
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 6 (2022), Article ID: JPHIP-205
https://doi.org/10.33790/jphip1100205Research Article
The Impact of the COVID-19 Pandemic on the Opioid Epidemic: A Statewide Analysis
Peter J. Fos1*, Peggy A. Honoré2, & Katrina P. Kellum3
1Professor of Health Sciences, Dillard University, Minority Health and Health Disparities Research Center, 2601 Gentilly Blvd. New Orleans, LA 70122, United States.
2Professor, LSU Health Sciences Center, School of Public Health, Department of Health Policy and Systems Management, School of Medicine, United States.
3College of Nursing, Dillard University, United States.
Corresponding Author Details: Peter J. Fos, Ph.D., D.D.S., M.P.H., Professor of Health Sciences, Dillard University, Minority Health and Health Disparities Research Center, 2601 Gentilly Blvd. New Orleans, LA 70122, United States.
Received date: 06th April, 2022
Accepted date: 07th May, 2022
Published date: 09th May, 2022
Citation: Fos, P. J., Honore, P. A., & Kellum, K. P. (2022). The Impact of the COVID-19 Pandemic on the Opioid Epidemic: A Statewide Analysis. J Pub Health Issue Pract 6(1): 205.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
The COVID-19 pandemic has had a significant effect on the opioid epidemic, which has been increasing over the past decade. The increase in opioid-involved deaths have coincided with fentanyl use, and a combination of drugs. Since the beginning of the COVID-19 pandemic opioid-involved deaths have increased greater than 30% in the U.S. The COVID-19 mandates, including stay-at-home orders, has had a detrimental impact on opioid and drug abuse, and association mortality.
This paper describes a statewide study of the impact of the COVID-19 pandemic and opioid and drug-involved deaths. Data was acquired from the Louisiana Department of Health for 2018, 2019, and 2020. The percent increase statewide in opioid-involved deaths was 115.9% from 2018 through 2020. When the data is stratified by race, non-Hispanic Blacks had a 163.6% increase in opioid-involved deaths, which was 15% higher than in non-Hispanic Whites. The increase in opioid-involved deaths was similar in males and females. Statewide drug-involved deaths increased 59%, with a 107.5% increase in non-Hispanic Blacks compared to 44.4% in non-Hispanic Whites. Again, the increase in males and females was the same. The trends seen statewide was seen among the study parishes, with a few exceptions.
The study has observed the magnitude of the impact of the COVID-19 pandemic on the opioid epidemic in Louisiana. These results were seen across the U.S. It is important to not lose sight or emphasis of the opioid epidemic, which has been increasing over the last decade.
Keywords: Opioid-involved Deaths, Drug-involved Deaths, COVID-19, Health Disparities, Fentanyl Abuse
Introduction
The COVID-19 pandemic has been occurring for the past two years, with no end in sight. COVID-19 cases and deaths have overshadowed the ongoing opioid epidemic in the U.S. Previous research has shown an increasing trend in opioid-involved deaths, as well as trends across racial groups [1]. Due to the emerging public health crisis of COVID-19 the opioid epidemic has lost some of its importance. However, it is now apparent that the COVID-19 pandemic and the opioid epidemic are related with respect to increased mortality.
The COVID-19 pandemic has been associated with excess deaths in the U.S. A study of mortality between March and July 2020 identified a 20% increase in excess deaths, and not all can be attributed to COVID-19. The sudden increase in deaths due to COVID-19 were accompanied by increases in deaths from other causes [2]. Between March 1, 2020 and January 2, 2021 there was a 22.9% more deaths than expected, with a differing increase across racial groups. The excess non-COVID-19 deaths are thought to be related to the pandemic, due to delayed health care services or mental health issues [3].
Illicitly manufactured fentanyl began to affect an increase in drug overdose deaths in 2019, after two or three years of decline. This increase in drug overdose deaths have also been impacted by the combination of drugs and opioids [4]. The lack of social interaction and limitation in health care that are associated with the COVID-19 pandemic has had a significant effect on opioid-involved deaths. Social distancing mandates, restriction of mobility, and prioritization of health care services has resulted in additional barriers to accessing opioid abuse care [5].
