
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 6 (2022), Article ID: JPHIP-208
https://doi.org/10.33790/jphip1100208Research Article
Elimination of Neonatal Tetanus in Rural Central African Republic: Issues and Challenges
Longo Jean De Dieu1,2, Woromogo Sylvain Honore2,3*, Diemer Henri Saint Calvaire1,2, Niamate Lemotomo Christelle1, Fandema Emmanuel2, Tekpa Gaspard4 , & Gresenguet Gerard1,2
1National Reference Centre for Sexually Transmitted Diseases and Antiretroviral Therapy, Bangui, Central African Republic
2Department of Public Health, Faculty of Health Sciences, Bangui, Central Africa Republic
3InterState Centre for Higher Public Health Education in Central Africa (CIESPAC), Brazzaville, Congo.
4Infectious and Tropical Diseases Services University Hospital of Friendship, Central African Republic
Corresponding Author Details: Sylvain Honore Woromogo, MD, MPH, Department of Public Health, Faculty of Health Sciences, Bangui, Central Africa Republic.
Received date: 07th June, 2022
Accepted date: 21st July, 2022
Published date: 23rd July, 2022
Citation: De Dieu, L.J., Honore, W.S., Calvaire, D.H.S., Christelle, N.L., Emmanuel, F., Gaspard, T., & Gerard, G., (2022). Elimination of Neonatal Tetanus in Rural Central African Republic: Issues and Challenges. J Pub Health Issue Pract 6(2): 208.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Like other countries in the world, the Central African Republic is committed to the fight against the elimination of neonatal tetanus (NNT). Despite the efforts made, the number of NNT cases continues to grow. The objective of this work was to describe the epidemiological profile and identify the risk factors for the occurrence of NNT in rural Central African areas in order to improve control strategies in this context. This was a case-control study of newborns with tetanus (case) or not (controls), conducted between 2014 and 2019 at the Gazi Secondary Health Center. A questionnaire collected socio-demographic and clinical data that were entered and analyzed using the Epi info 7 software. Multiple logistic regression used to establish the relationship between the occurrence of tetanus and the characteristics of the mother and the newborn, through the ORs and their 95% CI. A total of 332 newborns were included, including 166 cases of NNT and 166 controls. The average age was 7.8 ±3.6 days. The incidence of NNT was 2.7 and 5.2 cases per 1000 live births in 2014 and 2019 respectively. The main risk factors for NNT were new males (p=0.04), low maternal education (p=0.001), separation from health care (p=0.006), primiparity (p<0.001), low number of antenatal visits (p<0.003) and low tetanus vaccine coverage (p<0.001). According to newborn care practices: home birth (p=0.002), delivery by unskilled personnel (p<0.001), umbilical cord septic section (p<0.001), no cord dressing (p<0.001) and septic dressing (p=0.012) were statistically associated with the occurrence of NNT in our context. In rural Central African Africa, the incidence of neonatal tetanus remains high and the risk factors are multiple. Effective health promotion measures can contribute to the elimination of this disease.
Keywords: Neonatal tetanus, epidemiology, rural environment, Central African Republic
Introduction
Tetanus is a non-communicable infectious disease caused by the action of a toxin secreted by the telluric bacillus called Clostridium tetani, which occurs naturally in the soil and feces of animals. A notifiable and eliminated disease in many countries around the world, tetanus remains a serious public health problem in developing countries. Being included in the fourth Millennium Development Goal (MDG) for elimination by 2015, a decision taken at the World Health Assembly in 1989 and updated in 2001, NNT is not eliminated in many countries, especially in sub-Saharan Africa. According to the World Health Organization (WHO), the number of cases recorded annually worldwide varies between 700,000 and 1 million, of which neonatal tetanus (NNT) is the most observed form [1-4]. It is considered eliminated in a country when there is less than one case per year per 1000 live births in the country. To move towards the elimination of NNT, WHO recommended to countries to ensure national vaccination coverage for at least two doses of tetanus Vaccine (TTCV 2+) greater than or equal to 80%, to promote hygiene during childbirth and finally to ensure good epidemiological surveillance [1,5,6].
