
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 5 (2021), Article ID: JPHIP-186
https://doi.org/10.33790/jphip1100186Review Article
An Illustrative Review of Positional Asphyxiation in Infants Secured Upright in Car Seats
Margaret L. Alston, PT, PhD1*, Malliga Jambulingam1, Uzma Binte Haidary1, Ariel Hunt1, David Thomas1, & Yvonne Bronner1
School of Community Health and Policy - Portage Hall, Morgan State University, 4530 Portage Ave., Room 302K, Baltimore, MD 21239, United States.
Corresponding Author Details: Margaret L. Alston, PT, PhD, Assistant Professor, Morgan State University, School of Community Health and Policy - Portage Hall, 4530 Portage Ave., Room 302K, Baltimore, MD 21239, United States. E-mail: margaret.alston@morgan.edu
Received date: 11th August, 2021
Accepted date: 05th November, 2021
Published date: 08th November, 2021
Citation: Alston, M. L., Jambulingam, M., Haidary, U. B., Hunt, A., Thomas, D., & Bronner, Y., (2021). An Illustrative Review of Positional Asphyxiation in Infants Secured Upright in Car Seats. J Pub Health Issue Pract 5(2): 186.
Copyright:©2021, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Introduction
Sudden Unexpected Infant Death (SUID) includes the full spectrum of all causes of infant death, which include “Determined” causes [e.g. Sudden Infant Death Syndrome (SIDS) at 42% and Accidental Suffocation and Strangulation at 24%], as well as “Undetermined” causes at 34% [1]. Literature is replete with studies that address the risk factors associated with SIDS, accounting for at least 42% of infant mortality,[1] but scarcely do published reports address risk factors associated with Positional Asphyxia (PA).
This illustrative narrative addresses the 2.8 – 3.0% (98-105) healthy infants who have no pre-existing medical conditions, including prematurity, who die from SUID primarily in car seats, and whose suspected cause of death is PA. Webster’s Dictionary defines PA as, “A condition of deficient oxygen supply to the body which occurs when a person’s physical position prevents adequate breathing.” This tragic phenomenon is suspected when the autopsy of an infant reveals no discovery of a traumatic injury, when there is no pre-existing medical pathology, and when the cause of death is determined to be “Undetermined or Unknown.”
Although PA is less common than other causes of SUID, the mechanism by which the infant’s airway becomes occluded has been scarcely analyzed, described and published. The phenomenon of PA applies more to young infants -- less than 4 months, a critical developmental period with respect to the morphology of the spine, head and neck alignment, upper back strengthening, and notable upper airway vulnerability.
Researchers who study car seat fatalities concur that there is no increased risk of SUID for healthy infants appropriately transported in vehicles in properly-used car seats. In other words, SUID occurring in car seats is very uncommon among the population of normal infants when the infant is properly positioned and secured [2].
For decades, many well-respected pediatric authorities (e.g. United States Centers for Disease Control and Prevention; American Academy of Pediatrics; US Consumer Product Safety Commission: Children’s Products, etc.) have published guidelines for proper use of infant sitting devices [3-5].
Despite widespread instructions and guidelines for proper use of car seats by pediatricians, public health experts, and other well-respected authorities of pediatrics, such as The American Academy of Pediatrics (AAP), the amount of time that some young infants are placed in car seats far exceeds the widely publicized transportation-safety purpose for their use –which puts each infant in this population at risk for PA.
An observational study entitled “Use of Seating Devices of Infants Too Young to Sit” where surveys focused on use patterns of sitting equipment by parents of infants less than 5 months, outcomes revealed that in their sample size of 187, 94% or 176 infants spent an average of 5.7 hours per day in their car seats [4]. These findings imply that car seats are being used to position infants in places other than in vehicles. The younger the infant, and the longer the infant spends in a car seat, the more vulnerable the young infant will be to SUID given greater opportunity to faulty sustained head-neck alignment with inadequate reclining of the device. In the studies cited above, researchers concur that when infants are seated or positioned incorrectly, infant safety is notably compromised [6-10].
Use of Car Seats in the United States
In the past 25 years, it has become the practiced norm by drivers across the US to use authorized car seats for safe vehicular transport of infants under the age of 4 years, to both secure them in a safe sitting position and to safeguard them in the event of a motor vehicle accident. The US federal government allows each state to write its own laws regarding child car seat requirements. Noteworthy is that in some states –car seat laws are not as stringent as the recommendations issued by expert device manufacturers and by pediatricians [11].
