
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 6 (2022), Article ID: JPHIP-202
https://doi.org/10.33790/jphip1100202Review Article
A review on the Cost-Utility Analysis for the FELDA Residents in Malaysia with “Health Care Scheme (Skim Peduli Kesihatan) for the B40 Group” (PeKa B40) Coverage
Abdul-Hadi Mohd-Zuki, Mohamad-Rodi Isa*, Leny-Suzana Suddin
Department of Public Health Medicine, Faculty of Medicine, Universiti Teknologi MARA, Sungai Buloh Campus, Jalan Hospital, 47000 Sungai Buloh, Selangor, Malaysia.
Corresponding Author Details: Mohamad Rodi Isa, MBBS, DAP&E, MPH, DrPH, Department of Public Health Medicine, Faculty of Medicine, Universiti Teknologi MARA, Jalan Hospital, 47000 Sungai Buloh, Selangor, Malaysia.
Received date: 07th April, 2022
Accepted date: 27th April, 2022
Published date: 28th April, 2022
Citation: Mohd Zuki, A.H., Isa, M.R., & Suddin, L.S. (2022). A review on the Cost-Utility Analysis for the FELDA Residents in Malaysia with “Health Care Scheme (Skim Peduli Kesihatan) for the B40 Group” (PeKa B40) Coverage. J Pub Health Issue Pract 6(1): 202.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Introduction:
People with low socioeconomic status are always found to be one of the significant factors to determine their health status. The Malaysian government has initiated multiple programs to address the issues related to the health quality improvement of the population in line with the United Nations (UN) target for Universal Health Coverage (UHC). One of them is the “Health Care Scheme (Skim Peduli Kesihatan)” or PeKa B40 which was recently launched in 2019 to improve the target community's health status by offering several benefits obtained by the program including free health screening at private or public facilities concerning non-communicable diseases (NCDs). The cost-utility analysis study for the FELDA residents in Malaysia with “PeKA B40” coverage is needed to increase the understanding of the program's benefits and weaknesses during its implementation. It will help in identifying specific factors related to the utilization of the PeKa B40 program and will fill the gap in the economic evaluation of the government initiative. The policymaker may take into consideration of the discussion and recommendation to improve awareness among healthcare providers, especially at the primary care level. Concerning the Sustainable Development Goals (SDG), the study can give an impact on achieving good health and well-being (SDG 3.0).
Conclusion: In the 12th Malaysia Plan, the Malaysian government showed commitment to combat NCDs in line with the international target by targeting to reduce the NCDs prevalence by focusing on non-communicable diseases (NCDs). Therefore, a health reform commission needs to be established to improve the effectiveness, efficiency and equity of healthcare access to all residents mostly among B40 group in Malaysia.
Keywords: Cost-Utility Analysis, FELDA residents, Health Care Scheme, Low-income individuals.
Introduction
Malaysia is a developing country geographically located in Southeast Asia. Since its independence in 1957, Malaysia has successfully transformed itself from a poor income country to a middle-income country. The incidence of poverty has been drastically reduced from 49.3% in 1970 to 3.8% in 2010 and hardcore poverty was nearly eradicated in 2009 [1]. In 2021, Malaysia's population is estimated to be around 32.7 million [2] and they are categorised into three different income groups: Top 20% (T20 – represents the top 20% (top-income earners)) which comprise of 1.46 million households, Middle 40% (M40 – represents the medium 40% (average income earners) which comprise of 2.91 million households, and Bottom 40% (B40 – represents the bottom 40% (low-income earners) which comprises 2.91 million households [3].
The classification of different income groups is based on the household income shown in Table 1 [3].