The Central African Republic (CAR), a country with limited resources, has a vaccination coverage in TTCV2+ that has increased from 50% in 2000 to 63% in 2016, of which 47% in rural areas. Among the problems that maintain this low vaccinal coverage is insecurity [6-9]. This work was carried out on the assumption that the incidence of NNT is still high in rural Central African Republic and the causes of occurrence will be multifactorial. Thus, the objective of this work was to describe the epidemiological profile and identify the risk factors for the occurrence of NNT in rural areas in order to improve control strategies in this context.
Methods
Type of study
This was a case-control study, running from January 1, 2014 to December 31st, 2019 and carried out in the paediatric facility of the Gazi Secondary Health Centre, located about 500 miles in the south-west of CAR. Outlying locality and difficult access.
Study population and sampling
The study population consisted of any newborn (from birth to 28 days), hospitalized during the study period. Sampling was exhaustive taking all cases of neonatal tetanus admitted to hospital during the study period, with a proportion of one case to a control. Controls were selected by simple random draw from medical records.
The cases were newborns with tetanus according to WHO criteria that define neonatal tetanus as a disease occurring in a newborn who normally cries and sucks during the first two days of life, but loses this ability between the third and twenty-eighth day of life and becomes stiff or has spasms (1). The controls were newborns who were followed in hospital during the same period of the study and who had not shown clinical signs suggestive of tetanus.
Variables and data collection
The dependent variable was the occurrence of neonatal tetanus and the independent variables were the characteristics of newborns (sex, age) and mothers (age, marital status, residence, level of education, occupation, parity, number of Antenatal Consultations (ANC) and number of doses of TTCV received, care practices related to childbirth (place of delivery, the mode of section and dressing of the umbilical cord, the qualification of the birth attendant) and the evolution of NNT. The information was collected using an anonymous data collection sheet from the medical records.
Data analysis
Text and table entry was done on Word and Excel 2016 software and data analysis was done with EpiInfo 7.2 softwares. For the comparison of proportions, we used the chi-square test at the significance threshold of 5%. The incidence of neonatal tetanus was assessed using the following formula: annual incidence of NNT = (number of NNT cases/number of live births) x1000.
The Chi-square and Wald tests were used as well as the odds ratio with their 95% confidence interval at the 5% threshold. Multiple logistic regression was used to establish the relationship between socio demographic, newborn characteristics and the occurrence of NNT. Multivariable logistic regression analyses with backward elimination stepwise selection with p < 0.20 were used to identify baseline explication that predicts NNT.
Ethical considerations
The study was conducted in accordance with the Good Clinical Practices (GCP) guidelines and the regulations of the Ministry of Public Health and Population. The study was approved by the Ethics Committee of the University of Bangui, Faculty of Health Sciences, Central African Republic. The survey was granted clearance N°17/ UB/FACSS/2016. The retrospective nature of the study did not allow us to apply an informed consent form. Thus, we decided to make each form anonymous before processing them.
Results
General characteristics of the study population
A total of 332 newborns were included, divided into 166 cases and 166 controls. There were 154 boys (46.4%) giving a sex ratio of 0.8. The mean age was 7.8 days (±3.6) in cases and 5.3 days (±4.7) in controls. Childbirth took place at home in 79.2% of cases. This frequency was 100% for newborns with neonatal tetanus compared to 58.4% for controls. The average age of mothers in our series was 21 years with extremes ranging from 14-40 years. The average age of mothers in cases was 23 years (±6) versus 23 years (±5) for mothers of controls. Adolescent and young mothers (under 25 years of age) accounted for 67.2%, with proportions of 71.1% and 63.3%, respectively among cases and controls. About four out of five women (79.8%) were housewives, followed by students (9.3%) and women traders (6.3%). In 70.5% of cases, mothers were not in school. They resided in 48.8% of cases more than 10 km from the health center. The proportion of mothers who had benefited from at least two “Number of Prenatal Consultation” (NPCs) was 2.4% in the cases compared to 10.2% for the controls. Overall, the mothers were primiparous (64.8%), of which 75.3% were in the cases and 54.2% in the controls.
Evolution of the annual incidence of neonatal tetanus
Between 1 January 2014 and 30 December 2019, the incidence of neonatal tetanus increased from 2.7 annual cases in 2014 to 5.19 cases per 1000 live births in 2019 (Figure 1).
