
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 6 (2022), Article ID: JPHIP-209
https://doi.org/10.33790/jphip1100209Research Article
Improving Life Skills through In School and Out of School Comprehensive Sexuality Education: A Mixed-Methods Evaluation in Four Provinces of Zambia
Dhally M. Menda1,2*, Joseph Zulu3, Mukumbuta Nawa4, Rosemary K. Zimba1, Catherine M. Mulikita1, Jim Mwandia1, Peter Banda1 & Karen Sichinga5
1Department of Health Programs, Churches Health Association of Zambia, Lusaka, Zambia.
2Adjunct Associate Professor of Health Sciences, Chreso University, Lusaka, Zambia.
3Department of Community Health, School of Public Health, University of Zambia, Lusaka, Zambia.
4Department of Biostatistics and Epidemiology, Levy Mwanawasa Medical University, Lusaka, Zambia.
5Executive Director, Churches Health Association of Zambia, Lusaka, Zambia.
*Corresponding Author Details: Dhally M. Menda, Department of Health Programs, Churches Health Association of Zambia, P. O. Box 34511, Lusaka, Zambia.
**Co-Authors: Joseph Zulu, Professor, Department of Public Health, Univeristy of Zambia, PO Box 50110, Lusaka, Zambia.
Received date: 10th June, 2022
Accepted date: 22nd July, 2022
Published date: 25th July, 2022
Citation: Menda, D.M., Zulu, J., Nawa, M., Zimba, R.K., Mulikita, C.M., Mwandia, J., Banda, P., & Sichinga, K., (2022). Improving Life Skills through In School and Out of School Comprehensive Sexuality Education: A Mixed-Methods Evaluation in Four Provinces of Zambia. J Pub Health Issue Pract 6(2): 209.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Introduction
Background: Many countries face several sexual and reproductive health (SRH) challenges, with HIV/ AIDS being one of them, and young people have been greatly affected by HIV [1,2]. It has been suggested that participation in “life skills” education can help reduce HIV related risk behaviours [3]. There have been increased calls for including life skills as a key component of HIV and AIDS education for children and young people [2]. There is a need to ensure that young people develop the life skills relevant to reducing their vulnerability to HIV infection [4,5]. Literature tends to present life skills as a possible solution to several social, gender and general behavioural problems; for example, it is stated that life skills can help trigger political, social and economic participation and help reduce gender inequalities [2]. In addition, life skills are also believed to positively impact deviant social behaviour, crime, and reduction of substance use [6,7].
Specifically for HIV, the literature suggests that life skills may positively contribute towards reducing contracting of HIV by, for example, enhancing negotiation and communication skills which may help the young people negotiate for safer sex by making them openly talk about risky sexual behaviours and how they can be prevented [8,9]. Life skills in HIV programming include reproductive and sexual health such as HIV and AIDS, condoms, communication skills, and information on addressing gender-based violence [4,2]. Positive outcomes from these studies included increased communication skills, improved risk perception, reduced stigmatisation of people living with HIV, decreased gender-based violence and improved positive living attitude [2].
In order to strengthen community response to HIV, the Churches Health Association of Zambia (CHAZ), a local faith-based Non-Governmental Organisation in Zambia, and its partners received funding from the Global Fund to fight AIDS, Tuberculosis and Malaria (GFATM) aimed at improving life skills education. The partner organisations were Kabwe Adventist Family Health Institute (KAFHI), United Church of Zambia (UCZ), Youth Alive Zambia (YAZ), Young Women Christian Association (YWCA), Zambia Interfaith Networking Group on HIV and AIDS (ZINGO) and Forum for African Women Educationist in Zambia (FAWEZA). The organisations have implemented life skills in communities and schools in eight districts in four provinces. CHAZ implemented a new life skills program in Luapula, Northern, Central and Southern Provinces in 2015. A baseline study was conducted to provide the program with tangible information to guide the implementation of the life skills program. In 2018, an end-line study was conducted to evaluate the program's impact in the communities where it was implemented. This article presents achievements and lessons learnt to inform policymakers and future programs in life skills among young people aged 15 – 24.
Methodology
Study design
A participatory and mixed approach was employed using quantitative and qualitative data collection and analysis methods. A Realist Evaluation study design was adopted because it allowed documentation of mechanisms driving change within the target group [10]. This design was suitable for this assignment and appropriate for documenting evidence for the project relevance, effectiveness, learning, scale-up, sustainability and documenting the transformative effect of the project.