In the web-based article, “Do You Know the 2020 USA Car Seat Laws for Your State and States You Visit?,” it outlines the car-seat laws for each state categorized by region [11]. Interestingly, most all states highlight: the age range for required rear-facing or front-facing, as well as height and weight requirements for booster seats, etc. None, however, address the need or importance of adequate reclining of infants. It is therefore very important for caretakers to follow manufacturer instructions which address the proper reclining method. It is also very important for caretakers to revisit the manufacturer’s instructions as the infant ages through 12 months, since proper positioning requirements change with the infant’s overall size and developmental stage.
When car seat instructions are not followed and out-of-car uses are the case, infants can succumb to accidents like: falling from a car seat that is placed on an elevated surface, flipping over the lateral sides of the device onto a soft surface (e.g. bed, sofa, plush carpet) with subsequent suffocation, or slipping under loose strap/belts to become hung by the neck and strangled to death [6,10]. Given these scenarios, “Determined” becomes the categorical cause of death given autopsy findings of: head trauma, suffocation, or strangulation respectively [6-9].
Incidence Rates of Positional Asphyxia in Infants Improperly Secured in Car Seats
In the comprehensive 2019 study by Liaw et al., whose aim was to analyze the characteristics of 11,779 sleep-related infant deaths, 348 or 3% occurred in sitting devices [9]. The majority of infants who died in a sitting device (219 of 348 or 69%) died in a car seat. The remainder (129 or 31%) died in bouncers, swings, strollers, or other sitting equipment [9].
The 3% of deaths that occur in sitting devices are consistent in other published work [8,10]. The grand majority of the 3% comprise approximately one-half of infants who: died in a car seat (vs. stroller), were less than 5 months (not including prematurity); were located in non-traveling settings; and were suspected of dying from PA with “Unknown” or “Undetermined” causes of death [6-9].
Regarding upper airway occlusion (not caused by equipment straps or belts), specific developmental and anatomic factors shall be analyzed to best understand what the infant’s positional requirements are to best ensure full airway patency in any sitting position, whether the young baby is on the lap of a caretaker or secured durable sitting device (e.g. car seat, stroller, swing, etc.).
In the aforementioned five studies, large to very large databases were investigated and published between 2007 and 2019. They addressed PA using infant death records with as well as common inclusion criteria. They were: infant age, no pre-existing pathologies (including prematurity), and no reports of trauma-caused deaths (e.g. no record of strangulation by a device belt or external neck impingement) [6-10].
Three of the above 5 studies cited a paucity of literature surrounding the mechanism of PA and physiologic explanation for the common autopsy findings of an “Undetermined” or “unknown” cause where PA was suspected. Additionally, with the tragedy of SUID occurring in car seats, accounting for 50% of deaths that occur in various sitting devices [6,7,9] it is evident that a composite presentation (outline along with illustrations) of the nature of PA is timely and proactive for the caretakers of the most innocent members of our society -- young infants. Equally important, doing so contributes not only to Public Health education, but also to the evolution of effective strategies to minimize annual SUID rates in the U.S.
Methods
Methods were largely comprised of a review of scholarly articles and texts, as well as a review of associated human anatomical and developmental images that depicting key stages of the infant (0-4 mos.) that addressed: airway and head control development, as well as milestone skills that contribute to the transition of the spine from a C-shape to the mature S-shape. Through description and images, these factors were presented in an integrated fashion over the 0-4 month period of the young infant who are vulnerable to varying degrees of PA given faulty upright positioning against gravity. Once this material was outlined and diagrammed based on chronological developmental sequence, findings were that the young infant’s airway can be partially to completely compromised to normal airflow given prolonged neck flexion with subsequent folding of the upper airway on itself given the weight of the head, the location and cellular properties of the larynx.
Developmental Factors that Contribute to Positional Asphyxia in Upright Positioned Infants
Neutral alignment of the infant head and neck is essential to optimize the patency or degree of openness of the upper airway. Positioning recommendations that follow have as their basis simple explanations involving the mechanical interrelationships between the spine, hips, and pelvis that together impact the position of the head and neck – critical in the discussion of airway patency or respiration safety. The requirement of head and neck alignment --where there is an absence of neck flexion (forward bending) and extension (backward bending) are unequivocally essential for safe positioning in car seats and all other sitting devices.