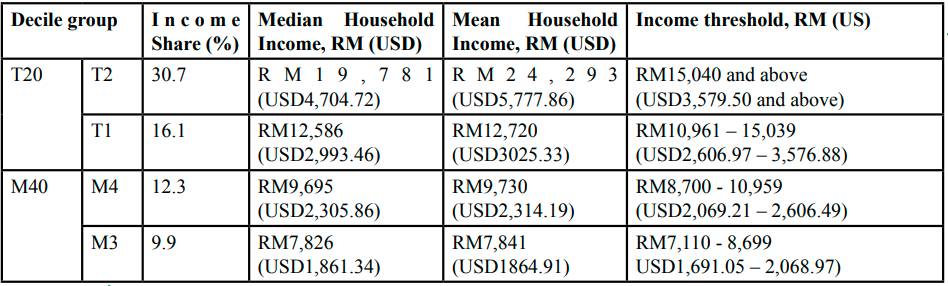
Table 1: Income Share, Median, Mean Household Income and Income Threshold by Household Decile Group, Malaysia, 2019
In Malaysia, the majority of the B40 group were presented in several states such as Sabah, Sarawak, Kelantan and Kedah, especially in the rural area. since the first New Economic Policy (NEP) was introduced in Malaysia. It was targeted to reduce the inequity of economic distribution among Malaysian citizens.
Federal Land Development Authority (FELDA)
Federal Land Development Authority (FELDA) or Lembaga Kemajuan Tanah Persekutuan, (LKTP) was established on 1 July 1956 under the Land Development Ordinance (now Land Development Act) 1956, given a specific mission by the government to handle the resettlement of rural poor into newly developing areas with agriculture as their main economic preference to improve their living status [4]. Between 1957 to 1990, there were 113,635 settlers were resettled in FELDA colonies throughout Malaysia on 811,140 hectares (2,004,400 acres) of land [4]. However, from 1996 onwards, there was no annual budget allocated to FELDA by the government. It believes that FELDA has the credibility to stand financially independent and becomes a statutory body that generates its income through diverse business activities.
Although there is an improvement in the economic status of the FELDA generations, the income level of the FELDA resident is still low and the majority of them are in the B40 category. It could be due to the geographical location of the FELDA as well as the migration of economic preference of government from agriculture to industrial [5]. The Malaysian government shows its commitment to reducing Development Goals (SDGs) (SDG 1) and No Poverty [6]. There are many suggestions to transmit assistance and welfare toward the poor and vulnerable. One of them was for the government to provide necessary social services such as free education, public utilities and health assistance with the target to improve the target group inequity [7].
Health Care Scheme (Skim Peduli Kesihatan) for the B40 group (PeKa B40)
Health Care Scheme (Skim Peduli Kesihatan) for the B40 group (PeKa B40) is a Malaysian government initiative via the Ministry of Health (MOH) which aims to sustain the healthcare needs of low-income groups by mostly focusing on non-communicable diseases (NCDs). On 27th September 2021, the Malaysia Prime Minister launched the 12th Malaysia Plan which highlighted the NCDs in the second theme, the fourth chapter on the commitment from the government in the next 5 years plan to encounter these issues with the focus on cancers, diabetes mellitus and mental health [8]. This program is a subsidiary financial protection plan to ensure health equity and equal access to the healthcare facilities among the B40 community [9].
This program has four benefits and the recipient must undergo health screening (benefit 1) in order to be eligible for health aid (benefit 2), completing cancer treatment incentive (benefit 3) and transport incentive (benefit 4). It is shown in Figure 1 [10].
Since launched in 2019, PeKa B40 was reported to diagnose many chronic diseases among the B40 community which was not been diagnosed before such as diabetes mellitus (10.4%), hyperlipidemia (29.8%), hypertension (13.8%) and mental health problem (1.6%) [11]. Even though this program had proven the success in diagnosing several chronic diseases among the targeted community, however during the implementation of this program there were only 40,119 people underwent the health screening program out of 800,000 eligible persons [12]. Underutilization of health services was considered a significant factor that contributed to a substantial case of avoidable mortality and morbidity.
Primary Health Care and Health Screening
After the 1978 International Conference on Primary Health in Alma Ata, where a unified agreement was reached for all governments and world communities in general to take responsibility for the promotion of their people's health, the idea of primary health care became well known. The declaration reaffirmed an individual's health as a state of complete well-being, not just the absence of disease; it also acknowledged the disparities in health between developed and developing countries, as well as the right of individuals to fully participate in the planning and implementation of health-care policies [13]. The primary health care system is intended to serve as the first point of contact for individuals in the community and to serve as the foundation for a long-term healthcare system based on practical, scientifically proven, and socially acceptable methods and technology that is made available to all families in the community at a cost that is both affordable to the community and the country [14].
