
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 6 (2022), Article ID: JPHIP-211
https://doi.org/10.33790/jphip1100211Research Article
Perceived Mental Health Among Adult Residents Living in Region 4 Illinois, U.S., During COVID-19 Pandemic: A Cross-Sectional Study
Kailah Hilmes1, Alice Ma2*, Cedric Harville, II2, & Huaibo Xin2
1Bond County Health Department, Illinois, United States.
2Department of Applied Health, School of Education, Health & Human Behavior, Southern Illinois University Edwardsville, Illinois, United States.
*Corresponding Author Details: Alice Ma, PhD, MPH, CHES, Department of Applied Health, Southern Illinois University Edwardsville, Campus Box 1126, Edwardsville, Illinois, United States.
Received date: 15th September, 2022
Accepted date: 26th October, 2022
Published date: 28th October, 2022
Citation: Hilmes, K., Ma, A., Harville II, C., & Xin, H., (2022). Perceived Mental Health Among Adult Residents Living in Region 4 Illinois, U.S., During COVID-19 Pandemic: A Cross-Sectional Study. J Pub Health Issue Pract 6(2): 211.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
As of July 22, 2022, there were 3,528,282 total confirmed COVID-19 cases in Illinois, United States. The purpose of this study was to examine how the COVID-19 pandemic has contributed to Illinois Region 4 adult residents’ poor mental health and assess the mental health burden the residents experienced during the pandemic. A cross-sectional survey was administered via Qualtrics. Participants (N=632) living in the Illinois Region 4 counties of Bond, Clinton, Madison, Monroe, Randolph, St. Clair, and Washington were recruited through Facebook. The questionnaire was developed based on the current literature review and was validated by colleagues in public health. Both descriptive statistics and logistic regression were used for data analysis using SPSS. Most of the participants identified as female (86.7%). Many of the participants had an associate’s (23.6%) or a bachelor’s (29.4%) degree. About 84% of the participants reported that COVID-19 had changed things in their daily life (e.g., work, family, and social life). There was significantly more perceived mental health burden during the pandemic than there was before the pandemic (p<0.001). Approximately 68% of participants believed more mental health resources should be made available within their county of residence. Overall, the study findings suggest the perceived mental health burden among Region 4 adults, which highlight the need for mental health issues to be prioritized and the allocation of mental health resources to be optimized.
Key Words: Mental Health, COVID-19, Pandemic, Adult Residents, Illinois
Introduction
The United States experienced a peak in new confirmed COVID-19 cases in January 2022 with roughly 800,000 new daily cases [1]. In March 2022, the United States had upwards of 79 million cumulative confirmed COVID-19 cases. In January 2021, the United States peaked thus far in COVID-19 deaths with 3,400 daily reported COVID-19 deaths. The actual number of daily deaths due to COVID-19 was determined to be much higher because of the limitations in testing and reporting cause of death. In July 2022, the cumulative confirmed deaths in the United States were upwards of 1.03 million [1]. The pandemic has had far-reaching impacts across the United States. In Illinois, as of July 22, 2022, there were 3,528,282 total confirmed COVID-19 cases, with a total of 55,387,904 total tests performed [2]. Thus far, there have been 34,309 deaths and 4,503 probable deaths in the state of Illinois due to the COVID-19 virus. Region 4 is in the southwest portion of Illinois and includes the following counties: Bond, Clinton, Madison, Monroe, Randolph, St. Clair, and Washington. For Region 4, as of July 22, 2022, there has been a great number of confirmed COVID-19 cases and deaths: Bond County has had 4,294 confirmed cases and 29 deaths, Clinton County has had 11,840 confirmed cases and 113 deaths, Madison County has had 69,868 confirmed cases and 778 deaths, Monroe County has had 9,435 confirmed cases and 130 deaths, Randolph County has had 10,394 confirmed cases and 121 deaths, St. Clair County has had 63,226 confirmed cases and 716 deaths, and Washington County has had 4,407 confirmed cases and 34 deaths [2].
