
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 5 (2021), Article ID: JPHIP-187
https://doi.org/10.33790/jphip1100187Research Article
COVID-19 Mortality, Diabetes, and Obesity: The Impact of Health Inequity
Peter J. Fos, Ph.D., D.D.S.1*, M.P.H., Peggy Honoré2, Katrina Kellum3
1Professor of Health Sciences, Dillard University, Minority Health and Health Disparities Research Center, 2601 Gentilly Blvd. New Orleans, LA 70122, United States.
2 Professor, LSU Health Sciences Center, School of Public Health, Department of Health Policy and Systems Management, School of Medicine, United States.
3College of Nursing, Dillard University, United States.
Corresponding Author Details: Peter J. Fos, Ph.D., D.D.S., M.P.H., Professor of Health Sciences, Dillard University, Minority Health and Health Disparities Research Center, 2601 Gentilly Blvd. New Orleans, LA 70122, United States. E-mail: pfos@dillard.edu
Received date: 18th October, 2021
Accepted date: 09th November, 2021
Published date: 11th November, 2021
Citation: Fos, P. J., Honore, P., & Kellum, K. (2021). COVID-19 Mortality, Diabetes, and Obesity: The Impact of Health Inequity. J Pub Health Issue Pract 5(2): 187.
Copyright:©2021, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Early in the COVID-19 pandemic, minorities experienced the greatest burden of infection and death. These disparities were studied and related to the disproportionate distribution of comorbidities among minority, especially diabetes and obesity in non-Hispanic Blacks. Additionally, health equity has been linked to health disparities of chronic disease and COVID-19 infection. The same effect of the social determinants of health on chronic diseases in minorities is now seen in the COVID-19 pandemic. This study, which is a follow-up of research in the early stages of the pandemic, is focused on determining if the disparity in mortality is still present in the second year of the COVID-19 pandemic. Data were collected for state health departments in Georgia, Louisiana, Michigan and Mississippi on mortality due to COVID-19 infection. Mortality and case-fatality rates were collected for each state and selected counties in the study states. Mortality and case-fatality rates were determined according to race, comparing non-Hispanic Whites with non-Hispanic Blacks. The prevalence of diabetes and obesity was evaluated in relation to mortality and case-fatality rates. Results of this study indicate that the disparity between non-Hispanic Whites and non-Hispanic Blacks continues to be observed in the second year of the COVID-19 pandemic. Non-Hispanic Blacks, in the study states and counties, have higher mortality and case-fatality rates than non-Hispanic Whites. This difference ranges from nearly 1.2% greater in Georgia to 71% greater in Michigan. In the study counties with diabetes prevalence of ≥12.0% and obesity prevalence of ≥38.0% had the highest mortality rates. This study indicates that the effect of health inequities must be addressed for both chronic diseases and COVID-19.
Keywords: COVID-19, Diabetes, Obesity, Mortality Rates, Case-Fatality Rates, Health Inequity, Health Disparities.
Introduction
Previous research has established a linkage between chronic conditions, especially diabetes and obesity, with COVID-19 infections, hospitalizations, and deaths. One study presented the argument that COVID-19 was an infectious disease health disparity [1]. This paper describes a follow-up study, which was conducted early in the pandemic, of the relationship between the relationship between diabetes and obesity and COVID-19 deaths. A question is why does this health disparity exist?
What has been learned during the COVID-19 pandemic is the effect of comorbidities on mortality. Hypertension, diabetes, obesity, and several other chronic conditions increase the risk of death if infected by COVID-19. This is particularly the case with obesity. Someone who is obese has an increased risk of COVID-19 infection, hospitalization and death [2]. It is estimated that over 40% of adults in the US are obese, and the percentage continues to increase [3-4]. Nearly 20% of children in the US are obese [5]. The prevalence of obesity is disproportionally higher in Blacks, and is an example of the impact of structural racism [6].
