
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 6 (2022), Article ID: JPHIP-207
https://doi.org/10.33790/jphip1100207Review Article
Health Disparities for Rural Youth
Anissa K. Howard, Bridget Holyfield-Moss, and Komanduri S. Murty*
*Alma Jones Endowment Professor and Chair, Department of Behavioral Sciences, Fort Valley State University, United States.
Corresponding Author Details: Komanduri S. Murty, PhD., Alma Jones Endowment Professor and Chair, Department of Behavioral Sciences, Fort Valley State University, United States.
Received date: 16th May, 2022
Accepted date: 11th June, 2022
Published date: 13th June, 2022
Citation: Howard, A.K., Holyfield-Moss, B., & Murty, K. S., (2022). Health Disparities for Rural Youth. J Pub Health Issue Pract 6(1): 207.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
This chapter examines the complexities surrounding exacerbated health disparities and their impact on rural youth mental health outcomes amid a global pandemic. Indisputably, a host of health, economic, and social challenges are associated with the unprecedented interruption caused by the global pandemic. In the same vein, several challenges and concerns about the overall academic and personal/ social experiences and outcomes of school-aged children have resulted in societal concerns about the overall preparation of this generation to meet the leadership and employment demands of a global society.
While the COVID-19 pandemic highlighted chronic issues related to health disparities to include intergenerational health, environmental and socioeconomic disparities, and educational inequities, many of these issues have had a longstanding, disproportionate effect on African American (AA) youth and their families. This is particularly the case with AA youth who live in rural communities, that are largely characterized by persistent poverty along the margins of society. Food and housing insecurities, social isolation, and lack of access to adequate physical and mental health resources are a few of the issues faced by these youth and other individuals who belong to these often tight-knit, rural communities. These issues, along with scarce or no availability of medical and mental health care services reflect larger systemic issues which speak to cultural determinism and social justice.
Keywords: Health Disparities; Global Pandemic; Mental Health, Social Justice, Cultural Determinism
Introduction
The COVID-19 pandemic continues to wreak havoc across the globe for its impact has had lasting effects on global healthcare. From the discovery of more contagious variants, medical staff shortages to hospital beds and supply shortages, the face of healthcare has been forever changed by the presence and persistence of the coronavirus. Concerted efforts from health scientists and healthcare professionals across the globe have contributed tremendously to advancements in understanding the transmission and treatment of COVID-19 [1]. Despite these efforts, there has been a steady increase in total cases worldwide. The United States leads the world in total number of cases with close to 60 billion confirmed cases of COVID-19 [2]. As the number of coronavirus cases steadily increases in the United States, so too does the demand for vaccinations, testing, and adequate treatment facilities. The demand for these things is most felt in rural America. For the purposes of this chapter, “rural” is referenced, consistent with the definition of the United States Census Bureau [3]. According to the Census Bureau (2019) [3], as any population, housing, or territory not located in an urban area.
As with the rest of the nation, individuals who reside in rural American communities are faced with dire circumstances in the fight against coronavirus. Many scientific studies of the impact of the COVID-19 pandemic have focused primarily on urban areas. Only a small number of studies have been dedicated to assessing the impacts of the pandemic on health-related and economic dimensions of rural constituent wellbeing [4]. Notably, the effects of the COVID-19 pandemic on rural populations have been devastatingly disproportionate. Rural Americans comprise of approximately 19% of the US population [5]. Recent statistics report that rural Americans are dying of COVID-19 at more than twice the rate of their urban counterparts [6]. During the second coronavirus surge of summer 2020, COVID-19 related incidence and mortality rates of rural communities began to surpass those of urban communities [7]. Those rates have continued to increase with peaks in January of 2021 and Since the start of the pandemic, approximately 1 in 434 rural Americans have died of COVID-19 [8]. This includes a significant amount of Native American, Black, and Hispanic people who reside within these areas [6]. Despite, higher COVID-19 incidence rates and lower vaccination rates, the disproportionate impact among rural Americans is better explained by preexisting circumstances that made this population more susceptible to the perils of the COVID-19 pandemic [6]. Furthermore, Minorities who reside in rural areas experience many social inequities and health disparities which subject them to higher rates of psychological distress, unresolved physical ailments, and limited access to healthcare providers [9]. These experiences are also compounded by poverty, discrimination, and disproportionate exposure to trauma and stress [9]. When considering youth of color, the impact of the disparities is far greater. To fully understand the impact of the pandemic on rural populations, it is necessary to closely examine how health disparities generally impact minorities in rural America. Then a closer examination of rural youth health disparities will be undertaken. This section will be followed by a brief overview of mental health disparities and rural youth of color.
