
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 7 (2023), Article ID: JPHIP-217
https://doi.org/10.33790/jphip1100217Research Article
Gender Difference in Blood Pressure Control among Low-Income Individuals (B40) with Hypertension in Malaysia: the RESPOND Study
Mazapuspavina Md Yasin1, Mohamad-Rodi Isa2*, Nafiza Mat-Nasir1, Farnaza Ariffin1, Fadhlina Abd-Majid3, Benjamin Palafox4, and Martin McKee4
1Department of Primary Care Medicine, Faculty of Medicine, Universiti Teknologi MARA, Sungai Buloh Campus, 47000, Selangor, Malaysia.
2Department of Public Health Medicine, Faculty of Medicine, Universiti Teknologi MARA, Sungai Buloh Campus, 47000, Selangor, Malaysia.
3Centre for Translation Research and Epidemiology (CenTRE), Faculty of Medicine, Universiti Teknologi MARA, Sungai Buloh Campus, 47000, Selangor, Malaysia.
4Department of Health Service Research & Policy, London School of Hygiene & Tropical Medicine, 15 – 17 Tavistock Place, London WC1H 9SH, United Kingdom.
*Corresponding Author Details: Mohamad Rodi Isa, MBBS, DAP&E, MPH, DrPH, Department of Public Health Medicine, Faculty of Medicine, Universiti Teknologi MARA, Jalan Hospital, 47000 Sungai Buloh, Selangor, Malaysia.
Received date: 26th March, 2023
Accepted date: 13th April, 2023
Published date: 15th April, 2023
Citation: Md Yasin, M., Isa, M. R., Mat-Nasir, N., Ariffin, F., Abd-Majid, F., Palafox, B., & McKee, M., (2023). Gender Difference in Blood Pressure Control among Low-Income Individuals (B40) with Hypertension in Malaysia: the RESPOND Study. J Pub Health Issue Pract 7(1): 217.
Copyright: ©2023, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Hypertension is a major modifiable determinant of the increasing burden of cardiovascular disease (CVD) in Malaysia. The aim of this study is to determine the factors associated with hypertension control in men and women among the low-income individuals (B40) group with hypertension in Malaysia. The communities were selected from rural and urban populations in four peninsular states. Following a multistage sampling approach, communities in each stratum were selected according to probability proportional to the size and identified based on national census data by the community and administrative registers. Eligible individuals were those aged between 35 and 70 years old, self-reported or identified as hypertensive at screening. A survey using validated questionnaires was conducted. The prevalence of controlled hypertension was 33.1% (95%CI: 24.7, 41.5) in men and 34.0% (95%CI: 29.0, 39.0%) in women respondents. In men, hypertension control rates were positively associated with individuals who received or heard any information about hypertension [(Adj. OR: 2.95 (95%CI: 1.02, 8.52)], having two or more comorbidities [Adj. OR: 6.38 (955CI: 1.37, 29.62)] and those who had regular treatment for hypertension [Adj. OR: 14.51 (95%CI: 1.46, 44.21)]. Whereas, in women, hypertension control rates were positively associated with race whereas the non-Malay had more controlled status compared to Malay [Adj. OR: 5.94, (95%CI: 1.26, 28.09)] and those who regularly see the health professional [Adj. OR: 5.68 (95%CI: 1.94, 16.63)]. Health education and promotion programs need to be conducted to disseminate more information about hypertension to the community. Clinical services need to be improved mostly on regular follow up, giving proper consultation on treatment and treating patients to increase the prevalence of hypertension control.
Introduction
Hypertension it is a modifiable risk factor for cardiovascular disease, heart failure, kidney problems and stroke [1-3]. It is a major modifiable determinant of the increasing burden of cardiovascular disease (CVD) in Malaysia [4]. The burden of treating non communicable diseases (NCDs) is high and will continue to increase. Based on current trends, a Malaysian will be spending an estimated 9.5 years of life expectancy in poor health due to NCDs or chronic diseases [5].