When the number of drug overdose deaths are reviewed, there was a 28.5% increase from 2019 to 2020, the largest increase in decades [6]. In addition to opioid-involved deaths, which represents majority of deaths, deaths from cocaine and other stimulants overdoses, as well as alcohol consumption also increased [7]. Many researchers predicted that the COVID-19 pandemic would have a significant impact on drug overdose deaths due to social restrictions and economic effects [8].
A study simulated indirect effects on health due to physical distancing and social limitations associated with the COVID-19 pandemic among the opioid use disorder subpopulation. Negative effects are associated with social isolation and economic instability [9]. The study found that the COVID-19 pandemic will have long-term negative effects on the opioid epidemic. These effects include delays in seeking of treatment, disruption of treatment, and mental health impact of social isolation. In fact, the COVID-19 pandemic has increased the risk of overdose deaths due to limiting the supply of opioids, which leads to use of any drugs that are available, despite their inherent lethal characteristics.
A study in Ontario, Canada evaluated the excess burden on opioid-involved deaths during the COVID-19 pandemic. The study focused on the first six months of the pandemic. Study findings indicated that there was a 135% increase in opioid-involved deaths, with majority of deaths among males, aged between 35 and 54 years. The study stated that causes of the increase were due to social isolation and changes to health care services delivery patterns, resulting in additional barriers to care [10]. An important aspect of opioid abuse treatment is frequent in-person treatment, which has been disrupted during the COVID-19 pandemic. Given this, the COVID-19 pandemic has resulted in higher risk for death in those with an opioid use disorder [11]. The increased demand for health care services to treat COVID-19 disease has reduced access to emergency department care for opioid abuse. An additional barrier is the negative impact on recovery from social isolation and distancing protocols [12].
In response to the emerging COVID-19 pandemic the federal government instituted a national stay-at-home order, which was followed by state-wide stay-at-home orders, in March 2020. At the same time health care service institutions began to prioritize care and delayed elective services. As a result, emergency department visits declined over 40% over the first few months of the pandemic [13]. Fear of COVID-19 and the stay-at-home orders caused delays in treatment and changes in care-seeking behavior [14]. Stay-at-home orders resulted in isolation, social distancing, closure of community and religious facilities, and disruption of social support systems. This has a negative impact mental health, especially depression disorders, which is a risk factor for drug abuse [15].
A study of the stay-at-home order in Cook County, Illinois illustrated the increased risk of opioid-involved death during the COVID-19 pandemic. Between December 2020 and April 2020 opioid-involved deaths increased 55.3% compared to what was expected. The increase in opioid-involved deaths was 92.0% when comparing mortality between May 2020 and July 2020 to what was expected. The study concluded that the stay-at-home order caused disruption treatment services, potential loss of social support, and substitution of potentially fatal drugs [16].
A retrospective study of the effect of stay-at-home orders conducted in Los Angeles found increases in opioid-involved deaths [17]. This result was seen across the U.S [18]. Non-Hispanic Whites experienced a greater increase in opioid-involved deaths compared to Hispanics. The study found that opioid-involved deaths are prevalent in populations with relatively low educational attainment, a well-established social determinant of health. Other findings included the suggestion that COVID-19 increased deaths from diseases of despair, and fatal opioid overdoses. Among Non-Hispanic Whites the risk of opioid overdose is greater because of a disruption of social support systems, limited health care services, and a lack of adequate medications.
This paper describes the study of the comparison of opioid deaths in Louisiana before and during the COVID-19 pandemic, 2018 through 2020. The comparison is intended to determine whether the COVID-19 pandemic had an impact on opioid-involved and drug-involved deaths in Louisiana as was seen in other parts of the U.S. Additionally, an objective of the study was to evaluate whether the COVID-19 pandemic has an effect on opioid-involved and drug-involved deaths across race and gender.
