
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 6 (2022), Article ID: JPHIP-198
https://doi.org/10.33790/jphip1100198Research Article
Chronic Kidney Disease Staging Among Type II Diabetes Mellitus Patients in Kedah, Malaysia: Prevalence and its Factor Associated
Abdul Hadi Mohd Zuki 1, & Mohamad Rodi Isa 1*
1Department of Public Health Medicine, Faculty of Medicine, Universiti Teknologi MARA(UiTM) Selangor, Jalan Hospital, 47000 Sungai Buloh, Selangor, Malaysia.
Corresponding Author Details: Mohamad Rodi Isa, MBBS, DAP&E, MPH, DrPH, Department of Public Health Medicine, Faculty of Medicine, Universiti Teknologi MARA, Jalan Hospital, 47000 Sungai Buloh, Selangor, Malaysia. E-mail: rodi@uitm.edu.my
Received date: 11th January, 2022
Accepted date: 22th March, 2022
Published date: 25th March, 2022
Citation: Mohd Zuki, A.H., & Isa, M.R. (2022). Chronic Kidney Disease Staging Among Type II Diabetes Mellitus Patients in Kedah, Malaysia: Prevalence and its Factor Associated. J Pub Health Issue Pract 6(1): 198.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Diabetes mellitus is often associated with chronic kidney disease (CKD) and is one of the significant predictors of the development of CKD. The study aimed to determine the prevalence and associated factors for CKD among diabetes type II diabetes mellitus patients. This crosssectional study using secondary data from National Diabetes Registry’s (NDR) audited patients for the year of 2018 to 2020 at Padang Terap, Kedah. All audited patients were included in the analysis of the study. The eGFR was calculated from serum creatinine value and classified into CKD status based on KDIGO classification. Multiple logistic regression analysis was used to determine the associated factors. A total of 963 patients were involved in this study. The prevalence of CKD among T2DM patients was 38.6% (95% CI: 35.5, 41.7). The factors associated with CKD among T2DM patients were age group (p<0.05), female [adj. OR: 1.974 (95%CI: 1.460, 2.669). triglyceride [Adj. OR: 1.263 (95%CI: 1.099, 1.451)], high density lipoprotein [Adj. OR: 0.663 (95%CI: 0.425, 0.989)] and patients received calcium channel blocker [Adj. OR = 0.658 (95%CI: 0.499, 0.868)]. The statistical model can discriminate 68.8% [95%CI: 65.4, 73.5), p<0.001]) to predict CKD among DM patients. Age, female, triglyceride, high-density lipoprotein, and treatment with calcium channel blocker were found to be significant factors for CKD among T2DM patients. Treating patients with anti-hypertensive and anti-hyperlipidemic are very important to reduce the prevalence of CKD among T2DM patients.
Keywords: Chronic Kidney Disease, Type 2 Diabetes Mellitus, Prevalence of CKD, Associated factors.
Introduction
The prevalence of diabetes mellitus in Malaysia is increasing in trend. The National Health and Morbidity Survey (NHMS) has been reported that the prevalence of DM was 15.1% in 2011 which is double the prevalence that was reported in 1996. The prevalence of DM continues to increase to 17.5% in 2015 and 18.3% in 2019 [1-3].
As the prevalence of DM in Malaysia is increasing in trend over the years, the prevalence of CKD is estimated to be higher because DM is the significant factor for CKD. There are numerous studies have been conducted to determine the prevalence of CKD among T2DM patients. The prevalence was in the range of 16.8% to 83.7% with variability in the prevalence in each CKD staging [4-13].
CKD patients have an extremely high risk of developing kidney failure [14], cardiovascular disease [14,15] and premature death [14]. The progression of CKD to end-stage renal disease (ESRD) is an important clinical event with substantial morbidity among the elderly population [16] and the cardiovascular mortality is 10 to 20 times higher than in the general population in dialysis patients [14]. It has been estimated that approximately 9% of cardiovascular mortality per year is due to CKD [17]. The prevalence of left ventricular hypertrophy was approximately 75% and coronary artery disease was approximately 40% among patients treated by haemodialysis or peritoneal dialysis [17].
There were numerous factors be associated with CKD among T2DM patients from the literature search. However, there was a review on the developing renal risk scores that discussed two risk factors related to CKD, which were the initiating and the progression factors [18]. Diabetes mellitus and metabolic syndrome were identified as the most common cause of CKD worldwide that involve multiple mechanisms, including glomerular hemodynamic factors and advanced glycation end product [19].
There are three main factors associated with CKD which are the presence of hypertension [20,21,11], age as a significant predictor of the development of CKD [10,21-24] and the duration of diabetes mellitus as the risk factor [4,22,25]. Other predictors that also have been discussed were the use of traditional medications and the educational level [24], alcohol consumptions and smoking behaviours [23], HBA1c [6], gender [22], excessive body mass index (BMI) [25] and the presence of cardiovascular disease (CVD) events [27].