First, it is important to first visualize or illustrate an infant improperly positioned infant in a car seat –who is at risk for PA, contrasted by an infant properly positioned. (Figure 1: Position A & B). Given these images that differ relative to head and neck alignment, it is important to appreciate that when pliable mucosal tissues of the upper airway are permitted to fold, airway patency will be reduced or obliterated, thus disrupting normal air flow or breathing.
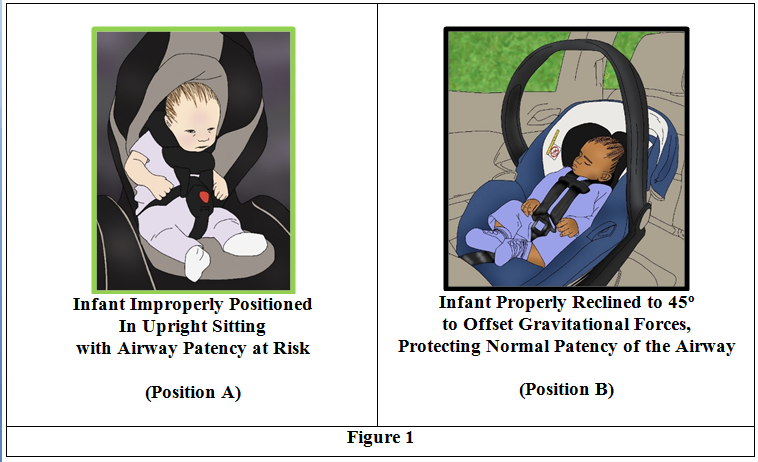
Figure 1:
Three Anatomical and Developmental Factors Hypothesized to Cause Positional Asphyxia
The triad (3) of key anatomical and developmental factors that when superimposed or occurring together make especially the young (<5 mos. of age) infant’s airway vulnerable to airway obstruction when seated in the upright or vertical position.
They are: 1. The C-shaped rounded spine (in the sagittal plane or when viewed from the side) along with a posteriorly-tilted pelvis.
2. Inadequate head control. Given its weight at approximately 25-30% of the full body weight and underdeveloped neck and upper back strength, the infant struggles to control its head position against the force of gravity.
3. The tissue properties of the larynx within the upper airway, causing it to be very deformable. Additionally, its superior location at the level of the lower jaw or mandible, and its conical shape make the laryngeal organ complex in cellular and structural make-up, and very vulnerable to occlusion –when ‘folding” forces impact the pliable structures.
1. The C-Shaped Rounded Spine of the Young Infant
With normal prenatal development, the embryonic spine is C-Shaped in the sagittal plane [12]. The sagittal plane divides right and left sides, as one of three spatial planes. The C-shaped spine persists from the fetal period (10 weeks gestation) through birth and very early infancy (1-2 mos.) [12]. Additionally, the rounding of the spine at the rump contributes to the spine’s C-shape, which is in part due: to the winged-shape of the pelvis [13] and the rounding external forces directed to the spine from the mother’s strong uterine and abdominal walls.
The infant’s progressive motor development, beginning especially in the 3rd month, helps to transform the immature convex C-shaped spine to the mature adult-like S-shape [14]. New secondary concave curves begin with the cervical spine initiated with neck extension during supervised prone “tummy times” in early infancy. The second secondary curve emerges in the lumbar region once the infant begins to circle-sit (e.g. soles of feet face themselves) while propping onto palms with outstretched arms at 5-6 months [12]. The mechanics of these complimentary curves help bring the pelvis to a more neutral tilt (e.g. not tipped backward or forward) in the horizontal plane –the spatial plane that divides top from bottom. These curvature changes help elongate and create vertical balance of the now “S-shaped” spine comprised of the cervical, thoracic, lumbar, and sacral-coccygeal segments (Figure 2). The head is more balanced atop the cervical spine and aligned with the vertical axis of the spine –without the need for much muscular effort to maintain its upright position when the infant is alert. As purported by Gerber et al. (2010), the evolved complementary spinal curves help to reduce the vulnerability of the upper airway from mechanical occlusion, since the neck is more elongated, [13] with the head being less at risk for falling forward into gravity-assisted flexion.