Study Settings
The HIV pandemic remains a challenge in Zambia. According to the Zambia Demographic Health Survey 2018 [11], 11.1 percent of adults aged 15-49 are infected with HIV (14.2 percent of women and 7.5 per cent of men) [11]. HIV prevalence among the young people aged 15-24 was 3.8 per cent (5.6 per cent among young women and 1.8 per cent among young men) [11]. In terms of sexual behavioural practices among young people, there is early initiation of sexual intercourse. By the age of 18, more than half have had sexual intercourse. Using condoms during sexual intercourse with non-marital and non-cohabiting partners is not high, i.e. 35% for women and 54% for men [11].
Zambia has ten provinces which are subdivided into one hundred and sixteen districts. This project was implemented in four out of the ten provinces, namely Eastern, Central, Luapula, Northern, and Southern Provinces; and two districts were covered in each of the four provinces.
Study Participants
The studies targeted young people aged 15 to 24 in the participating districts, both in and out of school. In-school young people were interviewed at respective schools, while out of school young people were interviewed in the communities. Authorities from the schools and communities were also interviewed in order to have wider contexts of perspectives.
Sample Size and Sampling Process
The evaluation sample size for the end-line was the same as the baseline survey to facilitate the comparison of the data (before and after the programme's implementation process). We used Cochrane's formula for sample size calculations based on a 50% desired effect (proportion) assumption.
N= Z2 pq/e2
where n = sample size, Z is the Z score for the 95% confidence level (1.96), p is the proportion (0.5), q is the 1-p (1-0.5 = 0.5) and e is the margin of error (5% for 95% confidence level.)
n = 1.962x 0.5 x 0.5/0.052 = 384
The 384 were sampled systematically from the schools and communities with the help of school authorities and community leaders.
For the qualitative component, purposive sampling was used to select study participants relevant to the study objectives and enable gender balance in the samples. Furthermore, this sampling process facilitated the identification of young people from various backgrounds within a given area to cover various socio-demographic characteristics. The actual numbers were determined by thematic saturation in the field.
Data collection process
The Knowledge, Attitude and Practice (KAP) analysis was used to collect data. Data were collected using a self-administered semi-structured questionnaire used during both the baseline survey and end-line to compare the results. This evaluation collected both secondary and primary data. Primary data was collected using participatory and respondent-driven/peer engagement as follows:
Systematic desk-based review: Electronic and physical databases of the life skills programme documents were identified and reviewed: baseline report, Theory of Change, results framework, and monitoring reports. Data review helped systematically examine the approaches, program package, and changes in target girls, pupils, community schools, teachers, and parents and partners.
Focus Group Discussions (FGD):The FGDs captured individual and group experiences among adolescents and young people participating in the project. SDGs facilitated the assessment of the extent to which the outcomes of the inclusive education project are being achieved relative to the project design and outputs.
Questionnaire interviews: Individual self-administered interviews using a structured questionnaire were administered to the young people. The interview structure was a Knowledge, Attitude and Practice (KAP) approach. The KAP survey helped contextualise the qualitative data generated by the interviews and focus groups.
Key informant interviews (KII): The rationale for key informant interviews was to discuss in detail project interventions. KII guides were done with selected children, teachers, community leaders, government, project staff, and partners. These helped in gathering stories of best practices and project success. The KII also helped examine how project activities have established and built institutional capacity to continue project outcomes beyond the project lifespan.
Data analysis
Quantitative data analysis
The questionnaire items were coded, and then the data was entered into the Statistical Package for Social Sciences (SPSS) version 20 template. Data was scrutinised for erroneous and missing values that could have been entered during entry by counterchecking with the questionnaires. Analysis of the data was done using statistical techniques, including descriptive statistics: means, standard deviations, frequencies and percentages and hypothesis tests in Pearson's Chi-square tests of association. Reliability tests were performed by visual check, percentiles, outliers and normality plots with accompanying statistical tests, including the use of Cronbach alpha to test for reliability for a measurement scale with a set of items varying from 0 to 1 to reflect homogeneity among a set of items. A reliability score of 0.70 and above was considered good enough to suggest reliability for this study. Graphical illustrations to enhance the findings.
Qualitative data analysis
Interviews were recorded digitally and later transcribed verbatim. Data analysis followed thematic analysis, a method for identifying, analysing and reporting patterns (themes) within data. This method minimally organises and describes the dataset in (rich) detail and further interprets various aspects of the research topic. The first step in analysing data was the development of codes. The coding process was then carried out using NVIVO version 7 (QSR Australia). Codes were subsequently grouped into categories – groups of content that share a commonality were then developed into broader themes. Finally, the themes were cross-checked with the interview transcripts to ensure they apply to relevant responses found within and across the interviews. The focus was on identifying, summarising, and retaining the patterns and similarities, differences, and new emerging themes.