Uncontrolled hypertension is the single largest contributor to CVD which can cause stroke, heart failure, and coronary artery disease. It is also a major contributor to kidney disease [6]. There are about 36 million adults had uncontrollable blood pressure [7]. Hypertension control is known to differ by age, sex, and various other factors [8,9]. In Malaysia, hypertension control among those on treatment has improved from 27.5% in 2006 to 45.0% in 2019 [10]. However, despite the progress of hypertension treatment in Malaysia, the control of hypertension is still below 50% with some cohorts faring worse than others [4]. In the US, from the National Health and Nutrition Examination Survey 1999–2004 database, the blood pressure control in 1999-2000 was 29.2 ± 2.3% and in 2003 2004 was 36.8 ± 2.3% [11].
In Malaysia NHMS 2019 study found the prevalence of hypertension in females was 29.7% (95% CI: 27.98, 31.46) [10]. Among American Women, hypertension accounts for 1 in 5 deaths and is the most risk factor for death and the development of cardiovascular and other diseases [12]. In Framingham Heart Study found that blood pressure control rates declined in older women with increasing age [13]. However, there were many clinical trials have been conducted and found that hypertensive women had a better blood pressure response to the antihypertensive drug such as a diuretic [14] and beta blockers [14,15] compared to men. Effective treatment and control of hypertension improve cardiovascular outcome in women [12].
Men are more likely to develop hypertension than women [3,16] and have higher mean systolic and diastolic compared to women [16]. It is due to a lack of endogenous oestrogen that may modulate vascular function, resulting in vasodilation and contributing to lower blood pressure [17]. The prevalence of hypertension in males was 30.3% (95% CI: 28.22, 32.50) from the result of the Malaysia NHMS 2019 study [10]. The Third National Health and Nutrition Examination (NHANES) survey found there was only 19% of men had their blood pressure controlled. It is due to men being less aware and receiving less treatment [16]. A study by Ong, Annette-Tso [18] in the National Health and Nutrition Examination Survey 1999 –2004 found there was no significant superiority in blood pressure control in men compared to women. The Cardiovascular Research Network (CVRN) Hypertension Registry from 2001-2006 found that men 18-49 years old had 17% (95%CI: 16,20) lower odds but men 65 years old and above had a 12% (95%CI: 7,16) higher odds of having hypertension control compared to women at the same age [9].
There were many studies have been conducted on hypertension control among Malaysian. However, there is no study was conducted on low-income individuals (B40) with hypertension. Studied had identified that there was an association between poverty and environmental factors has a significant burden of disease, death and disability in many parts of the world [19]. Therefore, the aim of this study is to determine the factors associated with hypertension control in men and women among the B40 group with hypertension in Malaysia.
Material and method
Definition
At the time when the study was planned, those in the low-income individuals (B40) category had a household income of less than RM3,855 (€832; US$932) (level set in 2014). The cut-off point has changed over time. Those in the B40 category can be found in urban and rural areas and the study design included communities in both settings. Urban and rural areas were defined according to the Malaysian Population and Housing Census 2000 [20].
Data were collected within the ‘Responsive and Equitable Health Systems – Partnership on Non-communicable Diseases’ (RESPOND) Project, being undertaken in Malaysia and the Philippines. Unlike the surveys described earlier that offer wide coverage of the country, RESPOND has been designed to gain in-depth knowledge of the lived experience of those with hypertension living in low-income communities using a mix of quantitative and qualitative methods, with a particular emphasis on their therapeutic journeys. The protocol and detailed methodology have been published elsewhere [21].
Sampling method
The urban and rural B40 communities were selected using a multistage sampling approach. The first stage was a purposive selection of four states in Peninsular Malaysia, Selangor, Perak, Kelantan, and Johor, all larger states with a mix of urban and rural communities. The second stage was the selection of 24 communities, three urban and three rural from each of the four states. Communities in each stratum were selected according to probability proportional to size using sampling frames based on national census data by the community and administrative registers. The third stage involved the recruitment of 25 households from each community, randomly selected using a random online generator. Nearby communities were substituted where it was not feasible to ensure high levels of engagement with the chosen communities. This could arise from a lack of community support, the security risk for study personnel, inaccessibility by usual means of transportation, poor internet connection, or the existence of ongoing activities that may affect hypertension treatment-seeking behaviour. The flowchart of the study is shown in Figure 1.