The primary health care system was considered a way for developing countries to attain optimal health care for their populations [15]. One of the main functions of primary care is by providing healthcare screening services because the ability to detect disease in the early phase was associated with the prevention of illness and death in the long run [16]. The responsibility for health screening programs should be equally distributed between the public and private health facilities to ensure the served community gaining the utmost benefit from the program [17].
The Malaysia National and Health Morbidity Survey 2019 (NHMS 2019) reported that the prevalence of NCDs health screening in Malaysia was 33.3% [18]. This proportion was considered low compared to developed countries such as the United State of America (USA) who reported the prevalence of chronic disease screening
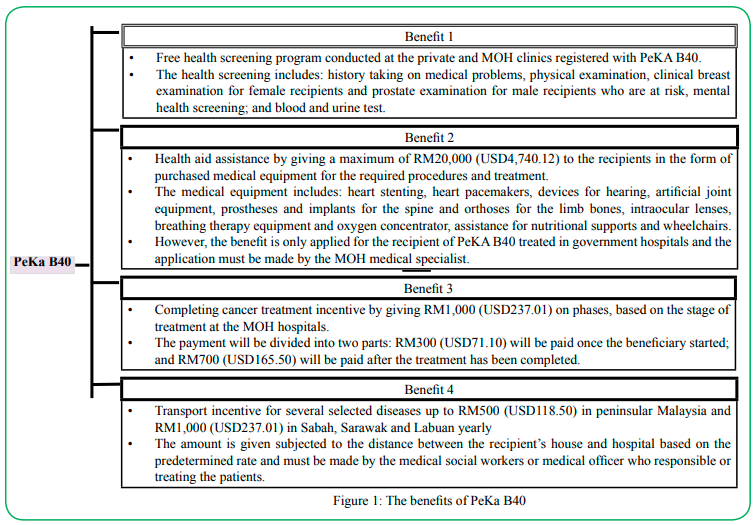
Figure 1: The benefits of PeKa B40
was increase from 46.8% in 2010 to 55.02% in 2017 [19]. Another study stated that for diabetes mellitus, the recommended proportion to be screened every year based on American Diabetes Association (ADA) for the person over 45 years old was approximately 76.6% [20]. However, several factors were reported to be the major reason that halted the community from utilizing the health screening services such as socioeconomic, accessible to healthcare facilities, belief and satisfaction [21].
Early health screening is useful in the detection of chronic diseases at an early stage before any symptoms become noticeable. Hence it will have the advantage of being able to treat the disease at an earlier stage before it complicated in the later stage [22]. At the same time, early health screening also has an important role to improve patient’s quality of life (QOL) [23]. However, socioeconomic factors have become an obstacle for a certain communities, especially among the B40 group to take part in the health screening activities [24]. Studies done in several countries found that the percentage of health screening for chronic diseases such as cancer is different according to the socio-economic status of the country and its residents [25]. A study by Lee et al. [26] in Taiwan on factors influencing the intention to utilize out-of-pocket health screening found that the fee charged by the healthcare provider will determine the individual ability to use the health services.
In Malaysia, the government has launched several initiatives to reduce the inequity related to health status by introducing the PeKa B40 program among low household income groups. This program contains several benefits including a health screening program and other incentives that will help to improve the health status and quality of life (QOL) among B40 groups [27]. Since this program was recently launched, there is limited evidence regarding its finding of this program. A study by Syed Ahmad Yunus et al. [28] in 2020 at the Klang Valley found that the proportion of people who were using this scheme was still low at 7.6% indicating the underutilized of government initiative among the targeted community. Multiple factors may contribute to the underutilization of government health services, hence a series of comprehensive strategies need to be the plan to provide a practical suggestion to the nation based on the data available in line with evidence-based medicine [29].
Health Seeking Behavior
Fatmi and Avan [30] reported that the utilization of health services mostly is a consequence of the health-seeking behaviour of individuals in the community and the behaviour has also been affected by several determinants such as physical, political, socioeconomic and sociodemographic. One of the factors under the health-seeking behaviour is self-rate general health status. A study in Jordan found that those who have poor self-rate health status are more likely to use healthcare services compare to those who self-rate better health status (p < 0.01). The authors reported that a person who responded with poor self-rate either on response day or for the past 12 months has a significant finding in determining the utilization of primary care services (p < 0.01) [31]. The same finding was reported in 2016 where a poor self-rate status increased the probability for that particular person to use health service compare to good self-rate health status (p = 0.003) [32]. However, this study found that people who seek traditional health treatment did not associated with the utilization of the health services (p value 0.093).
