
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 6 (2022), Article ID: JPHIP-206
https://doi.org/10.33790/jphip1100206Review Article
Empirical Evidence on the Impact of Infectious Diseases on Health-Outcome in Nigeria
Declan Chibueze Onyechege, PhD.1, Norashidah Mohamed Nor, PhD.2*, Wan Azman Saini Bin Wan Ngah, PhD3, & Mohd Naseem Bin Niaz Ahmad, PhD4
1Student School of Business and Economics, (Formerly Known Faculty of Economics and Management), Universiti Putra Malaysia, 43400 UPM Serdang, Selangor, Malaysia.
2Associate Professor, School of Business and Economics, Deputy Dean Undergraduate and Alumni, (Formerly Known Faculty of Economics and Management), Universiti Putra Malaysia, 43400, Selangor, Malaysia.
3Associate Professor, School of Business and Economics, (Formerly Known Faculty of Economics and Management), Universiti Putra Malaysia, 43400 UPM Serdang, Selangor,Malaysia.
4Senior Lecturer, School of Business and Economics, (Formerly Known Faculty of Economics and Management), Universiti Putra Malaysia, 43400 UPM Serdang, Selangor,Malaysia.
Corresponding Author Details: Norashidah Mohamed Nor, PhD., Associate Professor, School of Business and Economics, (Formerly Known Faculty of Economics and Management), Universiti Putra Malaysia, 43400 UPM Serdang, Selangor, Malaysia. E-mail: norashidah@upm.edu.my
Received date: 12th May, 2022
Accepted date: 10th June, 2022
Published date: 13th June, 2022
Citation: Onyechege, D.C., Mohamed Nor, N., Bin Wan Ngah, W. A. S., & Bin Niaz Ahmad, M. N., (2022). Empirical Evidence on the Impact of Infectious Diseases on Health-Outcome in Nigeria. J Pub Health Issue Pract 6(1): 206.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Purpose: This research is an empirical investigation on the rate in which infectious diseases have impacted on health outcome in Nigeria. Over the years, infectious diseases such as HIV/AIDS, Tuberculosis and others have been rampaging the health outcome of the people mostly those in Africa and in Nigeria to be precise. Many people have lost their precious life because of these infectious diseases and many are still in anticipation of losing their lives too. Efforts by the Nigeria government to curtail the prevalence of infectious diseases seems abortive. This paper is to find out the level in which infectious diseases have been affecting health outcome of the people in Nigeria and proffer a solution to the menace.
Design/Methodology/Approach: This paper is an empirical research. The methodology used is the Auto Regressive Distributed Lag (ARDL) model which helps to find out the rate of impacts and effects of infectious diseases on health outcome in Nigeria. Being an empirical study, secondary annual data (1985 – 2018) were used and their sources are reliable.
Findings: The result from the findings shows that infectious diseases have negative impacts on health outcome in Nigeria over the years of study. However, HIV/AIDS was significant at 10% over those years, while Tuberculosis showed no significance impact on health outcome.
Originality/Value: This study approached infectious diseases and health outcome in Nigeria. It will help to foster good economic policies to curb the prevalence of infectious diseases and boast health outcome in Nigeria knowing that most of the efforts the government of Nigeria abducted previously seem abortive. The conclusion part of this study is a good policy implementation ideas and strategic plans to eradicate the menace.
Keywords: ARDL model, Health outcome, HIV/AIDS, Tuberculosis, Nigeria.
Introduction
Health is a major component of human development and it is a relative term that can be defined in many ways according to scholastic perceptions. Health is defined as the state of wellbeing of a man, absence of diseases or the general condition of someone’s mind and body, WHO (1948). Human health is a component which fosters economic growth and investment in health improves the productive and earning capacity of individuals and consequently for nations at large, Grossman [1] and when the health of people in a country is affected negatively, the economic growth of that country will be expected to decrease [2,3].
Health outcome is broadly used in health care industries and the meaning of the term varies according to the user and the context. In health care industry, Health outcome means the changes that occurs in current and future population health status that can be attributed to an intervention, which can be measured with the rate of mortalities or life expectancy of the people in the society while life expectancy is the number of years a new born baby is expected to live should the prevailing pattern of mortalities at the time of birth remain the same. Life expectancy is a major indicator of the status of health. As of 2009, the average life expectancy of Nigerians is 60.87 which is 63 for women and 59 for men, which is among the lowest in Sub-Sahara Africa, Lower Middle Income Countries and in the world, World Bank (2021). See figure 1 above.
