
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 6 (2022), Article ID: JPHIP-203
https://doi.org/10.33790/jphip1100203Research Article
Assessing Occupational Stress and Preparedness Among Campus Safety Officers and Dental School Employees at an Academic Medical Center During COVID-19
Decature Banker1, Lorena Baccaglini2, Miriam McCann3, & Chandran Achutan1*
1Department of Environmental, Agricultural & Occupational Health, College of Public Health, University of Nebraska Medical Center, 984388 Nebraska Medical Center, Omaha, NE 68198-4388, United States.
2Department of Epidemiology, College of Public Health, University of Nebraska Medical Center, 984388 Nebraska Medical Center, Omaha, NE 68198-4388, United States.
3Department of Environmental Health & Safety, University of Nebraska Medical Center, 985480 Nebraska Medical Center, Omaha, NE 68198- 5480 United States.
Corresponding Author Details: Chandran Achutan, PhD, CIH, Associate Professor, Department of Environmental, Agricultural & Occupational Health, College of Public Health, University of Nebraska Medical Center, 984388 Nebraska Medical Center, Omaha, NE 68198-4388, United States.
Received date: 01st December, 2022
Accepted date: 30th April, 2022
Published date: 02nd April, 2022
Citation: Banker, D., Baccaglini, L., McCann, M., & Achutan, C. (2022). Assessing Occupational Stress and Preparedness among Campus Safety Officers and Dental School Employees at an Academic Medical Center during COVID-19. J Pub Health Issue Pract 6(1): 203.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Job stress can lead to adverse physical and emotional health effects in employees. It is worse during an emergency or pandemic. This cross-sectional study looked at Campus Safety Officers and Dental School employees, who’s work puts them at risk for COVID-19 exposure. We hypothesized that Campus Safety Officers and Dental School employees who felt adequately trained to conduct COVID-19 related work would not feel more stressed during the COVID-19 pandemic than they did before the pandemic. We provided a self-administered questionnaire to 148 employees between April and July 2020. Of the 148 questionnaires, 147 were included in our study. There were 42 Campus Safety Officers (28.6%) and 105 Dental School employees (71.4%). Most study participants were younger than 40 years of age (51.1%), and male (52.4%). Forty-four had over 20 years of work experience. We found a significant association between employee perception of stress, perception of adequate training to conduct pandemic work (p≤0.0001), and gender (p=0.022). Although most study participants felt adequately trained to conduct work relating to COVID-19 (60.9%), they still felt more stressed during the pandemic than before (47.6%). Mental health support is critical to reduce the impact of stress.
Keywords: COVID-19, Occupational Stress, Preparedness, Training, Healthcare Workers, Academic Medical Center
Introduction
Job stress can lead to adverse physical and emotional health effects in employees [1]. The National Institute for Occupational Safety and Health (NIOSH) lists cognitive and behavioral adverse effects as possible symptoms of stress [2]. The Encyclopedia of Occupational Health and Safety indicates that job stress can increase the risk of cardiovascular disease, musculoskeletal disorders, and psychological disorders [3].
Stress-related adverse health effects can occur when the worker's resources, training, or other requirements do not meet the demand of the job [1]. These health effects can worsen when workers have minimal control over job processes or feel support from management, and coworkers are lacking [4]. The World Health Organization (WHO) places workplace stress-related hazards into two categories; work content or work context [4]. Work content includes job content, workload, pace, and hours. Occupations, such as first responders and healthcare workers, are inherently stressful due to the work content. Work context includes the employee’s role within the organization, interpersonal relationships, and the organizational culture [4]. Perceived lack of support from management, poor relationships with colleagues, or lack of resources and training, are examples where work context makes a job more stressful.
A study conducted by Northwestern National Life Insurance Company to assess employee burnout indicated that 25% of employees see their jobs as the leading stressor in their life [5]. Stress in the workplace can lead to a financial burden for employees. Health care expenditures are 46% higher for employees who report high levels of stress [6]. Stress in the workplace can also lead to time away from work. The Bureau of Labor Statistics indicated 3,418 illness cases due to occupational stress in 1997 and the median day away from work was 23 days [7].
Job stress is worse during an emergency or during a pandemic and can lead to traumatic incident stress [2]. A study assessing mental health outcomes in police personnel after Hurricane Katrina concluded that incidences of post-traumatic stress disorder (PTSD) and depression resulted from the work [8]. Research also indicates that an unprecedented infectious disease outbreak, like the severe acute respiratory syndrome (SARS) outbreak, induces stress in healthcare workers [9].
Several differences exist between the coronavirus disease 2019 (COVID-19) pandemic and past pandemics. The number of COVID-19 cases is significantly higher than the SARS and the Middle East respiratory syndrome (MERS) cases [10]. Clinical features of COVID-19 include severe pneumonia [10], arterial hypoxemia [11], acute cardiac injury [12], hepatitis [13], loss of taste or smell [14], coagulopathy [15], neurological manifestations [16], and kidney disease [17]. Clinical features for both SARS and MERS were limited to severe pneumonia [10].