Ethics
During the data collection process, consent or assent was obtained from the study participants before interviewing them. All the study objectives were explained to them, and they were informed that they were free to withdraw from the study at any point. Informants were also assured that none of their details or other identifiers would be included during the analysis and subsequent publication of the findings. By withholding respondents' details, readers cannot attribute views or statements to specific study participants.
Results and Discussion
A total of 385 participants took part in the Baseline, while 526 took part in the end-line survey; 306 were from schools, and 78 were from communities. Table 1 summarises the numbers of participants in the end-line survey.
For the qualitative component, 34 interviews were conducted, six focus group discussions with four members, sixteen key informant interviews with six teachers, six health workers and six implementing partners, all done separately.
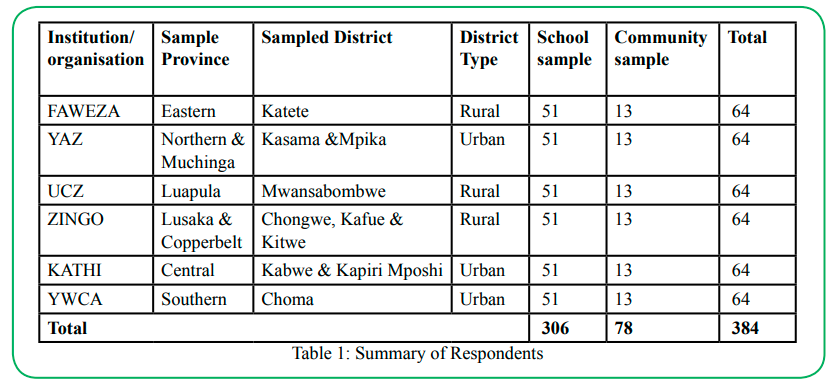
Table 1: Summary of Respondents
Socio-demographic Characteristics
The concentration of people in the program area is in the 15-24 age cohort (65.6%), while those above the 25+ age cohort were the least at 11.8%. At Baseline, the mean age for the adolescent was 17.90 (SD =3.3), with a minimum age of 10 and maximum age of 32. At the end-line, the findings of the study established a significant difference (P-value <0.001) in average age between male (18.4years (SD=3.3) and female adolescents (17.40(SD=3.2)) who were enrolled in the project at either a school or community clubs. The most common religious affiliations were the Catholic, Pentecostal and other protestants, each represented 22.6%, 76.2% and 1.1% of the young people, respectively. At least 61.0% of the young people had both parents alive at the time of the interview, as shown. Regarding orphan status, 30.1% were single orphans, while 10.0% were double orphans. Slightly less than half (45.1%) of the young people interviewed reported staying with their parents, followed by those staying with their mothers (25.7%) only, while those staying with their cousins were the least at 2.0%. Table 2 summarises the socio-demographic characteristics.
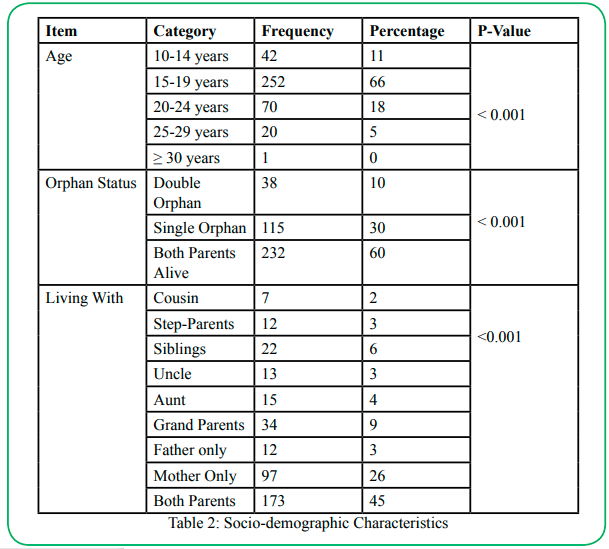
Table 2: Table 2: Socio-demographic Characteristics
Changes in knowledge levels among Adolescents and Young People Baseline Versus End-line
Implementation of program activities such as life skills training, awareness campaigns on life skills, debates and life skills clubs in schools resulted in increased life skills knowledge at the school level. The project was successful in reaching the targeted number of 10-24-year-old who received life skills-based HIV/AIDS education in school (33, 335/25,375 (131%)) as well as out of school (35, 389/25,373 (139%) and the difference percentage achievements among school-going and out of school was not