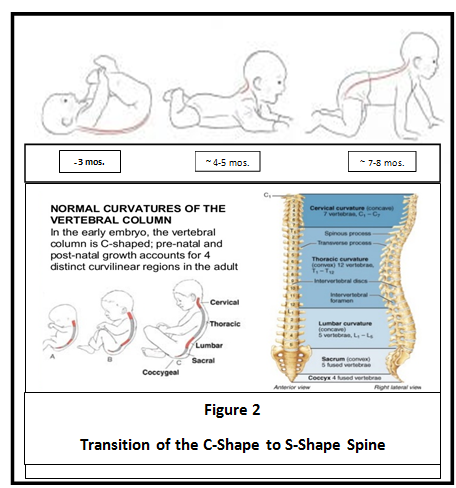
Figure 2:Transition of the C-Shape to S-Shape Spine
2. Inadequate head control
Inadequate head control of the young infant against gravity is due in part to antigravity strength incompetence of the posterior neck and upper back muscle groups, especially in the first 3-4 months. Additionally, the aforementioned C-shaped spine, with the posteriorly tilted pelvis, plays a notable role in fostering the “head forward” with neck flexion position. Normal nurturing, which includes handling and placing the infant in various positions help foster independent head control in supported sitting around the 6th month of normal development [15]. The progressive strength balance of flexor and extensor muscle groups about the neck and upper back beginning when the young infant is regularly supported against the chest of an upright caretaker, and when active in the supervised tummy position (2-4 months of age). Both opportunities are key in helping the developing baby to lift and independently control its head against gravity.
Of paramount importance is the realization of what happens to the upper airway –naturally in the young infant (< 4 mos.) when placed in upright sitting (Figure 3). The weight of the head along with the downward force of gravity – combined with a rounded spine mechanically puts the infant’s head forward of the upper body’s center of mass. These factors together cause uncompensated or uncontrolled neck flexion. This scenario maintains the head in a forward and downward position. If sustained, the neck flexion imparts a “folding or collapsing force” on the upper airway, causing airway occlusion with the risk of PA and SUID (Figure 3).
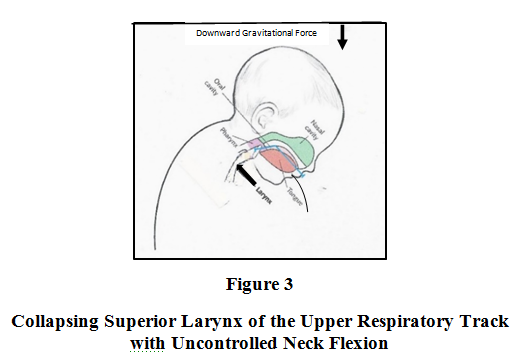
Figure 3:Collapsing Superior Larynx of the Upper Respiratory Track with Uncontrolled Neck Flexion
Around the 4th month of age, active muscle efforts around the spine, neck, chest, and abdomen occurring from the prone position helps midline regard and right/left symmetry to emerge. This phase of development is key for the emergence of independent antigravity head control [15]. Centered head control is assisted when the forearms push against a supportive surface [16]. In keeping with the normal developmental progression, core or axial component parts (e.g. head, neck, and spine with trunk) mature before the more distal or peripheral segments. In the infant who is being handled and stimulated in all positions when alert, the axial development of the muscles about the neck and upper trunk becomes stronger, balanced, and able to work with competence against the downward force of gravity within the first 4-5 months. The importance of this order of developmental events is that the older infant (> 4 mos.) can better steady its head upright and is less vulnerable to uncontrolled neck flexion and airway constriction. Upper airway occlusion is therefore no longer a high risk in the older infant who is alert and in supported sitting.
3. Upper Airway Properties
The third developmental factor specifically addresses the laryngeal complex of the upper airway. Its high (superior) location in the neck- - which approximates the C3 and C4 cervical vertebrae levels, along with its cellular pliability, and its conical shape puts the larynx, in the upper respiratory tract, at risk for occlusion given maximal and sustained neck flexion (Figure 3). The cellular make-up of the larynx is diversified, due to its varying degrees of elastic tissue that span the length of the organ. Additionally, the 7 cartilaginous structural regions that provide its composition, and its ellipsoid or conical shape contribute to its complexity [17].