It has been difficult to quantify the total number of COVID cases, which illustrates the complexity of the pandemic [10]. Many COVID-19 infected patients are asymptomatic or develop only mild symptoms, but virus transmission is still possible [18]. The lack of typical clinical symptoms and signs in asymptomatic infections significantly underestimates the total number of infections [18]. Shortages of testing kits, reagents, and supplies mean fewer people tested, which could also minimize the total number of infections [19]. The unavailability of testing leads to underestimated COVID-19 attributed deaths [10]. False-negative and false-positive results can also impact the total number of infected cases [20].
The complexity of this pandemic is taking a toll on the healthcare systems and their employees [21]. Hospitals in the United States are functioning at maximum capacity [22]. Healthcare workers are facing unparalleled workloads with shortages of Personal Protective Equipment (PPE) and medical supplies [21,22]. The financial impact on healthcare providers is substantial [23]. Floods of patients and front-line workers falling ill has increased salary and wage costs due to increased overtime costs [24]. The loss for hospitals and health systems is estimated to be $323.1 billion in 2020 [25]. Hospital financial reserves are drained, resulting in layoffs and salary reductions [22]. A Department of Labor (DOL) news release indicated that the health care industry is a large contributor to unemployment insurance claims [26]. Employment in health care and social assistance is down by 1 million since February 2020 [27]. Healthcare workers are paying the ultimate price. An estimated 1,718 healthcare workers have died of COVID-19 and related complications [28].
We know that conducting pandemic related work can lead to occupational stress [29]. Studies indicate that training is a critical component in preparing healthcare workers to perform work during infectious disease outbreaks [30-33]. The academic medical center involved in this study treated some of America’s first COVID-19 patients [34]. Due to the infectious nature of COVID-19, we had to get employees fit tested for respirators rapidly
This study looked at two different groups of academic medical center employees. Campus Safety Officers, who are first responders for the health center, conduct work that puts them at risk for COVID-19 exposure. This work includes interacting, transporting, and performing aerosol-generating procedures such as cardiopulmonary resuscitation on patients [35,36]. Dental School employees also conduct work that puts them at risk for COVID-19 exposure. This work can include performing aerosol-generating procedures, collecting or handling specimens, providing urgent or emergency dental care, and entering patient rooms [37,38]. We hypothesized that Campus Safety Officers and Dental School employees who felt adequately trained to conduct COVID-19 related work would not feel more stressed during the COVID-19 pandemic than they did before the pandemic.
Subject and Methods
Study Design
For this cross-sectional study, occupational stress and preparedness to perform COVID-19 related work were assessed through questionnaires. The questionnaires were administered to academic medical center workers prior to undergoing initial fit testing or refitting their N95 respirator. Fit testing sessions took place in April 2020 for Campus Safety Officers and between April and July 2020 for Dental School employees. The dates of fit testing for Dental School employees were extended due to a lack of respirator fit testing supplies and group representatives determining which employees needed fit testing.
The institution’s human subject review board exempted this study because it fell under quality improvement and not research.
Participants
The population assessed was Campus Safety Officers and Dental School employees, including faculty, program directors, dental assistants, sterilization specialists, group practice coordinators, and implant specialists. These two groups, who were required to participate in the respirator fit testing sessions as part of the COVID-19 pandemic response, were chosen as convenient and representative samples for our study. The selection of participants and eligibility criteria was determined by department chairs, program directors, and administrative staff, based on CDC guidelines and recommendations made by the organization's infectious disease experts. Eligibility criteria for Campus Safety Officers were all Officers without an N95 respirator fit test within the last three years. Campus Safety Officers who were known to be leaving the organization or unable to perform a respirator fit test due to medical conditions were excluded from the fit testing sessions. Eligibility criteria for Dental School employees were employees with the potential to be working with aerosol-generating procedures or working with patients not tested for COVID-19. Employees who were known to be leaving the organization or unable to perform a respirator fit test due to medical conditions were excluded from the fit testing sessions.
Questionnaire
We provided a self-administered questionnaire to 148 employees (43 Campus Safety Officers, 105 Dental School employees). The questionnaires were given to employees when they arrived to check-in for their N95 respirator fit test. Once employees were checked-in, they were given as much time as they needed to sit down and complete the questionnaire. Upon completion of the questionnaire, employees were sent to the fit testing stations to receive their fit test.
The questionnaire was designed to assess general and demographic information (3 questions), respirator use experience (1 question), perception of workplace preparedness (2 questions), perception of pandemic related stress (1 question), perception of employer pressure to conduct pandemic related work (1 question), perception of personal pressure to conduct pandemic related work (1 question) and perception of pandemic related changes to job duties (1 question).
The question assessing employees’ perception of pandemic-related stress is the outcome variable. The question assessing if employees’ felt adequately trained to conduct COVID-19 related work is the exposure and predictor variable. All other questions were potentially confounding variables.
All data collected was categorical qualitative data. Five of the questions were measured on a 5-point Likert scale for responses (strongly agree, agree, undecided/neutral, disagree, and strongly disagree), three questions were measured on a nominal scale for responses (female/male/other and yes/no/I don’t know), and two questions were measured on an ordinal scale for responses (age and work experience range).