Studies have shown the prevalence of obesity and type 2 diabetes continues to increase in the United States, and worldwide. This increase is particularly seen in lower-income individuals [7]. Hypertension prevalence in these subpopulations is increasing at a greater level [8]. To better understand the distribution of diabetes screening across the United States, a cross-sectional analysis was conducted [9]. The analysis evaluated diabetes screening on a national, regional, and state levels. One objective of the analysis was to determine if racial disparities affected screening. The distribution of diabetes across the United States is not random, but the prevalence is higher in non-Hispanic Blacks and American Indian/Alaska Natives. Diabetes screening is lower across all racial groups compared to non-Hispanic Whites [10]. The study found a racial disparity in diabetes screening but could not explain these differences in screening across races.
For the past several decades there has been an emphasis on health equity to explain health disparities. A health disparity is worse health among disadvantaged racial/ethnic groups who are at an economic and social disadvantage [11]. The focus has been on the social determinants of health and the reduction of health inequities. Health inequities are a result of avoidable social injustice. These health inequities have been linked to differences in social, economic, and resource situations between subpopulations. The impact of health inequities can be addressed upstream by mitigating the negative effects of social determinants of health [12-13].
Health equity denotes striving for the best possible health for all people. The exact meaning of health equity has not gained consensus, but it has been defined in four ways: equal utilization, distribution according to need, equal access, and equal health outcomes [14]. Another definition of health equity is having a fair and just opportunity to be healthy. A result of health inequities is health disparities which have been linked to structural racism and, if addressed, are preventable [15]. Health equity is a concern in the U.S. and in other parts of the world. Global health inequities have been defined as systematic differences in health across countries, which are preventable [16]. In developing countries these inequities are very apparent in children’s health [17]. As may be expected there is a great deal of variation in health inequities worldwide [18].
A study of the effects of socioeconomic factors on the risk of COVID-19 in minorities with chronic liver disease had several interesting findings. This prospective study found that non-Hispanic Blacks, as well as Hispanics, were less likely to have private insurance; these groups had a higher likelihood to have Medicare and Medicaid, or no health insurance.
Additionally, non-Hispanic Blacks were more likely to live in multi-family housing, with more than 5 family members. Finally, the study found that non-Hispanic Blacks were more likely to low in low household income neighborhoods [19].
It is important to note that health disparities are preventable, systematic, and are prevalent in socially, geographically, or economically disadvantaged groups of people [20]. These disadvantages affect specific subpopulations, defined according to race, ethnicity, age, social orientation, and other characteristics [21]. Understanding the linkage between the social determinants of health and health disparities is important to addressing urgent health equity, such as in the COVID-19 pandemic. After more than a year of the COVID-19 pandemic it is now clear that cases and deaths are not randomly distributed in the population. This has been particularly the case in the United States, as well as over areas of the world. Globally, the health of migrants, indigenous populations, and racial and ethnic minorities has been adversely affected by the COVID-19 pandemic [22].
Recently, the director of the U.S. Centers for Disease Control and Prevention stated racism is a serious public health threat. In a released statement the Director discussed the effect of pre-existing inequities on health, in general, and on COVID-19 cases and deaths among racial minorities. Racism is outlined as more than discrimination against a group of people, but is those structural racial barriers which have influenced the lives and health of minorities differently from Whites. The resulting social determinants of health have had a detrimental effect on health among minorities for generations [23].
Structural racism (also called systemic racism) can be defined as “the processes of racism that are embedded in laws (local, state, and federal) policies, and practices of society and its institutions that provide advantages to racial groups deemed superior, while differentially oppressing, disadvantaging, or otherwise neglecting racial groups viewed as inferior [24]. Structural racism is a complex system which ultimately classify groups into social hierarchies. In fact, structural racism is a driver of health disparities among racial and ethnic groups [25].
This study attempts to explain the differential of COVID-19 deaths across racial minorities. This study is follow-up research that has that COVID-19 is an infectious disease health disparity. This disparity is closely associated with the major COVID-19 comorbidities, such as hypertension, diabetes, obesity and cardiovascular disease. The prevalence of the major comorbidities are most prominent in racial minorities, especially African Americans [1].