There is a certain level of fear that many people have felt at some point during the pandemic, including lockdown and quarantine mandates [3]. Stay at home orders utilized different strategies for social distancing, such as curfews, remote learning, and teleworking [4]. Many people were forced into accepting a new normal way of life [4]. False information about how the virus, in particular, how it transmits among people, contributed to panic [5]. People began impulse buying items for fear or running out of said items, not knowing if grocery stores would close, which caused national product shortages [3]. Throughout the pandemic we have seen revisions on restrictions, such as with travel and elective surgeries [6]. There has also been changes in restrictions and guidance of the COVID-19 vaccines [6]. It is evident that the pandemic has influenced the mental health of individuals as people try to adjust and cope with how their lives have been altered, and fear of the unknown has undoubtedly played a role [3]. In addition, other contributing factors exacerbated by the pandemic also corresponded to poor mental health, including access to mental health resources [7]. Not having access to resources even during pre-pandemic life can have negative impacts on mental health (e.g., unmanaged anxiety and depression, unprocessed trauma, and increased suicidal thoughts) [7]. During the lockdown and throughout the pandemic, some people who typically had access to help have lost access to mental health services and resources [7].
Unavoidably, the COVID-19 pandemic and the mental health of individuals have been intertwined. COVID-19 associated mental illnesses have been well documented and researched. For example, a study conducted in the United States with primarily Caucasian females suggested that there were negative correlations between mental health and COVID-19 [8]. Age, working status, insurance status, and financial status demonstrated significant relationships between COVID-19 and poor mental health. Older respondents were significantly less likely to report symptoms of depression, stress, and anxiety compared to younger respondents [8]. Those who lost employment due to the pandemic were approximately 2.25 times more likely to have signs of depression compared to those working remotely [8]. Another study conducted in the United States focused on college students, and the authors found that more than 71% of students reported that their stress and anxiety increased compared to pre-pandemic levels [9]. Less than half of the participants felt that they could cope with pandemic stress sufficiently [9]. Moreover, in a study carried out in Chicago, Illinois, participants with chronic health conditions were examined to see how their mental health was impacted by COVID-19 [10]. The increased severity of anxiety and the increased level of stress were significantly associated with the emotional distress caused by the fear of contracting the COVID-19 virus [10].
The present study examined how COVID-19 has impacted the mental health of Illinois Region 4 (Bond, Clinton, Madison, Monroe, Randolph, St. Clair, and Washington County) adult residents and assessed the mental health burden that the residents experienced during the pandemic. The study aimed to provide evidence to prioritize local mental health needs and to optimize the allocation of mental health resources.
Materials and Methods
Participants
Participants were recruited using a convenient sample via Facebook. An initial post including a brief introduction of the Principal Investigator (PI) for the study with an informed consent prompt, and IRB approval was posted on the PI’s Facebook page. The participants’ inclusion criteria included adults 18-80 years old currently living in the seven counties of Illinois’ COVID-19 Region 4: Bond, Clinton, Madison, Monroe, Randolph, St. Clair, and Washington. The final sample included 632 adult participants.
Measures
The survey instrument consisted of 14 multiple choice questions and was developed based on the current literature [11,12,13,14]. The instrument was pilot tested among colleagues in public health for accuracy of measurement. There were four demographic questions to collect information on participants’ age, gender, level of education, and residence location. The other 10 questions were developed to examine participants’ perceptions on their mental health burden and how their mental health had been impacted by the pandemic. Sample questions included: (1) Before the COVID-19 pandemic (i.e., before March 2020), did you feel you had poor mental health? (2) Did you feel a mental health burden at any point during the COVID-19 pandemic? (3) If you felt any mental health burden during the COVID-19 pandemic (i.e., March 2020 to the present time), do you expect this feeling to continue after the pandemic ends? (4) Has COVID-19 changed anything in your daily life (work, family, social life, etc.)? (5) Has having to isolate/quarantine (staying home while potentially infectious) affected your mental health negatively? (6) Has your mental health been negatively impacted by viewing the media’s reporting (i.e., press conferences, breaking news, repeated presentation of information) of COVID-19? (7) Has the increased use of technology (i.e., teleworking, online schooling, telemedicine, etc.) due to the COVID-19 pandemic negatively affected your mental health? (8) Do you believe that additional mental health resources need to be made available within the county you live in? The response options included yes, no, not sure, and not applicable.