Materials and Methods
The study focused on retrospective evaluation of data from the Louisiana Opioid Data and Surveillance System [19]. The source of mortality data source was death certificates, using coding according from the Tenth Revision of the International Classification of Diseases (ICD-10) [20]. Drug-involved deaths involve drug poisoning (sometimes called drug overdose) as any underlying cause of death. Drugs are defined as any medicine or substance that have a physiological effect when ingested, injected, or absorbed into the body. Drug-involved deaths are ICD-10 codes X40-X44, X60-X64, X85, and Y10-Y-14. Deaths related to opioid usage and overdose are ICD-10 codes T40.0, T40.1, T40.2, T40.3, T40.4, and T40.6. The time- period selected was 2018 through 2020 to evaluate pre-COVID-19 and during the COVID-19 pandemic (2020 is the latest data available). Parishes in metropolitan areas were selected: Alexandria, Baton Rouge, Lafayette, Lake Charles, and New Orleans. These parishes have relatively large populations with diverse demographics.
Percent change in opioid-involved and drug-induced death rates from 2018 to 2019, 2019 to 2020, and 2018 to 2020 were calculated. Mortality rates were calculated using the U.S. Census July 2020 population estimates [21]. Percent change in mortality rates were evaluated across race and gender.
Results
Overall, the opioid-involved death rates in Louisiana increased each year from 2018 to 2020 (Table 1). The death rate increased 26.0% from 2018 to 2019. The rate increased 68.6% from 2019 to 2020. However, the increase from 2018 to 2020 was 112.3 percent. Similarly, the drug-involved death rates increased over the three-year period. There was a decrease of 30.4% in drug-involved death rates from 2018 to 2019, but the rate increased 137.5% from 2019 to 2020. For the three-year study period the drug-involved death rate increased 65.2%.
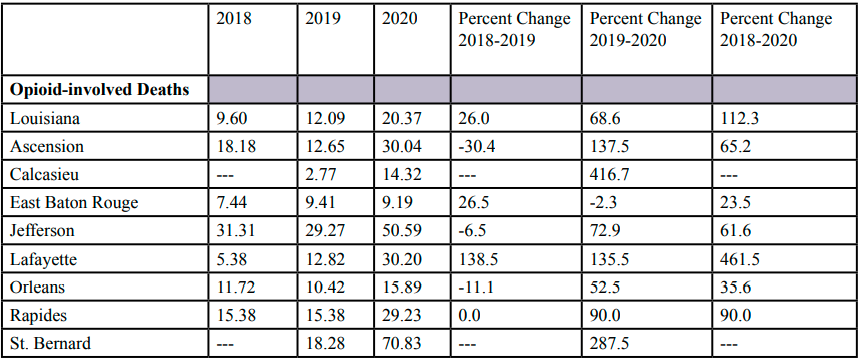
Table 1: Overall Opioid-involved and Drug-involved Death Rates*
The opioid-involved death rates across the study parishes experienced an increase during the three-year study period. The percent increase ranged from 23.5% to 461.5 percent. Due to data restrictions of the Louisiana Opioid Data Surveillance System with respect to low number of deaths, death rates were not available during 2018 for Calcasieu and St. Bernard Parishes. But both parishes experienced significant increases in opioid-involved death rate increased from 2019 to 2020 (416.7% and 287.5% increases, respectfully). Decreased death rates were seen from 2018 to 2019 in Ascension and Jefferson Parishes, but 2019 and 2020 showed increases in both parishes. The only other parish that experienced any reduction in death rates was East Baton Rouge Parish from 2018 to 2019.
The drug-involved death rates in the study parishes increased in all parishes except St. Bernard Parish, which remained the same during the three-year study period. The other parishes experienced an increase from 2.1% to 115.9% from 2018 to 2020. Ascension, Jefferson, and St. Bernard Parishes had a decrease in drug-involved death rates from 2018-2019, but, as was seen in opioid-involved death rates, they experienced an increase from 2019 to 2020 and over the three-year study period.
