
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 5 (2021), Article ID: JPHIP-194
https://doi.org/10.33790/jphip1100194Research Article
Motor Control Alterations and the Perception of Postural Instability in non-Fallers Latinx-Hispanic Adults Living with HIV
Martin G. Rosario PT, PhD, CSFI, ATRIC
Assistant Professor, Texas Woman’s University, Physical Therapy Program, Dallas Campus, 5500 Southwestern Medical Ave. Dallas, TX 75235-7299. United States.
Corresponding Author Details: Martin G. Rosario PT, PhD, CSFI, ATRIC, Assistant Professor, Texas Woman’s University, Physical Therapy Program, Dallas Campus, 5500 Southwestern Medical Ave. Dallas, TX 75235-7299. United States. E-mail: mrosario1@twu.edu%20
Received date: 03rd November, 2021
Accepted date: 13th January, 2022
Published date: 15th January, 2022
Citation: Rosario, M.G. (2022). Motor Control Alterations and the Perception of Postural Instability in non-Fallers Latinx-Hispanic Adults Living with HIV. J Pub Health Issue Pract 6(1): 194.
Copyright:©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
People who have advanced HIV can display inadequate postural control because of the virus affecting the brain. Antiretroviral therapy (ART) mitigates some repercussions of the disease, maintaining a healthy immune system. The issue is that prolonged usage of ART may affect balance at a slower pace.
Purpose: Assess postural control and balance perception in Latinx-Hispanic people living with HIV with a stable immune system.
Methods: 42 (30 men and 12women) subjects took part in the investigation (57.2± 8.7 years old). Participants had to be diagnosed with HIV to enroll in the study with a CD4 count of > 500 cells/µL. The eight balance tasks (15 s each) were accomplished on a thick balance foam mat and further partitioned into two parts, four single and four dual cognitive tasks (subjects counting backward three numbers at a time).
Results: We measured balance using body-worn accelerometers (ACC) and the ABC scale. There was a considerable increase in sway movements within the different tasks, χ2 (8) = 194.314, p = 0.00. This increment in postural movements was observed when single and dual tasks were contrasted for EO (Z=-2.169, p=005) and EOHUD (Z=-2.344, p 0.05). Related to the ABC scale, subjects scored lower, notably in tasks involving more balance demands.
Conclusion: HIV-diagnosed individuals with a stable immune system exhibit increased postural alteration and perceive balance difficulties with activities requiring higher motor control demands. Clinicians should assess the balance in people living with HIV in all stages of the disease as a prevention tool.
Keywords: HIV, Balance Instability, Sway ACC, ABC Scale, Motor control deficits, Latinx-Hispanic
Introduction
Human immunodeficiency virus (HIV) is a global plague involving millions of people (http://www.unaids.org). In the United States alone, over one million adults are living with this disease (www.cdc. gov). In districts like Texas and Puerto Rico, Hispanic/Latino males represent the largest cohort affected by the illness (in their latest surveillance report in 2015, revised in November 2018).
The problem is that when inadequately regulated, HIV can lead to a plethora of alterations. Several factors determine these alterations, including time since diagnosis, disease severity, cd4 count, and HIV-related comorbidities [1-4].
Motor control, explicitly gait and balance, are among the areas affected by HIV. HIV replicates in the brain area, provoking inflammation, producing motor impairments that alter gait and stability [5,6]. MRI images showed how HIV invades the frontal lobe, explaining many of the neurological complications displayed by those surviving with HIV [7-11]. With this type of brain modification, HIV infection can precipitate mild to severe motor-cognitive disruptions in people living with the disease [1,12-15].
The solution for many of the motor-cognitive difficulties engendered by poor management of HIV is mitigated by adequate handling of antiretroviral therapy (ART). ART has been proven to diminish the neurological burden prompted by the virus, reducing morbidity and mortality percentages among individuals with HIV, extending their lifespans, and improving the quality of life [16]. Withal, prolonged usage of ART disturbs the motor-cognitive system, altering postural control, and therefore increasing the risk of falls in these individuals [16,17].
Memory, attention, and motor speed are among the motor-cognitive dysfunctions and prominent traits of HIV [18,19]. Despite the implication of these characteristics among individuals with HIV, the expression and severity of these deteriorations are not universal, as the consistency differs across contrasting populations and backgrounds [19]. Nevertheless, HIV involves detectable balance and neuromuscular activation perturbations in different stages of the disease [20,21].
Considering the above, in seemingly asymptomatic HIV-diagnosed individuals, with a steady immune system (cd4 above 500) before the quality of living is disturbed, this research seeks to answer: 1) Can postural variation in low perturbation stability tests be observed in controlled stages of HIV? 2) Can we characterize these postural adjustments and determine the balance system (vestibular, proprioceptive, vision) altered by HIV? 3) Can these posture control alterations be perceived by those suffering this illness during everyday activities?
This work will attempt to deal with the above by examining standing postural control (during four single and four dual cognitive tasks) and perceived balance confidence to distinguish the manifestations of instability in non-fallers and HIV-diagnosed adults.