Procedure
This was a descriptive, quantitative, cross-sectional study. It was approved by the university’s Institutional Review Board (IRB) (#1465). An online anonymous self-reporting survey link using Qualtrics was disseminated through the social media platform, Facebook. The survey remained open between February 9 and March 6, 2022. Participants completed the survey in less than 5 minutes.
Analysis
SPSS version 28 (Armonk, NY) was used to analyze the data. Descriptive statistics, including frequencies and percentages, were conducted to determine the participants’ perceptions on their mental health burden during the COVID-19 pandemic and the factors that contributed to their mental health. A multinomial logistic regression model was used to examine the association of mental health burden experienced during the COVID-19 pandemic and location within Illinois’ COVID-19 Region 4. A total of 632 participants were included in the final data analysis.
Results
Table 1 indicates the demographics of the sample. Of the total 632 participants, the sample resided in Bond (9.7%), Clinton (11.6%), Madison (21.4%), Monroe (8.1%), Randolph (16.9%), St. Clair (19.9%), and Washington Counties (12.5%). The participants were between the ages of 18-80, with the largest group being 30- 44 (34.5%). The majority of participants were female (86.7%), with most reporting an associate’s degree (23.6%) or bachelor’s degree (29.4%).
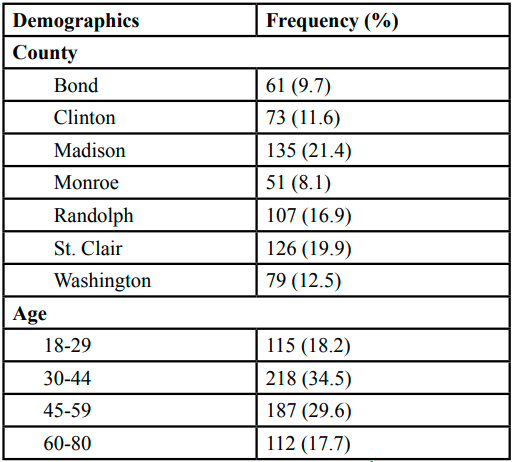
Table 1. Participant Demographics (N=632)
To identify a baseline of mental health burden, the question “Before the COVID-19 pandemic (i.e., before March 2020), did you feel you had poor mental health?” was asked. Approximately 14.9% of participants reported they had poor mental health before the COVID-19 pandemic, 80.4% reported they did not have poor mental health, and 2.8% were not sure about their mental health status before the COVID-19 pandemic. To gauge mental health during the pandemic, the question “Did you feel a mental health burden at any point during the COVID-19 pandemic?” was asked. Most participants (70.4%) reported they did feel a mental health burden, compared to 26.7% who said “No” and 2.8% who said “Not sure.” Of those who answered “Yes” to feeling a mental health burden during the pandemic, the question “If you felt any mental health burden during the COVID-19 pandemic (i.e., March 2020 to the present time), do you expect this feeling to continue after the pandemic ends?” was asked. The results for this question were nearly equally split, with 25.8% answering “Yes,” 20.6% answering “No,” and 26.9% were “Not sure.” When asked if participants believe that additional resources need to be made available within the county they live in, despite varying demographics, 67.9% of participants believed that additional resources need to be made available within the county they live in.
Table 2 describes the COVID-19 associated factors that contributed to participants’ mental health. Overall, the COVID-19 pandemic impacted the daily life of many people residing in the Region 4 counties, with 84% of people responding "Yes” to this question. Slightly more people (55.2%) answered “Yes” to having their mental health negatively impacted by the initial lockdown in March 2020, compared with 41% of individuals who answered “No.” Of those who were asked to isolate or quarantine themselves at any point of the pandemic, 50.6% of people felt their mental health was negatively impacted. More than half of participants (61.9%) who viewed the media’s reporting of COVID-19 felt their mental health was negatively impacted. With the pandemic there has been an increase in use of technology (i.e., teleworking, online schooling, and telemedicine), however, 52.7% of people reported it did not impact their mental health negatively.