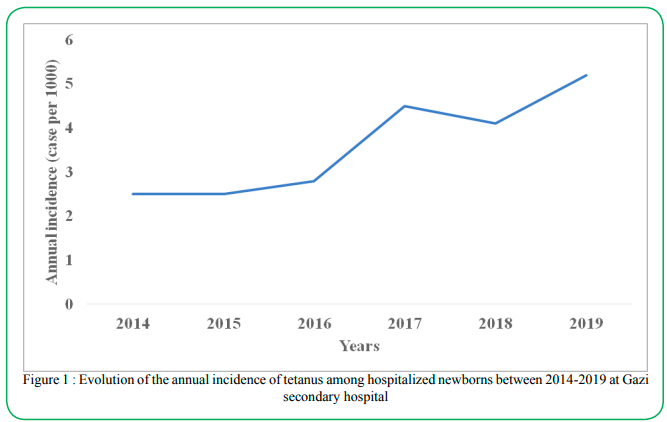
Figure 1 : Evolution of the annual incidence of tetanus among hospitalized newborns between 2014-2019 at Gazi secondary hospital
Risk factors for neonatal tetanus
The occurrence of neonatal tetanus is not related to the characteristics of newborns (sex, birth weight) but rather to those of mothers (Table 1). In univariate analysis, the factors significantly associated with the occurrence of NNT were male newborns, maternal age less than 30 years, primiparity, number of NPCs less than 2, number of tetanus vaccine doses less than 2, lack of schooling mothers, the place of residence more than 10 miles from the maternity facility, and care practices (home birth, delivery by an unqualified person, section of the umbilical cord with septic equipment, absence of dressing of the umbilical cord).
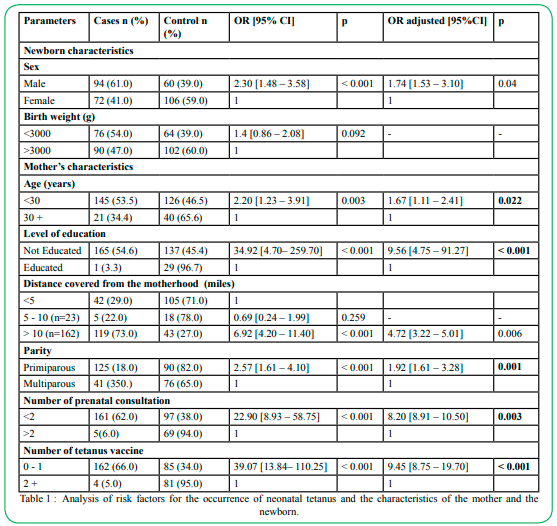
Table 1 : Analysis of risk factors for the occurrence of neonatal tetanus and the characteristics of the mother and the newborn.
Thus, neonatal tetanus occurred much more in children from mothers under 30 years of age than in those from mothers over 30 years of age [ORa = 1.67; 1.11 – 2.41, p = 0.022], in newborns from out-of-school mothers [ORa = 9.56; 4.75 – 91.27, p < 0.001] than in those from school mothers, in newborns from mothers living more than 10 miles from the maternity facility than in those from mothers who live less than 10 miles away, in newborns from mothers who received less than 2 doses of tetanus vaccine than in those from mothers who received more than 2 doses of tetanus vaccine (ORa = 4.72; 3.22 – 5.01, p < 0.006; ORa = 9.45; 8.75 – 19.70, p < 10-3 respectively). It is the same for newborns from primiparous mothers compared to multiparous mothers and newborns from mothers with less than 2 prenatal consultations compared to mothers with more than 3 prenatal consultations.
In connection with childbirth practices in this city in the Central African Republic, neonatal tetanus occurred much more in home-born children than in those born in the maternity facility (ORa = 9.9; 8.71 – 11.02, p = 0.002). Thus, the same thing was observed when delivery is performed by unqualified personnel compared to delivery performed by skilled personnel, when the umbilical cord is severed in a non-sterile manner compared to the sterile section of the umbilical cord and when the umbilical cord has no bandage or has a non-sterile bandage compared to an umbilical cord with sterile bandage (ORa = 4.1, 5.6 – 6.32 ; p < 10-3; ORa = 11.0, 8.60 – 15.1, p < 10-3 ; ORa = 8.9; 6.44 – 9.35, p < 10-3 respectively), Table 2.