Understanding Health Disparities in Rural America
Over 700,000 Americans have now succumbed to COVID-19 [7]. Deaths in the United States have been disproportionately high among Hispanic, Black, and Indigenous communities in rural areas [7]. According to the Centers for Disease Control and Prevention [10], Hispanic, Indigenous, and Black people are twice as likely to die of COVID-19 in comparison to their white counterparts. Black people have died from COVID at almost the same rate as white people who are more than one decade older [11]. Furthermore, Black and Latino males have experienced a decline of approximately three years in life expectancy [12].
There are many rural risk factors for health disparities. The Rural Health Information Hub (RHIH) website identified such risk factors as geographic isolation, hospital closures, lower socioeconomic status, higher rates of health risk behaviors, limited access to healthcare specialists and subspecialists, and limited job opportunities [13] to be responsible for wider health disparities. Additionally, individuals who reside in rural areas are also likely to have higher incidence of disease and/or disability, increased mortality rates, and higher rates of pain and suffering [13]. Personal histories of adverse childhood experiences (ACEs) further complicate outcomes, for research has consistently linked childhood trauma and adult well being [14]. ACEs include exposure to trauma, parent mental health difficulties, family dysfunction, and community level adversities that increase an individual’s risk for negative health outcomes [15]. Negative health outcomes can be detrimental to the lives of under resourced individuals who reside in rural areas.
Unfortunately, America’s well-established history of racial discrimination and segregation has directly influenced the inequities that persist in the healthcare system [7,16]. Prior to the start of the global pandemic, health disparities were rampant among minorities in the United States in the areas of disease, disability, and mortality. All these areas are largely influenced by various social determinants of health. A closer examination of rural youth health disparities provides insights on the impact of COVID-19 and overall youth well being in rural areas.
Rural Youth and Health Disparities
Youth who reside in rural areas are likely to experience worse health related outcomes in comparison to their urban counterparts [17]. Rural American population is comprised approximately of 11.8 million children and adolescents of various racial ethnicities [17]. Roughly 24 percent of rural children lived in poverty in 2016. This number is growing as COVID-19 has further exacerbated economic conditions in rural communities. On the other hand, economic hardship in rural communities can also be attributed to declining population, limited employment opportunities, and insufficient industry developments [17]. Higher poverty rates are also consistently attributed to low employment, low education, delayed immunizations, and high delinquency rates in adolescence [17].
In addition to harsher economic conditions, children who live in rural areas are also more likely to succumb to injury [17]. Research as pointed to environmental factors as significant contributors to child injury in rural communities. For example, car accidents are more likely to be fatal in rural areas due to lower-quality road design and greater distances to hospital care. Agricultural and unintentional firearm discharge accidents have also claimed the lives of children in rural areas. Finally, because rural communities have lower levels of prevention behavior, children in rural communities often sustain injuries due to matters such as lack of seatbelt use and water safety practices.
Children who live in rural areas are more likely than urban children to be exposed in utero to maternal smoking and are also likely to be born to teen mothers [17]. Rural children are also more likely to have gaps in health care as rural parents are less likely to report their child has had a preventative health care or oral health care visit. Lack of preventative visits has been linked to insurance coverage, provider workforce shortages, and transportation difficulties [17]. Although many rural children are eligible for federal Medicaid, Hispanic children are least likely to be insured in comparison to their non-Hispanic peers.