The significance of its conical shape is that the least stable or most pliable aspect is closest to the most superior aspect of the upper airway-- close to the infant’s jawline, where occlusions occur. In contrast, the most stable or least pliable aspect is distal or furthest away from the top of the airway, near the transition to the trachea-- the anatomical segue to the lung’s main bronchus.
The Oct. 2017 article entitled, “The Anatomy of the Pediatric Airway: Has our Knowledge Changed in 120 Years” [17] confirmed that the laryngeal organ complex has the three main functions: safe swallowing (given its epiglottal folds) at the upper end, sound production (given the V-shaped vocal cords), and respiration (air exchange to/from the lungs). The various cartilaginous types are mucosa-covered, highly deformable and flexible [17] and able to withstand repeated bending and rebounding dynamics, just as other bodily structures made of elastic cartilage are capable of.
It should be reiterated that the most vulnerable developmental stages of the larynx are greatest in the young infants (less than 5 mos.), which is coincident with the population of infants who succumb most to PA in the upright seating position. In keeping with the discussion of developmental maturation, there becomes greater histologic stability (less flexibility) of the upper airway region as the infant ages to childhood [18]. For example, a 3-year-old child can better withstand deformable forces of neck flexion because of their more mature histological or tissue make-up, and additionally since the laryngeal complex in the respiratory track shifts to a lower position by toddlerhood [19].
Results
Developmental and position-based evidence reveals that the immature conditions of the cervical spine shape; muscular weakness about the neck and upper back; cellular properties, location, and shape of the upper airway all together contribute to the vulnerability for upper airway occlusion in especially young infants when the head falls forward and the neck is maintained in flexion. This high-risk life-threatening scenario is fostered by improper vertical-sitting positioning (Figure 1; Position A).
Also highlighted is that older infants (5-11 months) are also at risk for PA when they fall asleep in the upright position in a car seat or stroller, given neck and upper back muscle inactivity that permits gravity to maintain the head in the forward and lowered position. The same anatomical and mechanical mechanism that constricts the airway in young infants can impact the older sleeping infant. In the alert state, strong upper back and neck extensor muscles would otherwise maintain the head upright, rendering the patency of the upper airway open.
The interrelated factors causing younger infants to be most vulnerable to PA compared to older infants as well as young children have been enumerated and illustrated in Graph 1. There is an indirect relationship between an infant’s age and the magnitude of elasticity or deformability of the upper airway. As the baby ages, progressive maturation of the laryngeal complex, including declining pliability, takes place which helps to protect the airway from the risk of deformable forces. In contrast, spinal curve maturation and head control have a direct relationship with the aging infant. They increase and mature together.
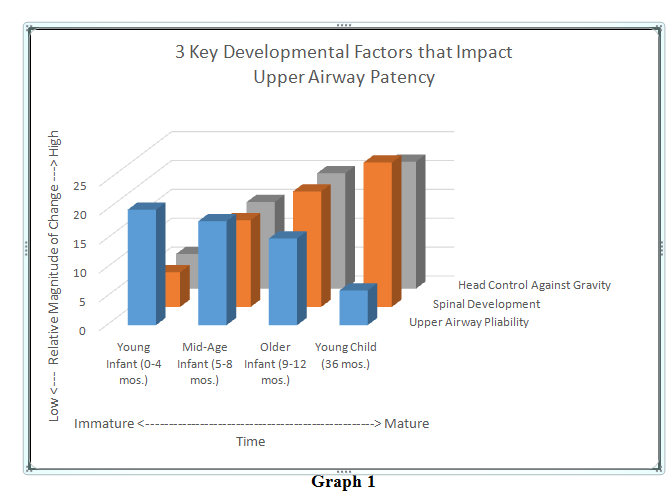
Graph 1
Discussion
The root cause or reason for the “Undetermined” or “Unknown” post-autopsy cause of death finding when PA is suspected is most likely that the spring-back resilience of the elastic cartilage structures making up the laryngeal complex permit the organ to resume its original conical shape once the compressive folding forces are reversed or removed. Return of the original cylindrical and ellipsoid shape would be expected along with normal airway patency once gravitational forces that caused neck flexion are removed. Upper airway structures, therefore, would spring back to their normal shapes even in the post-mortem state once the neutral position of the head and neck are restored in the autopsy position of supine.
