secure funding to open and maintain operations of additional call centers throughout the U.S., as well as provide a mechanism to increase awareness and use of the Lifeline, which could connect more individuals to mental health resources and contribute to national suicide prevention.
Conclusion
Suicide is complex and affects a vast range of individuals and communities worldwide. The trend of suicide mortality in the county of IL between the years 2008 to 2020 found in the present study displays a decrease in the number of suicide deaths each year since hitting a peak of 53 suicide deaths in 2017. Yet, there is no denying the sustained need for suicide prevention. Ample prevention methods could be adopted, including self-compassion, family interventions, pharmacy programs, resource directories, and increasing funding for mental health resources. Just as everyone has the ability to contribute to the suicide death toll, each and every person also has the ability to contribute to suicide prevention within themselves, within close relationships, and within society at large.
Conflict of interests:
The authors declare no conflict of interest.
References
Czeisler, M. E., Lane, R. I., Petrosky, E., Wiley, J. F., Christensen, A., Njai, R., Weaver, M. D., Robbins, R., Facer-Childs, E. R., Barger, L. K., Czeisler, C. A., Howard, M. E., & Rajaratnam, S. M. W. (2020). Mental health, substance use, and suicidal ideation during the COVID-10 pandemic – United States, June 24-30, 2020. Morbidity and Mortality Weekly Report, 69(32), 1049-1057. https://www.cdc.gov/mmwr/volumes/69/wr/pdfs/ mm6932-H.pdf?deliveryName=USCDC_921-DM35222View
Centers for Disease Control and Prevention [CDC]. (2018). 10 leading causes of death, United States, 2018, all ages, all races, both sexes. WISQARS. https://www.cdc.gov/injury/wisqars/ index.html View
Xu, J., Murphy, S., Kochanek, K., & Arias, E. (2020). Mortality in the United States, 2018. NCHS Data Brief No. 355. https:// www.cdc.gov/nchs/data/databriefs/db355-h.pdfView
Centers for Disease Control and Prevention [CDC]. (2018). U.S. Map of injury-related deaths. WISQARS.View
Illinois Department of Public Health [IDPH]. (2019, June). All ages suicide mortality rate by county, Illinois, 2008-2017. Suicide Prevention. http://dph.illinois.gov/sites/default/files/ publications/suicide-combined.pdfView
Hedegaard, H., Curtin, S. C., & Warner, M. (2020). Increase in Suicide Mortality in the United States, 1999-2018. NCHS Data Brief No. 362. https://www.cdc.gov/nchs/data/databriefs/ db362-h.pdfView
Centers for Disease Control and Prevention [CDC]. (2018). 2018, United States, suicide, all ages, all races, both sexes, total deaths: 48,344. WISQARS.
Li, W., Dorstyn, D. S., & Jarmon, E. (2020). Identifying suicide risk among college students: A systematic review. Death Studies, 44(7), 450-458. https://doi.org/10.1080/07481187.201 9.1578305View
American College Health Association. (2019). American College Health Association-National College Health Assessment II: Reference Group Executive Summary Spring 2019. Silver Spring, MD: American College Health Association. https:// www.acha.org/documents/ncha/NCHA-II_SPRING_2019_ US_REFERENCE_GROUP_EXECUTIVE_SUMMARY.pdfView
Hawton, K., & van Heeringen, K. (2009). Suicide. In The Lancet, 373(9672), 1372-1381. https://doi.org/10.1016/S0140- 6736(09)60372-X View
Barna, M. (2021, January). Health workers reaching patients who may have suicidal thoughts. The Nation’s Health, 27.