Despite limited access to healthcare, there are still noticeable disparities between rural children with public and private insurance due to barriers and unmet health needs. Such barriers include but not limited to difficulty in getting scheduled appointments, locating general clinicians, and finding a provider who will accept a particular Medicaid plan [17]. Sometimes, individuals who live in rural areas with private insurance can experience barriers to access due to provider plan participation and plan limitations. Plan limitations can be problematic when it comes to adequate mental healthcare because limitations can contribute to treatment issues [18]. To understand the impact of COVID-19 on rural youth mental health disparities, it is important to examine preexisting issues in rural that impact the mental health of youth and their families. A clearer understanding of rural mental health provides contextual base for the composite narrative of resilience of rural African American youth, their families, and the mental health practitioners who assist those families.
Youth Mental Health Disparities
Persistent disparities exist in the rates, severity, and outcomes of mental illness in rural America. The rate of incidence of mental, behavioral, and developmental disorders is higher among rural children [17]. As with health disparities, generally, African American, Native American, Asian American, and Hispanic/Latinx Americans have experienced disproportionate rates of mental health burden [19]. Minorities typically experience greater rates of major depression and externalizing behaviors [19]. Suicide rates among rural youth are also problematic, for youth who reside in many rural areas are approximately double that rage of urban youth [20]. Extant literature also points to disparities in a range of outcomes for LGBTQIA+ youth who reside in rural areas [21].
Mental health related issues prevalent in rural America include lack of access to psychologists and psychiatrists, inadequate training of mental health professionals in the needs of rural constituents, and high rate of turnover in mental health professionals [22,18]. One additional problem that rural children and their families face pertains to mental health literacy. Many individuals who live in rural areas often do not understand how to appropriately identify and address mental health concerns [23]. Additional issues can occur with telehealth services, for if individuals and their families do not have adequate access to internet services, they may be unable to take advantage of this modality for service care delivery [17]. Although there are many issues that exist which complicate mental health service delivery and access for rural youth and their families, the resolution of such issues is not an easy undertaking. Cultural determinism provides a framework from which one can understand health disparities as they impact the lived experiences of rural youth and their families. A better understanding of the impact of health disparities can lead to the development of better processes and interventions that help to equip professionals as they work with this population.
Cultural Determinism: A Framework for understanding Health Disparities
Cultural determinism is a social science theory that posits cultural differences as the reason for societal differences [24]. Cultural determinism is based on the premise that individual and group characteristics are created by a given society’s economic, political, and religious organization [25]. In a general sense, cultural determinism is the notion that suggests that differences in health outcomes are the result of variances in cultural backgrounds and life choices [26]. Cultural determinism is used as a guiding theoretical framework for contextualizing the experiences of African American youth and their families as they navigate the rugged landscape of healthcare from their rural communities. In relation to mental health, cultural determinism defines mental illness as a culturally constructed term whereby (1) there are specific variables that cause mental disorders (2) there is an explanation for the causal relevance of variables that contribute to the development of mental disorders and (3) there are culturally based explanations with accompanying processes and mechanisms that produce putative psychological effects [24].
There is well established research that identifies issues that influence mental health services for people who live in rural America. When considering the factors that contribute to health disparities, all the previously noted conditions are applicable, for a myriad of culturally and socially sanctioned factors contribute to the persistence of these ailments. In the case of rural youth, the mechanisms and processes that contribute to the psychological distress experienced by rural African American youth and their families can largely be attributed to preexisting impoverished living conditions which are shaped historically and structurally by socioeconomic and environmental disadvantages [19]. For rural youth and their families, preexisting disparities worsened during the COVID-19 pandemic and continue to persist [19]. This was especially true for African Americans who witnessed and participated in protests across the country in the name of justice and equality. Furthermore, because mental health diagnoses and related pathologies are very much engrained in cultural definitions of abnormality and impairment, it is very important to look at the various ways that social constructions contribute to the perpetuation of disparities. An examination of the applicability of social justice as an adjunctive framework is warranted to advance the understanding of the lived experiences of rural youth as they relate to physical and mental health disparities.