Figure 1: The Flowchart of the study
Study population
The study population comprised of adults aged 35 to 70 years old with hypertension, living within B40 households that were expected to remain at the current address for at least 18 months from the date of screening, with either a self-reported history of hypertension (previously diagnosed whether on or off treatment) or found to have elevated blood pressure at screening. B40 households were identified by asking the household income directly of less than RM3,855 (€832; US$932) (level set in 2014) of the respondents. Exclusion criteria were those with a self-reported history of major chronic co morbidities that required regular contact with the health system such as cancer or HIV and those who were planning to move within the next 18 months. High blood pressure on screening was defined as when the average of two blood pressure measurements > 140/90 mmHg (using an OMRON blood pressure recorder from the non- dominant arm while in a sitting position after at least 5 minutes rest).
Sample size estimation was calculated based on detecting urban and rural differences in hypertension treatment in a middle-income country with α=0.05 and power of 0.8 (two-tailed), which we had previously found was as large as 14 percentage points (42% urban and 28% rural). This would require a minimum sample of 600 hypertensive individuals across 12 urban and 12 rural communities [21,22].
Study procedure and data collection process
A maximum of three attempts was made to contact identified households, with the substitution of another randomly selected household if contact could not be made. When a household responded but refused to participate in the full study, simple demographics, risk factors and cardiovascular disease (CVD) history were recorded. When an eligible household was identified and agreed to participate, all adults in the household were enumerated and initial data were collected using a household census form. Screening for eligibility was conducted and if more than one hypertensive individual was identified one was selected at random using a probability-based method and invited to participate. If none were present another household was selected. Those who agreed were provided with written informed consent and enrolled. A brief non-responder form was completed for those participants who refused, and substitute participants were asked.
Variable of interest
The variable of interest for the comparison was gender, whether the respondent is men or women. The independent variables of the sociodemographic characteristics include age group (less than 59 and 60 years old), ethnicity (Malay and non-Malay), location (urban or rural), marital status (currently married and other married), educational status (no formal and has formal education), current employment (yes and no) and tobacco user (former and current used and never used).
Independent variable on the hypertension characteristics includes: received or heard any information about hypertension (yes and no), another comorbidity (no, one and two & more), systolic blood pressure (SBP) (<140 and ≥ 140 mmHg), diastolic blood pressure (DBP) (< 90 and ≥ 90 mmHg), regular treatment (yes and no), duration of hypertension (less than 1 year, 1 – 5 years, 6 – 9 years and more than 10 years, see regular health professional (yes and no) and knowledge of hypertension (nothing, know little and very familiar). Blood pressure control is defined as an average of SBP < 140 mmHg and DBP < 90 mmHg regardless of medication [7].
Statistical analysis
Data were managed and analyzed using the Statistical Package for Social Science (SPSS) Version 28.0 (SPSS, Inc, Chicago, IL, version 27.0). Descriptive analyses were used to report sociodemographic characteristics based on gender (men and women). Categorical data were presented as frequencies (n) and percentages (%). The comparison of the variable interests between rural and urban respondents and other categorical variables was analyzed using Chi square or Fisher’s Exact test.
Multiple logistic regression models were used to identify factors associated with the prevalence of control of hypertension. Chi-square tests were conducted to compare categorical variables. The Hosmer Lemeshow goodness of fit for logistic regression and C-statistics were evaluated. Significance was set at a p-value < 0.05.