The death rates were stratified by race. Opioid-involved death rates among non-Hispanic Blacks increased in Louisiana 163.6% during the study period (Table 2). The increase from 2019 through 2020 was 130.7%, which followed an increase of 14.3% from 2018 through 2019. Opioid-involved death rates in the study parishes increased from 37.5% to 126.1 during the study period. As was mentioned above, due to data limitations death rates were not available for Ascension, Lafayette, and St. Bernard Parishes for each year during the study period. Data were available for 2020 for Ascension Parish which had a death rate of 29.64 deaths per 100,000 population. The greatest increases were seen in Jefferson and Orleans Parishes, which had increases over 100 percent. The drug-involved death rates increased over the study period, and more than double in Louisiana. The death rates increased in all the study parishes, except St. Bernard Parish, which experienced no change. The increases ranged from 25% to 191.2%, with the largest increase in East Baton Rouge Parish. Decreases were seen in different years in Ascension, Lafayette, and St. Bernard Parishes.
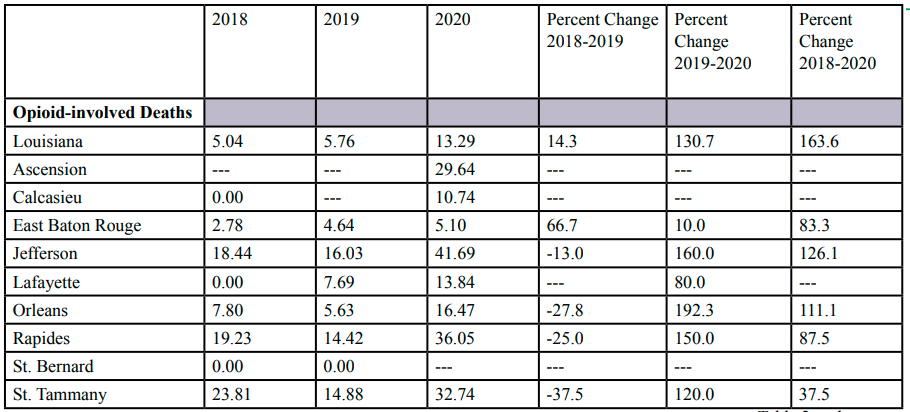
Table 2: Overall Opioid-involved and Drug-induced Death Rates,* Blacks
Opioid-involved death rates among non-Hispanic Whites increased every year in during the study period in Louisiana (Table 3). The increase during the study period was over 100%, with a 59.5% increase from 2019 to 2020. This same trend was seen in the study parishes except for Orleans Parish, which had an 8.3% reduction. The increases across the study parishes ranged from 14.8% to 384.6 percent, with the largest increase in Lafayette Parish and the smallest increase in East Baton Rouge Parish. Due to data limitations, percent change was not calculated for Calcasieu Parish. Again, decreases were seen in different years in Calcasieu and St. Bernard Parishes. Drug-involved death rates increased in Louisiana 44.4% during the three-year study period, with a 32.4% from 2019 through 2020. Increases were observed in all study parishes, except for Ascension Parish. The greatest increase was seen in East Baton Rouge Parish (86.8%) and the lowest increase in St. Bernard Parish (3.3%).