A Closer Look At Access, Equity,Participation, Harmoney, and Rights
Social justice ideologies offer a framework that allows counselors, educators, and community activists an opportunity to understand the intricacies of oppression, discrimination, marginalized statuses, and health outcomes in a pandemic era. It further provides a framework for preventing harm by identifying the social nuances and processes that perpetuate health disparities in America’s most vulnerable communities [23]. By adopting a social justice framework, professionals will establish a foundation from which they can identify and assess the needs of rural African American youth and their families. There are four principles that professional should focus on to help them better understand how to empower and advocate for the individuals and families that they will service. These principles include equity, access, participation, harmony, and rights [23,27].
Equity concerns fairness and the need for balanced distribution of resources, rights, and responsibilities [28]. In the case of rural African American youth and their families, it is important to understand how the unfair distribution of resources has resulted in underfunding for schools and other important infrastructure developments in rural cities. For example, lack of broadband access during COVID-19 also meant no engagement in remote learning activities for children in rural areas [18]. Subsequently, this meant that African American youth who lived in rural areas were also most likely to be disconnected from their peers and mentors and therefore at a further disadvantage in terms of academic and social/emotional development. To ignore the social milieu that perpetuates social injustice for rural youth and their families in these circumstances is to be complicit and complacent with the social forces that perpetuate inequities.
Access concerns ideals of fairness in terms of individuals being able to reasonably utilize resources, services, power, and information to evoke changes in their lives [28]. Access extends beyond age, gender, and ethnicity and can be thought of as the means that individuals employ to inform and impact changes in their lives. Rural African American youth and their families should be afforded the same access to educational systems, safe roads, hospitals, mental health practitioners, and educational systems that their rural counterparts can access. This means that rural African American youth and their families should be offered the resources necessary for influencing how they interact with local educational and health systems to receive the educational support and healthcare needed to enjoy positive outcomes.
The principle of participation concerns the act of individuals being afforded the opportunity to participate in decision making processes that impact their lives as well as the lives of individuals in similar contexts and circumstances [28]. Participation is often largely impacted by access and perceptions of equity. For example, individuals who reside in rural areas are not always extended opportunities to participate in decision making around hospital closures or schools because they often do not have access to information to participate, or they may feel powerless in the decision-making process. This is often interpreted as a lack of interest, but is most likely reflective of internalized oppression, helplessness, and mistrust due to past and present encounters with institutional barriers and racism.
Harmony refers to social-justice-orientated actions that produce results in the prime interest of common good; e.g. participation rights refer to the way in which individual liberties are exercised in gaining knowledge about circumstances and decisions affecting people as well as one’s rights to appeal unfair decisions [27]. When seeking harmony in working on behalf of rural African American youth and their families, it is necessary to understand their perceptions of their rights and what that means in terms of the power they can exercise to impact decisions that affect their lives and the lives of others in their communities. Special emphasis is placed on the ways in which these principles are enacted by individuals and those who identify as members and advocates of the rural community.
Engaging Rural African American Families To Foster Youth Resilience
To improve resiliencies and outcomes for rural youth and their families, it is important to encourage engagement through the creation of positive experiences. Additionally, it is necessary to initiate locally driven approaches that can help fill gaps where other resources have failed by employing the actions of individuals who identify as members of the community. For rural African Americans, individuals who identify as belonging to the community are more likely to be trusted in the role of advocate or vested individual [29]. Furthermore, this idea permeates color lines as rural America is economically and rurally diverse [17,30]. The proposed model offers a four-tiered approach to engagement of rural African American youth, families, and members of the community (see Figure 1). Social justice principles influence each tier of the model as the principles of participation, access, harmony, rights, and equity are used to inform the actions of educators and practitioners as they interact with individuals and families. The E.S.S.I. Model of Engagement utilizes strategies proposed by Stanford scholars Chavez-Dueñas and Adames [31] for engaging communities of color in health initiatives. These strategies include empathy-building, self-awareness, and skill development. The authors of this chapter propose the steps as a tiered model with one additional tier involving involvement and dissemination.