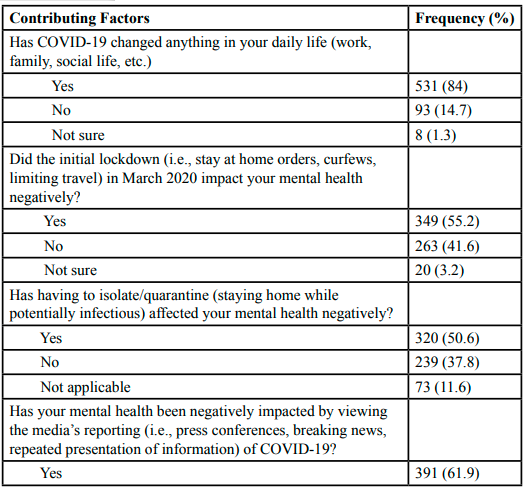
Table 2. Contributing Factors to Participants’ Mental Health Burden During the Pandemic (N=632)
A multinomial logistic regression was conducted to examine the relationship between feeling mental health burden and living within Illinois’ COVID-19 Region 4. For those who answered “Yes” to feeling a mental health burden at any point during the pandemic, significant relationships were found with five counties. Clinton County residents (B= (1.045), SE=0.267, Wald=15.335, p<0.001) were more than two times (OR=2.84, 95% CI [1.7, 4.8]) more likely to answer “Yes” to feeling a mental health burden, compared with those who answered “No.” Madison County residents (B= (1.386), SE=0.219, Wald=39.974, p<0.001) were four times (OR=4.00, 95% CI [2.6, 6.2]) more likely to answer “Yes” to feeling a mental health burden, compared with those who answered “No.” Monroe County residents (B= (0.847), SE=0.309, Wald=7.538, p=0.006) were two times (OR=2.33, 95% CI [1.3, 4.3]) more likely to answer “Yes” to feeling a mental health burden, compared with those who answered “No.” Randolph County residents (B= (0.723), SE=0.212, Wald=11.614, p<0.001) were two times (OR=2.06, 95% CI [1.4, 3.1]) more likely to answer “Yes” to feeling a mental health burden, compared to those who answered “No.” St. Clair County residents (B= (1.534), SE=0.235, Wald=42.581, p<0.001) were four times (OR=4.64, 95% CI [2.9, 7.4]) times more likely to answer “Yes” to feeling a mental health burden, compared to those who answered “No.”
Discussion
Findings from the current study support the existing literature [11,13]. For instance, more than half of the current study participants reported that COVID-19 related lockdowns, isolations, and quarantines had a negative impact on their mental well-being and contributed to their mental health burden. Fiorenzato and colleagues [11] found that compared to pre-lockdown, COVID-19 associated lockdown significantly increased their study participants’ levels of depression and anxiety during the pandemic. Henssler and colleagues’ (2021) systematic review and meta-analysis also revealed that compared with those not quarantining/isolating, people who were quarantined/isolated due to an infectious disease outbreak were at least two times more likely to experience depression and anxiety. Moreover, more than 60% of the participants in the current study reported that their mental health had been compromised due to viewing the media’s reporting of COVID-19. Likewise, previous studies demonstrated the evidence of mental health burden when examining the relationship between mental health and COVID-19 media consumption [11,12]. Among 1,215 Italian residents, those who constantly watched media coverage of COVID-19 were more likely to report worsened mood and to experience symptoms of mental disorders [11]. Gill and colleagues [12] reported similar findings from their study. Among young Canadian adult participants, those who viewed the media’s hourly reporting of COVID-19 were 3.24 times more likely to experience symptoms of depression and 3.22 times more likely to experience symptoms of anxiety than those who did not [12].
Overwhelmingly, the current study participants felt a mental health burden at any point during the COVID-19 pandemic and believed that additional mental health resources needed to be made available within the county they live in in order to alleviate their county residents’ mental health burden. Participants’ feelings of mental health burden also varied by county. Results from an online survey in March 2020 by the Pew Research Center’s American Trends Panel, which consisted of a representative sample of 9,687 U.S. adults without a pre-existing mental health condition, indicated that during the COVID-19 pandemic, 15% of these individuals experienced two psychological distress symptoms for three days in a week, and 13% experienced three or more symptoms [15]. Aragona and colleagues [16] revealed similar findings from 286 mental health patients who were immigrants living in Italy and socially and economically disadvantaged that demonstrated a significant reduction in patient visits for psychiatric interview and follow-up visits after the March 2020 COVID-19 lockdown. Earlier, Saxena and colleagues [17] discussed and compared the scarcity, inequity, and inefficiency of mental health resources in high-income, middle-income, and low-income counties, and cited that two-thirds of the U.S. population with mental disorders received no treatment, and ironically, about half of the individuals who received mental healthcare did not meet diagnostic criteria for a mental disorder.