Methodology
Participants: This study recruited male and female participants from La Perla de Gran Precio, a Community wellness center specialized in Latinx-Hispanic people with HIV located in San Juan, Puerto Rico. A total of 42 (30 male and 12 female) subjects signed the informed consent and participated in this study. The participants were 57.5± 8.7 years old, on average, with a CD4 count of 775.7± 341.2 cells/µL and an average BMI of 25.7± 4.4, as reported in Table 1.
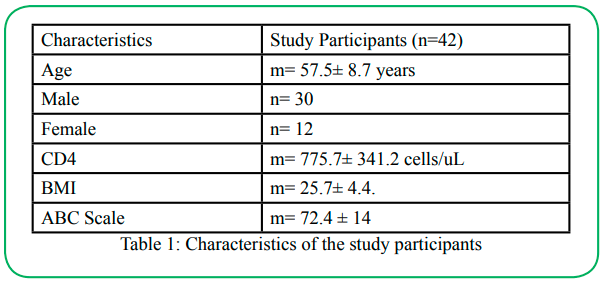
Table 1: Characteristics of the study participants
The requirement to participate in this study included the following:
• Diagnosis of HIV by a medical doctor.
• CD4 levels above 500 cells/µL, representing a stable immune system.
• Adults within the age of 25-80 years.
• Walking without an assistive device.
• Stand for at least 30 minutes.
• No reported falls during the last six months.
• No back or lower extremity injury during the last six months.
• Use of medications that cause drowsiness 24 hours before the study (data collection).
• Women who are pregnant or think they might be pregnant.
• A negative Romberg test maintaining a standing position for 30 seconds with their eyes closed.
Balance Assessment:
The current study assessed the perception of balance using the activity-specific balance confidence (ABC) scale [22]. Additionally, we measured postural control using instrumented accelerometers (mobility lab™, Arlington VA). These sensors detect the displacement as the body sways anterior-posterior, or medial-lateral (left or right).
Measured Balance: A member of the research team located a lumbar accelerometer and gyroscope on each subject. The balance examination included a previous protocol utilized by Rosario et al. [23] in HIV subjects.
In summary, all tasks were executed at a distance of 10 feet from the wall. The open eye tasks were performed simultaneously while having participants looking at a fixed point on the wall. Further, the head movement component instructed partakers to maintain a movement frequency of 60 bpm with a metronome in the room and flexion/extension range of approximately 45 ° in each direction. Finally, all tasks were executed on a foam surface, a thick foam pad (15. 5”L x 12. 5”W x 2. 5”H size) located on the floor. Each task took 15 seconds to complete, plus 2 minutes of rest between every two tasks.
These four tasks were considered single tasks and are depicted as follows:
1. Eyes open on foam (EOFOAM)
2. Eyes closed on a firm surface (ECFOAM)
3. eyes open with head movements on a firm surface (EO+HUD)
4. Eyes closed with head movements EC+HUD).
Each subject was asked to accomplish four more tasks, continuing to bear weight on a thick foam pad placed on a firm surface. The remaining four tasks were identical to the tasks mentioned above. However, to add the dual-task component to the balance assessment, participants counted backward by threes. Since neurocognitive impairments are evident at some stages of the disease, we added the cognitive dual-task to the balance test to divide attention and identify alterations that potentially influence motor control in these individuals [24].
Perception of balance: We used the ABC scale for this purpose. The ABC scale [22] is a 16-item questionnaire about various activities that involve maintaining balance to achieve. Participants consider each item on a scale from zero% to 100%. A rating of zero% indicates no confidence in maintaining balance during the activity (without falling), while 100 percent indicates full confidence that they would hold their balance safely. The activities diverge in difficulty and cognitive demand.
Data Analysis:
Measured Balance: A Friedman non-parametric test was used to evaluate the sway velocity of acceleration and both directions between tasks. A Friedman test non-parametric combined with a post hoc analysis, Wilcoxon signed-rank tests were conducted with a Bonferroni correction.
Perceived Balance: For the ABC scale, balance perception, a repeated-measures ANOVA was used to evaluate differences between test items. This analysis was performed to determine if one activity was perceived as, to a greater extent, challenging or difficult by participants than other activities. The mean and standard deviation of the ABC scale score were obtained to assess perceived balance dysfunction or difficulty. A Bonferroni post hoc test was performed to correct for multiple comparisons using an alpha value of 0.05 ABC data analysis.
Results
Measured Balance: Table 2-5 illustrates the jerk sway acceleration (sway, A-P, and M-L) and how was it influenced by the standing surface, head movement, visual input, and cognitive factors during the eight balance activities given to each subject. There was a statistically significant increase in sway movements (Table 3) within the different tasks, χ2(8) = 194.314, p = 0.00. This increase in postural movements was observed when single and dual tasks were compared for EO (Z=-2.169,p=005) and EOHUD (Z=-2.344, p 0.05).