Statistical Analysis
SPSS version 27 (IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp) and SAS version 9.4 (SAS Institute Inc. 2013. SAS® 9.4 Statements: Reference. Cary, NC: SAS Institute Inc.) were utilized for all statistical analysis with counts and percentages. SPSS was utilized to obtain descriptive statistics for demographic information. Due to data being ordinal, Cochran-Mantel-Haenszel (CMH) analysis was utilized to test for associations between employee perception of stress during the pandemic, perception of adequate training to conduct pandemic related work, and potential confounders. A p-value of ≤ 0.05 was utilized to indicate significance.
Results
Demographic characteristics
We administered 148 questionnaires of which 43 were given to Campus Safety Officers and 105 were given to Dental School employees. At the time of our evaluation, we estimated that there were a total of 57 Campus Safety Officers and 266 Dental School employees at this academic medical center.
Of the 148 questionnaires that were administered, 147 were included in our study, indicating a response rate of 99.3%. We received 43 questionnaires from Campus Safety Officers, however, one questionnaire was excluded from our study due to illegible responses. Campus Safety Officers accounted for 42 (28.6%) of the total responses included in our study and had a response rate of 97.7% (42 of 43). Dental School employees accounted for 105(71.4%) of the total responses included in our study and had a response rate of 100% (105 of 105). Most study participants were younger than 40 years of age (75 [51.1%]), and 32 (21.8%)study participants were 60 and over. Males accounted for 77 (52.4%) responses. A total of 44 (29.9%) study participants had over 20 years of work experience (Table 1).
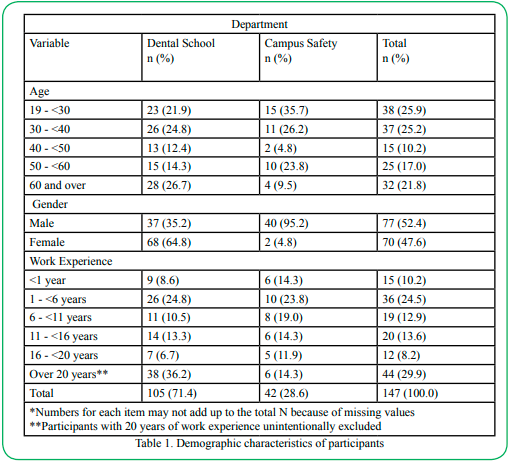
Table 1. Demographic characteristics of participants
Perception of increased stress during COVID-19
The question “I feel more stressed now (during the pandemic) than before the pandemic” was used to measure the outcome variable. Overall, 12.2% of employees strongly agreed, 35.4% agreed, 34.0% were undecided, 12.9% disagreed, and 5.4% strongly disagreed that they felt more stressed during the COVID-19 pandemic than before the pandemic. We found a significant association between employee perception of stress during the pandemic, perception of adequate training to conduct pandemic work (p ≤0.0001), and gender (p=0.022). We also found a significant association between employee perception of stress during the pandemic and the following confounders; department (p≤0.0001), adequate employer-provided PPE (p=0.008), and pandemic related job duty changes (p=0.003) (Table 2).
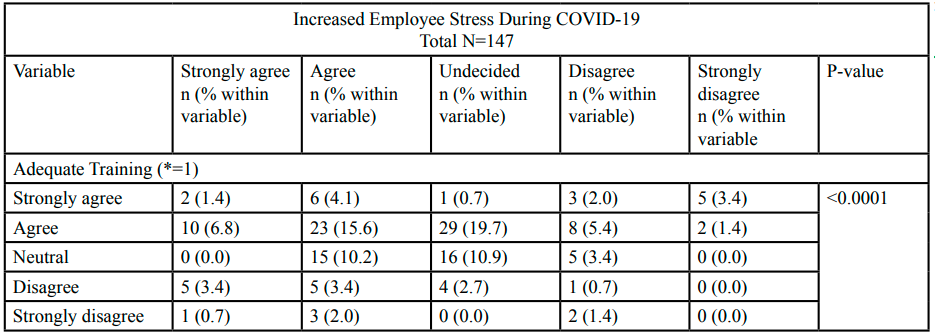
Table 2.Perception of increased stress during COVID-19
Perception of adequate training to conduct COVID-19 related work
The question “Do you feel that you are adequately trained to conduct work relating to COVID-19?” was used to measure the exposure/predictor variable. Overall, 11.6% of employees strongly agreed, 49.3% agreed, 24.6% were neutral, 10.2% disagreed, and 4.1% strongly disagreed that they were adequately trained to conduct COVID-19 related work. We found a significant association between employee perception of adequate training to conduct pandemic work and the following confounders; department (p=0.0059), adequate employer-provided PPE (p=<0.0001), and pandemic related job duty changes (p=0.0072). We also found a significant association between employee perception of adequate training to conduct pandemic work and age (p=0.0121), work experience (p=0.0002), employer pressure to conduct COVID-19 related work (0.0070), and personal pressure to conduct COVID-19 related work (p=0.0008) (Table 3).