Haas, A. P., Eliason, M., Mays, V. M., Mathy, R. M., Cochran S. D., D'Augelli, A. R., Silverman, M. M., Fisher, P. W., Hughes, T., Rosario, M., Russell, S. T., Malley, E., Reed, J., Litts, D. A., Haller, E., Sell, R. L., Remafedi, G., Bradford, J., Beautrais, A. L., Brown, G. K., Diamond, G. M., Friedman, M. S., Garofalo, R., Turner, M. S., Hollibaugh, A., & Clayton P. J. (2010). Suicide and suicide risk in lesbian, gay, bisexual, and transgender populations: Review and recommendations, Journal of Homosexuality, 58(1), 10-51, https://doi.org/10.1080 /00918369.2011.534038 View
McClure, J. R., Criqui, M. H., Macera, C. A., Ji, M., Nievergelt, C. M., & Zisook, S. (2015). Prevalence of suicidal ideation and other suicide warning signs in veterans attending an urgent care psychiatric clinic. Comprehensive Psychiatry, 60, 149-155. https://doi.org/10.1016/j.comppsych.2014.09.010View
Ronzitti, S., Loree, A. M., Potenza, M. N., Decker, S. E., Wilson, S. M., Abel, E. A., Haskell, S. G., Brandt, C. A., & Goulet, J. L. (2019). Gender differences in suicide and self-directed violence risk among veterans with post-traumatic stress and substance use disorders. Women’s Health Issues, 29, S94-S102. https://doi. org/10.1016/j.whi.2019.04.010View
Pelkonen, M., & Marttunen, M. (2003). Child and adolescent suicide: Epidemiology, risk factors, and approaches to prevention. Pediatric Drugs, 5(4), 243-265. https://doi. org/10.2165/00128072-200305040-00004View
Yuodelis-Flores, C., & Ries, R. K. (2015). Addiction and suicide: A review. American Journal on Addictions, 24(2), 98- 104. https://doi.org/10.1111/ajad.12185View
Conner, K. R., Beautrais, A. L., & Conwell, Y. (2003). Risk factors for suicide and medically serious suicide attempts among alcoholics: Analyses of Canterbury suicide project data. Journal of Studies on Alcohol, 54(4) 551-554. https://doi.org/10.15288/ jsa.2003.64.551View
Miller, M., Barber, C., White, R. A., & Azrael, D. (2013). Firearms and suicide in the United States: is risk independent of underlying suicidal behavior? American Journal of Epidemiology, 178(6),946-955.https://doi.org/10.1093/aje/kwt197View
Goldstein, E. V., Prater, L. C., & Wickizer, T. M. (2019). Behavioral health care and firearm suicide: Do states with greater treatment capacity have lower suicide rates? Health Affairs, 38(10), 1711-1718. https://doi.org/10.1377/hlthaff.2019.00753View
Stack, S. (2003). Media coverage as a risk factor in suicide. Journal of Epidemiology and Community Health, 57. 238-240. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1732435/pdf/ v057p00238.pdfView
Stanley, B., & Brown, G. K. (2012). Safety Planning Intervention: A brief intervention to mitigate suicide risk. Cognitive and Behavioral Practice, 19(2), 256-264. https://doi. org/10.1016/j.cbpra.2011.01.001View
Rudd, M. D., Goulding, J. M., & Carlisle, C. J. (2013). Stigma and suicide warning signs. Archives of Suicide Research, 17(3), 313-318. https://doi.org/10.1080/13811118.2013.777000View
Gould, M. S., Lake, A. M., Galfalvy, H., Kleinman, M., Munfakh, J. L., Wright, J., & McKeon, R. (2017). Follow-up with callers to the National Suicide Prevention Lifeline: Evaluation of callers’ perceptions of care. Suicide and Life-Threatening Behavior, 48(1), 75-86. https://doi.org/10.1111/ sltb.12339View
Mann, J. J., & Michel, C. A. (2016). Prevention of firearm suicide in the United States: What works and what is possible. In American Journal of Psychiatry, 173(10), 969-979. https:// doi.org/10.1176/appi.ajp.2016.16010069View
Celentano, D., Szklo, M. (2019). Cross-Sectional Studies. In Gordis Epidemiology (6th ed., pp. 154). Philadelphia, PA: Elsevier.View
Creswell, J. W., & Creswell, J. D. (2018). Research Design: Qualitative, quantitative, and mixed methods approaches (5th ed.). SAGE Publications.View
Johnson, O. (2017). Suicide in St. Clair County, Illinois – 2006-16: Recommendations and strategies towards improved awareness, prevention, and intervention measures. Behavioral Health, 5(1), 1-89. View
Centers for Disease Control and Prevention [CDC]. (2018). 2018, United States, suicide – firearm, all ages, all races, both sexes, total deaths: 24,432. WISQARS.