Self-treatment for the past 12 months was found to be the associated factor in the utilization of health services in Mongolia. Gan-Yadam et al. [33] reported that self-treatment reduced the visit to the healthcare facility (p < 0.001). The article also found that people that expose to the internet also tends to increase the utilization of healthcare facility compared to people who do not expose to the internet (p = 0.03). The family doctor concept or having contact with a usual healthcare provider reduced the utilization of healthcare services (p < 0.001) [34]. The presence of chronic pain also reduced health service utilization (p < 0.001) as well as the emergency department visit (p < 0.01) and hospitalization (p = 0.001) [35].
There are several reasons for people who did not use healthcare services. Based on research on the community with low socioeconomic status, Fantahun and Degu [36] highlighted a few reasons related to health-seeking behaviour:
i. the community has a cultural belief that some of their diseases do not need health attention from healthcare institutions.
ii. they have more tendency to buy the medication/drugs from the drug vendors to reduce the cost.
iii. some of them tend to visit the traditional healers' medication or used holy water to improve their health condition.
Some individuals may have the motivation to seek care at the health facilities or be demotivated due to certain enablers or barriers that present moment based on the societal expectation of norms [37]. Another factor that can affect health-seeking behaviour in determining health services utilization is the presence of chronic pain. Experience of having chronic pain would be very challenging with the issues of anxiety, depression and psychosomatic disorders as a patient usually struggle with worries, fear and insecurity about their condition. The patients often present with sleep disturbance, fatigue and activity limitation. All of the factors mentioned will lead to the health-seeking behaviour decision to utilize the health services [38].
Economic Evaluation - Cost-Utility Analysis (CUA)
In health economics, the economic concepts and methodologies are used to investigate and explain how people make decisions about their health behaviours and the use of health care. It also provides a framework for considering how society should allocate limited health resources to meet people's demand for health care services, as well as health promotion and prevention. The economic evaluation will generate evidence-based information to assist the healthcare manager to decide the allocation of resources [39]. The economic evaluation will consider both the cost and benefit parameters to help the healthcare provider to evaluate which of the treatment/services with the better result at the most effective cost. Due to limited resources present to the health sector, public health physicians must be decided to sacrifice the least effective services (opportunity cost) for the one with the highest priority at present [40]. There are several tools used to measure economic evaluation such as Cost-Benefit Analysis (CBA), Cost Minimization Analysis (CMA), Cost-Effective Analysis (CEA) and Cost-Utility Analysis (CUA). Each of the tools has its advantages and disadvantages and should be chosen wisely according to the type of comparison [41].
Cost-utility analysis (CUA) is an economic analysis in which the incremental cost of a program is compared to the incremental health improvement expressed in the unit of quality-adjusted life years (QALYs) [42]. This approach incorporates both the increase in survival time and changes in quality of life (QOL) into one measure. The incremental value ratio enables the cost of achieving a health benefit by treatment with a drug to be assessed against similar ratios calculated for other health interventions [43]. The results of cost-utility analyses are useful in many situations such as planning of service development, resource allocations and finding out the best available intervention for persons with a certain health status [44].
For example, one study in the US use the CUA to determine the efficiency of annual screening for diabetic retinopathy for two groups: high-risk group (diabetic patient with age more than 45 years old with HBa1c of more than 11%) and low-risk group (diabetic patient with age less than 65 years old with HBa1c less than 7%). After analysis, they found that the high-risk group cost an additional USD40,530 per QALY gained while those from the low-risk group required an additional USD211,570 per QALY gained [45].
CUA was also used in another study that measure the second eye cataract surgery effectiveness compared to unilateral pseudophakia. In the result, they found that the second eye cataract surgery resulted in USD2,727 per QALY gained compared to unilateral pseudophakia [46]. A study by Surendra et al. [47] in Malaysia compared the CUA for 2 types of interventions: hemodialysis (HD) and continuous ambulatory peritoneal dialysis (CAPD) for end-stage renal disease (ESRD) patients. The authors reported that the difference was RM46595 per QALY gain for HD and RM41,527 for CAPD. These findings have suggested a provision of both modalities is fiscally feasible and an increasing the CAPD as initial dialysis modality would be more cost-effective rather than straight away used of HD.