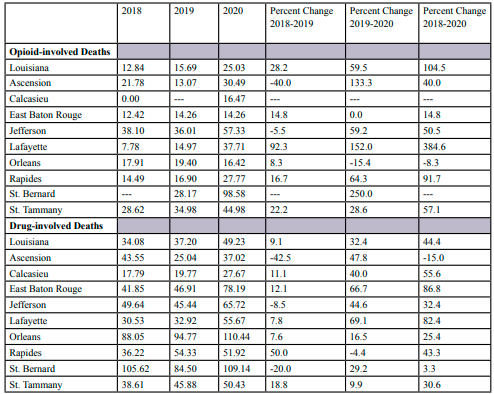
Table 3: Overall Opioid-involved Death Rates,* Whites
Table 4 shows opioid-involved and drug-involved death rates for females. In Louisiana, opioid-involved death rates increased 110.4% during the study period. The increase from 2018 to 2019 was 33.6%, and increased 57.5% from 2019 through 2020. Opioid-involved deaths increased in every study parish except for Rapides Parish, which had no change. Due to data limitations, rates were not calculated for Calcasieu and St. Bernard Parish for the study period. The increases ranged from 64% (St. Tammany Parish) and 20% (East Baton Rouge Parish). Decreases in opioid-involved death rates occurred from 2018 through 2019 in Ascension, Jefferson, and Orleans Parishes. Drug-involved death rates increased 50.7% in Louisiana during the study period, after a 54.2% decrease between 2018 through 2019. The increase from 2019 through 2020 was 228.8%, which was greater than any of the study parishes. Drug-involved death rates increased in the study parishes during the study period except for Ascension and St. Bernard Parishes. The greatest increase was seen in East Baton Rouge Parish and Rapides Parish had the lowest increase in drug-involved deaths. As was seen in Louisiana, reductions in death rates were seen in Ascension, Calcasieu, and Jefferson Parishes from 2018 through 2019.
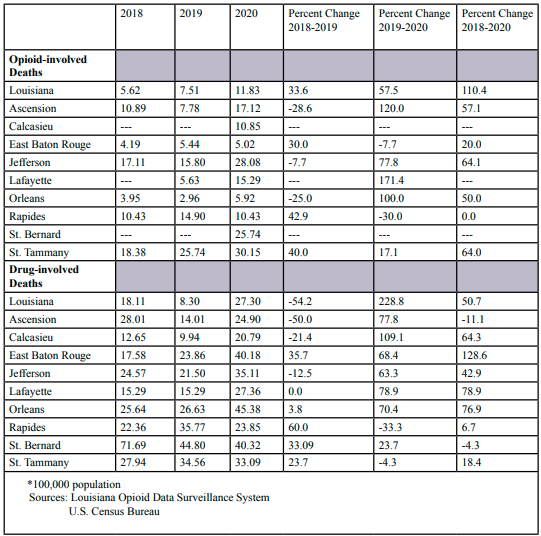
Table 4: Overall Opioid-involved and Drug-induced Death Rates,* Females
Opioid-involved deaths trends among males are similar as was seen among females (Table 5). In Louisiana, opioid-involved death rates increased every year during the study period. From 2018 through 2020 death rates increased 113.1%, which is slightly higher than was seen in females. Increases in opioid-involved death rates also were observed across all study parishes. The parish-wide death rates increases ranged from 32.4% (Orleans Parish) and 440.6% (Lafayette Parish). Percent changes could not be calculated for Calcasieu and St. Bernard Parishes because of data limitations. As was seen among females, decreases in the opioid-involved death rates from 2018 through 2019 were seen in Ascension, Jefferson, Orleans, and Rapides Parishes. Drug-involved death rates among males increased every year in Louisiana, with a 54.3% increase during the study period. Drug-involved death rates increased in every study parish and ranged from 10% to 125% from 2018 through 2020. Increases were observed each year among study parishes except from 2018 through 2019 in Ascension, Jefferson, and St. Bernard Parishes.
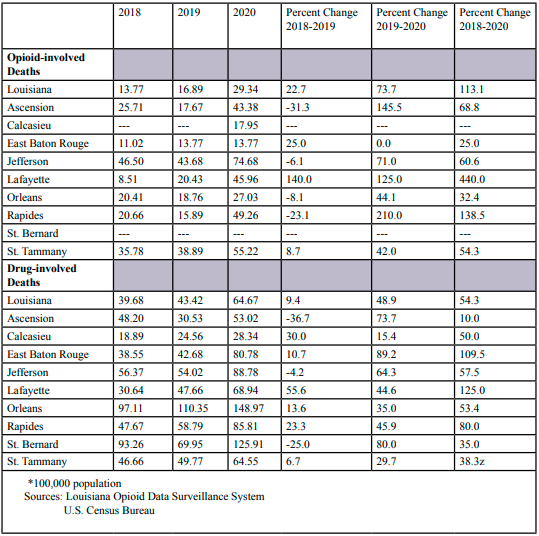
Table 5: Overall Opioid-involved and Drug-involved Death Rates,* Males
Discussion
The emergence of COVID-19 has had an amplifying effect on the opioid epidemic. In fact, it has been stated that the COVID-19 pandemic has caused a national relapse trigger [22]. COVID-19 response has offered insights to the unintended consequences for individuals who abuse and overdose opioids. Social distancing and isolation have boosted the opioid epidemic. This increasing epidemic has been obscured by the COVID-19 pandemic [23].