Hayden, J. (2019). Chapter 10: Social Ecological Model. In Introduction to Health Behavior Theory (3rd ed., pp. 255-250). Jones & Bartlett Learning.View
Cramer, R. J., & Kapusta, N. D. (2017). A Social Ecological Framework of theory, assessment, and prevention of suicide. Frontiers in Suicide, 8. 1-10. https://doi.org/10.3389/ fpsyg.2017.01756View
Goldstein, E. (2016). Beyond mindfulness: The power of self-compassion, purpose, play, and confidence in the clinical treatment of the depressed client. In I. Ivtzan & T. Lomas (Eds.), Mindfulness in positive psychology. (pp. 308-320). Routledge.View
Mandhouj, O., Perroud, N., Hasler, R., Younes, N., & Huguelet, P. (2016). Characteristics of spirituality and religion among suicide attempters. The Journal of Nervous and Mental Disease, 204(11), 861-867. https://doi.org/10.1097/ NMD.0000000000000497 View
Lawrence, R. E., Oquendo, M. A., & Stanley, B. (2016). Religion and suicide risk: a systematic review. Archives of Suicide Research, 20(1), 1-21. https://doi.org/10.1080/1381111 8.2015.1004494View
Gearing, R. E., & Lizardi, D. (2009). Religion and suicide. Journal of religion and health, 48(3), 332-341. https://doi. org/10.1007/s10943-008-9181-2View
Wagani, R., & Colucci, E. (2018). Spirituality and wellbeing in the context of a study on suicide prevention in North India. Religions, 9(6), 1-18. https://doi.org/10.3390/rel9060183View
Kyle, J. (2013). Spirituality: Its role as a mediating protective factor in youth at risk for suicide. Journal of Spirituality in Mental Health, 15(1), 47-67. https://doi.org/10.1080/1934963 7.2012.744620 View
Grant, C., Ballard, E. D., & Olson-Madden, J. H. (2015). An empowerment approach to family caregiver involvement in suicide prevention: Implications for practice. The Family Journal, 23(3), 295-304. https://doi.org/10.1177/1066480715572962 View
Velasquez, M. M., Maurer, G. G., Crouch, C., & DiClemente, C. C. (2001). Group treatment for substance abuse: A Stages of Change therapy manual. The Guilford Press. View
Oka, T., Tanaka, S., Ake, H., & Kuwabara, S. (2011). Self-help groups for family survivors of suicide in Japan: For empowerment, not grief care. In Proceedings of 21st Asia-Pacific Social Work Conference (pp. 526-533View
Weiss, G. L., & Lonnquist, L. E. (2012). Complementary and alternative medicine. In The sociology of health, healing, and illness (pp. 243-271).
Chevalier, J., & Gheerbrant, A. (1996). The Penguin dictionary of symbols. Penguin books.View
McKenzie, J. F., Pinger, R. R., & Kotecki, J. E. (2002). An introduction to community health (4th ed.). Jones and Bartlett Publishers, Inc. View
Toumbourou, J. W., & Gregg, M. E. (2002). Impact of an empowerment-based parent education program on the reduction of youth suicide risk factors. Journal of Adolescent Health, 31(3), 277-285. https://doi.org/10.1016/S1054-139X(02)00384-1View
Carpenter, D. M., Lavigne, J. E., Colmenares, E. W., Falbo, K., & Mosley, S. L. (2020). Community pharmacy staff interactions with patients who have risk factors or warning signs of suicide. Research in social and administrative pharmacy, 16(3), 349- 359. https://doi.org/10.1016/j.sapharm.2019.05.024View
Morton, K.J., Harrand, B., Floyd, C. C., Schaefer, C., Acosta, J., Logan, B. C., & Clark, K. (2017). Pharmacy-based statewide naloxone distribution: a novel “top-down, bottom-up” approach. Journal of the American Pharmacists Association, 57(2), 99- 106. https://doi.org/10.1016/j.japh.2017.01.017View
The Illinois Substance Use Disorder Act, 20 ILCS § 301/5-23 Drug Overdose Prevention Program. (2019). https://ilga.gov/ legislation/ilcs/ilcs5.asp?ActID=232
Contos, P., & Tunnel, T. (2020). The firearms restraining order: A violence prevention tool for Illinois. [PowerPoint slides]. Speak for Safety Illinois. https://docs.google.com/presentation/ d/1GbivEun_z4QZ3cLr40BdwvnGVSe7Jix_NYf_s9jEVSw/ edit#slide=id.g8391296fa3_2_186View
Zeoli, A. M., & Paruk, J. K. (2019). Potential to prevent mass shootings through domestic violence firearm restrictions. Criminology & Public Policy, 19(1). 129-145. https://doi. org/10.1111/1745-9133.12475View
McCourt, A. D. (2021). Firearm access and suicide: Lethal means counseling and safe storage education in a comprehensive prevention strategy. American Journal of Public Health, 111(2), 185-187. https://doi.org/10.2105/AJPH.2020.306059View
Gibbons, M. J., Fan, D. M., & Rivara, F. P. (2020). Legal liability for returning firearms to suicidal persons who voluntarily surrender them in 50 US States. American Journal of Public Health, 110(5), 685-688. https://doi.org/10.2105/ AJPH.2019.305545 View
National Suicide Prevention Lifeline. (2019). Illinois callers to the National Suicide Prevention Lifeline. https:// suicidepreventionlifeline.org/wp-content/uploads/2019/10/ Illinois-Lifeline-2018-Report.pdf View
United States Postal Service [USPS]. (2021). Healing PTSD First Class Semipostal Stamp. https://store.usps.com/store/ product/buy-stamps/healing-ptsd-S_572104 View
Federal Communications Commision [FCC]. (2021). Fact sheet: 988 and suicide prevention hotline. FCC. https://www. fcc.gov/sites/default/files/988-fact-sheet.pdfView