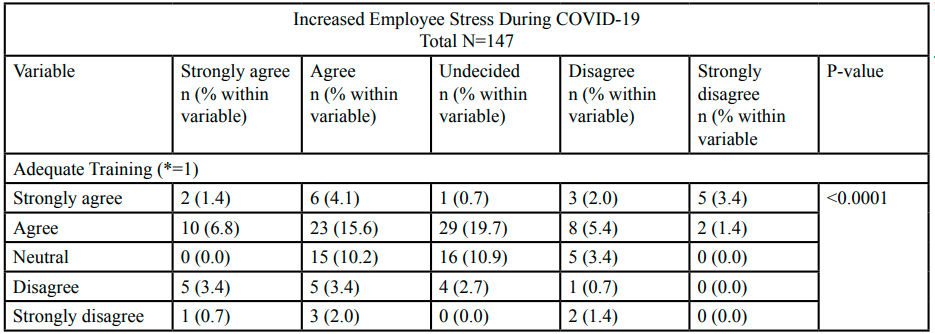
Table 3. Perception of adequate training to conduct COVID-19 related work
Discussion
This cross-sectional study of academic medical center personnel indicated elevated levels of stress during the COVID-19 pandemic). Yet, most of our study participants felt that they were adequately trained to conduct work relating to COVID-19 (60.9% of our study participants either strongly agreed or agreed that they felt adequately trained to conduct work relating to COVID-19). Although there was statistical association between the two variables of stress and training, these results are contradictory of our hypothesis that employees who felt adequately trained to conduct COVID-19 related work would not feel more stressed during the COVID-19 pandemic than they did before the pandemic. Further, our study indicated that gender was associated with stress.
Other research has shown that conducting pandemic related work can lead to occupational stress [29,39-44]. A study assessing the mental health impact on healthcare workers in Wuhan during COVID-19 reported that 34.4% had mild mental health disturbances, 22.4% had moderate disturbances and 6.2% had severe disturbances [39]. A different study indicated that healthcare workers in Wuhan reported depression (50.4%), anxiety (44.6%), insomnia (34.0%) and distress (71.5%) [40]. A study administered a mental health survey to medical staff in a tertiary infectious disease hospital which resulted in incidences of anxiety (23.04%), and stress disorder (27.39%) [41]. Medical workers in Pakistan have been reporting psychological pressure from COVID-19, resulting in mental health issues [42]. A study assessing healthcare workers in Spain during COVID-19 indicated that 56.6% of healthcare workers had symptoms of PTSD [43]. During the SARS outbreak, 89% of healthcare workers conducting high-risk work reported negative psychological effects [44].
Several factors can induce stress and negative psychological effects among healthcare workers during COVID-19. A study assessing the psychological impact of SARS indicated that stress levels were high and associated sources were feelings of vulnerability or loss of control and concerns of personal health, health of family and others, spread of the virus, changes in work, and being isolated [45]. The COVID-19 pandemic has presented a high number of cases [10], several associated clinical features [10-17], difficulties quantifying the total number of cases [10,18-20], shortages of PPE and medical supplies [21-22], financial loss [25], layoffs and salary reductions [22], illness [24] and death among healthcare workers [28], resulting in unparalleled stress.
Training is a critical component in preparing healthcare workers to perform work during infectious disease outbreaks [30-33]. Enhanced support and training may reduce posttraumatic stress and burnout in healthcare workers during an infectious disease outbreak [46]. A study assessing healthcare trainees in the United Kingdom indicated a significant proportion of trainees (24%) felt that training on personal protection while treating COVID-19 patients was inadequate, resulting in the majority of trainees reporting physical (63%) and mental (32%) health concerns [47]. A rapid systematic review and meta-analysis on the impact of viral epidemic outbreaks on mental health of healthcare workers indicated that a lack of specialized training is associated with anxiety, PTSD and burnout [48].
While our study participants felt that they were adequately trained to conduct COVID-19 related work, they still felt more stressed during the pandemic than before. It is possible that training may have resulted in greater awareness of pandemic associated risks, which could increase stress. Research indicates a higher perception of threat and risk is associated with depression, anxiety and PTSD [48]. During an infectious disease outbreak, healthcare workers may have greater concerns compared to the public as they probably have a better understanding of associated risks [49]. A study assessing frontline healthcare workers in Hong Kong during the SARS pandemic concluded that psychological morbidity among healthcare workers was best understood by their perceptions of personal vulnerability, stress and support [50]. A different study quantified stress and the psychological impact of SARS on healthcare workers, indicating elevated stress levels [44]. When compared to control subjects, 94% of healthcare workers reported more positive psychological effects (awareness of hygiene, focus on current affairs, and awareness of danger) [44]. Yet, 89% of healthcare workers also reported more negative psychological effects (tiredness, health concerns, and fear of social contact) than control subjects [44].
This study assessed training in relation to employees conducting COVID-19 work. Research shows conducting COVID-19 work will lead to stress and adverse mental health concerns [29,39-43,47]. We recommend that future studies assess training in relation to reducing the impact of stress and adverse mental health outcomes during COVID-19. A study assessing mental health care for medical staff in China during COVID-19 indicates a lack of mental health training can lead to adverse effects in health outcomes of healthcare workers [51]. Providing healthcare managers with trauma awareness training could be a proactive approach to reduce the impact of stress on workers during the pandemic [52]. A study assessed a digital learning package aimed to mitigate the psychological impact of COVID-19 on healthcare workers. Healthcare workers felt that health and wellbeing training should be mandatory for all healthcare workers [53]. The study noted that the learning package was highly accessed, indicating the desire healthcare workers have for support of their psychological wellbeing [53]. The study participants reported that they took some action to improve their psychological wellbeing after accessing the learning package [53]. Health system leaders, first responders and health care workers should receive training regarding psychosocial issues [54]. The efficacy of mental health training on reducing the impact of stress and adverse mental health effects in healthcare workers during COVID-19 warrants further investigation.