Tier one synthesizes knowledge about culture, racism, and history and the way in which these things impact the lives or rural African American youth and their families. The emphasis at this tier also relates to efforts of practitioners and educators at understanding universal and culturally specific factors that contribute to hesitancy to engage and interact with social institutions. At this tier, the focus is on the establishment of rapport and trustworthiness. Here practitioners should focus on appreciating client world views and life experiences.
Tier two is reserved for self-reflective activities that enhance practitioner and educator awareness of self in relation to their attitudes, biases, prejudices, privileges, etc. Activities in this tier should be aimed at gaining awareness of the cultural and racialized experiences of persons of color and how that is situated in the rural experience Efforts within this tier may also reflect additional training in multicultural and social justice competencies. Tier three relates to the promotion of co-learning and capacity building among all parties involved through the establishment of partnerships and training programs. Tier four encompasses the ongoing synthesis, exchange, and application of knowledge by stakeholders, educators, and practitioners [31].
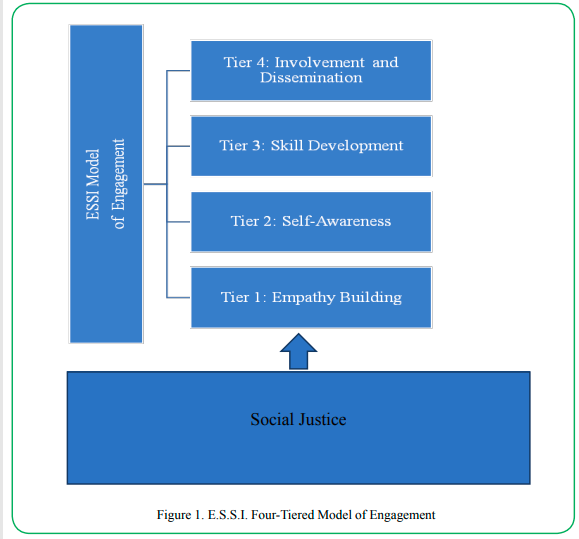
Figure 1. E.S.S.I. Four-Tiered Model of Engagement
E.S.S.I. Model of Engagement in Action: A Phenomenological Undertaking
The next section focuses on the implementation of the E.S.S.I. model while working in the capacity of a mental health professional with two African American individuals who reside in rural communities. The highlights of these individuals’ experiences are representative of a youth and parent. Semi-structured interviews were used to explore and gather information about the experiences of these individuals as well as to learn about their perceptions of mental health professionals’ efforts at engaging and fostering resiliencies during the COVID-19 pandemic.
A modified phenomenological interview approach was utilized to gather information about the lived experience of a guardian and youth in Peachgrove, a fictitious named used to reference two rural communities in Southeastern United States. The phenomenological interview, as proposed by Siedman (2006), is based on Schutz’s interpretation of Husserl’s [32] phenomenology. On the basis of this approach, the three interviews were consolidated into one as the purpose of the interview was not to conduct research but was rather to formulate an analysis of the experience with a superimposed structure. Interviews were completed with Ms. Evans, a single African American mother of two African American teenagers and Edwin, a 16-year-old African American male. Both are recipients of mental health services and have been assigned pseudonyms to protect their identities.
The areas of focus for the facilitated interview included focused life history, reconstruction of the experience, and reflection of meaning on the experience. Sample questions from the interview protocol can be found in Table 1. The questions were developed using current literature pertaining to rural health disparities and the COVID-19 pandemic. An abbreviated version of reflexive thematic analysis was utilized to identify preliminary themes from the interviews given the limited amount of data. Three broad themes were identified. These themes included: (1) Desensitization to resource limitations (2) Disparaging mental health experiences and (3) Idealized support.