Results
A total of 611 were involved in this study including 162 (26.5%) men and 449 (73.5%) women. Table 1 shows the characteristics of the men and women respondents and compares variables among gender. Among men respondents, the majority of them were 60 years old and above (45.1%), Malay (98.1%), stay in the rural area (53.7%), currently married (88.9%), has formal educational status (95.7%), not working (62.3%) and current and formerly tobacco user (55.8%). The characteristics among women respondents were almost the sample as men respondents however, the majority of them were staying in the urban area (51.9%) and never used any tobacco product (97.5%). There were significant differences in the martial status [x2(1) = 30.172, p<0.001], educational status [x2(1) = 4.970, p=0.026], employment status [x2(1) = 32.672, p<0.001] and tobacco user [x2(1) = 235.014, p<0.001] between men and female respondents.
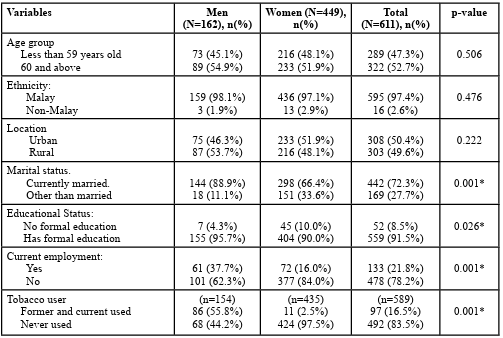
Table 1: The sociodemographic characteristics of the B40 group with hypertension stratified by gender (N=611)
The hypertension characteristics of the B40 group with hypertension stratified by gender are shown in Table 2. Among male respondents, the majority of them received or heard any information about hypertension (68.5%), no other comorbidities (50.0%), mean systolic blood pressure of more than 140 mmHg (63.7%), mean diastolic blood pressure with less than 90 mmHg (50.4%), has regular treatment (88.4%), duration of hypertension of 1 to 5 years (55.8%), has regular see a health professional (86.0%) and known little about knowledge of hypertension (75.2%). Among female respondents, the hypertension characteristics were almost the sample as male respondents. There were significant differences in the number on comorbidities [x2(2) = 6.816, p=0.033] and the knowledge of hypertension [x2(2) = 10.967, p=0.004] between male and female respondents.
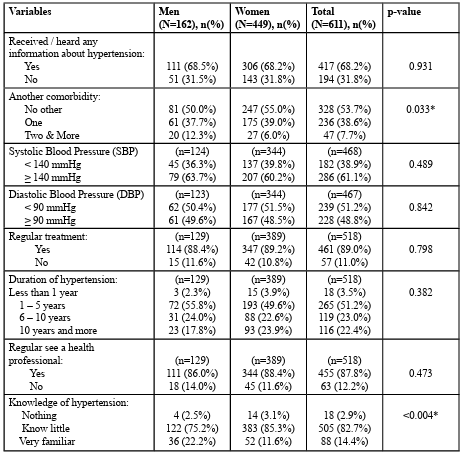
Table 2: The hypertension characteristics of the B40 group with hypertension stratified by gender (N=611)
The number of people with controlled hypertension, unadjusted odds ratio (OR), adjusted OR, and its confidence interval for men and women are shown in Table 3. Adjusted OR was adjusted for thirteen variables. For the stratification of control and uncontrol hypertension, there were 143 respondents excluded from the study due to no record of blood pressure. Among the 124 men and 344 women with hypertension, 41 (33.1%) and 117 (34.0%) kept their blood pressure controlled. Overall, the prevalence of controlled hypertension was 33.8% (95%CI: 29.5, 38.1%). The prevalence of controlled hypertension among men respondents was 33.1% (95%CI: 24.7, 41.5) and among women, respondents were 34.0% (95%CI: 29.0, 39.0%). There was no significant difference in the hypertension control status between gender [(OR: 0.96 (95%CI: 0.62, 1.48), p=0.848].
Among hypertensive men in the adjusted model, control rates were positively associated with individuals who received or heard any information about hypertension [(Adj. OR: 2.95 (95%CI: 1.02, 8.52)], having two or more comorbidities [Adj. OR: 6.38 (955CI: 1.37, 29.62)] and those who had regular treatment for hypertension [Adj. OR: 14.51 (95%CI: 1.46, 44.21)]. Whereas, among hypertensive women in the adjusted model, control rates were positively associated with race whereas the non-Malay had more controlled status compared to Malay [Adj. OR: 5.94, (95%CI: 1.26, 28.09)] and those who regularly see the health professional [Adj. OR: 5.68 (95%CI: 1.94, 16.63)].