However, the transition from conventional practice to telepsychology and telepsychiatry as an immediate response to the COVID-19 pandemic made it promising to sustain and expand mental healthcare delivery [18,19,20,21]. A total of 2,619 U.S. licensed psychologists reported that during the pandemic, the utilization of telepsychology for their clinical work was increased from 7.1% to 85.5%, and it remain increased after the pandemic. About 67.3% of these psychologists used telepsychology to perform all of their clinical work, and the use of telepsychology appeared more prevalent among outpatient facilities [21]. Digital technology broadened access to mental healthcare and enhanced equity in access to services [19]. Moreover, in an effort to guide the development, implementation, and evaluation of mental health interventions during the pandemic, early career psychiatrists from each World Health Organization region were invited to develop an overarching conceptual framework at the beginning of the COVID-19 outbreak [22]. The Mental Health Preparedness and Action Conceptual Framework was developed and constructed by five major components which included preparing infrastructures (e.g., telepsychiatry, mental health surveillance system, psychological first aid, and training for primary healthcare workers) and coordination; identifying and monitoring risk/vulnerable populations, and assessing and monitoring health technology; reducing mental distress by addressing misinformation through proper channels; sustaining mental healthcare services through funding, policy, and coordination and collaboration within the healthcare system; and enhancing both risk and health communication through conventional and unconventional communication platforms [22]. Furthermore, more concrete plans and recommendations were made by other researchers and practitioners. For instance, Maulik and colleagues [23] published recommendations for low, middle, and high resource settings to recognize the disparities of capabilities between and within countries. They further emphasized the needs of developing or strengthening “equitable, accessible and appropriate community-based mental health services and clinic-based services for those needed special care”; enabling “employers to manage stress at workplaces”; and promoting research to improve information systems and develop special population-based interventions [23].
Implications
The findings from the current study demonstrated a mental health burden among Illinois Region 4 adult residents, which highlight the need for enhancing mental health resources for the region and additional resources to be made available and accessible. These findings can inform the existing work of local health departments, clinics, and other mental health efforts. Boden and colleagues [24] offer a framework for developing mental health-based interventions that emphasize population health, rather than patient-level health. Qualitative and mixed method studies can further aid in understanding the mental health needs in Illinois’ Region 4 and other regions [25]. Burgeoning research on the mental health impact from the COVID-19 pandemic suggest that focusing on individual health benefits, social connectedness, mental health outcomes, and the promotion of community-tailored and evidence-based information may be useful strategies in future interventions [26]. Locally, the passing of Senate Bill 3617, which serves to increase the number of mental health professionals in Illinois, expand behavioral health training, and fortify the mental health infrastructure in the state, as well as the new 988 suicide prevention and mental health crisis line, may improve residents’ access to mental healthcare [27,28]. Future studies should be conducted on the multilevel and longitudinal impacts that structural and environmental forces, including pandemics, can contribute for this region, as well as other regions in the U.S. with high mental health burden.
Limitations
The current descriptive study adopted a cross-sectional study design and used a convenience sampling strategy, which could inherit biases for both internal and external validity. The survey was only shared through Facebook, which means that only those who had an account on the platform would have access to the survey. The majority of respondents were female (86.7%), compared to male (13.1%) and non-binary/third gender (0.2%). There were only three participants who answered “some high school” as their highest level of education, therefore, the sample is not representative of that group. Thus, larger studies should be conducted with gender-diverse participants across varied levels of education. In addition, some of the questions such as, “Did the initial lockdown (i.e., stay at home orders, curfews, limiting travel) in March 2020 impact your mental health negatively?” may subject participants to recall bias, as they had to recall their mental health experience retrospectively. Moreover, both reliability and validity of the survey instrument should be further examined for any future use.
Conclusion
Overall, the study findings suggest the mental health burden among Illinois Region 4 adult residents, which highlight the need for mental health issues to be prioritized, additional resources to be made available and accessible, and future studies on the deeper impacts a pandemic can Contribute.
Competing Interests:
The authors declare that they have no competing interests.