Desensitization to resource limitations not only speaks to the preexisting nature of problems with access and participation in healthcare, but it also speaks to the resiliencies of youth and their families to overcome barriers to mental health systems. Ms. Evans mentioned repeatedly how difficult it had been for her prior to COVID-19 to gain access to adequate long-term mental health care for her daughter who had been hospitalized over 17 times in the past two years. Although Ms. Evans recognized that the COVID-19 pandemic had posed additional barriers by increasing the waiting time for appointments and institutionalization, she did not see such barriers as inherently different from those she had experienced prior to the COVID-19 pandemic. Ms. Evans longed for more appropriate support to address the long-term mental health needs of her daughter. Similarly, Edwin, who resides in a city with no African American therapists and only one therapist overall, had waited years to schedule an appointment with a therapist in another city. He explained that he realized that it was “the norm” for him to not have an opportunity to work with a counselor of color in his rural community. When applying the E.S.S.I. model of engagement to these circumstances, educators and practitioners may be successful when enacting Tier 1 and Tier 2 interventions, for the experiences of Ms. Evans and Edwin warrant a level of empathy that is reflective of a sincere understanding of their frustrations and circumstances in a culturally sensitive, person-centered way
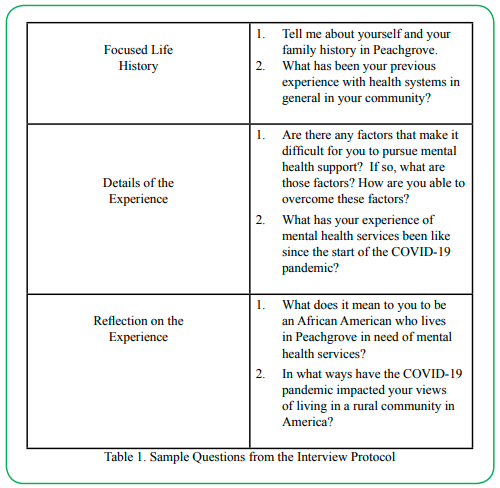
Table 1. Sample Questions from the Interview Protocol
Disparaging mental health experiences reflects the negative experiences of the individuals throughout the course of their varied interactions and efforts at attempting to gain access to needed services. For example, Edwin spoke at length about how he was referred to a mental health provider who abruptly stopped providing services in his rural community at a time where he had contemplated suicide and had made several homicidal gestures towards his guardian. When working with individuals who present in similar circumstances like Edwin in communities and schools, it is essential to begin work in Tiers 3 and 4 of the engagement model because Edwin’s needs are beyond those of awareness and require a much more intentional effort at gathering resources for support of a clearly developed need.
The final theme, Idealized support, targets primary efforts out of Tier 4, but may also call for efforts in others tiers as well. Ms. Evans struggled with finding support for her daughter due to her status in the community as a leader. Although the services needed by her daughter were offered in her rural community, her daughter’s service needs at elevated to a level of care that required her to reach out beyond her rural community. Furthermore, her status in the community complicated her outreach process because she had social and or business affiliations with many of the practitioners in the neighboring urban community. She ultimately had to find a provider who was 45 minutes away from her home. While Ms. Evans’ circumstances are rare in that she had access to resources she could utilize, it was not always easy for her to identify and utilize those resources once they were identified. She had to wrestle with meeting her daughter’s mental health needs while also maintaining her identity as a high-profile professional in her community. In this case, intervention from any of the tiers would have been beneficial, but perhaps not welcomed.
Conclusions
The COVID-19 pandemic posed a challenge in many ways to rural youth of color. Although alarming numbers of people of color continue to be disproportionately impacted by the COVID-19 pandemic, there is an even larger number or rural persons of color impacted by the COVID-19 pandemic. For many, the existence of the COVID-19 pandemic has exacerbated already dire conditions in health and educational systems. Social justice and cultural determinism frameworks can help practitioners and educators better contextualize those experiences. Additionally, the E.S.S.I. model of engagement can help with approaches that can be used to foster resiliencies in rural youth and families of color.