Given this, there would be no expected physical evidence of upper airway occlusion. One wouldn’t expect that there would be any observable structural abnormalities, trauma-based tissue disruption, external bruising, or evidence of airway occlusion. For all that, anautopsy would reveal no definitive cause of death upon gross examination. The merit of this hypothesis is based on the widely-accepted cellular and mechanical properties of elastic cartilage. They allow the tissue to behave in resilient ways given action/reaction and force-couple principles.
Recommendations for Infant Airway Protection:
Though proper handling of infants most always occurs instinctively or naturally. However, due to the existing 3% incidence rate of PA, heightened awareness about the importance of neutral alignment of the infant’s head and neck by caretakers is indicated. Alignment in the young infant is best facilitated by external support –to include: the palm of the caretaker’s hand when the infant is held upright, the crook of the elbow when infant is cradled, the firm mattress during “back to sleep” slumbering, and the reclined car seat in-car use. Additionally, it is very important to follow the manufacturer’s seating device instructions, which includes adjustments as the infant ages.
Car Seat Positioning Recommendations – For PA Prevention:
1. Semi-recline the backward-facing car seat to approximately 40- 45 degrees for all infants (0-12 mos.) whether awake or asleep, while ensuring that the head and neck alignment is in neutral, checked in all 3 spatial planes. That is, ensure that the neck is not in: forward flexion, backward extension, extreme rotation (right/left), or extreme side bending (right/left); (Figure 1: Position B).
Following these guidelines will best ensure that neck flexion will not occur –whether the infant is awake or asleep, and that neutral alignment of the head and neck will be preserved to best ensure normal airway patency.
2. The adequate angle of recline will differ slightly among infants of varying ages. The ultimate aim is to ensure neutral alignment of the head and neck to protect the upper airway. Even when a tilt gauge is built into the sitting device, normal head and neck alignment will be ultimately visually assessed.
3. Have knowledge of the infant’s age and refer to the device’s instructions with regularity --since the age will correlate with proper use and adjustment recommendations by the car seat’s manufacturer.
4. Soon after purchase of the device, register the device online, including an active email address, so that Inbox notification of any consumer alerts or recalled parts/devices can occur.
5. When choosing an infant in a car seat for proper positioning:
• Ensure that the seat width allows for adequate spreading of the thighs with outward rotation of the hips so that the pelvis can be maintained in neutral (e.g. not tilted backward or forward)/ (Figure 1; Position B). This position helps the spine to maintain the mature elongated S-shape, allowing the baby to control its head in neutral and in midline to withstand uncontrolled neck flexion.
• Parents and caretakers should take care to use car seats and other sitting devices for their original and recommended use, since doing otherwise can introduce significant safety risks to the infant, which could result in injury or SUID [20].
• All sleeping infants should be removed from their car seat or other sitting devices as soon as is plausible and laid down on their back (e.g. infants less than 7 months) in a safe-sleep crib, bassinet, transportable bed, etc.
Suggested Sources of Information About Infant Safety and Equipment:
a) https://www.cdc.gov/motorvehiclesafety/child_passenger_safety [CDC: Motor Vehicle & Child Passenger Safety]
b) https://www.cdc.gov/injury/features/child-passenger-safety [CDC: Child Passenger Safety Guidelines]
c) https://www.nhtsa.gov [National Highway Traffic Safety Administration]
d) https://www.safekids.org [Safe Kids Worldwide]
e) https://www.nsc.org [National Safety Counsil]
f) https://bestcarseathub.com/blog/usa-car-seat-laws-2020 [2020 USA Car Seat Laws for Your State]
g) https://www.cpsc.gov [Consumer Protection Safety]
Competing Interests:
The authors assert that there are no conflicts of interest.