References
Ritchie H., Mathieu E., Rodés-Guirao L., Appel C., Giattino C., Ortiz-Ospina E., Hasell J., Macdonald B., Beltekian D., and Roser M. (2022). Coronavirus Pandemic (COVID-19). Retrieved on March 8, 2022, from https://ourworldindata.org/ coronavirus View
Illinois Department of Public Health. (2022). COVID-19 Statistics. Retrieved March 8, 2022, from https://dph.illinois. gov/covid19/data.htmlView
Ornell, F., Halpern, S. C., Kessler, F., & Narvaez, J. (2020). The impact of the COVID-19 pandemic on the mental health of healthcare professionals. Cadernos de saude publica, 36(4), e00063520. https://doi.org/10.1590/0102-311X00063520View
Medline, A., Hayes, L., Valdez, K., Hayashi, A., Vahedi, F., Capell, W., Sonnenberg, J., Glick, Z., & Klausner, J. D. (2020). Evaluating the impact of stay-at-home orders on the time to reach the peak burden of Covid-19 cases and deaths: Does timing matter? BMC Public Health, 20(1), 1–7. https://doi-org. libproxy.siue.edu/10.1186/s12889-020-09817-9View
Mian, A., & Khan, S. (2020). Coronavirus: The spread of misinformation. BMC Medicine, 18(1), 89. https://doi-org. libproxy.siue.edu/10.1186/s12916-020-01556-3View
Department of Defense. (2021). Coronavirus: Latest DOD Guidance. Retrieved November 2,2021, from https://www. defense.gov/Spotlights/Coronavirus-DoD-Response/Latest-DOD-GuidanceView
Raval, N. (2020). Mental health implications of COVID-19 in India. Indian Journal of Health & Wellbeing, 11(7–9), 276–281.
Jewell, J. S., Farewell, C. V., Welton-Mitchell, C., Lee-Winn, A., Walls, J., & Leiferman, J. A. (2020). Mental health during the COVID-19 pandemic in the United States: Online survey. JMIR Formative Research, 4(10), E22043. doi:10.2196/22043View
Wang, X., Hegde, S., Son, C., Keller, B., Smith, A., & Sasangohar, F. (2020). Investigating mental health of US college students during the COVID-19 pandemic: Cross-sectional survey study. Journal of Medical Internet Research, 22(9), e22817. doi:10.2196/22817View
Lovett, R. M., Opsasnick, L., Russell, A., Yoon, E., Weiner-Light, S., Serper, M., ... & Wolf, M. S. (2022). Prevalence of anxiety and depressive symptoms and impact on self-management among adults with chronic conditions in Chicago, Illinois, USA, during the COVID-19 pandemic: A cross-sectional survey. BMJ Open, 12(1), e052495. doi: https://doi. org/10.1136/bmjopen-2021-052495View
Fiorenzato, E., Zabberoni, S., Costa, A., & Cona, G. (2021). Cognitive and mental health changes and their vulnerability factors related to COVID-19 lockdown in Italy. PLoS ONE , 16(1), 1–25. https://doi-org.libproxy.siue.edu/10.1371/journal. pone.0246204 View
Gill, P. K., Du, C., Khan, F., Karimi, N., Sabharwal, K., & Agarwal, M. (2022). The psychological effects of COVID-19 spread in young Canadian adults. International Journal of Social Psychiatry, 68(1), 216–222. https://doi-org.libproxy.siue. edu/10.1177/0020764020988878View
Henssler, J., Stock, F., van Bohemen, J., Walter, H., Heinz, A., & Brandt, L. (2021). Mental health effects of infection containment strategies: Quarantine and isolation—a systematic review and meta-analysis. European Archives of Psychiatry & Clinical Neuroscience, 271(2), 223–234. https://doi-org.libproxy.siue. edu/10.1007/s00406-020-01196-xView
Lee, C. M., Cadigan, J. M., & Rhew, I. C. (2020). Increases in loneliness among young adults during the COVID-19 pandemic and association with increases in mental health problems. Journal of Adolescent Health, 67(5), 714-717. https://doi. org/10.1016/j.jadohealth.2020.08.009View