Competing interests:
The authors declare that they have no competing interests.
References
World Health Organization. (2022). Global research on coronavirus disease (COVID-19).https://www.who.int/ emergencies/diseases/novel-coronavirus-2019/global-research-on-novel-coronavirus-2019-ncov. View
Our World in Data. (2022). Coronavirus (COVID-19). Retrieved from Coronavirus (COVID-19) - Google NewsView
U.S. Census Bureau (n.d.). How does the US census bureau define “rural?” (n.d.) Retrieved from https://mtgisportal.geo. census.gov/arcgis/apps/MapSeries/index.html?appid=49cd4bc 9c8eb444ab51218c1d5001ef6
Mueller, J.T., McConnell, K., Burow, P.B, Pofahl, K., Merdjanoff, A.A., & Farrell, J. (2021). Impacts of the covid-19 pandemic on rural America. Proceedings of the National Academy of Sciences of the United States of America, 118(1), 1-6. https://doi.org/10.1073/pnas.2019378118. View
U.S. Census Bureau. (2010). American FactFinder. Retrieved from http://factfinder.census.gov/servlet/ DCGeoSelectServlet?ds_name=DEC_2000_SF1_UView
Weber, L. (2021, September 30). Covid is killing rural americans at twice the rate of urbanites. Retrieved from https://khn.org/ news/article/covid-death-rate-rural-america/View
McKeever, A. (2021, October 1). 700,000 Americans now dead from covid-19-but deaths reveal deep disparities. National Geographic. Retrieved from https://www.nationalgeographic. com/science/article/700000-americans-now-dead-from-covid-19-but-deaths-reveal-deep-disparitiesView
CUllrich, F. & Mueller, K. (2022). Covid-19 cases and deaths, metropolitan and nonmetropolitan counties over time (update). RUPRI Center for Rural Health Policy Analysis: Rural Data Brief. Retrieved from https://rupri.public-health.uiowa.edu/ publications/policybriefs/2020/COVID%20Longitudinal%20 Data.pdfView
Goodkind, J.R., Bybee, D., Hess, J., Amer, S., Ndayisenga, M., Greene, R.N., Choe, R., Isakson, B., Baca, B., & Pannah, M. (2020). Randomized controlled trial of a multilevel intervention to address social determinants of refugee mental health. American Journal of Community Psychology, (65), 272-289 doi 10.1002/ajcp.12418. View
Centers for Diseases Control and Prevention (2021). Risk for COVID-19 infection, hospitalization, and death by race/ethnicity. Retrieved from https://www.cdc.gov/coronavirus/2019-ncov/ covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.htmlView
Ford, T., Reber, S., & Reeves, R.V. (2020, June 16). Race gaps in covid-19 deaths are even bigger than they appear. Retrieved from https://www.brookings.edu/blog/up-front/2020/06/16/ race-gaps-in-covid-19-deaths-are-even-bigger-than-they-appear/View
Perry, A., Shiro, A., Barr, A., & Romer, C. (2021, October 11). Amid the pandemic, Black and Latino men have experienced the largest drop in life expectancy. Retrieved from https://www. brookings.edu/research/amid-the-pandemic-black-and-latino-men-have-experienced-the-largest-drop-in-life-expectancy/View
The Rural Health Information Hub (2019). Rural Health Disparities. Retrieved from https://www.ruralhealthinfo.org/ topics/rural-health-disparitiesView
National Advisory Committee on Rural Health and Human Services (2018). Exploring the rural context for adverse childhood experiences (ACEs) (Policy Brief and Recommendations). Retrieved from: https://files.eric.ed.gov/fulltext/ED591840.pdfView
Woods-Jaeger, B., Briggs, E., Gaylord-Harden, N., Cho, B., & Lemon, E. (2021). Translating cultural assets research into action to mitigate adverse childhood experience-related health disparities among African American youth. American Psychologist, 76(2), pp. 326-336. https://doi.org/10.1037/ amp0000779. View
Murty, K.S., & Payne, T.B. (2021). Pandemics of COVID-19 and racism: How HBCUs are coping. AIMS Public Health 8(2), 333-351, 2021. Doi:10.3934/publichealth.2021026. View
Hung, P., Workman, M., & Mohan, K. (2020). Overview of rural childhealth. Retrieved fromhttps://www.ruralhealth.us/NRHA/ media/Emerge_NRHA/Advocacy/Policy%20documents/2020- NRHA-Policy-Document-Overview-of-Rural-Child-Health.pdfView
Summers-Gabr, N. M. (2020). Rural–urban mental health disparities in the United States during COVID-19.Psychological Trauma: Theory, Research, Practice, and Policy, 12(S1), S222– S224. https://doi.org/10.1037/tra0000871View
Valdez, C., Guidino, O., Cort, N., Rodgers, C., Isaac, P., & Casas, M. (2019). Translatingresearch to support practitioners in addressing disparities in child and adolescent mental health and services in the united states. Cultural Diversity and Ethnic Minority Psychology, 25(1), pp- 126-135. http://dx.doi. org/10.1037/cdp0000257.
