
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 6 (2022), Article ID: JPHIP-201
https://doi.org/10.33790/jphip1100201Review Article
The Global Impact of COVID-19 Misinformation and Politicization on Vaccination Compliance
Robert W Buckingham*, Renata Ferretti, Brittany Adams, & Timolin Kepon
University of Michigan, Flint, Michigan, United States.
Corresponding Author Details: Robert W Buckingham, PhD, Department of Public Health, University of Michigan, Flint, Michigan, United States. E-mail: bucking@umich.edu
Received date: 29th March, 2022
Accepted date: 21st April, 2022
Published date: 23rd April, 2022
Citation: Buckingham, R.W., Ferretti, R., Adams, B., & Kepon, T., (2022). The Global Impact of COVID-19 Misinformation and Politicization on Vaccination Compliance. J Pub Health Issue Pract 6(1): 201.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Vaccine hesitancy regarding the COVID-19 vaccine is widespread and disadvantageous. Anti-vax beliefs threaten health systems and open pathways for reemerging infectious diseases. In order to begin a return to normalcy around the world, high vaccination rates are necessary but are not currently being witnessed. This paper discusses two hypotheses to explain the hesitancy surrounding the COVID-19 vaccine: exposure to misinformation and the politicization of COVID-19. Misinformation and politicization by governments, political parties, and the media will continue to make the COVID-19 pandemic more harmful than it needs to be.
Keywords: Anti-vaccine Movement; COVID-19; Pandemic Misinformation; Politicization of COVID-19 vaccination; Vaccine Hesitancy.
Introduction
Rates of COVID-19 vaccination have increased all over the world. However, we have seen vaccine resistance in a significant portion of the world population. In some instances, this is due to a lack of access to the vaccine. However, most of this resistance is certainly due to vaccine misinformation in the media, social media, and political stances by various governmental leaders.
We, in the Public Health Community, are concerned about vaccine hesitancy and/or rejection of available effective vaccines. This hesitancy or rejection of vaccination will significantly impact resurgence and increase vaccine-preventable diseases. It is noted that online misinformation is one of the reasons for the public hesitancy or public denial to get vaccinated against COVID-19. The acknowledgment of an effective COVID-19 vaccine was created by the scientific community as a great achievement in such a short time frame. However, many governmental leaders were skeptical and hesitant to endorse the scientifical findings.
An effective and efficient way of increasing vaccine misinformation is through social media, such as Facebook and YouTube. Of course, many anti-vaccination websites are also widely available to the public. This has been frustrating and problematic for the scientific community.
Vaccine Hesitancy
The United States of America would receive 1.2 billion doses of the COVID-19 vaccine by the end of 2021 [7]. This number represents that the country in 2021 would have four doses of vaccine available for every person living in the country, considering that the U.S. on March 26th, 2022, is 332,585,425 [25]. However, as of March 20, 2022, only 65.38% of the American population were fully vaccinated, and only 558,410,936 doses were administrated (Table 1) [19,24]. So, if some countries like the United States of America have enough vaccines for the entire population, why is the percentage of people fully vaccinated lower than expected?
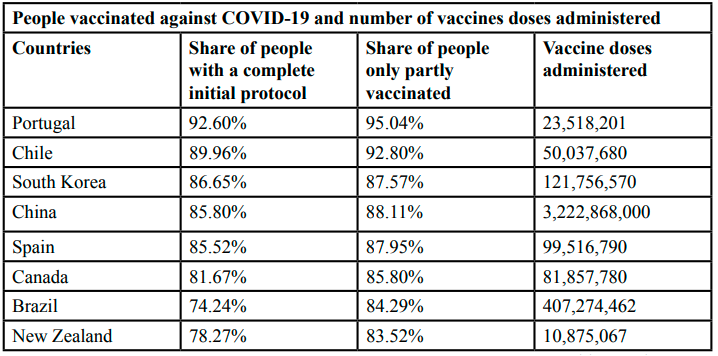
Table 1: Demographic data of all participants.
As news of the effectiveness of the COVID-19 vaccine emerged, people globally had different types of feelings such as optimism, joy, anxiety, fear, hesitation, among others. While positive sentiments led millions of people to seek a vaccine as soon as they were released, negative feelings may have delayed or even prevented the action of thousands of people worldwide. For example, a survey conducted before the availability of the COVID-19 vaccine in the United States identified that more than 55% of U.S. adults surveyed expressed hesitation in obtaining the vaccine. The study also identified reasons for vaccine hesitancy: efficacy, side effects, trust, policy, and convenience in production [9]. In England, the Center for Countering Digital Hate (CCDH) reported that one in six Britons would not accept to be vaccinated against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), and a similar proportion had yet to decide [3,5].