Quality of Life (QOL) among people who utilize health service
Several studies found that person that utilizes the health service will improve their QOL due to better control of chronic disease and well manage the acute problem [48]. A patient that has a low score of the physical domain in the QOL instrument tools is found to have an odds ratio of 0.93 (95% CI: 0.91 – 0.96) infrequent attend to healthcare facilities in Slovenia [49]. However, Kurpas et al. [50] found that the number of visits to a doctor was higher among patients with low QOL in all domains. A study by Agborsangaya et al. [51] found that patient with multiple comorbid wills has higher numbers of health facilities visits and was associated with lower QOL (EQ5D index score) by -0.12 (95% CI: -0.14 - -0.11).
Cost-Utility Study for the FELDA Residents with PeKa B40 Coverage in Malaysia
There are many significances in the study of the Cost-Utility for the FELDA Resident in Malaysia with PeKa B40 coverage. Since it has been launched in 2019, the study will increase the understanding of the program's benefits and weaknesses during its implementation. The program evaluation will also be done. It will help in identifying specific factors related to the utilization of the PeKa B40 program and will fill the gap in the economic evaluation of the government initiative.
The policymaker may take consideration of the discussion and recommendation by this study to improvise the current PeKa B40 guideline. It will improve awareness among healthcare providers, especially at the primary care level whether to encourage the B40 community to utilize the service or not and identify specific reasons for utilizing or non-utilized the service base on the qualitative study finding.
Concerning the Sustainable Development Goals (SDG), the study can give an impact on achieving good health and well-being (SDG 3.0). It can highlight the target of reducing premature mortality from NCDs and promoting mental health and well-being (Target 3.4). At the same time, it can emphasize Universal Health Coverage (UHC) including financial protection and access to quality and affordable essential health services and medicines (Target 3.8).
Conclusion
In the 12th Malaysia Plan, the Malaysian government showed commitment to combat NCDs in line with the international target by targeting to reduce the NCDs prevalence by focusing on cancers, cardiovascular disease (CVDs), diabetes mellitus and mental health problems. Due to the overwhelming COVID-19 pandemic, there was an overloaded backlog of 57,000 medical and surgical procedures. Therefore, a health reform commission needs to be established to improve the effectiveness, efficiency and equity of healthcare access to all residents mostly among B40 group in Malaysia.
Abbreviations
CAPD: continuous ambulatory peritoneal dialysis; COVID-19: Coronavirus Disease: CVD: cardiovascular disease; ED: emergency department; EPU: Economic Planning Unit; ESRD: end-stage renal disease; FELDA: Federal Land Development Authority; HD: hemodialysis; MOH: Ministry of Health, Malaysia; NCD: Non-communicable disease; NHMS: National & Health Morbidity Survey; PeKa B40: Skim Peduli Kesihatan for the B40 group (PeKA B40); QALYs: quality-adjusted life years; QOL: Quality of Life; SDG: Sustainable Development Goals: UHC: Universal Health Coverage.
Acknowledgement:
This review is part of the postgraduate student’s thesis write up.
Author’s contributions:
The authors were responsible for the article review and manuscript writing. The authors read and approved the final manuscript.
Funding:
This is a self-funding study
Declarations
Ethics approval and consent to participate:
This study was conducted in accordance with the Institutional Research Ethics and the declaration of Helsinki. Ethical approval for this research was obtained from UiTM Research Ethics Review Boards Committee (REC/04/2021 (MR/197)) in January 2022 and the Medical Research and Ethics Committee (MREC), Ministry of Health Malaysia (MOH) (NMRR-20-3082-57796 (IIR)) on March 2021.
Consent for publication:
Not applicable
Competing interests:
The author declares that he has no competing interests.