The direction of these alterations was significantly increased in the AP [χ2(8) = 211.566, p = 0.00] and ML [χ2(8) = 137.056, p = 0.00] directions. Similar to sway, AP movement (Table 4) was significantly increased when single and dual tasks were compared for EO (Z=-3.110, p=005) and EOHUD (Z=-2.813, p 0.005). ML movements (Table 5) were increased as well when single and dual tasks were compared for EO (Z=-2.929, p=005) and EOHUD (Z=- 1.984, p 0.05).
Perceived Balance: Table 2 displays the ABC scale score (SD) of participants, 72.4 (28.5). The mean and standard error of the mean (SEM) of single activities within the ABC scale were also analyzed. Item 16, walking on an icy sidewalk, had the lowest mean rating with a mean (SEM) of 46.2 (8.4). Item 9, getting into or out of a car, had the highest rating with a mean (SEM) of 87.1 (4.8). The ABC scale results showed a statistical difference between items 1 and 16 (p < 0.05), 4 and 16 (p < 0.05) 8 and 16 (p < 0.05), 9 and 16 (p < 0.05), and 14 and 16 (p = 0.05).
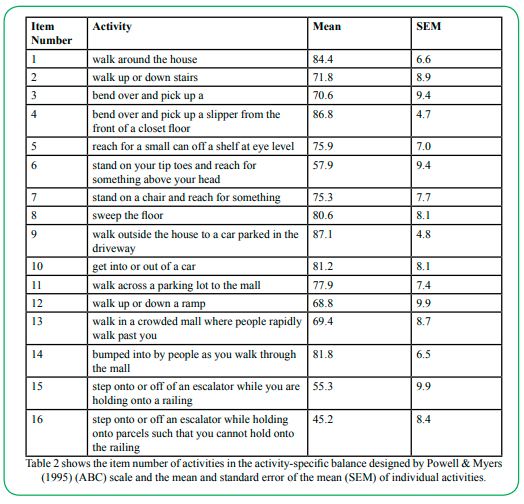
Table 2: shows the item number of activities in the activity-specific balance designed by Powell & Myers (1995) (ABC) scale and the mean and standard error of the mean (SEM) of individual activities.
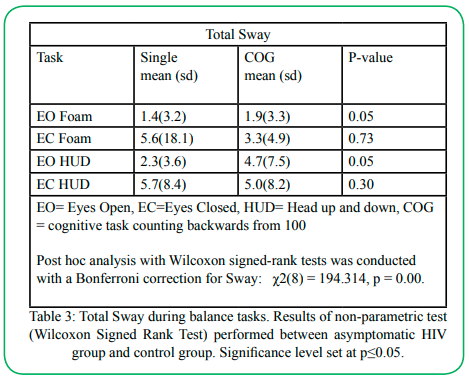
Table 3: Total Sway during balance tasks. Results of non-parametric test (Wilcoxon Signed Rank Test) performed between asymptomatic HIV group and control group. Significance level set at p≤0.05.
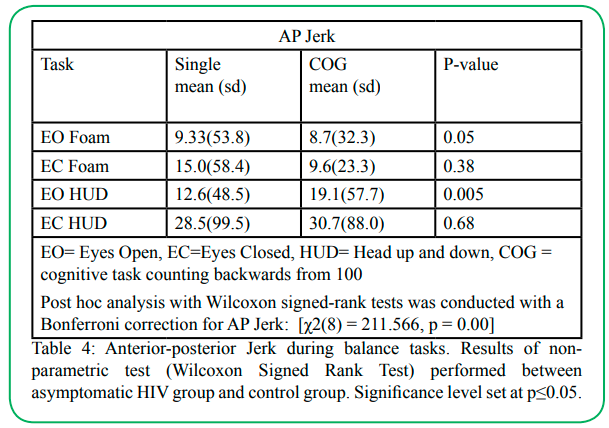
Table 4: Anterior-posterior Jerk during balance tasks. Results of non-parametric test (Wilcoxon Signed Rank Test) performed between asymptomatic HIV group and control group. Significance level set at p≤0.05.
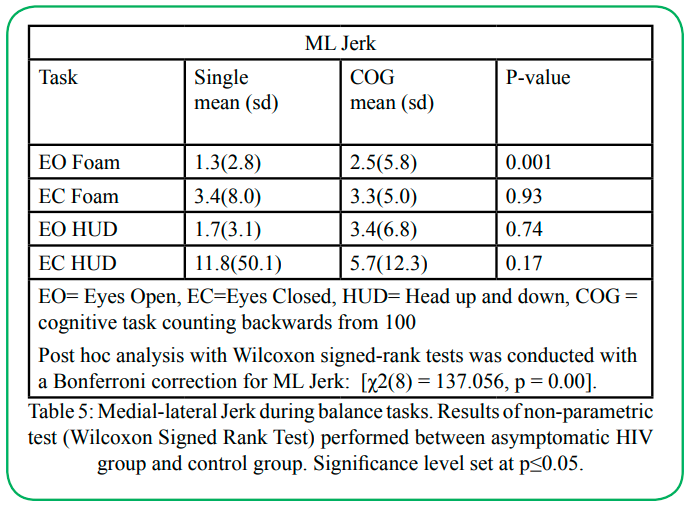
Table 5: Medial-lateral Jerk during balance tasks. Results of non-parametric test (Wilcoxon Signed Rank Test) performed between asymptomatic HIV group and control group. Significance level set at p≤0.05.