The awareness of CKD remains low not only in communities but also in healthcare providers [28]. Therefore, this study objectives aimed to determine the prevalence and its associated factors of CKD among T2DM in Padang Terap, Kedah, Malaysia. It is hoped that this study can expand the current knowledge to assist the health care worker to have better decision-making when they encounter CKD patients with multiple risk factors. Thus, early screening and better treatment should be aimed in the early stage of CKD to reduce the Disability-adjusted Life Years (DALYs) and improve the prognosis of the disease.
Methodology
Underlying Data and Study Design
A cross-sectional study was conducted using secondary data from The Malaysia National Diabetes Registry (NDR). NDR was established in 2009 to monitor clinical outcomes of diabetes patients managed at the primary health clinics of the Ministry of Health, Malaysia (MOH). All diabetic patients who receive diabetes care at participating health clinics are required to be registered in this registry. A proportion of patient records are audited annually, and all information about the clinical and treatment is stored in this registry [29].
Inclusion and Exclusion Criteria
All T2DM patients that have been registered in the NDR under District Health Office, Padang Terap, Kedah and audited in the year 2018 to 2020 were included in this study. Since CKD stages were used as the outcome variable, any patient without serum creatinine value was excluded from the study.
Diagnosis of CKD
The diagnosis of CKD is defined as when the estimated glomerular filtration rate (eGFR) is less than 60 ml/min/1.73 m2 and is present for more than three months with or without evidence of kidney damage or if there is evidence of kidney damage that is present for more than three months with or without eGFR <60 ml/min/1.73 m2 [30]. The presence of proteinuria is considered kidney damage in this study.
The eGFR value requires renal profile blood investigation with a creatinine value. The serum creatinine value from renal profile blood investigation was be converted into eGFR by using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation [30]:
eGFR = 141 x min (SCr/κ, 1)α x max(SCr/κ, 1)-1.209 x 0.993Age x 1.018 [if female] x 1.159 [if Black].
where:
SCr is serum creatinine (in mg/dl) κ is 0.7 for females and 0.9 for males. α is -0.329 for females and -0.411 for males. min indicates the minimum of SCr/κ or 1 max indicates the maximum of SCr/κ or 1
Data management
The initial data received was 1047 patients after the data provider removed the duplication data for repeatedly audited patients from the year 2018 until 2020. However, 84 patients were excluded due to no serum creatinine value giving the remaining 963 patients.
From 21 variables received, seven variables are removed because they were not related to the study. Another four variables have been created based on the 14 existing variables which were the duration of diabetes mellitus (patient's age minus patient's age during diagnosis of DM), eGFR (serum creatinine from renal profile transform into eGFR using CKD-EPI formula), CKD staging classification (classify the eGFR into six stages based on KDIGO classification) and the use of Renin-Angiotensin System (RAS) blocker drugs (Angiotensin Converting Enzyme Inhibitor and/or Angiotensin Receptor Blocker drugs). 11 out of 18 variables were presented with a missing value. The lowest missing value is 0.6% (systolic and diastolic blood pressures) while the highest missing value is 26.2% (serum low-density lipoprotein (LDL)). The missing value has been managed using multiple imputations.
Statistical Analysis
Data were managed and analyzed using the Statistical Package for Social Science (SPSS) Version 27.0 (SPSS, Inc, Chicago, IL, version 27.0). The descriptive analysis was used to describe the sociodemographic characteristics, anthropometric, medical illness, biochemical profile and medication history. Normally distributed data were presented in mean and standard deviation and non-normally distributed data was presented in median and interquartile range (IQR), respectively. Categorical data were presented in frequency (n) and percentage (%). Univariate analysis was conducted to determine the factors associated with CKD among T2DM patients. Odds ratios (OR) and their 95% confidence intervals (CI) were calculated using simple logistic regression (SLogR). The independent variables with less than 0.05 in SLogR were included for further analysis using multiple logistic regression (MLogR) to adjust for confounding factors. The level of statistical significance was set at p<0.05.
Ethical consideration
Ethical approval for this research was obtained from UiTM Research Ethics Review Boards Committee (REC/04/2021 (MR/197)) and The Medical Research and Ethics Committee (MREC), Ministry of Health Malaysia (MOH) (NMRR-20-3082-57796 (IIR))
Result
A total 963 patients in the NDR involved in this study. 372 patients were diagnosed as CKD fiving the prevalence of CKD among T2DM patients was 38.6% (95% CI: 35.5, 41.7). Base on KDIGO Classification, the overall prevalence of CKD among T2DM patients was 38.6% (95% CI: 35.5, 41.70). The prevalence of Stage 1 CKD was 6.95% (95%CI: 3.81, 10.09); stage 2 CKD was 5.40% (995%CI: 2.26, 8.54); stage 3a CKD was 12.35% (95%CI: 9.21, 15.49); stage 3b CKD was 8.1% (95%CI: 4.96, 11.24); stage 4 CKD was 3.86% (95%CI: 0.73, 6.99) and stage 5 CKD was 1.93 (95%CI: 0.10, 5.10).