Materials and Methods
The number of COVID-19 deaths, since the beginning of the pandemic, were obtained from various data sources, including the Centers for Disease Control and Prevention (CDC), the Alabama Department of Health, the Georgia Department of Health, the Louisiana Department of Health, the Mississippi Department of Health, and the Michigan Department of Health. Population estimates were obtained from the U.S. Census Bureau.
Overall mortality rates were calculated for the US and study states. The rates of the study states were compared to the US. Additionally, mortality rates were calculated for non-Hispanic Whites and non-Hispanic Blacks in the study areas. Racial comparisons were determined for all study areas. The age distribution across states was not available, so age adjusted rates were not attempted. Comparison of the rates was accomplished to identify any differences.
Case-fatality rates were calculated to illustrate the severity of COVID-19 across the different study areas.
Diabetes prevalence data were acquired from the CDC’s United States Diabetes Surveillance System. Data were age-adjusted percentage of adults 18 years and older with diagnosed diabetes. Obesity data were acquired from the Center for Disease Control and Prevention. Data were the percent of adults aged 18 years and older who have obesity. Obesity was defined as body mass index (BMI) ≥ 30.0. The source of obesity data was the Behavioral Risk Factor Surveillance System.
Results
Table 1 presents data for the U.S. and the study states, and selected counties. The overall mortality rate from COVID-19 in the U.S. is 214.95 deaths per 100,000 population. Alabama, Louisiana, and Mississippi have higher COVID-19 mortality rates than the U.S. Compared to the U.S., Alabama’s COVID-19 mortality rate is 19.60% higher, Louisiana’s COVID-19 mortality 30.1% higher, and the Mississippi COVID-19 mortality rate is 39.20% higher. This is not the case in Georgia and Michigan. However, one county in Georgia and two counties in Michigan have higher mortality rates than the U.S. Dougherty County Georgia has a COVID-19 mortality rate that is 84.6% higher than the mortality rate in the U.S. When compared to the U.S., Macomb County Michigan’s mortality rate is 36.3% higher and Wayne County’s mortality rate is 41.6% higher.
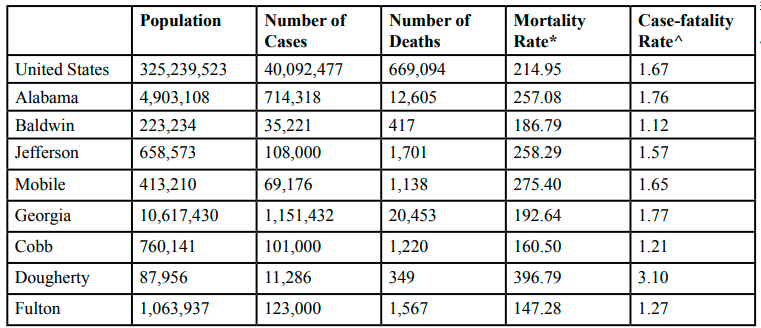
Table 1 COVID-19 Mortality, by State and County
The case-fatality for the U.S. is 1.67%, which indicates that nearly 2% of cases of COVID-19 results in death. Compared to the seasonal influenza which has on average a case fatality rate far less than 1%, COVID-19 is over six times more deadly [38]. The case-fatality rate is higher in every state compared to the U.S. Mississippi, with a case-fatality rate of 1.93, is the highest among the study states. Dougherty County’s case-fatality rate is over 3%, which is the highest among counties. Wayne County (2.96%), St. John the Baptist Parish (2.60%), Macomb County (2.35%), and Orleans Parish (2.10%) have case-fatality rates greater than 2 percent.