References
Hatta, Z., & Ali, I. (2013). Poverty Reduction Policies in Malaysia: Trends, Strategies and Challenges. Asian Culture and History, 5. https://doi.org/10.5539/ach.v5n2p48View
Department of Statistics, M. (2021). Department of Statistics Malaysia Official Portal. https://www.dosm.gov.myView
Fortune.com. (2021). Income Classification in Malaysia - The T20, M40 and B40. https://www.fortune.my/income-classifications-in-malaysia-the-t20-m40-and-bView
FELDA. (2019). FELDA - Mengenai Felda. Retrieved 16 January from https://www.felda.gov.my/umum/felda/mengenai-feldaView
Hussin, F., & Abdullah, H. (2012). The Role of FELDA and KESEDAR in the Development of Land in the District of Gua Musang: A Comparison the Socio-Economic Level of the Settlers. Sustainable Agriculture Research, 1, 284-291. https:// doi.org/10.5539/sar.v1n2p284View
UNDP Malaysia. (2020). SDG - Goal 1: No poverty. Retrieved 16 January from https://www.my.undp.org/content/malaysia/en/ home/sustainable-development-goals/goal-1-no-poverty.htmlView
Abdul-Hakim, R., Abdul-Razak, N., & Ismail, R. (2010). Does social capital reduce poverty? A case study of rural households in Terengganu, Malaysia. 14, 556-566. View
Economic Planning Unit. (2021). Twelfth Malaysia Plan, 2021- 2025 (Twelfth Plan), . https://www.epu.gov.my
ProtectHealth. (2019a). Peka B40. Retrieved 16 January from https://protecthealth.com.my/View
ProtectHealth. (2019b). Peka B40 - Manual for MOH Hospital. https://hqe2.moh.gov.my/v2/pusat-media/muat-turun/ category/22-peka-b40.html?download=90:manual-for-moh-hospitalView
Market, T. E. (2021, 16 Julai 2021). 'Worrying' data shows about 33% of B40 group detected with non-communicable disease via PeKA B40 health screening - MoH _ The Edge Markets. The Edge Markets. https://www.theedgemarkets.com/ article/worrying-data-shows-about-33-b40-group-detected-noncommunicable-disease-peka-b40-healthView
Bernama. (2019, August 4 2019). Age limit for PeKa B40 lowered to 40 - Health Ministry. https://www.nst.com.my/View
World Health Organization. (1978). Alma Ata Declaration. https://www.who.int/teams/social-determinants-of-health/ declaration-of-alma-ataView
Shi, L. (2012). The impact of primary care: a focused review. Scientifica, 2012, 432892-432892. https://doi. org/10.6064/2012/43289View
Chatora, R. R., & Tumusime, P. (2004). Primary health care: a review of its implementation in sub-Saharan Africa. Primary Health Care Research & Development, 5(4), 296-306. https://doi.org/10.1191/1463423604pc220oaView
Bell Neil R, Thériault Guylène, Singh Harminder, & Grad Roland. (2019). Measuring what really matters: Screening in primary care. Canadian family physician Medecin de famille canadien, 65(11), 790-795. https://pubmed.ncbi.nlm.nih. gov/31722909View
Wee, L. E., Cher, W. Q., Sin, D., Li, Z. C., & Koh, G. C.-H. (2016). Primary care characteristics and their association with health screening in a low-socioeconomic status public rental-flat population in Singapore- a mixed methods study. BMC Family Practice, 17(1), 16. https://doi.org/10.1186/s12875-016-0411-5View
Institute for Public Health (IPH). (2019). NHMS2019 - Healthcare Demand. National Institutes of Health, Ministry of Health Malaysia,.View
Tran, P., Tran, L., & Tran, L. (2019). Impact of rurality on diabetes screening in the US. BMC Public Health, 19(1), 1190. https://doi.org/10.1186/s12889-019-7491-9View
Kiefer, M. M., Silverman, J. B., Young, B. A., & Nelson, K. M. (2015). National patterns in diabetes screening: data from the National Health and Nutrition Examination Survey (NHANES) 2005-2012. Journal of general internal medicine, 30(5), 612- 618. https://doi.org/10.1007/s11606-014-3147-8View
Chien, S.-Y., Chuang, M.-C., & Chen, I. P. (2020). Why People Do Not Attend Health Screenings: Factors That Influence Willingness to Participate in Health Screenings for Chronic Diseases. International journal of environmental research and public health, 17(10), 3495. https://doi.org/10.3390/ ijerph17103495View
InformedHealth.org. (2019). Benefits and risks of screening tests. Institute for Quality and Efficiency in Health Care (IQWiG). Retrieved 16 January from https://www.ncbi.nlm.nih. gov/books/NBK279418/View
Demidova, T., & Plakhotnyaya, V. J. M. S. (2021). Prediabetes. A new paradigm for early prevention of cardiovascular disease. 124-132.