The distribution and comparison of the characteristics between CKD and without CKD are shown in Table 1. The T2DM patients with CKD were older, female, Malay, overweight, had proteinuria, received CCB but not RAS medications. The height, duration of DM, SBP, HbA1c, total cholesterol, triglyceride and LDL were higher in the CKD group. However, weight, DBP, HDL were higher in the non-CKD group. There were significant differences in the age group (p<0.001), gender (p<0.001), BMI group (p=0.011), duration of DM (p<0.001), triglyceride (p=0.019), HDL (p=0.018), proteinuria (p<0.001) and received CCB (p=0.001) between T2DM patients with and without CKD.
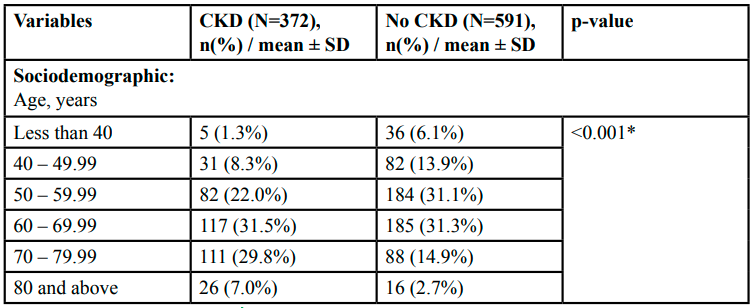
Table 1:The characteristics of the T2DM patients with and without CKD (N=963)
Table 2 shows the univariate analysis to determine the factors associated with CKD among T2DM patients. From this analysis, it was found that the factor considered for multivariable analyses were: age group (p<0.05), gender (p<0.001), BMI group (p<0.05), duration of DM (p=0.010), triglyceride (p=0.023), DHL (p=0.021) and CCB status (p=0.001).
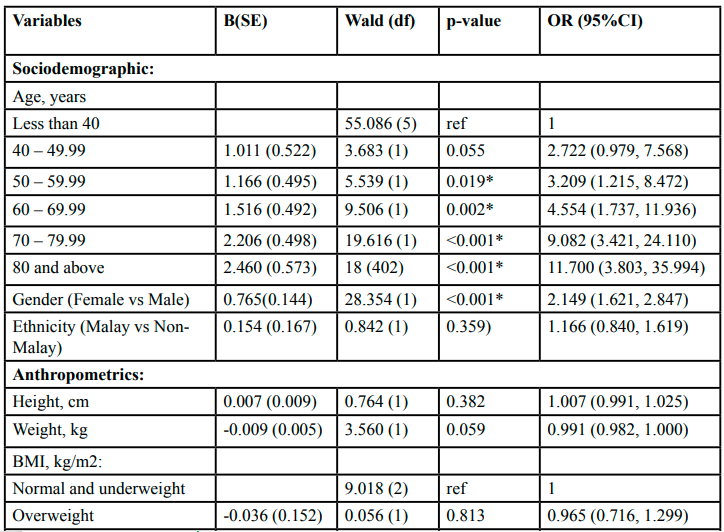
Table 2: Univariate Analysis to determine the factor associated with CKD among T2DM patients
Table 3 shows the multivariable analysis to determine the factor associated with CKD after controlling for the confounding factor. It can be concluded that the factors associated with undiagnosed hypertension were age group. The trend of age group increases in adjusted OR by increasing age group compared to the reference group (less than 40 years old). Female has almost 2 times the odds of having CKD compared to male [Adj. OR: 1.974 (95%CI: 1.460, 2.669). Increasing one unit of triglyceride was associated with an increase of almost 1.3 odds of having CKD. However, one unit increase in HDL was associated with reduced 0.663 odds of having CKD. Those patients who received CBB have protected of having CKD compared to those who did not receive CCB [Adj. OR = 0.658 (95%CI: 0.499, 0.868)].