Another finding in our study was the association between gender and stress. A greater percentage of female participants felt more stressed during the pandemic. Overall, 58.6% (41 of 70) of female participants either strongly agreed or agreed that they felt more stressed during the COVID-19 pandemic than before the pandemic, compared to 37.6% (29 of 77) of male participants. Lai et al. (2020) found that female healthcare workers reported more severe symptoms of distress, anxiety, and depression [40]. Kang et al. (2020) found high percentages of mental health disturbances in healthcare staff during COVID-19 and indicated that the burden fell heavily on young women [39]. Huang et al. (2020) reported higher incidence and mental health survey scores of anxiety and stress disorder among female medical staff [41]. Our results can potentially be attributed to the work conducted by female participants. Of the 70 female participants included in the study, 68 (97%) were Dental School employees. Dental School employees typically perform more direct patient care compared to Campus Safety Officers. It is possible that providing dental care for patients caused our female participants to feel more stressed during the pandemic than male participants. Special attention is justified regarding the well-being and mental health of female healthcare workers during COVID-19.
Strengths
This study had multiple strengths. The self-administered questionnaire eliminated the potential for interviewer bias. We estimated that there were a total of 57 Campus Safety Officers and 266 Dental School employees at this academic medical center. Of the 323 employees, 148 (45.8%) conduct work that puts them at risk for COVID-19 exposure and were eligible to participate in our study, making our sample representative. Of the 148 questionnaires that were administered, 147 were included in our study, indicating a response rate of 99.3%. Our high response rate eliminated the potential for non-response bias.
Limitations
There are several limitations to the study. The cross-sectional design only allowed us to evaluate occupational stress at the time of the survey. Due to the rapid need to get employees fit tested for respirators and how quickly the study had to be formed, we were not able to pilot test the questionnaire. Occupational stress was not clearly defined on the questionnaire. Although the questionnaire was titled “COVID-19 Workplace Stress Questionnaire” and the introductory sentence indicated that the purpose of the questionnaire was to “assess stress in the workplace due to the COVID-19 pandemic”, the question assessing stress did not indicate stress relating to work specifically, which could have impacted the way participants answered the question. For the work experience variable, the options on the questionnaire included “16 - <20 years” and “over 20 years”, which may have excluded or impacted the way that participants who had exactly 20 years of experience answered the question. Although the questionnaires were self-administered, study participants may have been influenced by the presence of personnel conducting fit testing, which could have impacted the way participants completed the questionnaire and led to observation bias. Study participants may have been nervous or fearful about answering questions truthfully, so the questionnaires should have been sent to participants prior to fit testing to be completed in a private setting.
Conclusion
In this study, elevated levels of stress were observed among Campus Safety Officers and Dental School employees during COVID-19. Although most study participants felt adequately trained to conduct work relating to COVID-19, they still felt more stressed during the COVID-19 pandemic than before the pandemic. Mental health training should be provided to healthcare workers during the COVID-19 pandemic to reduce the impact of stress and adverse mental health effects. Special attention should be paid to ensure the well-being of female healthcare workers during COVID-19.
Competing Interests:
The author(s) declare that they have no competing interests.
References
Sauter, S., Murphy, L., Colligan, M., Swanson, N., Hurrell Jr., J., Scharf Jr., F., Sinclair, R., Goldenhar, L., Alterman, T., Johnston, J., Hamilton, A., & Tisdale, J. (1999). Stress at work. DHHS (NIOSH) Publication, Number 99-101. doi:10.26616/ nioshpub99101.View
National Institute for Occupational Safety and Health (NIOSH) (2013). Traumatic Incident Stress. Accessed October 16, 2020. https://www.cdc.gov/niosh/topics/traumaticincident/default. htmlView
Sauter, S., Hurrell, J., Murphy, L., Levi, L (1997) Psychosocial and organizational factors. In: Stellman J, ed. Encyclopaedia of Occupational Health and Safety. Vol. 1. Geneva, Switzerland: International Labour Office, 4.1-34.77.View
World Health Organization (WHO). (2010). Stress at the workplace. Date accessed: October 16, 2020.https://www.who. int/occupational_health/topics/stressatwp/en/.View
Northwestern National Life Insurance Company (1991). Employee burnout: America’s newest epidemic. Minneapolis, MN: Northwestern National Life Insurance Company.