Paula B. (2014). What are health disparities and health equity? We need to be clear. Public health reports (Washington, D.C. : 1974), 129 Suppl 2(Suppl 2), 5-8. https://doi. org/10.1177/00333549141291S203View
Akinyemiju, T. F. (2012). Socio-Economic and Health Access Determinants of Breast and Cervical Cancer Screening in Low-Income Countries: Analysis of the World Health Survey. PLOS ONE, 7(11), e48834. https://doi.org/10.1371/journal. pone.0048834View
Lee, Y. S., Chiu, Y. L., Liao, H. L., Chen, J. T., & Lee, F. C. (2010). Factors influencing the intention to utilize out-of-pocket health checkup services: A sample of citizens from 12 townships of Taichung County in Taiwan. J Chin Med Assoc, 73(5), 252- 259. https://doi.org/10.1016/s1726-4901(10)70054-xView
ProtectHealth. (2021). Protect Health. Retrieved 26.11.2021 from https://protecthealth.com.my/View
Syed Ahmad Yunus, S. Z., Wan Puteh, S. E., Ali, A., & Daud, F. (2021). The Covid Impact to Public Healthcare Utilization Among Urban Low-Income Subsidized Community in Klang Valley Malaysia. Health Services Research and Managerial Epidemiology, 8, 233339282110024. https://doi. org/10.1177/23333928211002407View
Hu, H., Jian, W., Fu, H., Zhang, H., Pan, J., & Yip, W. (2021). Health service underutilization and its associated factors for chronic diseases patients in poverty-stricken areas in China: a multilevel analysis. BMC Health Services Research, 21(1), 707. https://doi.org/10.1186/s12913-021-06725-5View
Fatmi, Z., & Avan, B. (2002). Demographic, socio-economic and environmental determinants of utilisation of antenatal care in a rural setting of Sindh, Pakistan. JPMA. The Journal of the Pakistan Medical Association, 52, 138-142.View
Alkhawaldeh, A., Holm, M. B., Qaddumi, J., Petro, W., Jaghbir, M., & Al Omari, O. (2014). A Cross-Sectional Study to Examine Factors Associated with Primary Health Care Service Utilization among Older Adults in the Irbid Governorate of Jordan. Current Gerontology and Geriatrics Research, 2014, 735235. https:// doi.org/10.1155/2014/735235View
Gurung, L., Paudel, G., & Yadav, U. J. J. o. M. M. I. o. H. S. (2016). Health service utilization by elderly population in urban Nepal: a cross-sectional study. 2, 27-36.
Gan-Yadam, A., Shinohara, R., Sugisawa, Y., Tanaka, E., Watanabe, T., Hirano, M., Tomisaki, E., Morita, K., Onda, Y., Tokutake, K., Mochizuki, Y., Matsumoto, M., Sugita, C., & Anme, T. (2013). Factors associated with health service utilization in Ulaanbaatar, Mongolia: a population-based survey. Journal of epidemiology, 23(5), 320-328. https://doi. org/10.2188/jea.je20120123View
Tountas, Y., Oikonomou, N., Pallikarona, G., Dimitrakaki, C., Tzavara, C., Souliotis, K., Mariolis, A., Pappa, E., Kontodimopoulos, N., & Niakas, D. J. H. s. m. r. (2011). Sociodemographic and socioeconomic determinants of health services utilization in Greece: the Hellas Health I study. 24(1), 8-18.View
Robert J. Romanelli, P., Sonali N. Shah, R. M. B. A. M. P. H., Laurence Ikeda, M. D., Braden Lynch, P. M. S. C., Terri L. Craig, P. C., Joseph C. Cappelleri, P. M. P. H. M. S., Trevor Jukes, M. S., & Denis Ishisaka, P. M. S. (2017). Patient Characteristics and Healthcare Utilization of a Chronic Pain Population Within an Integrated Healthcare System. The American Journal of Managed Care, 23(2). https://www.ajmc.com/view/patient-characteristics-and-healthcare-utilization-of-a-chronic-pain-population-within-an-integrated-healthcare-system (February 2017)View
Fantahun, M., & Degu, G. J. E. J. o. H. D. (2003). Health service utilization in Amhara region of Ethiopia. 17(2), 140- 147.