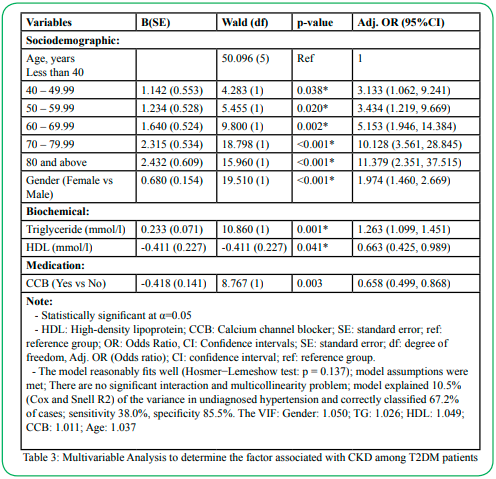
Table 3: Multivariable Analysis to determine the factor associated with CKD among T2DM patients
Diagnostic Tests for the Multiple Logistic Model
The null hypothesis shows that the model adequately fits well (Hosmer−Lemeshow test: p = 0.138). The checking of multicollinearity reveals that no collinearity exists among the independent variables as the variance inflation factor is less than 10 (VIF: Gender = 1.050, TG= 1.026, HDL = 1.049, CCB = 1.011, Age = 1.037). The model explained 10.5% (Cox and Snell R2) of the variance in undiagnosed hypertension. In the case to create the model, the sensitivity was 38.0%, and the specificity was 85.5%. Overall, 67.2% of the cases are classified correctly. Figure 1 shows the area under the received operative characteristic curve (AUROC). It can be concluded that the statistical model can discriminate 68.8% [95%CI: 65.4, 73.5), p<0.001]) to predict CKD among T2DM patients.
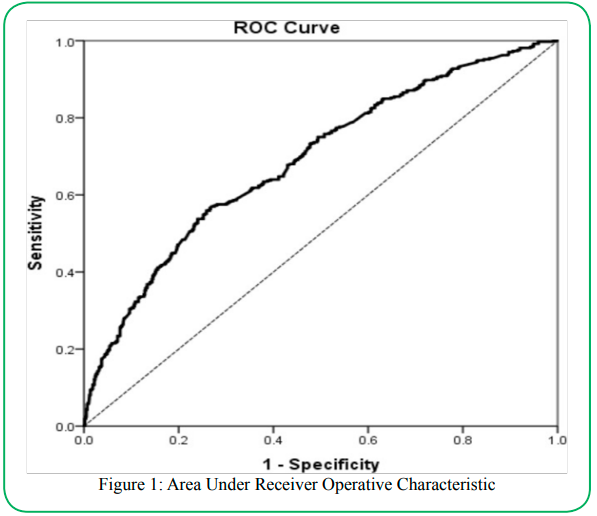
Figure 1: Area Under Receiver Operative Characteristic
Discussion
The prevalence of CKD among T2DM patients at PKD Padang Terap was 38.6% (95% CI: 35.5, 41.7). This finding was higher compares to the majority of a similar study done in other countries which found the prevalence of CKD of less than 30% [31]. The location of the study conducted explained the variety of ranges for the prevalence of CKD [31]. It is expected that the prevalence is lower compared to the tertiary setting and the prevalence differs between developing and developed countries.
The systolic blood pressure (SBP) and HbA1 were higher compared to the recommendation by Clinical Practice Guideline (CPG) management of diabetes mellitus in Malaysia [32]. HbA1c is the primary indicator to evaluate diabetes control worldwide. Malaysia has adopted a yearly audited program by National Diabetes Registries with a target of more than 30% from the randomly selected patient to have HbA1c of less than 6.5% [33]. Another finding from the distribution of is the biochemical investigation is Fasting Lipid Profile (FSL) consists of total cholesterol, LDL and TG. Their mean value was higher than the recommendation by the Ministry of Health Malaysia. However, the mean of HDL with more than 1.2 mmol/l, which can reduce the CKD incidence [34]. The high incidence of CKD will have resulted from inadequate control of the parameter that was highlighted in the guideline, subsequently increasing their prevalence [35].
The prevalence of overweight and obesity in this population was 38.8% and 24.5%, respectively. The prevalence of overweight and obesity was higher compared to national prevalence which was 30.4% (95% CI: 29.00, 31.90) and 19.7%, (95% CI: 18.43, 21.13), respectively [36]. Malaysia has the highest prevalence of obesity among adults in South East Asia and is a risk factor for various non-communicable diseases.
Age was found to be the risk factor of CKD among T2DM patients in this study. Increasing age leads to increased risk for CKD progression in most studies in similar fields [8,10,11]. The kidneys are affected by the ageing process which resulted from several morphological and functional process alterations along the course; thus the kidney disease has also been found to be more dominant in those over the age of 60 when compared to the rest of the general population [37]. A recent report by National Diabetic Registry (NDR) has found that the mean age for Malaysians to be diagnosed with T2DM is 53 years old [33]. However, NHMS 2019 reported that the prevalence of raised blood glucose among not known diabetes status was 8.9% (95% CI: 7.96, 9.93) and the majority of the participants presented at age group lower than 50 years old [1]. Therefore, an extensive screening program should be able to early detection of diabetic patients and the initiation of the treatment to prevent complications such as CKD.