The World Health Organization (WHO) [27] considers vaccine hesitancy a threat to global health. According to WHO [27], vaccine hesitancy refers to "the reluctance or refusal to vaccinate despite the availability of vaccines." Even though the reasons why people choose not to vaccinate are complex, factors that may influence vaccine hesitancy are personal beliefs, such as safety concerns and skepticism about vaccine efficacy, exposure to online misinformation, and social networks [9]. With the COVID-19 pandemic, many people rejected the possibility of taking a vaccine against the coronavirus, even as scientists rushed to develop it [21].
The world is witnessing disinformation and denial of scientific evidence. The emergence of the COVID-19 pandemic was accompanied by a crisis of misinformation about the SARS-CoV-2 virus [8]. Likewise, COVID-19 has been politicized in different populations around the world. Many political leaders, such as former President Trump of the United States and Jair Bolsonaro of Brazil, were endorsing misleading claims about the disease and the vaccine [8,21]. Thus, we chose two hypotheses to explain vaccine hesitancy in the face of the COVID-19 crisis: exposure to misinformation and the politicization of COVID-19.
Crisis of Misinformation
Health misinformation has critical consequences concerning the quality of life and even their mortality risk [8]. According to The Pan American Health Organization [20], "misinformation is false or inaccurate information deliberately intended to deceive." In the context of the current pandemic, misinformation about all aspects of the COVID-19 disease has been circulating very quickly, and it can severely affect all aspects of life and human health, such as altering human behavior and potentially driving them to take great risks [1,20]. The susceptibility to misinformation about vaccines is related to many factors, such as a lack of education and scientific comprehension and decreased public trust in authority figures [9].
Most vaccine misinformation is based on rumor, stigma, and conspiracy theories, and they are fabricated and shared without any background or quality checking [15,20]. A study conducted between January 2020 and April 2020 identified 2,311 reports related to information about COVID-19 in 25 languages from 87 countries, circulated on online platforms, which included Facebook, Twitter, and online newspapers. Of the total, 89% of the reports were classified as rumors, 3.5% were stigma, and 7.8% were conspiracy theories. In addition, of the 2,276 posts that had the text available, 82% were false, 9% were correct, 8% were misleading, and 1% were not proven. Most reports were identified from the United States, China, India, Indonesia, Brazil, and Spain [15].
Digital communications on social media platforms are associated with misperceptions regarding basic COVID-19 facts, catalyzing the rapid spread of misinformation and threatening public health [1,17]. A study conducted in Canada that examined 0.6 million tweets found a large difference between the levels of misinformation on Twitter and in the news media; disinformation was comparatively more common on Twitter [1]. The spread of misinformation about vaccines is also very popular on social media and has grown with the COVID-19 pandemic [3,5,17]. According to the Center for Countering Digital Hate [5], in 2020, their investigation identified 409 English language anti-vaccine groups on Facebook that have 58 million followers, 7.8 million more followers than in 2019. On YouTube, anti-vaccine accounts have nearly 17 million subscribers, 7 million on Instagram, and 2 million followers on Twitter [5].
Parents who seek information about vaccines on social media have less accurate knowledge compared to parents who received information from a health professional [9]. For this reason, in 2019, several social media companies like Facebook, YouTube, and Twitter pledged to take action against the anti-vaccination movement. Facebook no longer recommends content that contains misinformation about vaccines. YouTube removed ads from anti-vaccination videos and started not paying the channel owners. Twitter has chosen to give preference to the National Health Service in the United Kingdom or the Department of Health and Human Services in the U.S. as the result of vaccine-related surveys [1,3]. Despite social media companies going to great lengths to suppress misinformation on their platforms, there continues to be a high level of misinformation regarding the facts of COVID-19 [1].
The misinformation makes the COVID-19 pandemic much more severe, harming more people and compromising the reach and sustainability of the global health system [20]. The United Nations Development Program has urged governments, researchers, healthcare professionals, information professionals, IT experts, policymakers, and social media experts to prevent the spread of misinformation about COVID-19 [17]. In these times of heightened misinformation, government leaders should be advised to use their voices to bolster trust in science, knowledge, and evidence-based decision-making [21].