Anderson, D.R., Whitmer, R.W., Goetzel, R.Z., Ozminkowski, R.J., Dunn, R.L., Wasserman, J., & Serxner, S. (2000). The relationship between modifiable health risks and group-level health care expenditures. Health Enhancement Research Organization (HERO) Research Committee. Am J Health Promot. 15(1), 45-52. doi: 10.4278/0890-1171-15.1.45. Erratum in: Am J Health Promot 2001 Jan-Feb;15(3), 191. PMID: 11184118.View
U.S. Department of Labor Bureau of Labor Statistics. (1999). Issues in Labor Statistics Summary 99-10. Accessed October 16, 2020.https://www.bls.gov/opub/btn/archive/occupational-stress.pdfView
West, C., Bernard, B., Mueller, C., Kitt, M., Driscoll, R., Tak, S. (2008). Mental health outcomes in police personnel after Hurricane Katrina. J Occup Environ Med. 50(6), 689-95. doi: 10.1097/JOM.0b013e3181638685. PMID: 18545096. View
Maunder, R., Hunter, J., Vincent, L., Bennett, J., Peladeau, N., Leszcz, M., Sadavoy, J., Verhaeghe, L.M., Steinberg, R., & Mazzulli, T. (2003). The immediate psychological and occupational impact of the 2003 SARS outbreak in a teaching hospital. CMAJ. 168(10), 1245-51. View
Pitlik, S.D. (2020). COVID-19 Compared to Other Pandemic Diseases. Rambam Maimonides Med J. 11(3), 1-17. doi: 10.5041/ RMMJ.10418. PMID: 32792043; PMCID: PMC7426550.View
Tobin, M.J. (2020). Basing Respiratory Management of COVID-19 on Physiological Principles. Am J Respir Crit Care Med. 201(11), 1319-1320. doi: 10.1164/rccm.202004-1076ED. PMID: 32281885; PMCID: PMC7258630.View
Bansal, M. (2020). Cardiovascular disease and COVID-19. Diabetes MetabSyndr. 14(3), 247-250. doi: 10.1016/j. dsx.2020.03.013.View
Sun, J., Aghemo, A., Forner, A., & Valenti, L. (2020). COVID-19 and liver disease. Liver Int. 40(6), 1278-1281. doi: 10.1111/ liv.14470. PMID: 32251539.View
Mullol, J., Alobid, I., Marino-Sanchez, F., Izquierdo-Dominguez, A., Marin, C., Klimek, L., Wang, D.Y., & Liu, Z. (2020). The loss of smell and taste in the COVID-19 outbreak: a tale of many countries. Curr Allergy Asthma Rep. 20, 1-5. doi: 10.1111/ijd.14937.View
Connors, J.M., & Levy, J.H. (2020). COVID-19 and its implications for thrombosis and anticoagulation. Blood. 135(23), 2033-2040. doi: 10.1182/blood.2020006000. PMID: 32339221; PMCID: PMC7273827.View
Ahmad, I., & Rathore, F.A. (2020). Neurological manifestations and complications of COVID-19: A literature review. J Clin Neurosci. 77, 8-12. doi: 10.1016/j.jocn.2020.05.017. View
Cheng, Y., Luo, R., Wang, K., Zhang, M., Wang, Z., Dong, L., Li, J., Yao, Y., Ge, S., & Xu, G. (2020). Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 97(5), 829-838. doi: 10.1016/j.kint.2020.03.005. View
Gao, Z., Xu, Y., Sun, C., Wang, X., Guo, Y., Qiu, S., & Ma, K. (2021). A Systematic Review of Asymptomatic Infections with COVID-19. J Microbiol Immunol Infect. 54(1), 12-16.doi: 10.1016/j.jmii.2020.05.001.View
Yelin, I., Aharony, N., Tamar, E.S., Argoetti, A., Messer, E., Berenbaum, D., Shafran, E., Kuzli, A., Gandali, N., Shkedi, O., Hashimshony, T., Mandel-Gutfreund, Y., Halberthal, M., Geffen, Y., Szwarcwort-Cohen, M., & Kishony, R. (2020). Evaluation of COVID-19 RT-qPCR Test in Multi sample Pools. Clinical infectious diseases 71(16), 2073–2078. View
Long, C., Xu, H., Shen, Q., Zhang, X., Fan, B., Wang, C., Zeng, B., Li, Z., Li, X., & Li, H. (2020). Diagnosis of the Coronavirus disease (COVID-19): rRT-PCR or CT? Eur J Radiol. 126, 108961. doi: 10.1016/j.ejrad.2020.108961.View
Iyengar, K., Mabrouk, A., Jain, V.K., Venkatesan, A., & Vaishya, R. (2020). Learning opportunities from COVID-19 and future effects on health care system. Diabetes MetabSyndr. 14(5), 943- 946. doi: 10.1016/j.dsx.2020.06.036.View
Barnett, M.L., Mehrotra, A., & Landon, B.E. (2020). Covid-19 and the upcoming financial crisis in health care. AccessedOctober 17, 2020. https://catalyst.nejm.org/doi/ full/10.1056/CAT.20.0153View
Blumenthal, D., Fowler, E.J., Abrams, M., & Collins, S.R. (2020). Covid-19 - Implications for the Health Care System. N Engl J Med. 383(15), 1483-1488. doi: 10.1056/NEJMsb2021088. Erratum in: N Engl J Med. 2020 Jul 23; PMID: 32706956.View
American Hospital Association (AHA). (2020). Hospitals and Health Systems Face Unprecedented Financial Pressures Due to COVID-19: AHA. Accessed October 17, 2020.https://www.aha. org/guidesreports/2020-05-05-hospitals-and-health-systems-face-unprecedented-financial-pressures-duView