Females were found a higher risk of CKD among T2DM patients compared to males [adj. OR (1.974 (95%CI: 1.460, 2.669)]. This finding corresponded to the study by Tannor et al., [24] in Ghana. However, a study by De Cosmo et al., [22] reported that only the male sex was associated with CKD. A review report in 2006 found that the incidence of CKD among males was higher because they were more susceptible to age-related glomerulosclerosis than females [18].
This study found that T2DM patients who are treated with calcium channel blocker (CCB) have a protective factor to develop CKD [adj. OR: 0.658 (95%CI: 0.449, 0.868)]. A Randomized Controlled Trials (RCTs) on angiotensin-converting enzyme inhibitor (ACEi) and angiotensin II receptor blockers (ARBs) in Type 1 and Type 2 DM showed that the risk of end-stage of renal disease (ESRD) was significantly reduced by 40% with ACEi and 22% with ARB when compared to placebo [38]. In Malaysia, ACEi and ARB are the most recommended antihypertensive agents used to treat hypertension among CKD patients with or without proteinuria and should be used as the first-line treatment [39]. As for CCB, even the effectiveness for hypertension control is unquestionable, however, the evidence for the renoprotective effect is not conclusive. In clinical practices, CCBs can be added as a second-line therapy to RAS blockers in the management of CKD as a safe and reasonable approach to optimize blood pressure control [39].
Chronic kidney disease (CKD) is associated with dyslipidaemia comprising high triglycerides, low HDL and altered lipoprotein composition [40,41]. Dyslipidaemia is common in diabetes patients and diabetic dyslipidaemia is also correlated with diabetic nephropathy and CVD [42,43]. Based on the biochemical findings in this study, triglyceride was found to be the risk [adjOR: 1.263 (95%CI: 1.099, 1.451)] and HDL was found to be the protective factor [adj. OR: 0.663 (95%CI: 0.425, 0.989)] for the CKD among T2DM patients.
A study by Keiko et al., [44] found low HDL cholesterol to be a predictor of chronic kidney disease progression especially in female patients with CKD under 70 years of age. The kidney survival rate in the low HDL group was significantly lower than that in the high HDL group. Therefore, it is very important to clinicians when determining the expected prognosis of CKD in patients [44]. The LDL was independently associated with an increased likelihood of estimated glomerular filtration rate (eGFR) decline and development of incident CKD in the general Zhejiang population [45]. The use of cholesterol-lowering agents appears to be indicated in early CKD stages to prevent atherosclerosis-related risk [46]. It is suggested to start LDL cholesterol-lowering treatment in stages 1 to 4 CKD patients with pre-existing cardiovascular events or those with multiple risk factors and at high risk for coronary heart disease and when the LDL cholesterol level is more than 1.8 mmol/l [43].
Several screening tools can be used for the identification of CKD among T2DM patients. Early initiation of treatment may halt the CKD progression thus resulting in a better prognosis for the patients. The health care provider may perform periodic estimates of glomerular filtration rate (eGFR) and monitor other biochemical markers such as anaemia and proteinuria status. Regular training should be provided to enhance the clinical competence in managing the CKD [47].
Limitation
There were some limitations while conducting this study. The cross-sectional observational study has the disadvantage of causal inference as the study design was unable to measure temporality based on Bradford Hill's criteria. Secondary data from the National Diabetes Registry (NDR) used in this study has a lack of control over the quality of data because the researcher did not participate in the data collection processes [48]. Although this study was conducted using a universal sampling method in selecting the sample, however, its coverage was limited to the patients that have registered and audited in the National Diabetes Registry (NDR). This study was conducted at a single health care centre and has limited by the unique character of the current facilities based on the distributions of the variables Thus, the generalizability of our finding to other T2DM populations in Malaysia is uncertain and warrants further study.
Conclusion
The final model has illustrated age, female, triglyceride, high-density lipoprotein and treating with calcium channel blocker were found to be significant factors for CKD among T2DM patients. Treating patients with anti-hypertensive and anti- hyperlipidemic are very important to reduce the prevalence of CKD among T2DM patients.
Acknowledgement
I would like to acknowledge the immense contribution of study participants for agreeing to be part of the study.
Funding
This is self-funded research and did not receive any funding.
Conflict of interest
All authors declare that there is no conflict of interest.
References
Institute for Public Health (IPH). (2020). National Health and Morbidity Survey (NHMS) 2019: Vol. I: NCDs – Non-Communicable Diseases: Risk Factors and other Health Problems.View
Ministry of Health Malaysia. (2011). National Health and Morbidity Survey 2011 (NHMS 2011). Vol. II: Non-Communicable Diseases. National Institutes of Health, Ministry of Health Malaysia. View
Ministry of Health Malaysia. (2015). National Health and Morbidity Survey 2015 (NHMS 2015): Non-Communicable Diseases, Risk Factors & Other Health Problems (Vol. II). National Institutes of Health, Ministry of Health Malaysia.