Discussion
This study's foremost expectation was to describe posture adjustments and identify balance alterations in individuals living with HIV with no history of falls. To appropriately depict standing balance and recognize early signs of instability in HIV-diagnosed participants, we based this work on a motor control theory, the dynamic system theory framework. This theory states that sensory systems will equally engage in maintaining a dynamic or static postural balance, see figure 1. When a modification in the surface or environment occurs, the system works unitedly to adapt to this new surface or task. Within the dynamic system theory [25], there is a construct that explains how and when systems can adjust when one of the systems is impaired or challenged, called sensory reweighting. Sensory reweighting occurs when a sensory system is impaired, damaged, or simply challenged by shifting surfaces, making sensory reweighting valuable to studies of posture and balance such as this one [25].
Peterka [26], in his studies of human dynamic posture control, argued that depending upon the magnitude and other characteristics of an induced postural disturbance, the central nervous system can consider one source of sensory information (e.g., tactile or proprioceptive) less critical than another source (e.g., vestibular or visual). An illustration of this is walking into a dark room; the sensory information will reweight to the vestibular and proprioceptive systems to uphold posture without falling because no visual input is available. In pathological cases, for instance, when more than one system is impaired, the remaining sensory system is unable to sustain proper posture, and motor control alterations can be observed [25].
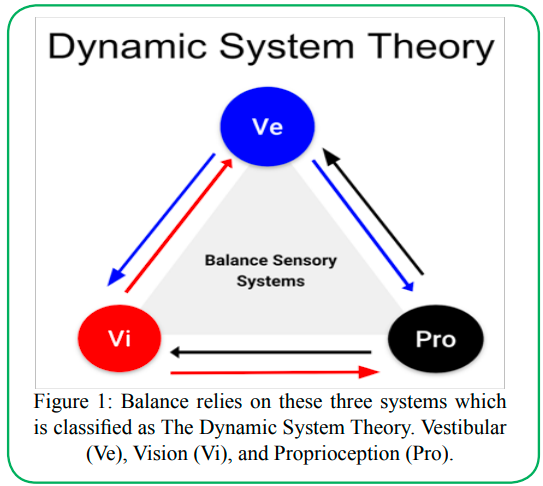
Figure 1: Balance relies on these three systems which is classified as The Dynamic System Theory. Vestibular (Ve), Vision (Vi), and Proprioception (Pro).
In Latinx-Hispanic people living with HIV with a stable immune system, we strived to assess postural control during four single and four dual-cognitive tasks to discern the role of the vestibular, proprioceptive, and visual input during these balance activities. We also aimed to determine the participant's perceptual balance experience among different dynamic common activities. To explain the above, the current study stated three main questions to differentiate the balance profile of those living with HIV with no reported history of falls and a stable immune system.
Can postural variation in low perturbation stability tests be observed in controlled stages of HIV? Yes. Our study found that people living with asymptomatic HIV have increased multi-directional postural sway and reduced balance before a reported history of falls. Outcomes are consistent with one meta-analysis that shows balance impairments in people with advanced HIV resembled fall risk characteristics in non-HIV older adults [1]. Prior studies have also shown an increased number of fall risk factors and the number of falls in those living with HIV compared to uninfected adults [16].
In our study, activities requiring dual splits cognitive interplay with eyes open showed increased postural sway. A possible explanation is the occurrence of higher center brain alterations, including frontal lobe structural modifications, brain white matter reduction [27], and dementia [1,12-15]. Higher center's functions, such as cognition, perception, and attention, are imperative for achieving proper balance [25]. Since the participants of this study had no signs of falls or dementia, we attributed these alterations in the tasks requiring attention and cognitive interplay by counting backward, as early signs of motor-cognitive alterations.
As reported in the literature, balance is achieved by the intricate coordination between three sensory systems: somatosensory, visual, and vestibular, and is subsequently integrated into the central nervous system [26]. Our tests were designed to challenge the sensory balance system's inputs while performing multiple tasks in a static low perturbation setting. We planned our tasks to challenge the sensory system and purposely provoke sensory reweighting. For instance, eyes closed to cancel visual systems and redirect sensory information to the vestibular and proprioception systems, similar to a dark room scenario. Standing on a thick foam is aimed at altering or challenging the proprioceptive input, and moving the head up and down (in a yes gesture) at 60 beats per minute (bpm) to challenge the vestibular input, as illustrated in figure 2.