American Hospital Association (AHA) (2020). New AHA Report: losses deepen forhospitals and health systems. Accessed October 17, 2020.https://www.aha.org/press-releases/2020-06- 30-new-aha-report-losses-deepen-hospitals-health-systemsView
U.S. Department of Labor (DOL) (2020). Employment and Training Administration. Unemployment Insurance Weekly Claims Report. Accessed: October 17, 2020. https://oui.doleta. gov/press/2020/032620.pdf
Bureau of Labor Statistics (BLS) (2020). The Employment Situation - September 2020. Accessed: October 17, 2020.https:// www.bls.gov/news.release/pdf/empsit.pdfView
National Nurses United (2020). Sins of Omission How Government Failures to Track Covid-19 Data Have Led to More Than 1,700 Health Care Worker Deaths and Jeopardize Public Health. Accessed October 17, 2020. https://act. nationalnursesunited.org/page/-/files/graphics/0920_Covid19_ SinsOfOmission_Data_Report.pdfView
Centers for Disease Control and Prevention (CDC) (2020). COVID-19 Stress Among Your Workers? Healthy Work Design and Well-Being Solutions Are Critical. Accessed October 17, 2020.https://blogs.cdc.gov/niosh-science-blog/2020/06/12/ covid-19-stress/View
Mo, Y., Deng, L., Zhang, L., Lang, Q., Liao, C., Wang, N., Qin, M., & Huang, H. (2020). Work stress among Chinese nurses to support Wuhan in fighting against COVID-19 epidemic. J NursManag. 28(5), 1002-1009. doi: 10.1111/jonm.13014.View
Wong, W.C., Wong, S.Y., Lee, A., & Goggins, W.B. (2007). How to provide an effective primary health care in fighting against severe acute respiratory syndrome: the experiences of two cities. Am J Infect Control. 35(1), 50-55. doi: 10.1016/j. ajic.2006.06.009. PMID: 17276791; PMCID: PMC7132727.View
Maunder, R.G., Leszcz, M., Savage, D., Adam, M.A., Peladeau, N., Romano, D., Rose, M., & Schulman, B. (2008). Applying the lessons of SARS to pandemic influenza: an evidence-based approach to mitigating the stress experienced by healthcare workers. Can J Public Health. 99(6), 486-488. doi: 10.1007/ BF03403782. PMID: 19149392; PMCID: PMC5148615.View
Maunder, R.G., Lancee, W.J., Mae, R., Vincent, L., Peladeau, N., Beduz, M.A., Hunter, J.J., & Leszcz, M. (2010). Computer-assisted resilience training to prepare healthcare workers for pandemic influenza: a randomized trial of the optimal dose of training. BMC Health Serv Res. 10, 72. doi: 10.1186/1472- 6963-10-72. PMID: 20307302; PMCID: PMC2851711.View
Smith, M. (2020). A Nebraska hospital aimed to contain the virusbut it had already spread. Accessed October 19, 2020.https://www.nytimes.com/2020/03/18/us/coronavirus-nebraska-biocontainment.htmView
Centers for Disease Control and Prevention (CDC) (2020). Interim Recommendations for Emergency Medical Services (EMS) Systems and 911 Public Safety Answering Points/ Emergency Communication Centers (PSAP/ECCs) in the United States During the Coronavirus Disease (COVID-19) Pandemic. Date accessed: October 17, 2020. https://www.cdc. gov/coronavirus/2019-ncov/hcp/guidance-for-ems.html
Occupational Safety and Health Administration. (2020). United States Department of Labor. Accessed October 17, 2020.https:// www.osha.gov/SLTC/covid-19/emergency-response.htmlView
Centers for Disease Control and Prevention (CDC) (2020). Guidance for Dental Settings. Accessed October 17, 2020. https://www.cdc.gov/coronavirus/2019-ncov/hcp/dental-settings.htm
Occupational Safety and Health Administration (2020). United States Department of Labor. Accessed October 17, 2020.https:// www.osha.gov/SLTC/covid-19/dentistry.htmlView
Kang, L., Ma, S., Chen, M., Yang, J., Wang, Y., Li, R., Yao, L., Bai, H., Cai, Z., Xiang Yang, B., Hu, S., Zhang, K., Wang, G., Ma, C., & Liu, Z. (2020). Impact on mental health and perceptions of psychological care among medical and nursing staff in Wuhan during the 2019 novel coronavirus disease outbreak: A cross-sectional study. Brain Behav Immun. 87, 11- 17. doi: 10.1016/j.bbi.2020.03.028.View
Lai, J., Ma, S., Wang, Y., Cai, Z., Hu, J., Wei, N., Wu, J., Du, H., Chen, T., Li, R., Tan, H., Kang, L., Yao, L., Huang, M., Wang, H., Wang, G., Liu, Z., & Hu, S. (2020). Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw Open. 3(3), e203976. doi: 10.1001/jamanetworkopen.2020.3976. PMID: 32202646; PMCID: PMC7090843.View