Alemu, H., Hailu, W., & Adane, A. (2020). Prevalence of Chronic Kidney Disease and Associated Factors among Patients with Diabetes in Northwest Ethiopia: A Hospital Based Cross-Sectional Study. Curr Ther Res Clin Exp, 92, 100578. https:// doi.org/10.1016/j.curtheres.2020.100578 View
Duan, J. Y., Duan, G. C., Wang, C. J., Liu, D. W., Qiao, Y. J., Pan, S. K., Jiang, D. K., Liu, Y., Zhao, Z. H., Liang, L. L., Tian, F., & Liu, Z. S. (2020). Prevalence and risk factors of chronic kidney disease and diabetic kidney disease in a central Chinese urban population: a cross-sectional survey. BMC Nephrol, 21(1), 115. https://doi.org/10.1186/s12882-020-01761-5View
Jitraknatee, J., Ruengorn, C., & Nochaiwong, S. (2020). Prevalence and Risk Factors of Chronic Kidney Disease among Type 2 Diabetes Patients: A Cross-Sectional Study in Primary Care Practice. Sci Rep, 10(1), 6205. https://doi.org/10.1038/ s41598-020- 63443-4View
Low, S. K., Sum, C. F., & Yeoh, L. Y. (2015). Prevalence of Chronic Kidney Disease in Adults with Type 2 Diabetes Mellitus. View
Lu, B., Song, X., Dong, X., Yang, Y., Zhang, Z., Wen, J., Li, Y., Zhou, L., Zhao, N., Zhu, X., & Hu, R. (2008). High prevalence of chronic kidney disease in population-based patients diagnosed with type 2 diabetes in downtown Shanghai. J Diabetes Complications, 22(2), 96-103. https://doi.org/10.1016/j. jdiacomp.2007.08.001View
Metsarinne, K., Broijersen, A., Kantola, I., Niskanen, L., Rissanen, A., Appelroth, T., Pontynen, N., Poussa, T., Koivisto, V., Virkamaki, A., & Investigators, S. T. o. N. i. D. S. (2015). High prevalence of chronic kidney disease in Finnish patients with type 2 diabetes treated in primary care. Prim Care Diabetes, 9(1), 31-38. https://doi.org/10.1016/j.pcd.2014.06.001View
Mubarakali N Janmohamed, Samuel E Kalluvya, Andreas Mueller, Rodrick Kabangila, Luke R Smart, Jennifer A Downs, & Robert N Peck. (2013). Prevalence of chronic kidney disease in diabetic adult out-patients in Tanzania. BMC Nephrology, 14, 183. View
Nazzal, Z., Hamdan, Z., Masri, D., Abu-Kaf, O., & Hamad, M. (2020). Prevalence and risk factors of chronic kidney disease among Palestinian type 2 diabetic patients: a cross sectional study. BMC Nephrol, 21(1), 484. https://doi.org/10.1186/ s12882-020-02138- 4View
Ohta, M., Babazono, T., Uchigata, Y., & Iwamoto. (2010). Comparison of the prevalence of chronic kidney disease in Japanese patients with Type 1 and Type 2 diabetes. 27(9), 1017-1023.View
Rodriguez-Poncelas, A., Garre-Olmo, J., Franch-Nadal, J., Diez-Espino, J., Mundet-Tuduri, X., Barrot-De la Puente J, Coll-de Tuero, G., & RedGDPS Study Group. (2013). Prevalence of chronic kidney disease in patients with type 2 diabetes in Spain: PERCEDIME2 study. BMC Nephrology, 4, 46. View
Levey, A.S, Eckardt, K.U, Tsukamoto, Y., Levin, A., Coresh, J., Rossert, J., Zeeuw, D.D., Hostetter, T.H, Lameire, N., & Eknoyan, G. (2005). Definition and classification of chronic kidney disease: a position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int, 67(6), 2089-2100. https://doi.org/10.1111/j.1523- 1755.2005.00365.xView
Hajhosseiny, R., Khavandi, K., & Goldsmith, D.J. (2013). Cardiovascular disease in chronic kidney disease untying the Gordian knot. Int J Clin Pract, 67(1), 14-31. https://doi. org/10.1111/j.1742-1241.2012.02954.xView
Anderson, S., Halter, J.B, Hazzard, W.R., Himmelfarb, J., Horne, F.M., Kaysen, G.A., Kusek, J.W., Nayfield, S.G., Schmader, K., Tian, Y., Ashworth, J.R., Clayton, C.P., Parker, R.P., Tarver, E.D., Woolard, N.F., High, K.P., & and for the workshop participants. (2009). Prediction, Progression, and Outcomes of Chronic Kidney Disease in Older Adults. Journal of The American Society of Nephrology, 20(6), 1199-1209. https://doi.org/10.1681/ASN.2008080860View