Table 3: Factors associated with control hypertension among individuals with hypertension
Discussion
This study found the prevalence of hypertension control among B40 groups with hypertension was 33.8% (95%CI: 29.5, 38.1). However, the prevalence was lower compared to the Malaysian population in 2019 which was 45.0% [23] and a study among the adult Iranian population which was 38.9% of the treated patients [24]. The prevalence of hypertension control in men was lower than in women (33.1% vs 34.0%). However, the Malaysia NHMS 2019 found the prevalence of hypertension control in men was higher compared to women (39.3% vs 35.7%) [10]. Women were a determinant of control hypertension [24]. Compared to their higher income counterpart, healthy low-income people are more likely to have poor self-reported health and greater health risks and less preventive healthcare [25]. Therefore, a paradigm shift towards care for hypertension in Malaysia is needed beyond the mere prescription of antihypertensive drugs [4].
Among hypertensive men, control rates were positively associated with individuals who received or heard any information about hypertension [(Adj. OR: 2.95 (95%CI: 1.02, 8.52)]. Surprisingly, 31.5% of men did not receive any information about hypertension. It could be related to the awareness of hypertension at the beginning. In Malaysia NHMS 2019 found the prevalence of awareness of hypertension was 50.0% [23] and a study by Annamalai, Govindaraja C. [26] found the awareness towards hypertension among estate workers was only 39%. A quantitative study by Khatib, Schwalm [27] concluded that lack of knowledge was the most common barrier to hypertension awareness. Therefore, an intervention should be done to raise public awareness about hypertension and to improve hypertension control under the supervision of a physician [24].
There were many studies have been conducted and concluded that hypertensive patients with multiple risk factors are more difficult to treat and require treatment with multiple antihypertensive drugs [28]. However, this study found those who had multiple comorbidities were associated with better hypertension control [Adj. OR: 6.38 (955CI: 1.37, 29.62)]. Hypertension frequently coexists with obesity, diabetes, hyperlipidaemia, or metabolic syndrome and their association with cardiovascular disease (CVD) is well established [28]. Therefore, patients with multiple comorbidities are likely to require combination therapy to prevent target organ damage (TOD) [29]. These are one of the reasons why those with more co-morbidities are associated with hypertension control.
In Malaysia NHMS 2019 reported that there were 89.4% of those who aware of hypertension had treatment for hypertension [23] which was higher compared to the study among the adult Iranian population which was 71.5% [24]. In adult patients. In most adult patients, two or more medications with complementary mechanisms of action should be used in combination [30]. This study found that those who had regular treatment with the antihypertensive drug for hypertension had better hypertension control compared to those who did not on regular treatment for hypertension [Adj. OR: 14.51 (95%CI: 1.46, 44.21)]. Therefore, an intervention needs to be highlighted to take an account how Malaysian hypertensive patients seek care treatment across different services such as private and public sectors and from western to various traditional practitioners [31]. Support care in social, environmental and financial must be addressed to achieve the full benefits of treatment and control of hypertension [30].
Among hypertensive women, control rates were positively associated with those who regularly see the health professional [Adj. OR: 5.68 (95%CI: 1.94, 16.63)]. During regular consultation, it is not just to monitor blood pressure, the adverse drug effects can be identified early and managed promptly to address patient safety and adherence [30]. In Malaysia, any stable patients will have their follow-up at Health Clinic rather than a hospital for their chronic non communicable diseases treated by the family medicine specialist. Therefore, implementing a family medicine specialist program is recommended in the health system [26]. Hypertension clinics in government hospitals are often overwhelmed by the number of patients, so health professionals have little time to engage effectively with patients [31]. Therefore, the Ministry of Health Malaysia needs about 8,000 family medicine specialists to be placed in its clinics, especially in rural areas to serve the community through master’s programs at local universities and parallel pathway training programs in collaboration with colleges abroad [32].