Huang, J.Z., Han, M.F., Luo, T.D., Ren, A.K., & Zhou, X.P. (2020). [Mental health survey of medical staff in a tertiary infectious disease hospital for COVID-19]. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi. 38(3), 192-195. Chinese. doi: 10.3760/cma.j.cn121094-20200219-00063. PMID: 32131151.View
Rana, W., Mukhtar, S., & Mukhtar, S. (2020). Mental health of medical workers in Pakistan during the pandemic COVID-19 outbreak. Asian J Psychiatr. 51, 102080. doi: 10.1016/j. ajp.2020.102080. View
Luceño-Moreno, L., Talavera-Velasco, B., García-Albuerne, Y., & Martín-García, J. (2020). Symptoms of Posttraumatic Stress, Anxiety, Depression, Levels of Resilience and Burnout in Spanish Health Personnel during the COVID-19 Pandemic. Int J Environ Res Public Health. 17(15), 5514. doi: 10.3390/ ijerph17155514. View
Chua, S.E., Cheung, V., Cheung, C., McAlonan, G.M., Wong, J.W., Cheung, E.P., Chan, M.T., Wong, M.M., Tang, S.W., Choy, K.M., Wong, M.K., Chu, C.M., & Tsang, K.W. (2004). Psychological effects of the SARS outbreak in Hong Kong on high-risk health care workers. Can J Psychiatry. 49(6), 391-393. doi: 10.1177/070674370404900609. PMID: 15283534.View
Wong, T.W., Yau, J.K., Chan, C.L., Kwong, R.S., Ho, S.M., Lau, C.C., Lau, F.L., & Lit, C.H. (2005). The psychological impact of severe acute respiratory syndrome outbreak on healthcare workers in emergency departments and how they cope. Eur J Emerg Med. 12(1), 13-18. doi: 10.1097/00063110-200502000- 00005. PMID: 15674079.View
Maunder, R.G., Lancee, W.J., Balderson, K.E., Bennett, J.P., Borgundvaag, B., Evans, S., Fernandes, C.M., Goldbloom, D.S., Gupta, M., Hunter, J.J., McGillis, Hall, L., Nagle, L.M., Pain, C., Peczeniuk, S.S., Raymond, G., Read, N., Rourke, S.B., Steinberg, R.J., Stewart, T.E., VanDeVelde-Coke, S., Veldhorst, G.G., & Wasylenki, D.A. (2006). Long-term psychological and occupational effects of providing hospital healthcare during SARS outbreak. Emerg Infect Dis.12(12), 1924-1932. doi: 10.3201/eid1212.060584. PMID: 17326946; PMCID: PMC3291360.View
Caruana, E.J., Patel, A., Kendall, S., & Rathinam, S. (2020). Impact of coronavirus 2019 (COVID-19) on training and well-being in subspecialty surgery: A national survey of cardiothoracic trainees in the United Kingdom. J Thorac Cardiovasc Surg. 160(4), 980-987. doi: 10.1016/j.jtcvs.2020.05.052. View
Serrano-Ripoll, M.J., Meneses-Echavez, J.F., Ricci-Cabello, I., Fraile-Navarro, D., Fiol-deRoque, M.A., Pastor-Moreno, G., Castro, A., Ruiz-Pérez, I., Zamanillo Campos, R., & Gonçalves-Bradley, D.C. (2020). Impact of viral epidemic outbreaks on mental health of healthcare workers: a rapid systematic review and meta-analysis. J Affect Disord. 277, 347-357. doi: 10.1016/j. jad.2020.08.034.View
Cheong, S.K., Wong, T.Y., Lee, H.Y., Fong ,Y.T., Tan, B.Y., Koh, G.C., Chan, K.M., Chia, S.E., & Koh, D. (2007). Concerns and preparedness for an avian influenza pandemic: a comparison between community hospital and tertiary hospital healthcare workers. Ind Health. 45(5), 653-61. doi: 10.2486/ indhealth.45.653. PMID: 18057808. View
Tam, C.W., Pang, E.P., Lam, L.C., & Chiu, H.F. (2004). Severe acute respiratory syndrome (SARS) in Hong Kong in 2003: stress and psychological impact among frontline healthcare workers. Psychol Med. 34(7), 1197-204. doi: 10.1017/ s0033291704002247. PMID: 15697046.View
Chen, Q., Liang, M., Li, Y., Guo, J., Fei, D., Wang, L., He, L., Sheng, C., Cai, Y., Li, X., Wang, J., & Zhang, Z. (2020). Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry. 7(4), e15-e16. doi: 10.1016/ S2215-0366(20)30078-X. Erratum in: Lancet Psychiatry. 2020 May;7(5):e27. PMID: 32085839; PMCID: PMC7129426.View
Tracy, D.K., Tarn, M., Eldridge, R., Cooke, J., Calder, J.D.F., & Greenberg, N. (2020). What should be done to support the mental health of healthcare staff treating COVID-19 patients? Br J Psychiatry. 217(4), 537-539. doi: 10.1192/bjp.2020.109. PMID: 32423523; PMCID: PMC7294074.View
Blake, H., Bermingham, F., Johnson, G., & Tabner, A. (2020). Mitigating the Psychological Impact of COVID-19 on Healthcare Workers: A Digital Learning Package. Int J Environ Res Public Health. 17(9), 2997. doi: 10.3390/ijerph17092997. PMID: 32357424; PMCID: PMC7246821.View
Pfefferbaum, B., & North, C.S. (2020). Mental Health and the Covid-19 Pandemic. N Engl J Med. 383(6), 510-512. doi: 10.1056/NEJMp2008017.View