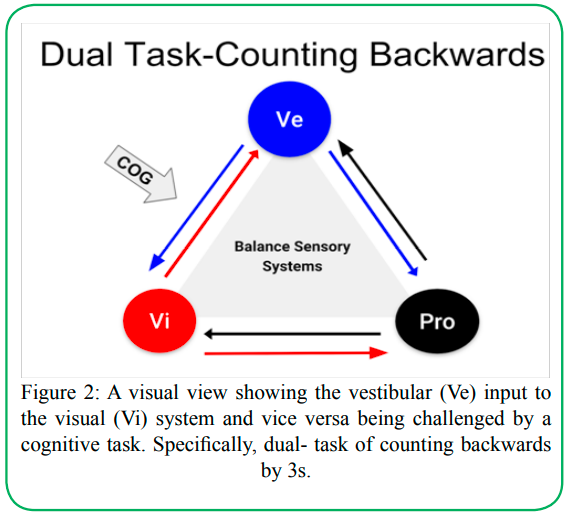
Figure 2: A visual view showing the vestibular (Ve) input to the visual (Vi) system and vice versa being challenged by a cognitive task. Specifically, dual- task of counting backwards by 3s.
Among these sensory balance tests, we made a combination of them to provoke reweighting of the system's input or give more importance to the unchallenged systems. In addition, we added the dual cognitive component to split the participant's attention and identify neurocognitive modifications during the balance activities, as depicted in figure 3. Since cognitive-perception interplay is essential for postural control, even mild cognitive impairment can directly affect the balance [24] system, causing an increase in sway and postural instability. Hence, according to the dynamic system theory, if there are more than two systems, impaired deficiencies will become apparent and identifiable as an increase in postural sway [25]. Since the balance tasks in this study were had low perturbation activity, we acknowledge that signs of balance alterations with cognitive involvement are displayed in controlled stages of HIV.
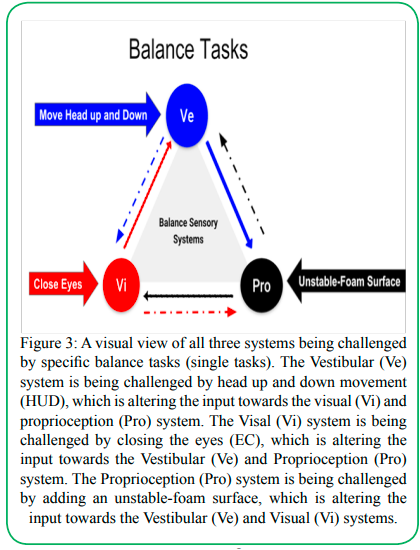
Figure 3: A visual view of all three systems being challenged by specific balance tasks (single tasks). The Vestibular (Ve) system is being challenged by head up and down movement (HUD), which is altering the input towards the visual (Vi) and proprioception (Pro) system. The Visal (Vi) system is being challenged by closing the eyes (EC), which is altering the input towards the Vestibular (Ve) and Proprioception (Pro) system. The Proprioception (Pro) system is being challenged by adding an unstable-foam surface, which is altering the input towards the Vestibular (Ve) and Visual (Vi) systems.
Can we characterize these postural adjustments and determine the balance system (vestibular, proprioceptive, vision) altered by HIV? Yes. Increased postural sway was observed when the vestibular input was challenged by a coordinated and constant rotation of the head in the sagittal plane. Postural instability was particularly noticeable when participants had to combine proprioceptive alterations by the unstable surface, foam, with the aforementioned head movements. This study confirms previously established research findings where the vestibular system (Heize, 2011,2013) shows signs of deficiency when associated with HIV. Withal, most participants showing signs of vestibular impairment in Heize’s reports had a variety of underlying conditions, comorbidities, or advanced HIV status [28]. Our study ushers in that participants had no apparent pre-indication of vestibular deterioration tested by the Romberg examination, and the absent history of falls, however, exhibited postural instability.
Our study also reveals the direction of the instability and the tendency to fall for these participants. The results showed an increase in the anterior-posterior direction when visual input was canceled, and the vestibular and proprioceptive inputs were challenged, particularly during dual-task interplay. During this previously mentioned task, we challenged the proprioceptive input with the unstable foam surface and the vestibular sensory input by moving the head up- down while looking at the fixed point at the wall. As stated earlier, with eyes closed, we elicit reweighting of the three systems to an interplay of two systems, vestibular and proprioception. Commonly, sway should slightly increase when the visual input is canceled. However, in a healthy balance system, reweighting can compensate and maintain the standing postural balance with minimal sway [21]. The reduced interaction between the vestibular and proprioceptive systems depicted by increased sway in the AP direction corroborates other reports. Trenkwalder C [29] outlined the increase in instability during activities requiring unstable surfaces and eyes closed in people living with HIV. The primary difference between the present study and Trenkwalder's is the status of participants with HIV diseases and the canceled visual input. Our study features early stages, physically active, non-fallers with HIV diagnosis (cd4 count above 200), while Trenkwalder's and other similar studies featured late stages, AIDS, low CD4, reported falls, in symptomatic individuals.