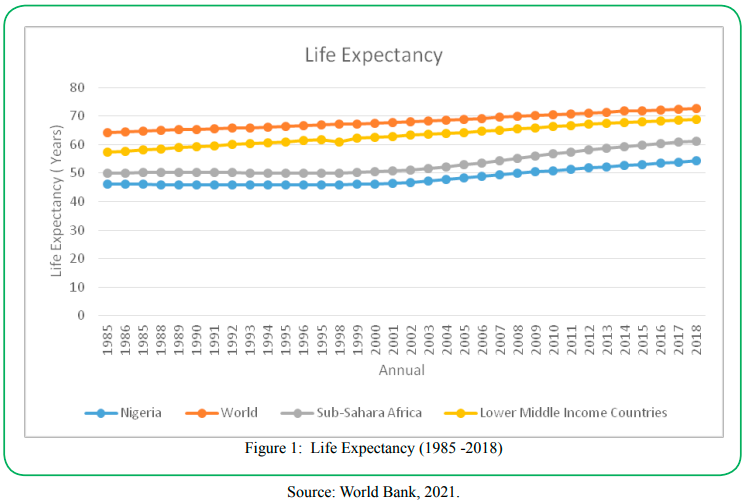
Figure 1: Life Expectancy (1985 -2018)
Infectious disease is a type of diseases that causes poor health outcome. Microorganisms are the major agents of infectious diseases which spreads from one person to the other by indirect means or by a vector.In Nigeria infectious diseases are very rampant, their impacts are immense, affecting life of the people directly, they are the most diseases that causes death as well create a remarkable impact in the society, political systems and plans of the country, WHO (2013). The prevalence of infectious diseases in Nigeria are seen as one of the problems in the country.
Human Immune Virus/Acquired Immune Deficiency Syndrome (HIV/AIDS), and Tuberculosis are two infectious diseases which have imposed high risk and challenge on the health outcome of Nigerians. HIV/AIDS which is incurable diseases posed a serious negative effect in the health outcome (life expectancy) and economic welfare of the citizens of Nigeria. Tuberculosis on the other hand, has caused a serious health Challenge, economic downfall and high health care expenditure in Nigeria. Both infectious diseases have great negative direct impact on health outcome in Nigeria.
In Nigeria, the total number of people living with HIV/AIDS were about 40.3 million in 2005, which represents about one-tenth of the worldwide pandemic and world’s third largest disease burden country. Nigeria is the second largest HIV/AIDS epidemic country in the world, as well Nigeria is one of the countries that has the highest rates of HIV new infection in Sub-Saharan Africa. Those who live with HIV/AIDS in Nigeria are mostly unaware of their status (UNAIDS/ WHO, 2005). In 2017, approximately 150,000 people died from HIV/AIDS in Nigeria and in 2018, about 1.9 million people were living with HIV and there are six states in Nigeria which accounts for 41% of people living with HIV, these states include Kaduna, Akwa Ibom, Benue, Lagos, Oyo and Kano.