It is important to note the increase in death rates in Louisiana from 2019 through 2020. This time-period coincides with the beginning of the COVID-19 pandemic. Overall, in Louisiana the increase in opioid-involved deaths was greater from 2019 through 2020 than from 2018 through 2019. The same is seen in the study parishes, except for East Baton Rouge Parish, which experienced a decrease in the death rate. For the most part the difference between the two time periods was substantial. This trend was similar in drug-involved death rates in Louisiana and the study parishes. The differential effect of COVID-19 on opioid-involved deaths is very clear when mortality rates are compared from 2018-2019 and 2019-2020.
Opioid-involved and drug-involved death rates increased among non-Hispanic Blacks in Louisiana from 2018-2020. The percent increase for opioid-involved death rates from 2018-2020 was 163.6%, with a 130.7% increase from 2019 through 2020. Drug-involved deaths rates increased 78.4% from 2019 through 2020 and 107.5% over the three-year study period.
Non-Hispanic Blacks are disproportionate affected by the COVID-19 pandemic, including those with opioid use disorder. A study in Philadelphia showed that non-Hispanic Blacks had a 12% greater increase in opioid-involved deaths compared to non-Hispanic Whites. One of the salient effects of COVID-19 is the racial disparity in opioid-involved deaths [24]. This was seen in the study of Louisiana and study parishes. Across the study parishes, opioid-involved death rates increased from 37.5% in St. Tammany Parish to 126.1% in Jefferson Parish. Due to data limitations, opioid-involved death rates were not available for Ascension, Calcasieu, Lafayette, and St. Bernard Parishes.
The comparison of opioid-involved and drug-involved death rates among males and females indicate similar increases state-wide. This is interesting because for decades the opioid epidemic has had a more profound impact on males. Specifically, the increase in drug-involved death rates increased 5-fold among females compared to males during the first year of the pandemic. Across the study parishes during the first year of the COVID-19 pandemic opioid-involved death rates increased from 17.7% to 120% in most parishes among females and two parishes experienced decreases of 7.7 to 30% in deaths. Among males, all study parishes experienced increases in mortality in both opioid-involved and drug-involved deaths.
The COVID-19 pandemic and the opioid epidemic has many commonalities. The main common aspect is both can be mitigated through vaccination. COVID-19 vaccines were initially used about 12 months ago, with subsequent booster doses. Vaccine compliance has been less than expected with less than 70% of the U.S. population fully vaccinated. Evidence has supported the use of COVID-19 vaccines in reducing infection and hospitalization [25]. Opioid abuse has been successfully treated, except for fentanyl. A fentanyl vaccine is currently in development stages, with less than optimum support for the government and private industry [26]. Due to the urgency of the COVID-19 pandemic it has been shown that treatment for opioid abuse has a lower priority [27]. A side effect is a reduced access to emergency services for opioid abuse treatment [28].
What is being done in response to this challenge regarding the opioid crisis we are being faced with? First, telehealth services for COVID-19 have been expanded by the Centers for Medicare and Medicaid services for providers that are reimbursed through Medicare. Secondly, the Substance Abuse and Mental Health Services Administration (SAMHSA) is recommending using outpatient treatment options when appropriate to decrease the transmission of COVID-19 in facilities used to treat opioid disorders. In addition, they are recommending more lenient in providing take home prescriptions. The Drug Enforcement Agency has waived federally mandated in person visits for controlled prescribing of drugs like buprenorphine, which is used to treat opioid dependency [29]. These steps are just the beginning in the ongoing battle to overcome opioid dependency in the aftermath of COVID-19.