Bailey, S., Oosterhoff, B., Lindow, J., Robecker, T., Bryan, B., & Byerly, M. (2021). Feasibility, acceptability, and fidelity: Extension agents teaching youth aware of mental health. Journal of Rural Mental Health, pp 1-12. https://doi.org/10.1037/ rmh0000170.View
Hatzenbuehler, M. (2017). Advancing research on structural stigma and sexual orientation disparities in mental health among youth. Journal of Clinical Child & Adolescent Psychology, 46(3), pp. 463-475. Doi: 10.1080/15374416.2016.1247360. View
Smalley, K.B. ,Warren, J.C., & Rainer, J.P. (2012). Rural mental health : Issues, policies, and best practices. New York: Springer Publishing Company.View
Crumb, L., Haskins, N., & Brown, S. (2019). Integrating social justice advocacy into mental health counseling in rural, impoverished American communities. The Professional Counselor, 9(1), pp.20-34. Retrieved from http://tpcjournal. nbcc.org. doi:10.15241/1c.9.1.20.View
Spiro, M. (2001). Cultural determinism, cultural relativism, and the comparative study of psychopathology. Ethos, 29(2), pp. 218–34, https://doi.org/10.2307/640637.View
VandenBos, G. R. (Ed.). (2007). APA Dictionary of Psychology. American Psychological Association.View
Shim, R.S., & Vison, S. (2021, March 29). To achieve mental health equity dismantle social injustice. Retrieved from https:// www.scientificamerican.com/article/to-achieve-mental-health-equity-dismantle-social-injustice/View
Health and Community Services Workforce Council (n.d.). “Fact sheet: Social justice and health” Retrieved from https:// www.checkup.org.au/icms_docs/182820_15_FACTSHEET_ Social_Justice_and_Health.pdfView
Crethar, H.C. & Ratts, M. (2008). Why social justice is a counseling concern. Retrieved from https://www.resesarchgate. net/publication/264847712View
Sankaré, I. C., Bross, R., Brown, A. F., Del Pino, H. E., Jones, L. F., Morris, D. M., Porter, C.,Lucas-Wright, A., Vargas, R., Forge, N., Norris, K. C., & Kahn, K. L. (2015). Strategies to Build Trust and Recruit African American and Latino Community Residents for Health Research: A Cohort Study. Clinical and translational science, 8(5), 412–420. https://doi.org/10.1111/ cts.12273View
Probst, J., Barker, J., Enders, A., & Gardner, P. (2016). Current state of child health in rural America: How context shapes children’s health. The Journal of Rural Health, pp 1-16. doi: 10.1111/jrh.12222.View
Chavez-Dueñas, N. Y. & Adames, H. Y., (2015). Building Trust with Communities of Color. Stanford Social Innovation Review. https://doi.org/10.48558/TASV-CW82View
Husserl, E. (1970). Logical investigations (Vol. 1 & 2). London: Routledge.View