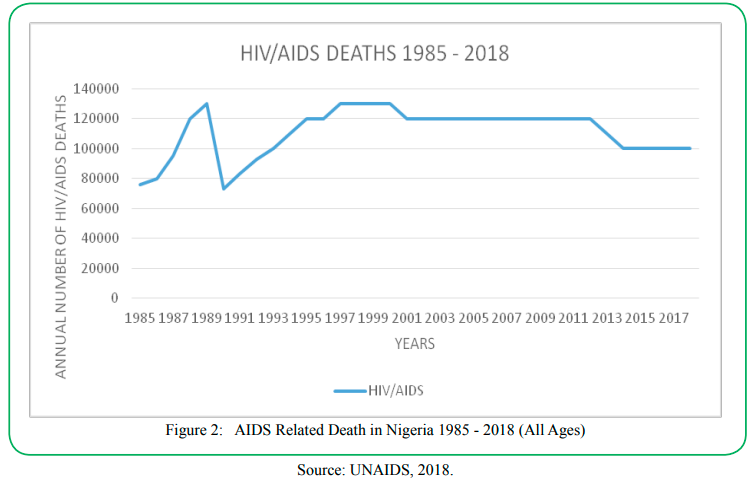
Figure 2: AIDS Related Death in Nigeria 1985 - 2018 (All Ages)
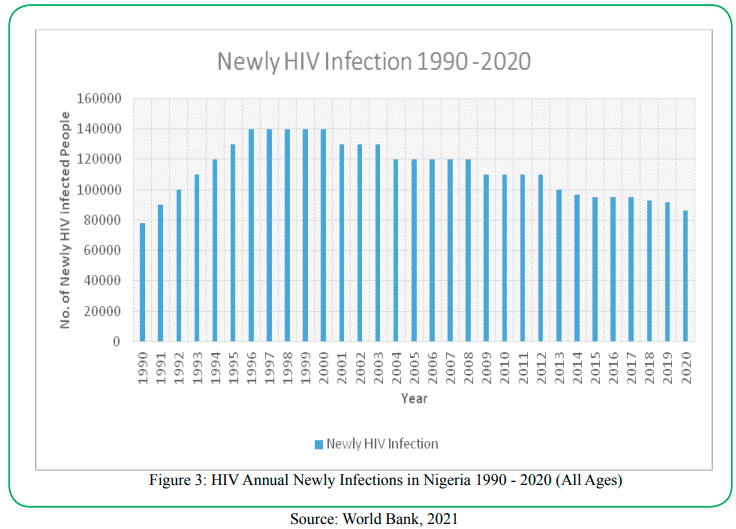
Figure 3: HIV Annual Newly Infections in Nigeria 1990 - 2020 (All Ages)
In Nigeria, 240,000 adolescents between the ages of 10 to 19 years lives with HIV, which made it 7% of the total number of people with HIV annually. The prevalence of HIV among this group varies regionally with 4.3% of 15-19 years old living with HIV in the South-South compared to 1.3% in the South East (WHO, 2016). The mortality rate in Nigeria among this group is rising. There are many factors that increase HIV vulnerability among young people which include, lack of knowledge and appropriate sexual reproductive health services.
Nigeria is ranked 10th among the 22nd countries in the world with a high burden of Tuberculosis. World Health Organization in 2010, estimated 210,000 new cases of all forms of TB in Nigeria, which is equivalent to 133/100,000 of the population. And, there were about 320,000 prevalent cases of TB in 2010, which is equal to 199/100,000 cases.
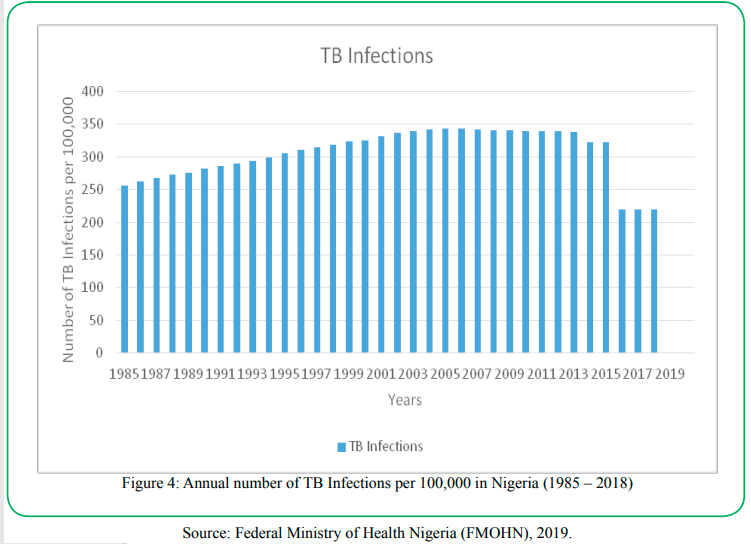
Figure 4: Annual number of TB Infections per 100,000 in Nigeria (1985 – 2018)
The Nigeria government fails to observe that the burden of infectious diseases is alarming, like Tuberculosis. Tuberculosis diseases in general, continue to make costly disruptions to trade and commerce in every region in Nigeria. FMOH (2003).
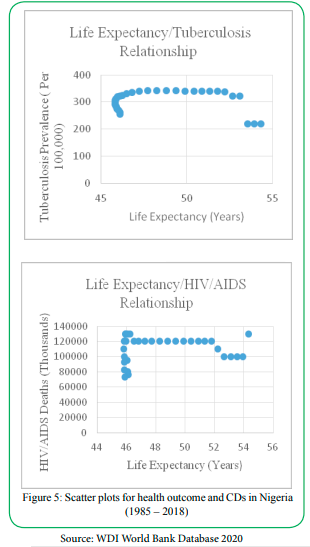
Figure 5: Scatter plots for health outcome and CDs in Nigeria (1985 – 2018)
The Health outcome and Communicable Disease relationship becomes important to be examined in Nigeria, considering the low life expectancy and its slow rate of increase and high rate of the prevalence of Communicable Disease in Nigeria.