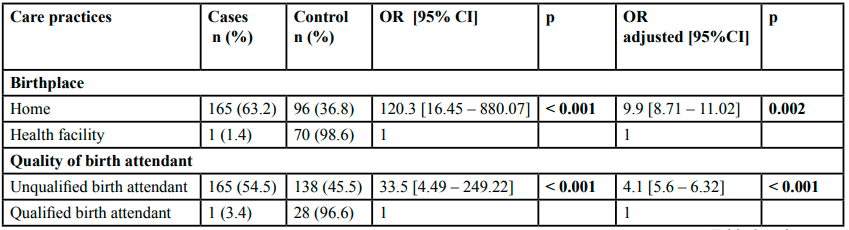
Table 2 : Analysis of risk factors related to childbirth care practices and the occurrence of neonatal tetanus.
Discussion
From the limit of our work
The study involved only one district secondary hospital in rural areas. There is no way to extrapolate the results to the national level. The remote location and difficult access of this district secondary hospital could partly explain this high prevalence of the disease.
The relevance of this study
Data on the frequency of newborn tetanus are scarcely available in the Central African context. Often cases of neonatal tetanus are reported as part of the health information system without a precise description. Through this work, we were able to use data from a district secondary hospital in rural areas to assess the incidence of the disease and the various factors associated with its occurrence.
The magnitude of NNT
The analysis of our results show that tetanus remains a frequent pathology of the newborn in rural Central African areas. Its incidence is still well above the elimination threshold of the disease as set by the WHO [1]. With regard to the place of delivery of newborns, all cases of neonatal tetanus were born at home except for one case. This is partly explained by the low health coverage, the lack of information on the importance of giving birth at the maternity ward or by financial difficulties. These results confirm the finding of the 2016 Herams survey, highlighting the inadequacy of functional health structures and coverage of essential services in the Central African Republic [9]. The high rate of home births is reported in the literature in varying proportions depending on the author (56% to 94.3%) [10-14]. However, it was mentioned in a meta-analysis conducted at the University of Lausanne (Switzerland) in 2014 that home birth posed no risk if it was done by a health professional [15]. This underlines the importance of qualified personnel in accompanying the woman during pregnancy until childbirth.
In our series, overall mothers were young, with an average age of 23. However, among the mothers of NNT cases, we found a high proportion of young adolescent girls (67%). This can be explained in part by the precocity of sexual activities in ours, as was highlighted during a national survey [8]. In Burkina Faso, one study reported a higher average age than ours (28.3 years) [16]. In terms of educational attainment, the majority of mothers were not in school (70%). This situation is consistent with the results of the survey carried out in the Central African Republic in 2010, according to which more than half (54%) of women are not in school. According to the same source, low levels of education are considered a risk factor for maternal and infant morbidity and mortality [8].
This study allowed us to determine the values of the annual incidence of NNT in a rural area in the Central African Republic and the hospital frequency of this disease. During this period, the annual incidence of NNT remained high with an increasing increase from 2.70 to 5.18 cases per 1000 live births. The incidence of NNT reported in our study is higher than that described by several authors in Africa or elsewhere [3,10,17-19]. A reservation is needed for the Central African Republic, which has been plagued by multiple recurring crises for several decades, with the consequences of insecurity. Under these conditions, the rural environment of the Central African Republic can be considered a high-risk area for neonatal tetanus. This context is a threat to the implementation of NNT elimination strategies by 2030, enshrined in the Sustainable Development Goals (SDGs) to which the country has subscribed. For this, innovative control strategies must be developed and implemented in order to claim to eliminate NNT by 2030 as recommended by the WHO [20].
Neonatal tetanus risk factors
A large number of risk factors associated with NNT that were related to the characteristics of the newborn, mothers or related to childbirth practices were found.
For the newborn, only male sex was the factor associated with NNT. Male predominance is reported by several authors. Studies conducted in China in 2015, Morocco in 2005 and Senegal in 2013 made the same finding with sex ratios of 2.88, 1.8, and 2.6 [10,13,19] respectively.