The outcomes of the current investigation showed that sway in the mediolateral direction was also altered to a lesser extent than AP. During double-leg standing balance, sway commonly occurs in an anterior-posterior direction at the ankle joint compared to the medial-lateral fluctuation [25]. According to reports such as the ones detailed in Shumway-Cook, A., & Woollacott, M. H., [25], abnormal mediolateral sway is related to alterations of the central nervous system or trunk musculature weakness. Hence, we expected these results and ML sway to increase in more advanced stages of HIV. Studies have shown higher center involvement in HIV participants such as the brainstem and cerebellar regions in those with HIV that contributed to postural instability and balance deficits [27].
Another explanation for the normal mediolateral sway is that early signs of postural instability are detected first in an increase in AP sway rather than ML movements. Participants in this setting engaged in regular exercise activities and severe weakness in the trunk muscles was a non-factor. Second, we recruited people with cd4 levels in a safe range. HIV/AIDS is defined by the cd4 count levels below 200 constituted an AIDS diagnosis, whereas values above 200 were related to HIV. Finally, we recruited independent physically active participants with no history of falls and with no apparent injury or impairment of the central nervous system.
The present study considered the unsteady foam surface to the examination protocol due to the evidence of peripheral neuropathy that some HIV-diagnosed individuals experience [3]. There is a wide range of neuromuscular diseases and impairments associated with HIV that can affect the musculature and peripheral nerves of the body [30]. The authors believe there is insufficient evidence assessing the efficiency of the proprioceptive input's role during motor control in people with HIV. As previously acknowledged, Figure 1 illustrates the interplay between the three main sensory systems. Since the visual system is apparently intact in the participants of this study, they can compensate and maintain balance. Thenceforth, this study's protocol highlighted the alteration and reduced reweighting of the balance systems when the proprioceptive input was altered while standing on foam in asymptomatic HIV individuals and demonstrated the necessity of including lower limb peripheral nerve assessment in clinical examinations.
Can those suffering from this illness during ordinary activities perceive postural control alterations? Yes. The mean balance confidence of the participants was below the cutoff score of 72.4. A score of 72.4 illustrates that participants in this study noticed their difficulties among several everyday tasks. It has been established that a cutoff score of 85 is optimal for the identification of balance dysfunction [31].
The three distinct components on the ABC scale scored fewer than other balance activities: standing on a chair and reaching for something, stepping on or off an escalator, holding an object, not using the railing, and walking outside on an icy sidewalk. It appears that the tasks requiring a more precise interplay of the balance systems (moving the head and standing on different surfaces) are the ones that scored lower among the participants of this study. One reason for this may be that the increased cognitive requirement imposed by balance activities as dual-task activities has been revealed to reduce postural stability [32]. Because these tasks demand more concentration to sustain balance, they may be perceived as more complicated and, consequently, given less confidence in completion.
Walking on an icy sidewalk had considerably less confidence among participants than other activities (items 1, 4, 8, 9, and 14). One likely interpretation is that postural responses and corrections take longer as adults age, leading to inefficient recovery strategies [33]. The reduction in postural adjustment might be intensified in individuals with HIV because of the virus's effect on the nervous system [1,34]. A low ABC scale score has also been associated with increased fall risk in other populations in which the nervous system is disturbed, including multiple sclerosis, stroke, and Parkinson's disease [35], proving that even during asymptomatic stages of the conditions, people living with HIV are at risk of falls.
The balance challenge of walking on an icy sidewalk and slippery surface requires an intact proprioceptive and vestibular pathway interplay. When this reweighting interplay is distorted, individuals may recognize this task as more complicated and have reduced confidence in conserving balance [36,37].
While our participants were active people, community ambulators, and had no history of falls, an underlying balance dysfunction may yet be present. What is concerning is that a lower perceived balance score is related to reducing community involvement. Decreased community participation is the starting period of affected life quality and independence. We recommend using the ABC scale in those living with HIV at any stage of the disease. Last, we encourage assessing the quantity and quality of social interaction since it is one of the first signs of reduced balance confidence that could influence the quality of life in this group.
Conclusion
Previously, we stated the intent of this report to answer the possibility of identifying neurocognitive or neuromotor alterations in apparently asymptomatic (early stages) HIV-diagnosed individuals before quality of life was negatively altered. This work illustrates individuals with HIV with noticeable signs of mild cognitive and motor alterations by an increased postural sway during standing postural balance, especially when the cognitive element was added to the balance activities. Dual cognitive tasks proved to constitute a challenge for participants in this study depicted by standing postural instability compared with single tasks. Among asymptomatic participants with HIV, sensory re-weighting is insufficient to maintain proper posture when the vestibular and proprioceptive inputs are challenged simultaneously during single or dual tasks.
Despite participants being active, asymptomatic adults, an underlying alteration in balance was noted with the ABC scale and postural sway. The ABC scale is a tool that may be able to identify balance dysfunction in asymptomatic individuals with HIV who have no history of falls and should be implemented in this population. The ABC scale and sensory testing may serve as a screening tool for balance impairment in the early stages of HIV. In future inquiries, we recommend dynamic postural analysis such as gait or single-leg balance. The neuromuscular assessment of ankle, hip and trunk musculature responsible for postural balance. Finally, we advise early vestibular and proprioceptive evaluation and intervention for people with HIV diagnosis at any stage of the condition.