The germ theory of diseases, Louis Pasteur [4] is a theory that is currently accepted scientifically for many diseases. The germ theory of diseases explains that, there are microorganisms known as pathogens or germs which can lead to diseases. It further illustrates that these small organisms are too tiny to see without magnification and they invade humans, animals and other living things which are known as their host. It clarified that the growth and reproduction of these microorganisms in their host can cause diseases. Also any microorganism or non-living pathogen that can cause diseases is also known as germs. Some of these microorganisms/pathogens are bacteria, protists, fungi, viruses, prions and others. Diseases caused by pathogens are known as infectious or communicable diseases. When pathogen is the principle cause of infectious diseases, environmental and hereditary factors can influence the seriousness of the infectious diseases, and also whether a future host/individual can be infected when exposed to the germs. Germ theory explains that infectious diseases are caused by the presence and actions of the micro-organisms in the body of the host.
The health outcome of the people or group of people in the same locality has many link with communicable diseases. This implies that it is the prevalence of diseases that leads to the quest to know the health outcome or health status of the people in the same locality. Related researches (time series and panel data estimation) have used single variables like life expectancy, infant and under-5 mortality rates, as well maternal mortality rates as a measure of health outcome. Many other researchers have used variables such as the prevalence of diseases or incidence of infections, number of visits to the hospital, work absence due to illness, perceived health status, quality-adjusted life years and disability-adjusted life years, to measure the rate or level of health outcome of people or group of people.
A. Boutayeb [5], conducted a study titled “The Impact of Infectious Diseases on the Development of Africa”, using Bivariate correlational analysis and multivariate linear stepwise regression as the method of analysis, the result of the study proved that HIV/AIDS, malaria, tuberculosis, acute respiratory infections and diarrheal disease are causing high mortality rates in Africa. Also, lker Etikan et al, [6] in their studies titled “Life expectancy; factors, malaria the most common disease affecting pregnant women in Africa [Nigeria and Cameroon]”, used the IBM SPSS 20, using the t-test method in their analysis concluded that Malaria, HIV/AIDS and Tuberculosis are most infectious diseases that affects people in Nigeria and Cameroun.
Empirical Model
This study used an economic model to express the relationship existing between health outcome and communicable diseases to evaluate the impact of communicable diseases on health outcome in Nigeria. The models for health outcome and communicable diseases is taken from the production function theory where output was specified as a function of factors of production, which depicts the relation between physical outputs of a production process and physical inputs (factors of production). It explains the amount of products that can be obtained from every combination of factors. It evaluates the marginal productivity of a particular factor of production, i.e the change in output for every additional unit of the factor of production, Mishra, S. K. [7]. A mathematical expression that explains the relationship between outputs and inputs is
Y = f( K, L, A) (1)
Where Y is output, K, L, and A are inputs which are combined in different ratios to obtain Y, and f is the functionality. This study adopts the same production function model stated in (1) to incorporate the impact of communicable diseases (inputs) on health outcome (outputs). The model is stated as below
LE = f (HA, TB, GEH, POP) (2)
where LE represents life expectancy (also known as health outcome), HA represents HIV/AIDS, TB represents Tuberculosis which are the communicable diseases, GEH which represents government expenditure on health, and POP represents the size of the people. Equation 2 is explaining what happens to health outcome (LE) when communicable diseases (HA and TB) are at prevalence and how does government expenditure on health (GEH) helps to improve health outcome considering the total population in the economy. Also the model in equation 2, explains how health outcome changes when there are changes in communicable diseases. Statistically, the empirical model for equation 2 are modified and the reduction of equations after taking the natural logarithm is written and stated below as:
InLEt = A + α1InHAt + α2InTBt + α3InGEHt + α4InPOPt + εt (3)
Where, A represents the intercept, while α1, α2, α3, α4 are coefficients of the independent variables. The coefficient of the independent variables α1, α2, α3 and α4 ranges between 0 and 1, as a result of the elasticity nature or characteristics of the coefficients because they explain the responsiveness of the dependent variables as a result of the changes that occurs in the independent variables in the model or equation with ceteris paribus, Cobb & Douglas [8]. From all equations, εt represents the error term restricted within the classical statistics assumptions. Subscript “t” represents time which is annually. For the sake of clarity, statistical analysis and understanding, all variables were converted into natural logarithmic form (ln) to enable result in elasticity form.