COVID-19 cases and mortality, according to race, is presented in Table 2. In each study state the percent of COVID-19 cases are higher in non-Hispanic Whites. In the U.S., 60.1% of cases are among non-Hispanic Whites. In Michigan, nearly three-fourths of cases are among non-Hispanic Whites. In all other states over 60% of cases are among non-Hispanic Whites. This same finding is seen in the number of COVID-19 deaths. The number of deaths is greater among non-Hispanic Whites than non-Hispanic Blacks. These case percentages and number of deaths are due to the fact than more non-Hispanic Whites live in the U.S. and study states than non-Hispanic Blacks.
However, the mortality rates are higher in non-Hispanic Blacks. This is the case in the U.S. and all the study states. The greatest percent difference is seen in Michigan where the mortality rate for non-Hispanic Blacks is 71.6% higher than in non-Hispanic Whites. The percent difference for the U.S. is 11.2% higher in non-Hispanic Blacks. Georgia has the lowest percent difference, 1.2% higher in non-Hispanic Blacks.
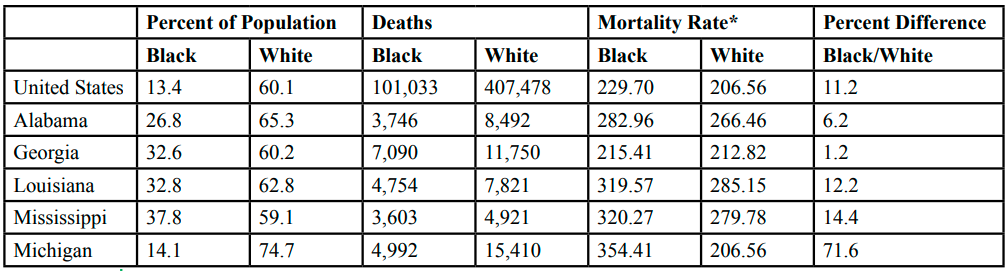
Table 2 COVID-19 Mortality Rate, by Race, by State
Table 3 shows diabetes and obesity prevalence in the U.S. and the study states and counties. The prevalence of diabetes in the U.S. is 9.6% of adults 18 years of age and older. The prevalence in diabetes is much higher in the study states. The highest diabetes prevalence of 14.0% is seen in Louisiana. This is 45.8% higher than in the U.S. The percent difference compared to the U.S. ranges from a high of 45.8% to a low of 13.5% in Michigan. In reviewing the study counties two counties have a diabetes prevalence greater than 14 percent; Dougherty County (17.0%) and Mobile County (15.0%).
Obesity prevalence in the U.S. is 41.2% of adults aged 18 years and older. Mississippi has an obesity prevalence equal to 40.8%, with the remaining states having an obesity prevalence between 33.1% and 36.1 percent. Two counties have an obesity prevalence greater than 40 percent; St. John the Baptist Parish (48.0%) and Hinds County Mississippi (41.0%). Several counties have obesity prevalence greater than 35.0. percent. These counties are Dougherty County (39.0%), Jackson County (39.0%), and Mobile County (38.0%).
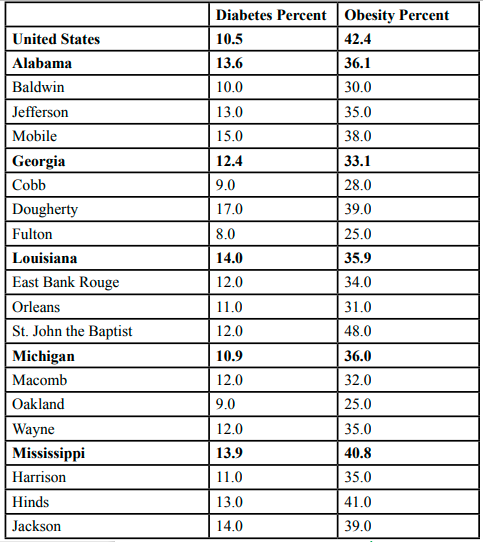
Table 3Diabetes and Obesity Prevalence, by State, and County
Table 4 shows the relationship between COVID-19 mortality, case-fatality and diabetes and obesity prevalence. One county for each study state was selected. Mobile County has a mortality rate of 275.40 deaths per 100,000, a case-fatality rate of 1.65% and a 15.0% diabetes and 38.0% obesity prevalence. Dougherty County has a COVID-19 mortality rate of 396.79 deaths per 100,000, a case-fatality rate of 3.10% and a 17.0% diabetes and 39.0% obesity prevalence. St. John the Baptist Parish has a COVID-19 mortality rate of 364.17 deaths per 100,000, a case-fatality rate of 2.60% and diabetes and obesity prevalence of 12.0% and 48.0%, respectively. Wayne County has a case-fatality rate equal to 2.96%, a mortality rate of 304.51 deaths per 100,000, and a 12.0% diabetes and 35.0% obesity prevalence. Hinds County has a mortality rate of 245.00 deaths per 100,000, a case-fatality rate of 1.87% and a 13.0% diabetes and 41.0% obesity prevalence.