For maternal risk factors, the data vary from study to study. In the Chinese study, unlike ours, it is the age over 30 years that is a risk factor, moreover there is no link between parity and the occurrence of NNT [10]. On the other hand, insufficient NPC and low tetanus immunization are two risk factors accepted by several authors [10,13,19]. This result can be explained by a low coverage of health facilities offering ANC, a lack of vaccination practice in advanced strategy, a low level of education, the lack of information and awareness of communities on the risks of occurrence of NNT in the absence of TTCV and especially by insecurity in the country.
The WHO states that short-term immunity is usually achieved 2 to 4 weeks after the second dose of VAT and cannot exceed one year. Immunity is acquired from 3 doses for a total of 5 to 6 depending on the country, in order to guarantee lifelong immunity, a driving force for the prevention and elimination of NNT. A single dose does not protect against NNT [22]. NNT can occur in both rural and urban areas [12,16].
Mothers of children with NNT
Maternal characteristics identified as risk factors were socio-demographic (age less than 30 years, lack of schooling, place of residence beyond 10 miles from maternity), clinical (absence or only one antenatal consultation, number of tetanus vaccinations less than two).
Delivery care for children with NNT
The delivery practices identified as factors associated with NNT were home birth, delivery by an unqualified person, umbilical cord section with septic equipment, and no cord dressing or septic dressing. These practices that promote umbilical wound contamination were predominant in our study. Infection with Clostridium tetani would be made from the umbilical cord stump during cleaning of the newborn or during care in the under-vaccinated mother. Also in our series, a small proportion of patients had benefited from dressing the umbilical wound with mud. Since the bacillus responsible for NNT is in the soil, dressing the cord with the mud would cause the disease to occur. Poor practices related to childbirth and which can expose the newborn to the risk of tetanus are widespread. Their importance varies according to the authors. Studies conducted in Senegal in 2003 and Morocco in 2005 indicate respectively that the dressing was made with traditional products in all cases and a proportion of 35% with soiled material (shea butter, mud ...) [13,22]. According to the literature, cultural practices harmful to the care and treatment of umbilical cord wounds prevalent in Africa may promote the occurrence of neonatal tetanus [1,16,22-24].
Conclusion
This study allowed us to find that the incidence of neonatal tetanus is high in rural Central African areas with multiple and varied risk factors. These factors are essentially maternal and related to poor care practices for the newborn and its mother. Our results suggest the interest of strengthening the vaccination of women of childbearing age, raising awareness among populations about the benefits of vaccination. In addition, particular emphasis should be placed on good practices in obstetric and neonatal care provided in a referral hospital. The starting point remains the organization of quality antenatal care and its accessibility to all pregnant women. To this end, the involvement of communities and the development of differentiated strategies adapted to the context of countries in crisis is crucial.
Fundings : None
Conflicts of interest :
The authors declare no conflict of interest.
Authors’ contributions :
JDDL designed the study, wrote the protocol and text and supervised the data analysis. SHW, JDDL, SCHD, EF, GT and CNL participated in the drafting of the protocol, data analysis and text writing. GG GG coordinated all stages of the research. All authors have read and approved the manuscript and contributed equally.
Acknowledgements :
The authors would like to thank the Ministry of Health of Central African Republic and the staff of Health District of Gadzi
Declarations : Availability of data and materials
The datasets used and analysed during the current study available from the corresponding author on reasonable request. The datasets generated and/or analysed during the current study are not publicly available due to the promise made to women to keep the data confidential when they are questioned, but are available from the corresponding author on reasonable request.