Methodology And Data
The methodology used for this study is the Auto Regressive Distributed Lag (ARDL) model. It was employed after the unit root test was conducted and the result proved that the variables are in mix mode stationary. The estimation method will proceed by computing the bound test to check the cointegration that exists among the variables during the period of study, there is long-run cointegration if the F-statistics value is greater than the upper bound value of the critical value and the otherwise holds. If the F-statistics value is in between the critical values, the result is inconclusive. The bound test model is written as follows:
∆InLEt = A +α1InLEt-1 + α2InHAt-1 + α3InTBt-1 + α4InGHEt-1 + α5InPOPt-1+ ∑ P i=1β1 ∆ InLEt-i + ∑q i=0 β2 ∆ InHAt-i + ∑ri=0β3 ∆ InTBt-i + ∑s i=0 β4 ∆ InGHEt-i + ∑t i=0 β5 ∆ InPOPt-i + εt (4)
where Δ, first difference operator; In, logarithm operator; A, intercept; α1-5; and β 1-5 are coefficient of the variables; p,q,r,s and t are maximum lag order; ɛt, is the white noise of error term and the hypothesis for the bound test is stated as;
Ha: α1 = α2 = α3 = α4 = α5 = 0 (There is no long-run cointegration between the variables)
Hb: α1 ≠ α2 ≠ α3 ≠ α4 ≠ α5 ≠ 0 (There is long-run cointegration between the variables)
The next test is the long-run coefficient test. The long run coefficient test is conducted in order to identify the long run relationship between the dependent variable and independent variables. The value of the coefficients of the variable explains the rate of relationship that exists in the model. The formula for this test is as below.
InLEt = A + ∑p i=1 α1 InLEt-i + ∑q i=0α2 InHAt-i + ∑r i=0α3 InTBt-i + ∑s i=0α4 InGHEt-i + ∑t i=0α5 InPOPt-i + ɛt (5)
The error correction model is the next test to run after the long run coefficient test. The error correction model test is the short run dynamic coefficient test which is conducted to identify the speed of adjustment to the equilibrium between the dependent and independent variables. The formula for this test in respect to the objective is:
ΔInLEt = δ0 + γ ECTt-1 + ∑P i=1β1 ΔInLEt-i + ∑q i=0β2 ∆ InHAt-i + ∑ri=0β3 ∆ InTBt-i + ∑s i=0β4 ∆ InGHEt-i + ∑ti=0β5 ∆ InPOPt-i + ɛt (6)
From equation 6, γ is the error correction term (ECT) which is used to measure the speed of adjustment parameter among the variables in the model. The diagnostic test is the last test to conduct when using the ARDL model to estimate the equation. The diagnostic test is conducted in order to identify and examine if problems exist in the model. The selected tests are the Cusum and Cusum square test, autocorrelation test, and heteroscedasticity test.
The cusum and cusum square test is conducted to diagnose the stability of the model. The test plots the cumulative sum together to ensure the regression result should be between the area of two critical lines of 5%. The autocorrelation test is performed to identify the correlation between the series members of observation. The test can be conducted by using the Run test, Durbin Watson d test, and Breush Godfrey test. According to this test, the null hypothesis is rejected when the autocorrelation is below the 1%, 5% and 10% level of significance. However, the null hypothesis is failed to be rejected when the Chi-square value is larger than the p-value. Heteroscedasticity test is conducted to check if there is existence of non-constant variance in the model. This test can be conducted by using different methods, namely white’s General Heteroscedasticity test, Pak test, Goldfeld-Quandt test, as well Breush Pagan Godfrey test. There is no heteroscedasticity problem in the model when the Chi-square value is more than the p-value.
Data
Life expectancy (LE) at birth in total years lived measured in years. Life expectancy is the dependent variable in this model used to measure the health outcome of the people in Nigeria. Life expectancy is a good measure of health outcome in this research because this research is focusing on the health outcome as a result of the impact of infectious diseases. HIV/AIDS (HA) and Tuberculosis (TB) are the population of the people in the society that have been infected by the diseases, and they are the most two communicable diseases used in this study and are chosen in this study because of their serious negative economic impacts they contribute to the Nigeria society. Government expenditure on health (GEH) which is the government health expenditure per capita measured in United State Dollars is a percentage of the gross domestic product per capita obtained by dividing the government health expenditure as percentage of gross domestic product with the total population of the people in Nigeria. Population (POP) is the number of people in the Nigeria society measured in millions and it has a positive and negative relationship to health outcome. The sources of all the variables are from world bank, except for Tuberculosis which was obtained from world health organization (WHO).
Result Estimation and Analysis
Descriptive statistics
The descriptive statistics of the variables are found in table 1 below. It contains the standard deviation, mean, minimum, maximum values of all the variables used in this study. In addition, table 2 is the covariance matrix of the variables used in this study.