The study of opioid-involved and drug-involved deaths increased significantly during the first year of the COVID-19 pandemic in Louisiana. This increase was seen across several parishes in areas of relatively large populations. It is notable that in some parishes the mortality rate the year before the COVID-19 were decreasing in both opioid-involved and drug-involved deaths. The COVID-19 pandemic reversed this decreasing trend, and exacerbated the death rates state-wide. Although the COVID-19 pandemic has caused less attention to the opioid epidemic, COVID-19 has had a negative impact on opioid-involved deaths.
Acknowledgements
Research reported in this study was funded, in part, by the National Institute of Minority Health and Health Disparities of the National Institutes of Health under grant S21MD1007136.
Conflict of interest:
The authors declare no conflict of interest.
References
Fos, P.J., Honoré, P.A.,& Kellum, K.P. (2020). The relationship of diabetes and COVID-19: A health disparity. Diabetes & its Complications. 4(1):1-8.View
Woolf, S.H., Chapman, D.A., Sabo, R.T., Weinberger, D.M., Hill, L., & Taylor, L.D.H. (2020). Excess deaths from COVID-19 and other causes. JAMA, 324(15):1562-1654.View
Woolf, S,H., Chapman, D.A., Sabo, R.T., Zimmerman, E.B. (2021). Excess deaths from COVID-19 and other causes in the US, March 1, 2020 to January 2, 2021. JAMA, 325(17):1786- 1789. View
Haley, D.F., & Saitz, R. (2020). The opioid epidemic during the COVID-19 pandemic. JAMA, 234(16): 1615-1615. doi:10.1001/ jama.2020.18543View
Wainwright, J.J., Mikre, M., Whitley, P., Dawson, E., Huskey, A., Lukowiak, A., & Giroir, B.P. (2020). Analysis of drug test results before and after the U.S. declaration of a national emergency concerning the COVID-19 outbreak. JAMA. doi:10.1001/jama.2020.17694View
National Center for Health Statistics (2021). Provisional Drug Overdose Death Counts. Retrieved from https://www.cdc.gov/ nchs/nvss/ysrr/drug-overdose-data.htmView
Tucker, Green
Wakeman, S.E., Green, T.C., & Rich, J. (2020). An overdose surge will compound the COVID-19 pandemic if urgent action is not taken. Nature Medicine, 26(6): 816-820. View
Linas, B.P., Savinkina, A., Barbosa, C., Mueller, P.P., Cerdá, M, Keyes, K., & Chhatwal, J. (2020). A clash of epidemics: Impact of the COVID-19 pandemic response on opioid overdose. Journal of Substance Abuse Treatment, 120:108158. View
Gomes, T., Kitchen, S.A., & Murray, R. (2021). Measuring the burden of opioid-related mortality in Ontario, Canada, during the COVID-19 pandemic. JAMA Network Open, 4(5):e2112865. View
Becker, W.C., & Fiellin, D.A. (2020). When epidemics collide: Coronavirus disease 2019 (COVID-19) and the opioid crisis. Annuals of Internal Medicine ?????????View
Chandler, R.K., Villani, J., Clarke, T., McCance-Katz, E.F., & Volkow, N.D. (2020). Addressing opioid overdose deaths: The vision for the HEALing communities study. Drug and Alcohol Dependence, 217:108329. View
Hartnett, K.P., Kite-Powell, A., DeVies, J., Colletta, M.A., Boehmer, T.C., Adjemian, J., & Gundlapalli, A.V. (2020). National Syndromic Surveillance Community of Practice, 2020. Impact of the COVID-19 pandemic on emergency department visits -- United States, January 1, 2019-May 30, 2020. MMWR Morbidity and Mortality Weekly Report 69, 699-704.View
Lange, S.J., Ritchey, M.D., Goodman, A.B., Dias, T, Twentyman, E., Fuld, J, … , Yang Q. (2020). Potential indirect effects of the COVID-19 pandemic on the use of emergency departments for acute life-threating conditions – United States, January – May 2020. MMWR Morbidity and Mortality Weekly Report 69, 795- 800. View
Liu, C.H., Stevens, C., Conrad, R.C., & Hahn, H.C. (2020). Evidence for elevated psychiatric distress, poor sleep, and quality of life concerns during the COVID-19 pandemic among U.S. young adults with suspected and reported psychiatric diagnoses. Psychiatry Research, 292, 113345.View
Mason, M., Welch, S.B., Arunkumar, P., Post, L.A., & Feinglass, J.M. (2021). Opioid overdose deaths before, during, and after an 11-week COVID-19 stay-at-home order: Cook County, Illinois, January 1, 2018-October 6, 2020. Morbidity and Mortality Weekly Report, 70(10): 362-363.View
Kelley, M.A., Lucas, J., Stewart, E., Goldman, D., & Doctor, J.N. (2021). Opioid-related deaths before and after COVID-19 stay-at-home orders in Los Angeles County. Drug and Alcohol Dependence, 228:109028.