statistically significant (P-value 0.329). Participation in the life skills program increased from 71 % in 2015 during the Baseline to 95% in 2017 during the end-line; this increase was statistically significant (P-value < 0.001). In addition, in 2017, more people reported that the services offered were adequate, and the increase was statistically significant (. i.e. 73.5% in 2017 and 64.9% in 2015, P-value = 0.032). The knowledge component analysis showed that knowledge scores were, in general, higher across most of the life skills parameters in 2017 compared to 2015. The majority (98.7 %) of the respondents attributed this change in knowledge to life skills activities. Table 3 summarises the thematic areas and percentages of responses:
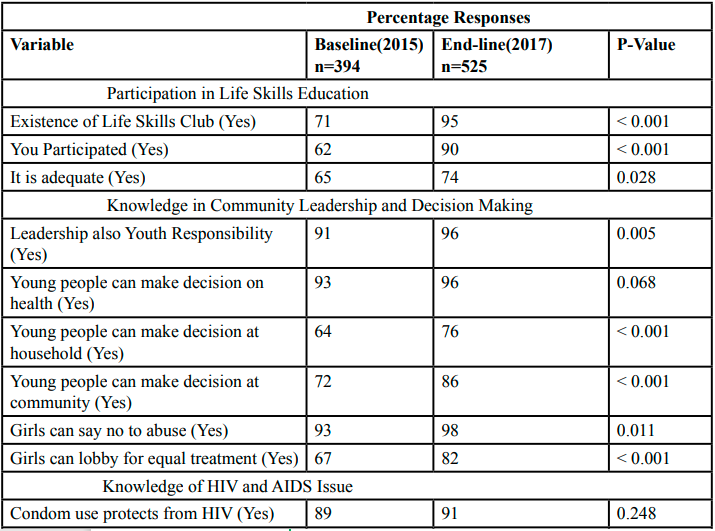
Table 3 : Summary of Knowledge Levels between Baseline and End-line
Changes in Attitudes between Baseline 2015 and End-line 2017 of the youth
Positive changes were noted across many attitudinal indicators from 2015 to 2017. Changes were noted in decision making, assertiveness, HIV/AIDS, general sexual and reproductive health, and alcohol and drug abuse. On community participation and decision-making attitudes, more people (90.9%) in 2017 reported that young people could participate in development activities in the community compared to 80.7% in 2015. Changes were also noted regarding perceptions that young people can make important decisions about their health (92.8% in 2015 and 96.2% in 2017); young people should help other young people report cases of abuse to relevant authorities (94.8% in 2015 and 7.0% in 2017. Table 4 summarises the findings.
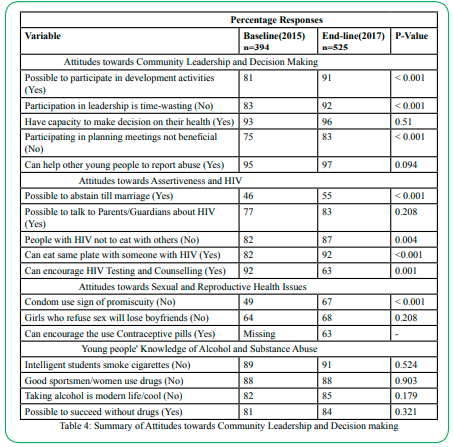
Table 4: Summary of Attitudes towards Community Leadership and Decision making
Changes in Practices in Community participation and decision making
Positive behaviour changes in the percentage difference between baseline and evaluation phases were noted across many practice parameters. Participation in leadership positions for youth-led activities in the community increased from 61.6% in 2015 to 66.3% in 2017. In comparison, the percentage of young people who made an important decision about their health increased from 89.6% in 2015 to 97.6%. Participation in meetings aimed at planning activities for youth also increased from 64.5% in 2015 to 84.4% in 2017, while young people who reported helping the other youth/s report cases to relevant authorities increased from 56.0% in 2015 to 71.0% in 2017 (Table 5).
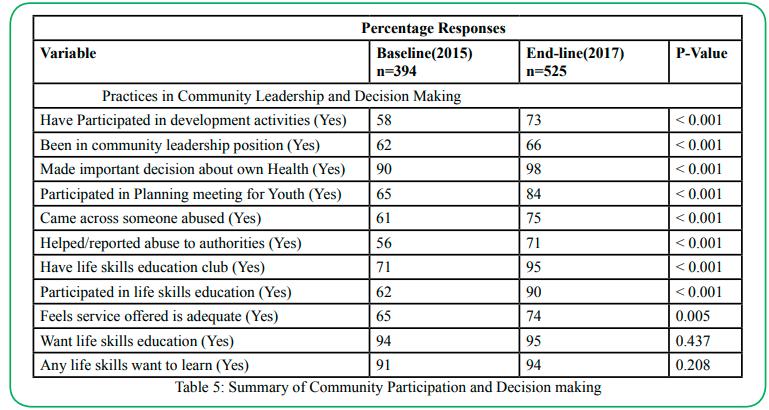
Table 5: Summary of Community Participation and Decision making
Improvement regarding sexual behaviour:
Overall, there was an improvement concerning sexual behaviour as although slightly fewer people reported abstaining from sexual intercourse in the last three months (43.2%) in 2017 compared to 50.2% in 2015, more people (35.2%) reported using condoms in 2017 compared to (29.5%) in 2015 (Table 6).