Foley, R.N., Parfrey, P.S., & Sarnak, M.J. (1998). Epidemiology of cardiovascular disease in chronic renal disease. J Am Soc Nephrol, 9(12 Suppl), 16-23. View
Taal, M. W., & Brenner, B. M. (2006). Predicting initiation and progression of chronic kidney disease: Developing renal risk scores. Kidney Int, 70(10), 1694-1705. https://doi.org/10.1038/ sj.ki.5001794 View
Amin, R., Turner, C., van Aken, S., Bahu, T. K., Watts, A., Lindsell, D. R., Dalton, R. N., & Dunger, D. B. (2005). The relationship between microalbuminuria and glomerular filtration rate in young type 1 diabetic subjects: The Oxford Regional Prospective Study. Kidney Int, 68(4), 1740-1749. https://doi. org/10.1111/j.1523- 1755.2005.00590.xView
Low, S.K.M, Sum, C.F, Yeoh, L.Y, Tavintharan, S., Ng, X.W., Lee, S.B.M., Tang, W.E.e, & Lim, S.C. (2015). Prevalence of Chronic Kidney Disease in Adults with Type 2 Diabetes Mellitus. Ann Acad Med Singap, 44(5), 164-171.View
Metsärinne, K., Bröijersen, A., Kantola, I., Niskanen, L., Rissanen, A., Appelroth, T., Pöntynen, N., Poussa, T., Koivisto, V., & Virkamäki, A. J. P. c. d. (2015). High prevalence of chronic kidney disease in Finnish patients with type 2 diabetes treated in primary care. 9(1), 31-38View
De Cosmo, S., Viazzi, F., Pacilli, A., Giorda, C., Ceriello, A., Gentile, S., Russo, G., Rossi, M. C., Nicolucci, A., Guida, P., Pontremoli, R., & Group, A. M.-A. S. (2016). Predictors of chronic kidney disease in type 2 diabetes: A longitudinal study from the AMD Annals initiative. Medicine (Baltimore), 95(27), e4007. https://doi.org/10.1097/MD.0000000000004007View
Duan, J.-Y., Duan, G.-C., Wang, C.-J., Liu, D.-W., Qiao, Y.-J., Pan, S.-K., Jiang, D.-K., Liu, Y., Zhao, Z.-H., & Liang, L.-L. J. B. n. (2020). Prevalence and risk factors of chronic kidney disease and diabetic kidney disease in a central Chinese urban population: a cross-sectional survey. BMC Nephrology, 21, 115.View
Tannor, E. K., Sarfo, F. S., Mobula, L. M., Sarfo-Kantanka, O., Adu-Gyamfi, R., & Plange Rhule, J. (2019). Prevalence and predictors of chronic kidney disease among Ghanaian patients with hypertension and diabetes mellitus: A multicenter cross-sectional study. J Clin Hypertens (Greenwich), 21(10), 1542- 1550. https://doi.org/10.1111/jch.13672View
Lu, B., Song, X., Dong, X., Yang, Y., Zhang, Z., Wen, J., Li, Y., Zhou, L., Zhao, N., Zhu, X. J. J. o. D., & Complications, i. (2008). High prevalence of chronic kidney disease in population-based patients diagnosed with type 2 diabetes in downtown Shanghai. J Diabetes Complications, 22(2), 96-103.View
Serena, KM Low., Chee Fang Sum., & Yeoh, L. Y. (2015). Prevalance of Chronic Kidney Disease in Adult with Type 2 Diabetes Mellitus.View
Antonio Rodriguez-Poncelas, Josep Garre-Olmo, Josep Franch-Nadal, Javier Diez-Espino, Xavier Mundet-Tuduri, Joan Barrot-De la Puente, & Tuero, G. C.-d. (2013). Prevalence of chronic kidney disease in patients with type 2 diabetes in Spain: PERCEDIME2 study.View
Jha, V., Garcia-Garcia, G., Iseki, K., Li, Z., Naicker, S., Plattner, B., Saran, R., Yee-Moon, W.A, & Yang, C.W. (2013). Chronic kidney disease: global dimension and perspectives. Lancet, 382(9888), 260-272. https://doi.org/10.1016/S0140- 6736(13)60687-X.View
Ministry of Health Malaysia. (2020b). National Diabetes Registry (NDR) Report 2013-2019. View
Ministry of Health Malaysia. (2018). CPG Management of Chronic Kidney Disease (Second Edition). Medical Development Division, Ministry of Health Malaysia. View
Koye, D. N., Magliano, D. J., Nelson, R. G., & Pavkov, M. E. (2018). The Global Epidemiology of Diabetes and Kidney Disease. Adv Chronic Kidney Dis, 25(2), 121- 132. https://doi. org/10.1053/j.ackd.2017.10.011View
Ministry of Health Malaysia. (2020a). CPG Management of Type 2 Diabetes Mellitus (6 ed.). Medical Development Division, Ministry of Health Malaysia.