References
WHO, UNICEF, UNFPA. Sustainably eliminating maternal and neonatal tetanus: Strategic Plan 2012-2015. www.who.int MNTE Strategic Plan F. (Accessed July 21, 2017).View
WHO, Unicef Haiti. The Region of the Americas eliminates maternal and neonatal tetanus. Washington, DC, September 20, 2017. https//: www.paho.org. (Accessed January 20, 2019). View
WHO. Validation of the elimination of maternal and neonatal tetanus in Algeria. 25 February 2018. www.aps.dz.santé-science-technologie . (Accessed 2019-02-15). View
Kalaivani A, Raja D, Geetha M. (2017). Elimination of Maternal and Neonatal Tetanus in India: A Triumph Tale. Int J Prev Med; 8:15-7.View
Aba YT, Cissé L, Abalé A K, et al. (2016). Morbidity and mortality of tetanus of newborns and children in the University Hospitals of Abidjan, Côte d'Ivoire (2001-2010). Bull Soc Pathol Exot; 109:172-9View
World Health Organization. Global Vaccine Action Plan Evaluation Report 2018: Strategic Advisory Group of Experts on Immunization. Available at https://apps. Who.int/iri/ handle/10665/27 7487. License: CC BY-NC-SA 3.0 IGO. (Accessed November 10, 2018).
Guerin N. (2003). Maternal and child immunization in developing countries: successes, challenges and new directions. Med Trop; 63:498-505View
Central African Institute of Statistics and Economic and Social Studies (2010). Monitoring the situation of children, women and men. Multiple Indicator Cluster Survey (MICS4).View
WHO. Rapid survey on the estimation of the health needs of populations affected by the crisis in the Central African Republic (Herams) in 2015. 2016 :116p
Zhou Z, Shi Hong A, Xu Yi, et al. (2015). Risk factors of neonatal tetanus in Wenzhou, China: a casecontrol study. WPSAR ;6(3) :28-33View
Mokhtari M, Huon C. Neonatal tetanus. Encycl Méd Chir (Elsevier, Paris), Pédiatrie, 4- 002-R-95, 1999 :4 p.
Randrianjafinimpanana M, Rakotomahefa N, Ratsimbazafy N, et al. (2014). Neonatal tetanus seen in the five University Hospitals of Antananarivo: epidemiological-clinical aspect and risk factor for mortality. Pediatric Archives; 5(21):818-22.
Oulahiane N, Laboudi A, Kabiri M. (2005). Neonatal tetanus: epidemiological, clinical and therapeutic aspects. About 34 cases. J Ped Child; 18:38- 43.View
Tall F, Patrick T, Roisin A, et al. (1991). Risk factors for neonatal tetanus in western Burkina Faso. Case control study. Bull Soc Path; 84:558-61.View
Houndole N, Künzi S, Meyer Y. (2014). Home birth, the controversy: Impact on the blue marine terrain in Lausanne. Haute Ecole de santé Vaud (HESAV) 78p.
WHO (2014). Vaccine-preventable diseases. Annual epidemiological report. Ecdc.europa.eu.AER-2014VPD-FINAL. (Consulted at 21/07/2017).View
Bairwa, M. (2012). India is on the way forward to maternal and neonatal tetanus eliminate. Hum Vaccin Immunother; 8:1129- 31.View
Deguenonvo, L., Diop, S., Diouf, A., et al. (2013). Elimination of maternal and neonatal tetanus in Senegal: evolution of surveillance indicators from 2003 to 2009. Med Sante Trop; 23(1):55-9.View
WHO. Routine immunization coverage worldwide. Weekly epidemiological record; 40(91):537-48.
WHO (2016). Executive Summary: WHO position on tetanus vaccines. Weekly Epidemiological Record 2017; 6(92):53-76.View
Seydi, M., Diop, B.M., Dia, N.M. et al. (2003). Risk factors for neonatal tetanus in Dakar. Pediatric Archives; 33:150-4.View
College of Academics of Infectious and Tropical Diseases (2016). Neonatal tetanus. In Epilly too. Paris, Paragraph plus:468-75.View
Delmont, J., Parola, P. (2005). Newborn tetanus. In Edmond Bernard et al, eds. Medical emergencies in Africa. Paris, estem:459- 66
Gody, J. , Yanza, M. , Mejiozem, O. , NGatimo, V. , Houndjahoué, F. , Sonny, V. , Kakounguere, E. , Anguize, B. , Guénefio, A. , Mbeko, A. , Engoba, M. and Moyen, G. (2021). Neonatal Tetanus at Pediatric Teaching Hospital in Bangui. Open Journal of Pediatrics, 11, 179-188. doi: 10.4236/ojped.2021.112017.View