List of Abbreviations
AAP - American Academy of Pediatrics
SIDS - Sudden Infant Death Syndrome
SUID - Sudden Unexpected Infant Death
PA - Positional Asphxia
Acknowledgements:
The authors thank reviewers: Colleen Wilburn (Maryland Department of Health); Dr. Beverly Tyler (Potomac Pediatric Physicians, Bel Air, MD); Jay Alston (Towson University: School of Art & Design, Towson, MD)
Funding Source:
Maryland Department of Health. BPO/PO: M00B9400330
References
National Center for Health Statistics. https://www.cdc.gov/nchsView
Batra, E., Midgett, J. & Moon R. (2015). Hazards Associated with Sitting and Carrying Devices for Children Two Years and Younger. The Journal of Pediatrics, 167(1): 183-187.https://doi. org/10.1016/j.jpeds.2015.03.044View
United States Center for Disease Control and Prevention. https://www.cdc.gov/grand-rounds/pp/2018/20181023-sudden-infant-deathView
The American Academy of Pediatrics. https://www.aap.orgView
United States Consumer Products. https://www.cpsc.govView
Bamber, A., Pryce, J., Ashworth, M., & Sebire, N. (2014). Sudden Unexpected Infant Deaths Associated with Car Seats. Forensic Sci Med Pathol, (10): 187-192.View
Cote, A., Bairam, M., Deschenes, M., & Hatzakis, G. (2008). Sudden Infant Deaths in Sitting Devices. Arch Dis Child (93): 384-389. DOI: 10: 1136/adc.2007.119180View
Freyne, B., Hamilton, K., Garvey, C., Matthews, T., & Nicholson, A. (2014). Sudden Unexpected Death Study Underlines Risks of Infants Sleeping in Sitting Devices. Acta Paediatrica, 103(3): 130-2.
Liaw, P., Moon, R., Han, A., Colvin, J. (2019). Infant deaths in sitting devices. Pediatrics, 143 (6):1-7. https://doi.org/10.1542/ peds.2018-2576View
Kassa, H., Moon, R., & Colvin, J.D. (2016). Risk Factor for Sleep-Related Infant Deaths in In-Home and Out-of-Home Settings. Pediatrics, 138(5): 1-6.View
Do You Know the 2020 USA Car Seat Laws for Your State and States You Visit? https://bestcarseathub.com/blog/usa-car-seat-laws-2020View
Bess, S., Varma, V. (2011). Embryology and Anatomy: Spine/ Spinal Cord, Springer-Verlag Berlin Heidelberg.View
Delaere, O., Dhem, A. (1999), Prenatal Development of the Human Pelvis and Acetabulum, Acta Orthopaedica Belgica, 65(3): 255-60.View
Gerber, R.,Wilks, T., Erdie-Lalena C. (2010). Developmental Milestones: Motor Development. Pediatrics in Review, 31(7): 267-277. DOI: https://doi.org/10.1542/pir.31-7-267.View
Alexander, R., Boehme, R., Cupps, B. (1993). Normal Development of Functional Motor Skills: The First Year of Life. Hammill Institute.View
Siddicky, S., Bumpass, D., Krishnan, A., Tackett, S. McCarthy, R., Mannen, E. (2020). Positioning and Baby Devices Impact Infant Spinal Muscle Activity. Journal of Biomechanics, (7)104. https://doi.org/10.1016/j.jbiomech.2020.109741.View
Holzki, J., Brown, K., Carroll, R., Coté, C. (2018). The Anatomy of the Pediatric Airway: Has Our Knowledge Changed in 120 Years? A Review of Historic and Recent Investigations of the Anatomy of the Pediatric Larynx. Pediatric Anesthesia, 28(1): 13-22. DOI: 10.1111/pan.13281.View
Yonekawa, S., Fukunaga, H., Umeno, H., Mori, K., Nakashima, T. (2000). Subglottic Airway Becomes Stable with Age in the Human Infant Larynx. Acta Oto-Laryngologica, 120(3):444- 449. DOI:10.1080/000164800750000711View
Xi, J., Si, X., Zhou, Y., Kim, J., Berlinski, A. (2014). Growth of Nasal and Laryngeal Airways in Children: Implications in Breathing and Inhaled Aerosol Dynamics. Respiratory Care, 59(2): 263-273. DOI: https://doi.org/10.4187/respcare.02568View
Callahan, C. & Sisler, C. (1997). Use of Seating Devices in Infants Too Young to Sit. Arch Pediatr Adolesc Med, 151(3): 233-235. DOI:10.1001/archpedi1997.02170400019004View