Declaration:
Funding:
Not Applicable
Conflicts of interest/Competing interests:
Author report no conflict or competing interest.
Ethics approval:
IRB approval TWU protocol # 20092
References
Berner, K., Morris, L., Baumeister, J., & Louw, Q. (2017). Objective impairments of gait and balance in adults living with HIV-1 infection: a systematic review and meta-analysis of observational studies. BMC Musculoskeletal Disorders, 18(1), 325.View
Richert, L., Dehail, P., Mercié, P., Dauchy, F., Bruyand, M., Greib, C., et al. (2011). High frequency of poor locomotor performance in HIV-infected patients. AIDS. 25(6):797–805. doi: 10.1097/QAD.0b013e3283455dff.View
Rosario, M.G., Jamison, L., & Gines, G. (2020). The Role of HIV Antiretroviral Medication on Motor-Cognitive and Neurological Alterations in Hispanic People Living with HIV. J Pub Health Issue Pract 4(1):160.https://doi.org/10.33790/ jphip1100160
Rosario, M.G., Gines, G., & Jamison, L. (2020). Lifestyle, Physical and Cardiovascular Components Associated with Immune Profile in Hispanic-Latino People Living with HIV. J Ment Health Soc Behav 2(2):121.DOI: https://doi.org/10.33790/ jmhsb1100121View
Calcagno, A., Perri, G. D., & Bonora, S. (2017). Treating HIV Infection in the Central Nervous System. Drugs,77(2), 145-157. doi:10.1007/s40265-016-0678-9View
Lucas, S., & Nelson, A. M. (2014). HIV and the spectrum of human disease. The Journal of Pathology, 235(2), 229-241. doi:10.1002/path.4449View
Chang, Y. L., Stanford, C. M., & Keller, J. C. (2000). Calcium and phosphate supplementation promotes bone cell mineralization: implications for hydroxyapatite (HA)-enhanced bone formation. J Biomed Mater Res. 52(2):270-8. doi: 10.1002/1097-4636(200011)52:2<270::aid-jbm5>3.0.co;2-1.View
Paul, I.M., Beiler, J., McMonagle, A., Shaffer, M.L., Duda, L., & Berlin Jr, C.M., (2007). Effect of honey, dextromethorphan, and no treatment on nocturnal cough and sleep quality for coughing children and their parents. Arch Pediatr Adolesc Med. 161(12):1140-6. doi: 10.1001/archpedi.161.12.1140.View
Sclar, E., & Northridge, M.E. (2001). Property, politics, and public health. Am J Public Health. 91:1013–1015.View
Ernst, C.C., Grant, T.M., Streissguth, A.P., & Sampson, P.D. (1999). Intervention with high-risk alcohol and drug-abusing mothers: II. Three-year findings from the Seattle Model of Paraprofessional Advocacy. Journal of Community Psychology, 27, 19–38.View
Heindel, W.C., Jernigan, T.L., Archibald, S.L., Achim, C.L., Masliah, E., & Wiley, C.A. (1994). The relationship of quantitative brain magnetic resonance imaging measures to neuropathologic indexes of human immunodeficiency virus infection. Arch Neurol 51: 1129–1135.View
Cysique, L., Brew, B., (2009). Neuropsychological Functioning and Antiretroviral Treatment in HIV/AIDS: A Review. DOI:10.1007/s11065-009-9092-3View
Ellis T, et al. (2009). Diversity-based, model-guided construction of synthetic gene networks with predicted functions. Nat Biotechnol, 27(5):465-71View
Woods, M.N., Wanke, C. A., Ling, P. R., Hendricks, K. M., Tang, A. M., Knox, T. A., et al. (2009). Effect of a dietary intervention and n-3 fatty acid supplementation on measures of serum lipid and insulin sensitivity in persons with HIV. Am J Clin Nutr, 90:1566-1578.View
Heaton, T. H., J. H. Hall, D.J. Wald, and M. Hailing, (1995). Response of high-rise and base-isolated buildings to a hypothetical M w 7.0 blind thrust earthquake, Science 267, 206- 211.View
Erlandson, K.M., Plankey, M.W., Springer, G., Cohen, H.S., Cox, C., & Hoffman, H.J., et al. (2016). Fall frequency and associated factors among men and women with or at risk for HIV infection. HIV Med. doi:10.1111/hiv.12378.View
Cohen, H. S., Cox, C., Springer, G., Hoffman, H. J., Young, M. A., Margolick, J. B., & Plankey, M. W. (2012). Prevalence of abnormalities in vestibular function and balance among HIV-seropositive and HIV-seronegative women and men. PloS one, 7(5), e38419. https://doi.org/10.1371/journal.pone.0038419View
Woods, S.P., Moore,D.J., Weber, E., & Grant, I., (2009). Cognitive Neuropsychology of HIV-Associated Neurocognitive Disorders. Neuropsychol Rev 19:152–168. DOI 10.1007/ s11065-009-9102-5View