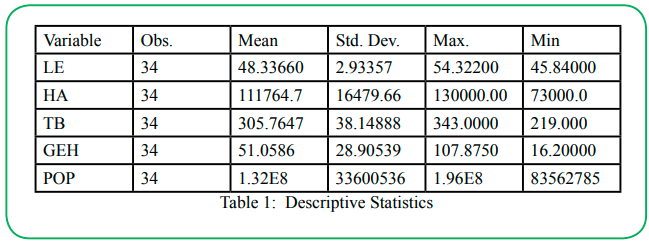
Table 1: Descriptive Statistics
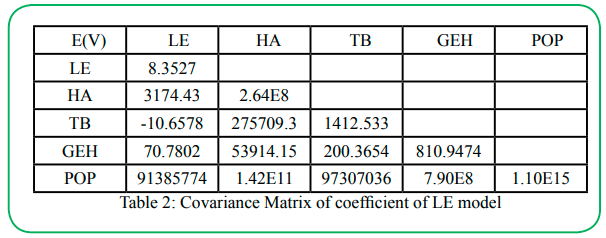
Table 2: Covariance Matrix of coefficient of LE model
Unit Root Test Result
We applied the Augmented Dickey Fuller (ADF) test to find out the integration of the series while Philip Perron (PP) test is employed for confirmatory analysis. The result shows that LE is stationary only at level with constant and trend. HA, TB and POP are stationary at level and first difference. While GEH is only stationary at the first difference. All the result mentioned is applicable to ADF and PP unit root test. The variables are of mix mode stationary.
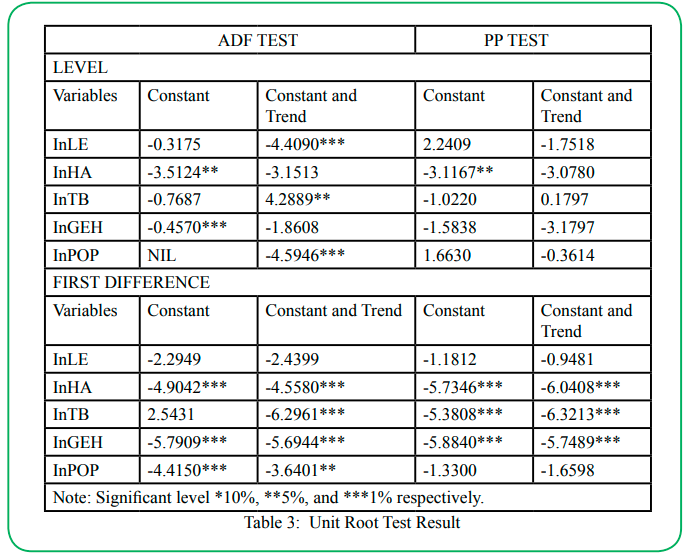
Table 3: Unit Root Test Result
ARDL Bound Test
The findings from this test prove that there is long-run cointegration because the computed F-statistics (16.9058) is greater than the 1% critical values of the upper bound (5.532). There is cointegration for all the variables in the model at 1% significant level, hence long-run relationship is confirmed.
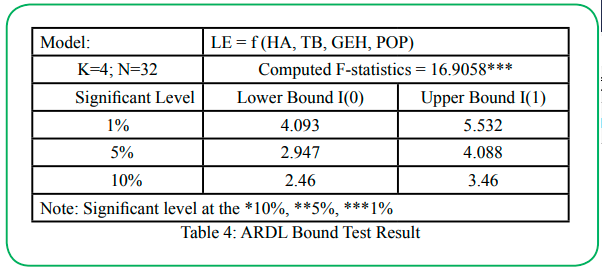
Table 4: ARDL Bound Test Result
ARDL Estimated Long-run Coefficient Test
The estimation of this model for LE is based on the ARDL lag (2, 0, 0, 2, 1) for LE, HA, TB, GEH and POP respectively. The result is presented in Table 5.
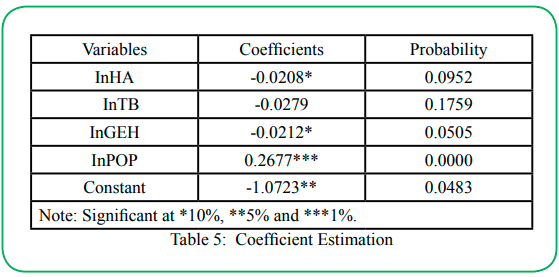
Table 5: Coefficient Estimation
The result from table 5 shows that when HA and GEH index decreases by 10%, while other variables remains constant (ceteris paribus assumption), there will be increase in health outcome (LE) at 0.2% and 0.21% respectively, hence there are negative and significant impact of HA and GEH on health outcome in the long-run relationship. TB has no significant impact on health outcome but there is negative relationship between TB and health outcome in Nigeria. Also, when POP index increases by 1% while other variables remain constant, there will be increase in health outcome at 0.27%, which proves a positive and significant relationship between POP and health outcome.