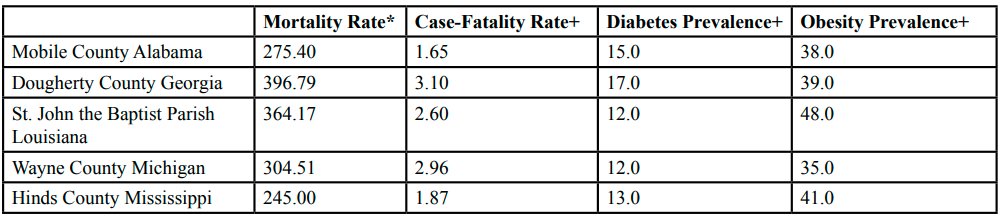
Table 4Mortality, Case-Fatality, Diabetes and Obesity Prevalence, Selected Counties
Discussion
The effects of structural racism were examined within areas of the United States on COVID-19 mortality. This study has illustrated the results of the absence of health equity on mortality, especially as it affect chronic disease prevalence, specifically diabetes and obesity. It is apparent that COVID-19 mortality has exposed the significant health inequities experienced racial minorities. The basis for these inequities is structural racism which has resulted in social injustices, highlighted by the social determinants of health. The lack, and inadequate, upstream social and health policies over the past several decades is a root cause of the disparity in COVID-19 mortality. The policy shortcomings have affected those marginalized subpopulations who have high rates of poly-chronic diseases [26].
The effect of health inequities among racial minorities is also seen in other areas in the world. Anti-Black racism in Canada has resulted disproportionate COVID-19 infection in Black Canadians [27]. The impact of racism is realized in stereotyping and provider bias [28]. Racism has impacted health in Europe. The fear of racism has a negative effect on health outcomes across gender and age [29]. Blacks are less likely to receive a kidney transplant than Whites [30]. An inimical effect of racism in Europe was a lack of adherence to treatment protocols, treatment compliance, as well as delay in receiving adequate, quality health care [31].
This study has illustrated the effect of health inequities on COVID-19 mortality. This study corroborates the previous research showing that COVID-19 is, indeed, and infectious disease health disparity. Three of the study states have higher COVID-19 mortality rates than the U.S. Additionally, all study states have higher case-fatality rates than the U.S. Even in the two states with a lower COVID-19 mortality rate, there are counties with mortality rates much higher than for the U.S. The same is seen with case-fatality rates. In fact, a few counties have case-fatality rates at or near 3%, which is over 75% higher than for the U.S.
The racial difference is strikingly obvious when COVID-19 mortality is stratified by race. In the U.S. the mortality rate among non-Hispanic Blacks is 11.2% higher when compared to non-Hispanic Whites. In Mississippi and Louisiana, the mortality rate among non-Hispanic Blacks is more than 10% higher than for non-Hispanic Whites, 14.4% and 12.2% respectively. The greatest difference in COVID-19 mortality between races is seen in Michigan, where the death rate for non-Hispanic Blacks is 71.6% higher when compared to non-Hispanic Whites.