The Politicization of covid-19
Science and politics are inevitably and often intertwined. Political actors often choose to cherry-pick science to support or diminish their preferred opinions, and COVID-19 was no exception. Public health experts have been “contradicted, muted, or even silenced when their recommendations do not align with political agendas” [14]. This interference in the scientific process undermines the trust and compliance necessary to handle a pandemic like COVID-19 successfully. Kang and Lee [12] state that pandemics threaten personal privacy, freedom of movement, and business activities needed for living. Because of this, decisions that are seemingly motivated by political desires are likely to cause anger and distrust among citizens. Experts disagree on the level of acceptable scientific politicization, with some arguing that any is too much, while others, like Schmid-Petri et al. [23], argue it is inevitable and necessary in order to make moral decisions. Bolsen & Palm [2] identify three different roots of the politicization of COVID-19: partisan divisions in public discourse, media coverage, and statements or actions by leading politicians.
COVID-19 has been politicized throughout different populations worldwide. Studies have indicated this is due primarily to differing levels of ideological politicization and trust in government and science [11]. Studies out of France indicate that both the Far Left and Far Right were more likely to be vaccine-hesitant and believe in hydroxychloroquine effectiveness despite scientific consensus stating otherwise [22,26]. Additionally, U.S. conservatives were less likely to participate in protective measures [11]. These factors were mainly due to mistrust of government decisions and either a complete distrust in science or simply apathy towards scientific facts. On the other end of the spectrum, people who were more likely to agree with scientific consensus were central voters in France or liberal voters in the U.S. [11,22]. A study comparing anti- or pro-mask Twitter hashtags by Lang et al. [13] illustrates this divide amongst the public. The study identified that while pro-mask tweets were the majority, most anti-mask tweets were wholly reactionary, indicating a level of anger and frustration in the discourse surrounding mask-wearing [13]. Conservatives are less likely to be conflict-averse and more likely to be reactive [28]. Lang et al. [13] theorize that bots on social media platforms might have used this fact to manipulate social media discourse surrounding the pandemic.
The news and media are essential to get information to the public, but many studies indicate its compliance in politicizing COVID-19. A report from Canada suggests that most journalists are untrained to report on scientific data specifically, so they lean on political debates and dramatizations surrounding the topic [4]. Further findings illustrated that reporters in Canada focused not only on scientific evidence but also on “transparency and leadership, duelling experts, and mixed messaging” regarding the pandemic [4]. Evolving public health decisions were primarily reported as leadership failures, conflicting opinions among scientists were used to criticize public health institutions, and frustrations over changing guidelines were used to fuel unhelpful political discourse. In the U.S., the focus of new stations on the social impacts of COVID-19 rather than the risks might have cemented the pandemic as “a threat to one’s way of life rather than a serious threat to one’s health” [10]. In India, the media was complicit in spreading fake videos of Muslims participating in acts to spread COVID-19 intentionally [6]. This was part of a larger politicization of COVID-19 in India and other countries that labeled oppressed groups as dirtier and more likely to carry COVID-19 than their majority counterparts.
The politicization of COVID-19 by governments is likely the most destructive of the three forms. In the U.S. and Europe, political parties used COVID-19 to support their positions. Prominently, President Donald Trump downplayed the risks associated with the pandemic then faced criticism for suggesting that rushing a vaccine would help him win the coming election [28]. Østebø et al. [18] on COVID-19 in Ethiopia discussed how the government postponed national and regional elections because of the pandemic and refused any suggestions for a temporary transitional government. A State of Emergency order was used to crack down on opposition events while political elites attended large gatherings unpunished [18]. Østebø et al. [18] quote that health in Ethiopia is used for “political control and surveillance, legitimizing the state and visions and ideologies of ruling elites, and as a strategic tool during times of war.” In Zimbabwe, the leading government, ZANU-PF, used lockdowns for similar reasons. Exemplifying the political nature of these decisions, Mutekwe & Vanyoro [16] cite that on July 19, 2020, 105,000 citizens had been arrested for lockdown-related crimes, but only 101,375 citizens had been tested for COVID-19. Laws were also created to arrest journalists for publishing “fake news” regarding the pandemic response, but, in reality, journalists faced jail time for any criticism of ZANU-PF [16].