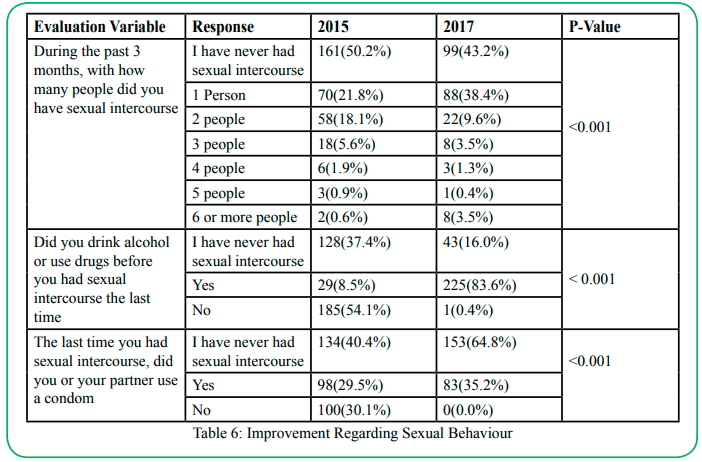
Table 6: Improvement Regarding Sexual Behaviour
Substance Abuse (Alcohol)
Of those who reported drinking, the majority (49.6%) of them started drinking at the age of 16 years and above, compared to 44.7% in 2015; this was not statistically significant (P-Value 0.0152). In 2017, the number of respondents indicating that they started beer drinking at nine years and below reduced significantly from 17.55 to 3.7%. The overall difference between the ages of commencement of beer drinking between 2015 and 2017 was not statistically significant (P-value = 0.941). Figure 1 summarises the comparisons between the two surveys.
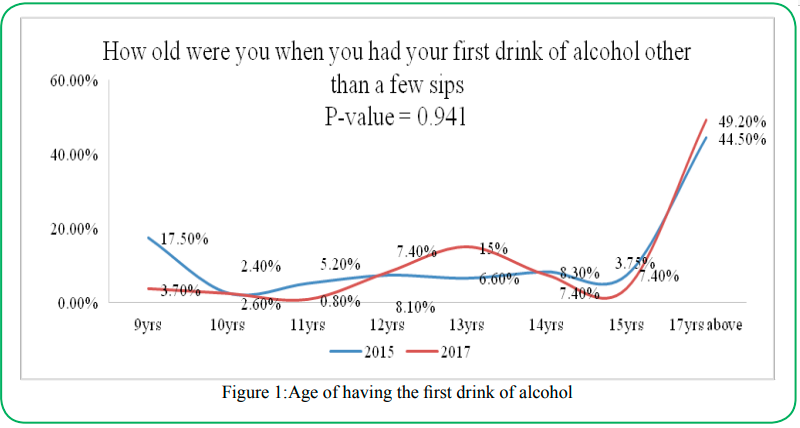
Figure 1: Age of having the first drink of alcohol
Qualitative Results:
The qualitative interviews showed that the adolescents and young people were involved in decision making at various levels. At household, young people reported participating in developing household budgets; “we are now involved in decision-making, for example, budgeting". The learners were also appointed to leadership positions in various committees at the school level such as safe clubs, disciplinary and school management committees; "They are also part of the disciplinary committee for the school, and they air out their views on what is affecting the pupils. In the safe club, they decide on what they want to do in a term." It was also reported that some leaners participate in school board meetings; “When we have board meetings, pupils through their representatives are invited to express their views on how the school should be run.” At the health facility level, some young people were actively involved in managing the youth-friendly corners; "The young people have been involved in decision making by joining the youth-friendly corners. They plan their activities." In the communities, executive committees for peer educators themselves have been formed to help with mobilisation processes. The committees make their own decisions on what is to be done and when to conduct the activities.
Assertiveness and confidence
Many young people reported that the training and sensitisation on family planning, early pregnancy and marriage, HIV/AIDS and communication skill increased their confidence and willingness to discuss sexuality issues freely. The sensitisation was done through face to face discussions, radio programs and drama; "We have seen that a number of them are free to talk about sexuality issues especially with their peers after the sensitisation."