It is interesting to note that counties with high COVID-19 mortality rates have high diabetes and obesity prevalence. For example, this is shown in Dougherty County, Georgia which has a COVID-19 mortality rate of 396.79 deaths per 100,000, a case-fatality rate of 3.1%, as well as a diabetes and obesity prevalence of 17.0% and 39%, respectively. It is interesting to note that when examining U.S. Census data for Dougherty County dramatic racial differences can be seen in lack of health insurance, median household income, poverty, percent change in employment, and per capita income. Another example is St. John the Baptist Parish, Louisiana which has a mortality rate of 364.17 deaths per 100,000, a case-fatality rate of 2.6%, a diabetes prevalence equal to 12.0%, and an obesity prevalence of 48.0 percent [32].
The health disparities exposed in this research can be directly linked to theories of how the social determinants of health (SDOH) impact the health of individuals and populations. The relationship between SDOH and health outcomes is indeed complex, and should be examined from a systems science approach to better understand the interrelationship between all relevant factors (e.g., community environment, socioeconomic conditions, behaviors, etc.) that must be considered when determining what influences specific health outcomes [33]. Even when considering linkages to chronic conditions as a contributing factor for poor health outcomes, the SDOH must be considered as underlying influences on those outcomes, as well.
What do we do as a society to help bridge these disparities especially regarding diabetes? The American Diabetes Association (ADA) has instituted the #HealthEquityNow campaign to ensure that people living with diabetes have access to health care and resources that they are many times lacking in their communities. In addition, this campaign rallies policymakers and leaders in the community to address “systemic inequity in cost, care, community, and cuisine faced by people of color and economically disadvantaged citizens”[34]. The ADA implores action in cost by making insulin and other diabetic drugs and supplies affordable and available. Black Americans account for more than 75% of low-income Americans in the country, while disproportionally having higher rates of diabetes than White Americans. Cost and accessibility to these vital items must be addressed to close the gap on inequity Accessibility to care can be addressed by providing quality care in the community and workplace for people of color. Cure ensures that research focuses specifically on risks and problems facing non-Hispanic Black Americans regarding diabetes. Connect involves building community partnerships that will advocate for people of color. Lastly, cuisine will help people of color make healthy choices regarding their individual nutritional needs based on a cultural foods and choices [35]. Cuisine will also address the fact that “food deserts” or areas where members of the community have decreased availability to healthy food options, are more prominent in Black and Hispanic neighborhoods. Less healthy food available, coupled with poverty and diabetes puts them in circumstances that negatively impact their health [36]. Another piece to the #Health Equity Now campaign is The Health Equity Bill of Rights. These include the right to have affordable diabetic drugs and insulin, healthy food, insurance that covers diabetes management, no stigma or discrimination, avoid preventable amputations, control prediabetes before it becomes diabetes, healthy environment, latest medical advancement, and the right to be heard. With the institution of these rights, it is possible to ensure health equity for our most vulnerable populations [35].
Limitations
The limitations of this study include the use of secondary data which were collected by four different state health departments. The data collection and aggregation methods may have varied across state health departments. A second limitation is that mortality rates are crude and race-specific, and were not age-adjusted. Finally, only hotspot counties in each study state were included in the study.
Conclusions
In conclusion, this study illustrated that the disparity in mortality and case-fatality rates observed in the early months of the COVID-19 pandemic still persist today. The effect of co-morbidities, especially diabetes and obesity, have an impact on COVID-19 mortality. An explanation for this disparity is health inequities which minorities populations have experienced for decades in the U.S. The effect of structural racism is illustrated in COVID-19 mortality disparity and should be addressed through public health policy and practices.
Acknowledgements:
Research reported in this study was funded, in part, by the National Institute of Minority Health and Health Disparities of the National Institutes of Health under grant S21MD1007136.
Conflict of interest:
The authors have declared no conflict of interest.