Holingue, C., Badillo-Goicoechea, E., Riehm, K. E., Veldhuis, C. B., Thrul, J., Johnson, R.M., ... & Kalb, L. G. (2020). Mental distress during the COVID-19 pandemic among US adults without a pre-existing mental health condition: Findings from American trend panel survey. Preventive Medicine, 139, 106231-106238. https://doi.org/10.1016/j.ypmed.2020.106231 View
Aragona, M., Barbato, A., Cavani, A., Costanzo, G., & Mirisola, C. (2020). Negative impacts of COVID-19 lockdown on mental health service access and follow-up adherence for immigrants and individuals in socio-economic difficulties. Public Health, 186, 52-56. https://doi.org/10.1016/j.puhe.2020.06.055View
Saxena, S., Thornicroft, G., Knapp, M., & Whiteford, H. (2007). Resources for mental health: Scarcity, inequity, and inefficiency. The Lancet, 370(9590), 878-889. https://doi.org/10.1016/ S0140-6736(07)61239-2View
Jurcik, T., Jarvis, G. E., Zeleskov Doric, J., Krasavtseva, Y., Yaltonskaya, A., Ogiwara, K., ... & Grigoryan, K. (2021). Adapting mental health services to the COVID-19 pandemic: Reflections from professionals in four countries. Counselling Psychology Quarterly, 34(3-4), 649-675. https://doi.org/10.108 0/09515070.2020.1785846View
Lattie, E. G., Stiles-Shields, C., & Graham, A. K. (2022). An overview of and recommendations for more accessible digital mental health services. Nature Reviews Psychology, 1(2), 87- 100. https://doi.org/10.1038/s44159-021-00003-1View
Li, H., Glecia, A., Kent-Wilkinson, A., Leidl, D., Kleib, M., & Risling, T. (2021). Transition of mental health service delivery to telepsychiatry in response to COVID-19: A literature review. Psychiatric Quarterly, 1-17. https://doi.org/10.1007/s11126- 021-09926-7View
Pierce, B. S., Perrin, P. B., Tyler, C. M., McKee, G. B., & Watson, J. D. (2021). The COVID-19 telepsychology revolution: A national study of pandemic-based changes in US mental health care delivery. American Psychologist, 76(1), 14-25. https://doi. org/10.1037/amp0000722View
Ransing, R., Adiukwu, F., Pereira-Sanchez, V., Ramalho, R., Orsolini, L., Teixeira, A. L. S., ... & Kundadak, G. K. (2020). Mental health interventions during the COVID-19 pandemic: A conceptual framework by early career psychiatrists. Asian Journal of Psychiatry, 51, 102085-102092. https://doi. org/10.1016/j.ajp.2020.102085 View
Maulik, P. K., Thornicroft, G., & Saxena, S. (2020). Roadmap to strengthen global mental health systems to tackle the impact of the COVID-19 pandemic. International Journal of Mental Health Systems, 14(1), 1-13. https://doi.org/10.1186/s13033- 020-00393-4View
Boden, M., Zimmerman, L., Azevedo, K. J., Ruzek, J. I., Gala, S., Magid, H. S. A., ... & McLean, C. P. (2021). Addressing the mental health impact of COVID-19 through population health. Clinical Psychology Review, 85, 102006. https://doi. org/10.1016/j.cpr.2021.102006View
Palinkas, L. A. (2014). Qualitative and mixed methods in mental health services and implementation research. Journal of Clinical Child & Adolescent Psychology, 43(6), 851-861. https://doi.org/10.1080/15374416.2014.910791View
Owens, C., Struble, N., Currin, J. M., Giano, Z., & Hubach, R. D. (2021). Beliefs about social distancing during COVID-19 stay-at-home orders: A theory-based salient belief elicitation. Health Behavior Research, 4(1), 6. https://doi.org/10.4148/2572- 1836.1094View
Federal Communications Commission. (2022). 988 Suicide and Crisis Lifeline. Retrieved July 19, 2022, from https://www.fcc. gov/988-suicide-and-crisis-lifeline#:~:text=The%20988%20 Lifeline%20provides%2024,professionals%20with%20the%20 Lifeline%20network.View
State of Illinois. (2022). Governor Pritzker Signs Legislation Increasing Mental Health Workforce in Illinois. Retrieved July 19, 2022, from https://www.illinois.gov/news/press-release.25035.htmView