Error Correction Model (ECM) Test
The error correction model or short run dynamic test is to find out the speed of adjustment which the dependent variable may use to return to normalcy or equilibrium when there are changes in the independent variables. See table 6 below for the results.
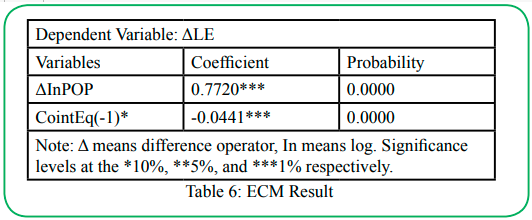
Table 6: ECM Result
According to Pahlavani et al. [9], the error correction term (ECT) is achieved and stable when the value of the ECT is negative and statistically significance at 1% level. Banerjee et al. [10] explains that when ECT is significance, it proves also the existence of long-run relationship in the model. From table 6 above, the ECT is -0.0441 and it is highly significant at 1% level, indicating that the ECT is stable and significant. It indicates that any deviation in the short-run will take 4.4% annually to restore the state of equilibrium in the long-run.
CUSUM and CUSUM of Square Test
The CUSUM and CUSUM of Square test is one of the diagnostic tests needed in the ARDL model in order to check the stability of the model. This is a graph showing the cumulative sum at the area of two critical lines of 5%. See figure 6.
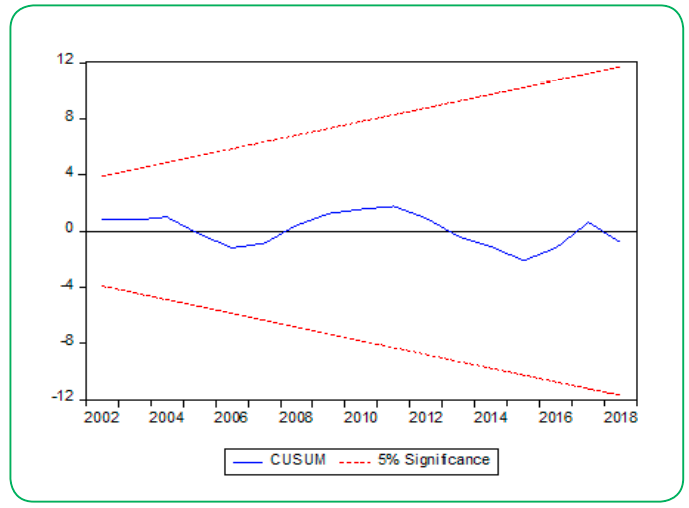
Figure 6(a): CUSUM Test and CUSUM of Square Test
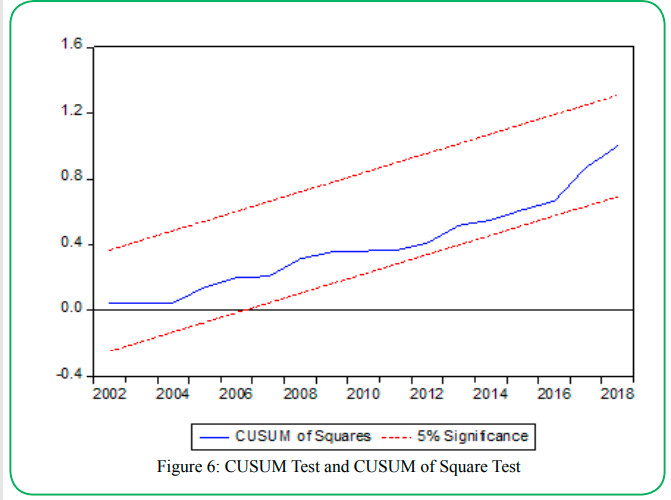
Figure 6(b): CUSUM Test and CUSUM of Square Test
Examining the stability of the long term on the variables as well the short term equations to ensure that the robustness of the specified models considering both the long-run and short-run coefficient is stable, figure 6 above are the result of the CUSUM and CUSUM of Square test respectively. It explains that at 5% level of significance, the specified model is stable and their test line falls within the boundary of the critical lines. It proves that there is a long-run relationship and stability of coefficient that exists among the variables over the sample period of 1985 -2018.
Diagnostic Test
Table 5 shows the result of the auto-correlation and heteroscedas ticity.