Mackian, S. (2002). A Review of Health Seeking Behaviour: Problems and Prospects. Health Systems Development. University of Manchester, Manchester, UK.View
Varsi, C., Ledel Solem, I. K., Eide, H., Børøsund, E., Kristjansdottir, O. B., Heldal, K., Waxenberg, L. B., Weiss, K. E., Schreurs, K. M. G., Morrison, E. J., Stubhaug, A., & Solberg Nes, L. (2021). Health care providers’ experiences of pain management and attitudes towards digitally supported self-management interventions for chronic pain: a qualitative study. BMC Health Services Research, 21(1), 275. https://doi. org/10.1186/s12913-021-06278-7View
Raftery, J. (1998). Economic evaluation: an introduction. BMJ (Clinical research ed.), 316(7136), 1013-1014. https://doi. org/10.1136/bmj.316.7136.1013View
Goodacre, S., & McCabe, C. (2002). An introduction to economic evaluation. Emergency Medicine Journal, 19(3), 198. https://doi.org/10.1136/emj.19.3.198View
Palmer, S., Byford, S., & Raftery, J. (1999). Economics notes: types of economic evaluation. BMJ (Clinical research ed.), 318(7194), 1349-1349. https://doi.org/10.1136/ bmj.318.7194.1349View
Phillips, C. (2008). Health Economics: An Introduction for Health Professionals. Health Economics: An Introduction for Health Professionals, 1-151. https://doi.org/10.1002/9780470755228View
Rai, M., & Goyal, R. (2018). Pharmacoeconomics in Healthcare. In (pp. 465-472). https://doi.org/10.1016/B978-0-12-802103- 3.00034-1View
Dernovsek, M. Z., Prevolnik-Rupel, V., & Tavcar, R. (2007). Cost-utility analysis. In Quality of life impairment in schizophrenia, mood and anxiety disorders (pp. 373-384). Springer.View
Vijan, S., Hofer, T. P., & Hayward, R. A. (2000). Cost-Utility Analysis of Screening Intervals for Diabetic Retinopathy in Patients With Type 2 Diabetes Mellitus. JAMA, 283(7), 889- 896. https://doi.org/10.1001/jama.283.7.889 %J JAMAView
Busbee, B. G., Brown, M. M., Brown, G. C., & Sharma, S. J. O. (2003). Cost-utility analysis of cataract surgery in the second eye. 110(12), 2310-2317.View
Surendra, N. K., Abdul Manaf, M. R., Hooi, L. S., Bavanandan, S., Mohamad Nor, F. S., Firdaus Khan, S. S., Meng, O. L., & Abdul Gafor, A. H. J. P. o. (2019). Cost utility analysis of end stage renal disease treatment in Ministry of Health dialysis centres, Malaysia: hemodialysis versus continuous ambulatory peritoneal dialysis. 14(10), e0218422.View
Parkerson GR Jr, & Gutman RA. (2000). Health-related quality of life predictors of survival and hospital utilization. Health care financing review, 21(3), 171-184. https://pubmed.ncbi.nlm.nih. gov/11481754View
Rifel, J., Svab, I., Selič - Zupančič, P., Pavlic, D., Nazareth, I., & Car, J. (2013). Association of Common Mental Disorders and Quality of Life with the Frequency of Attendance in Slovenian Family Medicine Practices: Longitudinal Study. PloS one, 8, e54241. https://doi.org/10.1371/journal.pone.0054241View
Kurpas, D., Mroczek, B., Sitko, Z., Helicka, D., & Kuchar, E. (2015). Quality of life and health care utilization in patients with chronic respiratory diseases. Adv Exp Med Biol, 834, 63-74. https://doi.org/10.1007/5584_2014_46View
Agborsangaya, C. B., Lau, D., Lahtinen, M., Cooke, T., & Johnson, J. A. (2013). Health-related quality of life and healthcare utilization in multimorbidity: results of a cross-sectional survey. Qual Life Res, 22(4), 791-799. https://doi. org/10.1007/s11136-012-0214-7View