Friedman, J., & Akre, S. (2021). COVID-19 and the drug overdose crisis uncovering the deadliest months in the United States, January – July 2020. American Journal of Public Health, e1-e8.View
Louisiana Department of Health. Louisiana Opioid Data and Surveillance System. http:///ldh.la.gov/index.cfm/page/3192. Accessed February 1, 2021.View
World Health Organization. International Classification of Diseases; Manual of the International Statistical Classification of Diseases, Injuries, and Causes of Death: Tenth Revision (ICD-10). Geneva, Switzerland, WHO. http://apps.who.int/ classifications/icd10/browse/2016/en.View
United States Census Bureau. U.S. Census Bureau Quickfacts. https://www.census.gov/quickfacts. Accessed February 1, 2021.View
Hoffman, J. (2020). With meetings banned, millions struggle to stay sober on their own. New York Times. March 26,2020. Retrieved from https://nytimes.com/2020/03/26/health/ coronavirus-alcoholics-drugs-online.htmlView
Silva, M.J., & Kelly, Z. (2020). The escalation of the opioid epidemic due to COVID-19 and resulting lessons about treatment alternatives. American Journal of Managed Care, 26(7): e202-e204.View
Khatri, U.G., Pizzicato, L.N., Viner, K., Bobyock, E., Sun, M., Meisel, Z.F., & South, E.C. (2021). Racial/ethnic disparities in unintentional fatal and nonfatal emergency medical services-attended opioid overdoses during the COVID-19 pandemic in Philadelphia. JAMA Open Network, 4(1): e2034878. doi:10.1001/jamanetworkopen.2020.34878View
Whitaker, H.J., Tsang, R.S.M., Byford, R., Andrews, N.J., Sherlock, J., Pillai, P.S., … . Bernal, J.L. (2022). Pfizer-NBioTech and Oxford AstraZeneca COVID-19 vaccine effectiveness and immune response among individuals in clinical risk groups. The Journal of Infection. View
Kosten, T.R., & Petrakis, I.L. (2021). The hidden epidemic of opioid overdoses during the coronavirus disease 2019 pandemic. JAMA Psychiatry, 78(6): 585-586.View
Ochalek, T.A., Cumpston, K.L., Willis, B.K., Gal, T.S., & Moeller, F.G. (2020). Nonfatal opioid overdoses at an urban emergency department during the COVID-19 pandemic. JAMA, 324(16):1673-1674. View
Slavoka, S., Rock, P., Bush, H.M., Quesinberry, D., & Walsh, S.L. (2020). Signal of increased opioid overdose during COVID-19 from emergency medical services data. Drug and Alcohol Dependence, 214:108176.View
U.S. Department of Health and Human Services. Indian Health Services. Opioids and the COVID-19 pandemic. http://www. ihs.gov/opioids/covid19. Accessed on March 29, 2022.