References
Fos, P.J., Honoré, P.A., & Kellum, K.P. (2020). The relationship of diabetes and COVID-19: A health disparity. Diabetes & its Complications, 4(1):1-8.View
Popkin, B.M., Du, S., Green, W.D., Skekar, M. (2020). Individuals with obesity and COVID-19: A global perspective on the epidemiology and biological relationships. Obesity Reviews, 21, e13128View
Hales, C.M., Carroll, M.D., Fryar, C.D., & Ogden, C.L. (2020). Prevalence of obesity and severe obesity among adults: United States, 2017-2018. NCHS data brief, no. 360. National Center for Health Statistics.View
Hales, C.M., Carroll, M.D., Fryar, C.D., & Ogden, C.L. (2017). Prevalence of obesity and severe obesity among adults: United States, 2015-2016. NCHS data brief, no. 288. National Center for Health Statistics.View
Ward, Z.J., Bleich, S.N., Craddock, A.L., …Gortmayer, S.L. (2019). Projected U.S. state-level prevalence of adult obesity and severe obesity. New England Journal of Medicine, 381, 2240-2450. https://doi.org/10.1056/NEJMsa1909301View
Bleich, S.N., &Ard, J.D. (2021). COVID-19, obesity, and structural racism: Understanding the past and identifying solutions for the future. Cell Metabolism, 33. https://doi. org/10.1016/j.cmet.2021.01.010.View
Marmot, M. (2005). Social determinants of health inequalities. Lancet, 365:1099-1104.View
Marmot, M., Friel, S., Bell, R., Houweling, A.J., & Taylor, S. CSDH (2008). Closing the gap in a generation: Health equity through addressing the social determinants of health. The Lancet, 372(9650(:1661-1669. https://doi.org/10.1016/S0140- 6736(08)61690-8View
Office of Disease Prevention and Health Promotion. (2021) US Department of Health and Human Services. Disparities. Retrieved from http://www.healthypeople.gov/2020/about/ foundation-health-measures/Disparities#6View
Braveman, P. (2014). What are health disparities and health equity? We need to be clear. Public Health Reports, 139, Suppl 2: 5-8.View
Braveman, P.A., Kumanyika, S., Fielding, J.,LaViest, T., Borrell, L.N., Manderscheid, R., & Troutman, A. (2011). Health disparities and health equity: The issue of justice. American Journalof Public Health, 101:S149-S155.View
Commission on Social Determinants of Health. (2008). Closing the gap in a generation: Health equity through action on the social determinants of health. Final Report of the Commission on Social Determinants of Health, World Health Organization. Geneva, Switzerland.View
Culyer, A,J.,& Wagstaff, A. (1993). Equity and inequality in health and health care. Journal of Health Economics, 12:431-477.View
Marmot, M., & Bell, R. (2018). The sustainable development goals & health equity. Epidemiology, 29(1):5-7View
Geronimus, A.T., Pearson, J.A., Linnenbringer, E., …Blackburn, E.H. (2015). Race-ethnicity, poverty, urban stressors, and telomere length in Detroit community-based sample. Journal of Health & Social Behavior, 56(2):199-224. https://doi. org.10.1177/0022146515582100View
Zar, H.J., Dawa, J., Fischer, G.B., Castro-Rodriguez, J.A. (2020). Challenges of COVID-19 in children in low- and middle-income countries. Paediatric Respiratory Review, 35:70-74. https://doi.org/10.1016/j.prrv.2020.060016View
Ansari, Z., Carson, N.J., Ackland, M.J., Vaughan, L., &Serraglio, A. (2003). A public health model of the social determinants of health. Soz Praventivmed. 48(4):242-251. https://doi. org/10.1009/s00038-003-205-4View
Beckfield, J., Olafsdothr, S., & Baktiari, E. (2013), Health inequities in global context. Americanof Behavioral Sciences, 57(8):1014-1039.View
Adeniji, N., Carr, R.M., Aby, E.S., Catana, A.M., Wegerman, K., & Dhanasekaram, R. (2021). Socioeconomic factors contribute to higher risks of COVID-19 in racial and ethnic minorities with chronic liver diseases. Gastroenterology, 160: 1406-1409. https://doi.org/10.1053/j.gastro.2020.11.035View