Political actors, journalists, and scientists alike push the politicization of science forward. Scientific politicization has existed throughout “most of human history,” but leaders need to adapt their communication tools to conquer modern misinformation [2]. Citizens of the world must understand that “scientific knowledge is premised on the best available evidence, and it is continuously revised in light of new evidence” [14]. Because of this, uncertainty to some degree is inevitable in novel situations, but this uncertainty does not need to equal ineffective responses to future issues. Bolsen & Palm [2] suggest that in the future, effective communication must have mutual respect, incorporate both technical details alongside relatable storytelling, and be clear, consistent, understandable, and actionable. Any course correction must occur promptly, but inevitably, the “correction of false information has less effect than its initial communication” [22]. Countries with the most well-perceived responses, like New Zealand, the Republic of Korea, and Canada, were likely successful because of a bipartisan acceptance that COVID-19 does not discriminate by ideology, and therefore, politics should play very little into its reception.
Discussion
Our findings highlight that misinformation and the politicization surrounding COVID-19 are critical factors in the perpetuation of vaccine hesitancy. The consumption of misinformation surrounding COVID-19 was linked to less concern about the risks of contracting it and greater amounts of conspiratorial beliefs regarding the vaccine. Additionally, perceived politicization of the pandemic was linked to less trust in science and governments and, therefore, less trust in public health measures. The combination of these two issues can be attributed to the extreme rates of vaccine hesitancy currently being observed. Further research should focus on preparation for future outbreaks. Misinformation can be combatted, and politicization can be cast aside in times of turmoil, but this research and its solutions should be available before we face another crisis of this magnitude. Additionally, the media, social media platforms, politicians, and scientists are largely responsible for ensuring these issues do not continue to wager on. Scientifically backed information and suggestions should be considered over all else in the fight against COVID-19.
Conclusion
The purpose of this article was to summarize existing literature to provide explanations for COVID-19 vaccine hesitancy around the globe. We hypothesized that exposure to misinformation and the politicization of COVID-19 are primarily responsible for COVID-19 vaccine hesitancy. This paper contributes to a growing consensus that partisanship and any information found to be without scientific support should largely be eliminated in response to COVID-19.
Conflict of interest:
The authors declare no conflict of interest.
References
Bridgman, A., Merkley, E., Loewen, P.J., Owen, T., Ruths, D., Teichmann, L., Zhilin, O. (2020). The causes and consequences of COVID-19 misperceptions: Understanding the role of news and social media. The Harvard Kennedy School Misinformation Review, 1. Available at https://doi.org/10.37016/mr-2020-028View
Bolsen, T., & Palm, R. (2022). Politicization and COVID-19 vaccine resistance in the U.S. Progress in Molecular Biology and Translational Science, 81–100. Progress in Molecular Biology and Translational Science. Available at https://doi. org/10.1016/bs.pmbts.2021.10.002View
Burki, T. (2020). The online anti-vaccine movement in the age of COVID-19. The Lancet Digital-Health, 2.View
Capurro, G., Jardine, C. G., Tustin, J., & Driedger, M. (2021). Communicating scientific uncertainty in a rapidly evolving situation: a framing analysis of Canadian coverage in early days of COVID-19. BMC Public Health, 21(1):1–14. Available at https://doi.org/10.1186/s12889-021-12246-xView
Center for Countering Digital Hate Ltd (CCDH). (2020). The Anti-Vaxx Industry: How Big Tech powers and profits from vaccine misinformation. Available at https://cdn.centerforinquiry. org/wp-content/uploads/sites/33/2021/01/22170728/the_anti-vaxx-Industry.pdfView
Dey, S. (2021) Corona-logy: A Re-Configuration of Racial Dynamics in Contemporary India. Research in Social Change, 13(1):150-157. Available at https://doi.org/10.2478/rsc-2021- 0001View
Evenett, S.J., & Linley, M. (2021). How Much Surplus Vaccine Will the U.S. Have? Global Trade Alert, 69.View