The increased confidence and assertiveness were also demonstrated by more young people reporting abuse against them; "Children can make decisions; like sexual abuse, they have started reporting the cases." Due to increased reporting and awareness of laws, it was reported that there has been a reduction in gender-based violence among young people; "Generally, I can say that there has been a reduction in GBV since they now know what the law states.”
Sense of responsibility and purpose
Training in financial literacy enabled most young people, especially out of school young people, to engage in income-generating ventures. The young people could finance some of their needs from these ventures and contribute to meeting basic needs at the household level; "Most of the families have become financially independent and have found ways of saving money and engaging in IGAs.” Some young people in schools were engaged in fundraising events. The money they raised from the shows was used to pay school fees and rehabilitation of schools; “The program has helped the boys and girls as some individuals have started businesses, they have learnt how to save money, keeping themselves and their siblings well.”
Furthermore, many young people reported that they now have hope for the future, believing they can excel. This new hope has been due to the training in goal setting, which made many of them start planning their future; "The goal-setting skills have helped the learners to know how to set goals in life."
Sexual Reproduction Health (including HIV/AIDS services)
The specific variables selected for analysing SRH practices included assessment of whether one has engaged in sexual activity before, age of first sexual activity, number of sexual partners in the past four weeks and lifetime, whether a condom was used the last time one had sex, family planning method used if any, and whether alcohol or other substances were used before the last sexual act. Overall, it was reported that improved access to SRH services was improved. This access had positively shaped sexual behaviour and the utilisation of family planning methods and helped reduce early pregnancies.
• Access to VCT and STI services: Before the project was implemented, many young people would shun accessing SRH services because of worrying that health providers would perceive them as being promiscuous. However, it was reported that they were now freer to access VCT and STI services following the introduction of youth-friendly corners in some health facilities and support from the counsellors; "The counsellors as they do door to door VCT, they pick a box of condoms and return with none. For example, for the past seven months, we have 1041 males coming for VCT and 952 females coming for VCT. Moreover, these figures are for the young people of the ages between 14 to 24 years."
• Seeking male circumcision services: More young people had accessed male circumcision and encouraged others to access the services due to increased awareness of sexual and reproductive health issues and services; "Yes, there has been a change in that last year as all the grade 12s decided to go for male circumcision."
• Family planning/ contraception use: The study revealed significant differences (P-value <0.001) between the use of family planning methods reported in 2015 and 2017. During the evaluation, there was more usage of birth control pills (54.5%) than in 2015 (2.5%). Similarly, there is a slight improvement in the number of people using other methods such as injectables to prevent pregnancy in 2017 than reported in 2015. However, the use of the withdrawal method remained consistently low after project implementation than reported during 2015. A review of data from the health facilities and interviews with the health workers and adolescents confirmed that there had been increased access to family planning services/ contraception; "We have seen several adolescents accessing family planning services which have protected them from unwanted pregnancies”. These changes were attributed to training in decision-making skills, development of youth-friendly services and training of peer education; "If you look at the statistics, the majority are accessing SRH services, and most of the young people between the age of 15 to 24 are accessing pills and condoms from this health facility through the youth-friendly corners."
• Reduction in teenage pregnancies and drug abuse: In all the interviews, it was reported that pregnancies have reduced at the community level. This reduction was attributed to sensitisation by the safe clubs, teachers and peer educators on the effects of early pregnancy. In addition, the life skills training increased assertiveness and confidence among girls to refuse sexual advances. Availability of youth-friendly corners and peer educators also improved access to contraception by bringing the services closer to the young people and reducing social stigmatisation. "Cases of pregnancies and rampant drug abuse have reduced because of the sensitisation going on around the school.”
Sustainability
The program was largely classified as sustainable by all respondents. Factors that would shape sustainability included using government structures such as schools to deliver life skills and the integration of project activities into the existing community structures. Capacity building of different stakeholders (NGOs, community leaders, parents and children) in life skills would also enable these institutions to deliver the activities beyond the project's scope; "The program is sustainable as our learners have been empowered with knowledge and skills they see the benefits. They are extending the knowledge even to their friends in the community. I am very confident that the program activities will last long."
Discussion
This paper summarises and compares the findings of a baseline study done in 2015 and an end-line evaluation done in 2017 for a three-year project in life skills education in four provinces in Zambia. The project reached its intended target by over a third of beneficiaries, and the majority of the respondents were aged 15 to 24 years. Nearly two-thirds of the respondents were vulnerable young people who had both parents alive, whilst double or single orphans only consisted of slightly over a third. Despite this, only 45% of the respondents lived with both parents; this reflects the social disruptions that are prevalent among vulnerable young people and no doubt partly contributed by the social effects of HIV and AIDS. Other studies have also documented the social disruption effects of the HIV and AIDS pandemic resulting in poverty, vulnerability, sexual exploitation, and child labour [12,13]. Intervention programs such as this life skills education program by CHAZ have also improved community participation, education outcomes, knowledge, attitudes and abilities [2,14]. Another study done in Zambia documented improved knowledge, assertiveness and self-esteem but reported challenges because some concepts were difficult to understand and translate into local languages [15]. This study, therefore, adds to the body of evidence on the benefits of life skills education alongside academic education in the face of social disruptions of the HIV and AIDS pandemic.