Dawes J. (2008). Do data characteristics change according to the number of scale points used? An experiment using 5-point, 7-point and 10-point scales. Int. J. Mark. Res. 50 61–104. https://doi.org/10.1177/147078530805000106View
Rosario, M.G. (B) (2020). Early signs of standing postural instability in asymptomatic people living with HIV. HIV & AIDS Review. International Journal of HIV-Related Problems, 19(3), 193-198. https://doi.org/10.5114/hivar.2020.99680View
Rosario, M.G., Bowman, C., & Jose, A. (2020). Neuromuscular timing activity on ankle musculature in young adults during single and dual-motor tasks accompanied with altered sensory conditions. J Rehab Pract Res 1(2):112. https://doi. org/10.33790/jrpr1100112View
Powell, L. E., & Myers, A. M. (1995). The Activities-specific Balance Confidence (ABC) Scale. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 50A(1). doi:10.1093/gerona/50a.1.m28View
Rosario, M.G. (A) (2020). Gastrocnemius and tibialis anterior neuromuscular modification recruitment during postural standing in people living with HIV. HIV & AIDS Review. International Journal of HIV-Related Problems.19(4):260-266. doi:10.5114/hivar.2020.101633.View
Pieruccini-Faria, F., Sarquis-Adamson, Y., Montero-Odasso, M. (2019). Mild Cognitive Impairment Affects Obstacle Negotiation in Older Adults: Results from "Gait and Brain Study". Gerontology. 65(2):164-173. doi: 10.1159/000492931View
Shumway-Cook, A., & Woollacott, M. H. (2017). Motor control: Translating research into clinical practice. Philadelphia: Lippincott Williams & Wilkins. APA (6th ed.) (Shumway-Cook, A., & Woollacott, M. H., 2017)View
Peterka, R.J. (2002). Sensorimotor integration in human posture control. J Neurophysiol, 88:1097-1118.View
Sullivan, E. V., Rosenbloom, M. J., Rohlfing, T., Kemper, C. A., Deresinski, S., & Pfefferbaum, A. (2010). Pontocerebellar contribution to postural instability and psychomotor slowing in HIV infection without dementia. Brain Imaging and Behavior, 5(1), 12–24. doi: 10.1007/s11682-010-9107-yView
Dellepiane, M., Medicina, M.C., Mora, R., Salami, A. (2005). Static and dynamic posturography in patients with asymptomatic HIV-1 infection and AIDS. Acta Otorhinolaryngol Ital. 25(6):353–358.View
Trenkwalder, P., Trenkwalder, C., Feiden, W., Vogl, T.J., Einhaupl, K.M., & Lydtin, H. (1992). Toxoplasmosis with early intracerebral hemorrhage in a patient with the acquired immunodeficiency syndrome. Neurology. 42(2):436–8. https:// doi.org/10.1212/wnl.42.2.436.
Prior, D. E., Song, N., & Cohen, J. A. (2018). Neuromuscular diseases associated with Human Immunodeficiency Virus infection. Journal of the Neurological Sciences, 387, 27–36. doi: 10.1016/j.jns.2018.01.016View
Whitney, S.L., Wrisley, D.M., Marchetti, G.F., Gee, M.A., Redfern, M.S., Joseph M Furman, J.M., (2005). Clinical measurement of sit-to-stand performance in people with balance disorders: validity of data for the Five-Times-Sit-to-Stand Test. Phys Ther 85(10):1034-45.View
Shashank, G., Ishan, G. & Alfred O., E. (2017). Effects of dual tasks and dual-task training on postural stability: A systematic review and meta-analysis. Clinical Interventions in Aging, 12, 557-577.View
Tang, P. F, and M .H Woollacott. (1998). "Inefficient Postural Responses to Unexpected Slips during Walking in Older Adults." The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences. 53.6: M471-480. Web.View
Yu, B., Pasipanodya, E., Montoya, J. L., Moore, R. C., Gianella, S., Mccutchan, A., . . . Marquine, M. J. (2019). Metabolic Syndrome and Neurocognitive Deficits in HIV Infection. JAIDS Journal of Acquired Immune Deficiency Syndromes, 81(1), 95- 101. doi:10.1097/qai.0000000000001964View
Beghi, E., Gervasoni, A., Pupillo, I., Bianchi, M., Montesano, D., Aprile, . . . Cattaneo. (2018). Prediction of Falls in Subjects Suffering From Parkinson Disease, Multiple Sclerosis, and Stroke. Archives of Physical Medicine and Rehabilitation., 99(4), 641-651.View
Rand, D. (2018). Mobility, balance and balance confidence – correlations with daily living of individuals with and without mild proprioception deficits post-stroke. NeuroRehabilitation,43(2), 219-226. doi:10.3233/nre-172398View
Horak, F. B., Wrisley, D. M., & Frank, J. (2009). The Balance Evaluation Systems Test (BESTest) to Differentiate Balance Deficits. Physical Therapy, 89(5), 484-498. doi:10.2522/ ptj.20080071View