Freiling, I., Krause, N.M., Scheufele, D.A., Brossard, D. (2021). Believing and sharing misinformation, fact-checks, and accurate information on social media: The role of anxiety during COVID-19. New Media & Society. Available at https:// doi.org/10.1177/14614448211011451View
Garett, R., & Young, S.D. (2021). Online misinformation and vaccine hesitancy. TBM, 11:2194–2199. Available at https://doi. org/10.1093/tbm/ibab128 View
Hubner, A. (2021). How did we get here? A framing and source analysis of early COVID-19 media coverage. Communication Research Reports, 38(2):112–120.View
Kerr, J., Panagopoulos, C., Van der Linden, S. (2021). Political polarization on COVID-19 pandemic response in the United States. Personality and Individual Differences, 179. Available at https://doi.org/10.1016/j.paid.2021.110892View
Kang, C., & Lee, I. (2021) COVID-19 Pandemic, Transparency, and “Polidemic” in the Republic of Korea. Asian Bioethics Review, 13 (2):213–224. Available at https://doi.org/10.1007/ s41649-021-00164-4View
Lang, J., Erickson, W. W., Jing-Schmidt, Z. (2021). #MaskOn! #MaskOff! Digital polarization of mask-wearing in the United States during COVID-19. PLoS ONE, 16(4):1–25. Available at https://doi.org/10.1371/journal.pone.0250817View
May, T. (2020). Anti-Vaxxers, Politicization of Science, and the Need for Trust in Pandemic Response. Journal of Health Communication, 25(10):761–763. Available at https://doi.org/1 0.1080/10810730.2020.1864519View
Islam, M.S., Sarkar, T., Khan, S.H., Kamal, A-H.M., Hasan, S.M.M., Kabir, A., Yeasmin, D., Islam, M.A., Chowdhury, A.I.A., Anwar, K.S., Chughtai, A.A., Seale, H. (2020) COVID-19–Related Infodemic and Its Impact on Public Health: A Global Social Media Analysis. The American Society of Tropical Medicine and Hygiene, 103(4):1621–1629. Available at https://doi.org/10.4269/ajtmh.20-0812View
Mutekwe, P., & Vanyoro, K. P. Politicising. (2021). “COVID-19”: an analysis of selected ZANU-PF officials’ 2020-2021 media statements on the pandemic in Zimbabwe. Acta Academica, 53(2):12–37. Available at https://doi.org/10.18820/24150479/ aa53i2/2View
Naeem, S.B., & Boulos, M.N.K. (2021). COVID-19 Misinformation Online and Health Literacy: A Brief Overview. International Journal of Environmental Research and Public Health, 18:8091. Available at https://doi.org/10.3390/ ijerph18158091View
Østebø, M. T., Østebø, T., Tronvoll, K. (2021). Health and politics in pandemic times: COVID-19 responses in Ethiopia. Health Policy & Planning, 36(10):1681–1689. Available at https://doi.org/10.1093/heapol/czab091View
Our World in Data. (2022) Coronavirus (COVID-19) Vaccinations. Available at https://ourworldindata.org/covid-vaccinationsView
Pan American Health Organization (PAHO). (2020). Understanding the infodemic and misinformation in the fight against COVID-19. Available at https://iris.paho.org/bitstream/ handle/10665.2/52052/Factsheet-infodemic_eng.pdfView
Pariente, N., on behalf of the PLOS Biology Staff Editors. (2020). We need leaders that believe in scientific evidence. PLOS Biology. Available at https://doi.org/10.1371/journal. pbio.3000992.View
Schultz, É., Atlani-Duault, L., Peretti-Watel, P., Ward, J. K. (2022). Does the public know when a scientific controversy is over? Public perceptions of hydroxychloroquine in France between April 2020 and June 2021. Therapies. Available at https://doi.org/10.1016/j.therap.2022.01.008View
Schmid-Petri, H., Bienzeisler, N., Beseler, A. (2022). Effects of politicization on the practice of science. Progress in Molecular Biology and Translational Science, 188[1]:45–63. Available at https://doi.org/10.1016/bs.pmbts.2021.11.005View
Statista. (2022). Number of COVID-19 vaccine doses administered worldwide as of March 21, 2022, by country. Available at https://www.statista.com/statistics/1194934/ number-of-covid-vaccine-doses-administered-by-county-worldwide/View
United States Census Bureau. (2022). U.S. and World Population Clock. Available at https://www.census.gov/popclock/View
Ward, J. K., Alleaume, C., Peretti-Watel, P. (2020). The French public’s attitudes to a future COVID-19 vaccine: The politicization of a public health issue. Social Science & Medicine, 265. Available at https://doi.org/10.1016/j. socscimed.2020.113414View
World Health Organization (WHO). (2019). Ten threats to global health in 2019. Available at https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019View
Young, D. G., Rasheed, H., Bleakley, A., Langbaum, J. B. (2022). The politics of mask-wearing: Political preferences, reactance, and conflict aversion during COVID. Social Science & Medicine, 298. Available at https://doi.org/10.1016/j. socscimed.2022.11483View