Respondents indicated improvements in most indicators in the five focus areas of life skills education for young people: community participation, leadership and decision-making, HIV prevention, sexual and reproductive health, and alcohol and substance abuse. In community participation and decision-making, more young people have expressed knowledge of community involvement and good attitudes to participating in community development activities, including reporting abuse to authorities. Some cultural norms encourage passivity, especially among young women, as they promote submissiveness instead of assertiveness among women [16,17]. Mshweshwe [17] argues that traditional patriarchal beliefs emphasise male assertiveness and dominance over women, reinforcing domestic violence [17]. Through interventions like this life skills education program for young people, both boys and girls become socialised to challenge such traditional cultural beliefs.
The study showed that young people increased their knowledge of community leadership, had good attitudes and, participated by taking on leadership roles, made decisions at household and community levels. Girls would say no to sex and lobby for equal treatment. Youth is a turning point from childhood to adulthood, and individuals need to craft their self-identities and life projects [18]. Therefore, the program on life skills education teaches young people to participate in developing their communities and their own personal autonomy [18,19]. In terms of HIV prevention and sexuality education, the study showed that young people increased their comprehensive knowledge of transmission, also avoiding myths such as avoiding sharing meals with an infected person. This knowledge, attitude, and practice can help reduce the stigma associated with HIV infection. This is in agreement with studies that showed that group learning helped reduce stigma [20,21]. Another study in Zambia showed that teachers had challenges delivering comprehensive sexuality education because the contents are local norms and understandings. Hence, teachers use their discretion and may not deliver the full package [22]. The blended learning approach of the life skills education program through workshops, debates, and peer to peer learning overcomes some of the cultural barriers to effective learning [20,21]. The study also showed that life skills education could help fight drivers of alcohol and substance abuse, such as correct knowledge of harmful effects of alcohol and drugs and debunking false ideation that alcohol or drugs make someone smarter or successful [23,24].
Conclusion
There were significant increases in the life skills of young people who participated in the program intervention, such as community participation and decision making, leadership and decision making, HIV prevention, Sexual and reproductive health and alcohol and substance abuse. The integrated approach to life skills education helps to effectively address communication barriers compared to didactic teaching, especially when translated into local languages because of cultural norms.
Limitations
Although the project scored success on many indicators, it was reported that there were some issues which limited project implementation. These issues included human resources, material, financial and contextual barriers as reflected below:
• Few children were involved in the school management committees and life skills clubs which reduced the voice of children in decision and planning processes in the schools.
• Mentioning the names of private parts in the local language was a challenge for some facilitators who noted that such words sound more insulting in the local language than when the English language was used.
• Mixed feelings from a few teachers and some community members who believed that sex education encourages pupils to have sex affected teaching and learning processes. Learning was also affected by the clashing of life skills activities with other school activities.
• Slow acceptability of family planning methods due to traditional beliefs and myths such as fear of becoming barren or weak affected uptake of such services by some people.
• Transferring trained teachers to other schools and mobility of trained volunteers from one place to another in search of jobs affected the delivery of life skills activities. For the peer educators, the problem was compounded by inadequate and lack of financial incentives.
• Use of referral forms that were too advanced for some peer educators in some health facilities affected referral processes.
Recommendations
• Address the attrition problem of the trained volunteers by empowering the clubs with income-generating activities.
• Strengthen adolescent responsive health systems by placing trained young people in all health facilities who should link the adolescents to the health facilities, follow up the referral process and provide feedback on the referral processes. There is a need to advocate for the training of all health workers in providing adolescent-friendly health services.
• Lobby for more representation of children in school management committees and village councils. Such representation will help advance the welfare of children. Participation in child protection clubs and radio clubs should also be enhanced.
• Organisations and institutions should develop policy statements that require the participation of young people in the design and validation of all the activities that affect them. This will facilitate ownership of project activities.
• Develop an memorandum of understanding (MoU) so that teachers trained in life skills stay at an implementing school for the project period.
• Further addressing the problem of gender-based violence or bullying, which is still being experienced in schools, by enforcing school policy; developing an MoU with the Ministry of Community Development to help with enforcement of child protection; and integrating the life skills activities in the existing child protection structures at the community level.