Ministry of Health Malaysia. (2020c). National Diabetes Registry (NDR)Report 2013-2019.
Ministry of Health Malaysia. (2017). CPG Management of Dyslipidemia (5th Edition of Clinical Practice Guidelines). Health Technology Assessment Unit.
Koye, D. N., Shaw, J. E., Reid, C. M., Atkins, R. C., Reutens, A. T., & Magliano, D. J. (2017). Incidence of chronic kidney disease among people with diabetes: a systematic review of observational studies. Diabet Med, 34(7), 887-901. https://doi. org/10.1111/dme.13324View
Ministry of Health Malaysia. (2020d). National Health and Morbidity Survey (NHMS) 2019:NCDs – Non-Communicable Diseases: Risk Factors and other Health Problems (Vol. 1). Institute for Public Health (IPH), National Institutes of Health.
Nitta, K., Okada, K., Yanai, M., & Takahashi, S. (2013). Aging and chronic kidney disease. Kidney Blood Press Res, 38(1), 109-120. https://doi.org/10.1159/000355760View
Zhang, Y., He, D., Zhang, W., Xing, Y., Guo, Y., Wang, F., Jia, J., Yan, T., Liu, Y., & Lin, S. (2020). ACE Inhibitor Benefit to Kidney and Cardiovascular Outcomes for Patients with Non-Dialysis Chronic Kidney Disease Stages 3-5: A Network Meta-Analysis of Randomised Clinical Trials. Drugs, 80(8), 797-811. https://doi.org/10.1007/s40265- 020-01290-3View
Ministry of Health. (2018). CPG Management of Chronic Kidney Disease (Second Edition). Medical Development Division, Ministry of Health Malaysia.View
Cohen, D.E, & Fisher E.A. (2013). Lipoprotein metabolism, dyslipidemia, and nonalcoholic fatty liver disease. Semin Liver Dis 33, 380-388.View
Tannock Lisa. (2018). Dyslipidemia in Chronic Kidney Disease. Endotext [Internet]. https://www.ncbi.nlm.nih.gov/books/ NBK305899/
Chen Szu-chi, & Tseng Chin-Hsiao. (2013). Dyslipidemia, Kidney Disease, and Cardiovascular Disease in Diabetic Patients. The Review of Diabetic Studies, 10, 2-3. https://doi. org/10.1900/RDS.2013.10.8View
European Association for Cardiovascular Prevention & Rehabilitation, Reiner, Z., Catapano, A.L., De Backer, G., Graham, I., Taskinen, M.R., Wiklund, O., Agewall, S., Alegria, E., Chapman, M.J., Durrington, P., Erdine, S., Halcox, J., Hobbs, R., Kjekshus, J., Filardi, P.P., Riccardi, G., Storey, R.F., & Wood, D. (2011). ESC/EAS guidelines for the management of dyslipidaemias: the task force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). Eur Heart J, 32, 1769–1818.View
Keiko Kawachi, Hiroshi Kataoka, Shun Manabe, Toshio Mochizuki, & Kosaku Nitta. (2019). Low HDL cholesterol as a predictor of chronic kidney disease progression: a cross classifcation approach and matched cohort analysis. Heart and Vessels, 34, 1440-1455. https://doi.org/10.1007/s00380-019- 01375-4View
Xudong Liang, Meiyu Ye, Mei Tao, Danna Zheng, Ruyi Cai, Yifan Zhu, Juan Jin, & Qiang He. (2020). The association between dyslipidemia andthe incidence of chronic kidney disease inthe general Zhejiang population. BMC Nephrology, 21, 252. https://doi.org/10.1186/s12882-020-01907-5View
Massy ZIad A, & de Zeew D. (2013). LDL cholesterol in CKD - to treat of not to treat? Kidney International, 84, 451-456. View
Cueto-Manzano, A. M., Martínez-Ramírez, H. R., Cortés-Sanabria, L., & Rojas-Campos, E. (2017). The Role of Primary Health Care Professionals. In G. García-García, L. Y. Agodoa, & K. C. Norris (Eds.), Chronic Kidney Disease in Disadvantaged Populations (pp. 329-335). Academic Press. https://doi.org/ https://doi.org/10.1016/B978-0-12-804311-0.00031-5View
Johnston Melissa P. (2014). Secondary Data Analysis: A Method of which the Time Has Come. Qualitative and Quantitative Methods in Libraries (QQML) 3, 619-626.View