Williams, D.R., Emamdjomeh, A., Davis, B.A. (2018). Racism and health: Evidence and needed research. Annual Review of Public Health, 40, 105-125. View
Williams, D.R., Lawrence, J.A., & Davis, B.A. (2019). Racism and health: Evidence and needed research. Annual Review of Public Health, 40, 105-125.View
Kluge, H.H.R., Jakab, A., Baronic, J., D’Anna, V., & Severoni, S. (2020). Refugee and migrant health in the COVID-19 response. Lancet, 395(10232): 1237-1239. https://doi.ordg/10.1016/ S0140-6736(20)30791-1View
Centers for Disease Control and Prevention (2021). Media statement from CDC Director Rochelle P. Walensky, MD, MPH, on racism and health. April 8, 2021. Retrieved from https:// www.cdc.gov/media/releases/2021/s0408-racism-health.htmlView
Egede, L.E., & Walker, R.J. (2020). Structural racism, social risk factors, and COVID-19: A dangerous convergence for Black Americans. New England Journal of Medicine, 383.e77. https://doi.ordg/10.1056/NEJMp2023616View
Kreiger, N. (2020). Measures of racism, sexism, heterosexism, and gender Binaism for health equity research from structural injustice to embodied harm: An ecosocial analysis. Annual Review of Public Health, 41, 37-62.
Bailey, Z.D., Kreiger, N., Agénor, M., Graves, J, Linos, N. & Bassett, M.T. (2017). Structural racism and health inequities in the USA: Evidence and interventions. The Lancet, 389, 1453-1463.View
Dryden, O. & Nnorom, O. (2021). Time to dismantle systemic anti-Black racism in medicine in Canada. Canadian Medical Association Journal, 193(2), E55-E57. https://doi.org/10.1503/ cmaj.201579View
Johnson, T.J. (2020). Intersection of bias, structural racism, and social determinants with health care inequities. Pediatrics, 146(12): e2020003657.https://doi.org/10.1052/peds.2020-003657View
Hamed, S., Thaper-Björkert, S., Brady, H., & Ahlberg, B.M. (2017). Racism in european health care: Structural violence and beyond. Qualitative Health Research, 30(1): 1662-1673. https:// doi.org/10.1177/104973230931430View
Tjaden, L.A., Jager, K.J., Bonthuis, M…Noordzij, M. (2017). Racial variation in cardiovascular disease risk factors among Europeanchildren on renal replacement therapy: Results from the European Society for Paediatric Nephology/European Renal Association – European Dialysis and Transplant Association Registry. Nephrology Dialysis Transplantation, 32(11): 1908- 1917. https://doi.org/10.1093/ndt/gfw423View
Muscat, N.A., Paget, D.Z., & McKee, M. (2017). Public health must confront racism and xenophobia. The Lancet, 390(10098). https://doi/org/10.1016/S0140-6736(17)32174-8View
U.S. Census Bureau. Quick Facts (2021). Retrieved from https:// www.census.gov/quickfacts/fact/table/waynecountymichigan/ laplaceddplouisiana.eastbatonrougeparishlouisiana. orleansparishlouisiana.doughertycountygeorgia/PST045219
Fink, D.S., Keyes, K.M., & Cerda, M. (2016) Social determinants of population health: A systems science approach. Current Epidemiology Reports, 3(1): 96-105. https://doi.org/10.1007/ s40471-016-0066-8View
American Diabetes Association (2020). American Diabetes Association unveils #HealthEquityNow platform for action. Retrieved from https://www.diabetes.org/newsroom/press-releases/2020/ada-unveils-healthequitynowplatform-to-ignite-actionView
American Diabetes Association (2021). #HealthEquiyt Now. Retrieved from https://www.diabetes.org/healthequitynowView
Brooks, K. (2014). Research shows that food deserts more abundant in minority neighborhoods. Johns Hopkins Magazine. Retrieved from https://hub.jhu.edu/magazine/2014/spring/ racial-food-desertsView