• Strengthen collaboration among the Ministries of Education, Health, and Community Development at national, provincial and district levels concerning the delivery of life skills education and services. Such collaboration can help address the negative tradition and attitudes among some teachers, health workers and community members regarding life skills education.
Conflict of interest:
The authors declare no conflict of interest.
References
Bearinger, L. H., et al. (2007). "Global perspectives on the sexual and reproductive health of adolescents: patterns, prevention, and potential." The Lancet 369(9568): 1220-1231.View
Yankah, E. and P. Aggleton (2008). "Effects and Effectiveness of Life Skills Education for HIV Prevention in Young People." AIDS Education and Prevention 20(6): 465-485.View
Garofalo, R., et al. (2012). "Life Skills: Evaluation of a Theory-Driven Behavioral HIV Prevention Intervention for Young Transgender Women." Journal of Urban Health 89(3): 419-431.View
Visser, M. J. (2005). "Life skills training as HIV / AIDS preventive strategy in secondary schools : evaluation of a large-scale implementation process : original article." SAHARA : Journal of Social Aspects of HIV / AIDS Research Alliance 2(1): 203-216.View
Pettifor, A., et al. (2018). "Adolescent lives matter: preventing HIV in adolescents." Current opinion in HIV and AIDS 13(3): 265-273.View
Griffin, K. W., et al. (2003). "Effectiveness of a Universal Drug Abuse Prevention Approach for Youth at High Risk for Substance Use Initiation." Preventive Medicine 36(1): 1-7.View
Botvin, G. J., et al. (2006). "Preventing Youth Violence and Delinquency through a Universal School-Based Prevention Approach." Prevention Science 7(4): 403-408.View
Mturi, A. J. and M. M. Hennink (2005). "Perceptions of sex education for young people in Lesotho." Culture, Health & Sexuality 7(2): 129-143.View
Buthelezi, T., et al. (2007). "Youth voices about sex and AIDS: implications for life skills education through the 'Learning Together project in KwaZulu-Natal, South Africa." International Journal of Inclusive Education 11(4): 445-459.View
Manzano, A. (2016). "The craft of interviewing in realist evaluation." Evaluation 22(3): 342-360.View
Zambia Statistics Agency, Z. S. A., et al. (2020). Zambia Demographic and Health Survey 2018. Lusaka, Zambia, ZSA, MOH, UTH-VL and ICF.
Scorgie, F., et al. (2012). "Socio-Demographic Characteristics and Behavioral Risk Factors of Female Sex Workers in Sub-Saharan Africa: A Systematic Review." AIDS and Behavior 16(4): 920-933.View
Harrison, A., et al. (2015). "Sustained High HIV Incidence in Young Women in Southern Africa: Social, Behavioral, and Structural Factors and Emerging Intervention Approaches." Current HIV/AIDS Reports 12(2): 207-215.View
Akyeampong, K. (2014). "Reconceptualised life skills in secondary education in the African context: Lessons learnt from reforms in Ghana." International Review of Education 60(2): 217-234.View
Chavula, M. P., et al. (2021). "Experiences of teachers and community health workers implementing sexuality and life skills education in youth clubs in Zambia." Global Public Health: 1-15.View
Mestry, R. and M. Schmidt (2012). "A feminist postcolonial examination of female principals' experiences in South African secondary schools." Gender and Education 24(5): 535-551.View
Mshweshwe, L. (2020). "Understanding domestic violence: masculinity, culture, traditions." Heliyon 6(10): e05334.View
Buchert, L. (2014). "Learning needs and life skills for youth: An introduction." International Review of Education 60(2): 163- 176.View
Aggleton, P., et al. (2018). "HIV Education: Reflections on the Past, Priorities for the Future." AIDS Education and Prevention 30(3): 254-266.View
Skinta, M. D., et al. (2015). "Acceptance and Compassion-Based Group Therapy to Reduce HIV Stigma." Cognitive and Behavioral Practice 22(4): 481-490.View
Nyblade, L., et al. (2018). "HIV Stigma Reduction for Health Facility Staff: Development of a Blended- Learning Intervention." Frontiers in Public Health 6.View
Zulu, J. M., et al. (2019). "Why teach sexuality education in school? Teacher discretion in implementing comprehensive sexuality education in rural Zambia." International Journal for Equity in Health 18(1): 116View
Botvin, G. J. and K. W. Griffin (2015). "Life Skills Training: A competence enhancement approach to tobacco, alcohol, and drug abuse prevention." American Psychological Association, doi:10.1037/14550-011.View
Nasheeda, A., et al. (2019). "A narrative systematic review of life skills education: effectiveness, research gaps and priorities." International Journal of Adolescence and Youth 24(3): 362-379.View