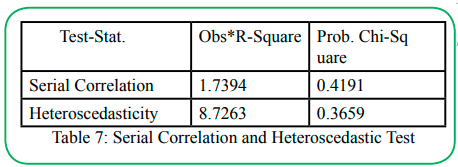
Table 7: Serial Correlation and Heteroscedastic Test
From table 7 the serial/auto correlation indicates that Obs*R-square recorded 1.7394 and its probability (Chi square) recorded 0.4191. Therefore, there is nonexistence of auto correlation problem in the model because the value of the Obs*R-square is greater than the value of the probability and the probability value is 41.9% which is above the 10% level of significance. Also the heteroscedasticity test proves that Obs*R-square has a value of 8.7263 which is higher than the value of the probability Chi-square of 0.3659 (36.5%) which is above the 10% level of significance. Hence, the model has no residual heteroscedasticity.
Conclusion
This study is to analyse the impact of communicable diseases on health outcome in Nigeria. This study is motivated by the high rate of prevalence of infectious diseases in Nigeria and low life expectancy which has eaten the fabrics of Nigerians. This study is based on the Germ theory of diseases which had the notion that diseases can be spread or transmitted from one person to another or from one point to another, Ferreira, L., Dupont, M., Fracastoro, G. and Bonati, M. [11]. The result shows that communicable diseases (HIV/AIDS and Tuberculosis) used in the model as the independent variables, has a negative relationship with life expectancy which is the dependent variable.
Policy Implications
This study provides an evidence that increase in communicable diseases decreases health outcome. It also proved that there has been high increase of communicable diseases prevalence in Nigeria over the years. The Nigeria government at the same time has engaged with many efforts to combat the high prevalence of communicable diseases in Nigeria. Despite all the efforts put by the government, communicable diseases are still rampant. Therefore, it is important for the Nigeria government to improve health care facilities and human capital which are most important in the health care industry. Embezzlement of public fund by the leaders, corruption among the leaders has become the order of the day in Nigeria and this should stop.
Political power acquisition and political thuggery, killings, assassinations, kidnappings and all sort of social ills going on in Nigeria is a propeller to prevalence of communicable diseases which decreases health outcome and shortens life expectancy, these should be corrected.
Limitations and Recommendation
The limitation of this study is the up to date data. The annual data used in this study is from 1985 to 2018. This study intended to use data up to the year 2021 but some of the data to some variable were not available. So there is need for further research using data from 2019. There may be need for a cross sectional data from states in Nigeria to find the actual state which has the highest number of communicable diseases in Nigeria. Life expectancy was used as a proxy for health outcome. It is pertinent to understand that there are other proxies for health outcome in a country such as infant mortality rate, maternal mortality rate, under-5 mortality rate that should be considered as a proxy in further research to see how communicable diseases affects health outcome.
Acknowledgements
We are thankful to God Almighty while this study is being executed. All papers cited for this study are referenced. Compliance on ethical standards are respected and there is no conflict of interest for this paper.
Competing interests:
The authors declare that they have no competing interests.
References
Grossman, M. (1972a). On the concept of health capital and the demand for health. Journal of Political Economy 80:223-255.View
Barro (1991). Economic Growth in a Cross Section of Countries. The Quarterly Journal of Economics, Vol. 106, No. 2, pp. 407- 443View
Mankiw et al. (1992). A Contribution to the Empirics of Economic Growth. The Quarterly Journal of Economics, Volume 107, Issue 2, Pp 407–437,View
Louis Pasteur (1860). Germ theory of diseases.
A. Boutayeb, (2010). The Impact of Infectious Diseases on the Development of Africa Handbook of Disease Burdens and Quality of Life Measures. 2010 : 1171–1188. View
Nİlker E, et al (2018). Life Expectancy; Factors, Malaria the Most Common Disease Affecting Pregnant Women in Africa [Nigeria and Cameroon]. Global Jounal of Reproductive Medicine. 5(1): 555-651.View
Mishra, S. K. (2007). A Brief History of Production Functions. Working Paper. SSRN 1020577View
Cobb, C. W., & Douglas, P. H. (1928). A Theory of Production. The American Economic Review, 18(1), 139–165.View
Pahlavani et al. (2005). Structural breaks and cointegrating relationships in Iranian exports, imports and economic growth: An application incorporating the Autoregressive Distributive Lag (ARDL) procedure. American Journal of Applied Sciences,2(7), 1158-1165.View
Banerjee, et al (1998). Error-correction mechanism tests for cointegration in a single-equation Framework. Journal of time series analysis, 19(3), 267-283.View
Ferreira, L. , Dupont, M. , Fracastoro, G. & Bonati, M. (2017). Girolamo Fracastoro and the Origin of the Etymology of Syphilis. Advances in Historical Studies, 6, 104-112.View