In Malaysia NHMS 2019 found that Chinese respondents had better hypertension control compared to Malay (46.8% vs 33.2%) [10]. However, in this study, only women found that non-Malay significantly controlled better compared to Malay (75.0% vs 32.5%) but not in men respondents. It could be related to the awareness of the respondent’s status on hypertension where 13.4% (95%CI: 11.86, 15.11) of adult Malay women was unaware that they are having hypertension which was among the highest percentage compared to other races in Malaysia [10]. A study by Shah, Rosenberg [33] also found that Malay was the highest percentage of undiagnosed hypertension and uncontrolled among the older population in Selangor. Applying cultural beliefs and combining modern and Chinese traditional medicines make Chinese respondents have better hypertension control compared to other races in Malaysia [34].
Malaysia has developed a National Strategic Plan for Non Communicable Diseases (NSPNCD 2016-2025). It is a medium-term strategic plan to further strengthen the NCD prevention and control program mostly to reduce the burden of the three types of NCDs i.e. cardiovascular disease (CVD), diabetes and cancer [35]. The healthcare provider also needs to address both the supply (healthcare services) and demand (behaviour of patients) for the continuum of NCD care [5]. Appropriate care must take an account the patient’s modifiable health system barriers for effective hypertension control [31]. It involves the relationship between the healthcare delivery system, healthcare provider and patients, economic, psychosocial, and recognising patient’s educational status and residentials [36].
Conclusion
Health education and promotion programs need to be conducted to disseminate more information about hypertension to the community. Clinical services need to be improved mostly on regular follow up, giving proper consultation on treatment and treating patients to increase the prevalence of hypertension control.
Abbreviation
CVD: cardiovascular disease; CVRN: Cardiovascular Research Network; DBP: Diastolic Blood Pressure; HIV: Human Immunodeficiency Virus; NCD: non-communicable diseases; NHANES: Third National Health and Nutrition Examination; NHMS: National & Health Morbidity Survey; OR: Odds Ratio; NSPNCD: National Strategic Plan for Non-Communicable Diseases; RESPOND: Responsive and Equitable Health Systems – Partnership on Non-communicable Diseases; SBP: Systolic Blood Pressure; TOD: Total Organ Damage;
Acknowledgement:
We would like to thank all respondents who participated in this study.
Author’s contributions:
Conceptualization, M.R.I, N.M.N, F.A, M.M.Y; Methodology, F.A; data collection, N.M.N, M.M.Y, F.A.M; data analysis: M.R.I; Writing-original draft preparation, M.R.I, N.M.N, F.A, M.M.Y; Writing-review and editing, M.R.I, N.M.N, F.A, M.M.Y; supervision, B.P and M.M; All authors have read and agree to the published version of the manuscript.
Funding:
This study has been funded by the Welcome Trust Welcome Trust. The research protocol addressed key principles set out in Welcome Trust guidance notes on conducting ethical research involving people in low- and middle-income countries.
Declarations:
Ethics approval and consent to participate: Ethical approval was provided by the National Medical Research Register, the Research Ethics Committees at LSHTM (Ref: 12214) and Universiti Teknologi MARA (600-IRMI(5/1/6) REC/313/18). We followed the Ethical Guidelines for good research practice of the Association of Social Anthropologists of the UK and the Commonwealth (ASA) (Association of Social Anthropologists, 2011).
Consent for publication:
Not applicable
Competing interests:
All authors declare that they have no competing interests.
References
Whelton, P.K., (1994). Epidemiology of Hypertension. The Lancet. 344(8925): p. 101-106.View
Ezzati, M., et al., (2008). Trends and cardiovascular mortality effects of state-level blood pressure and uncontrolled hypertension in the United States. Circulation. 117(7): p. 905 914.View
Banner Health Understanding High Blood Pressure In Men. 2019.View
Yusoff K., et al., (2021). Hypertension control: lessons from Malaysia, an upper-middle-income country. J Cardiol Curr Res, 14(4): p. 69-73.View
International Trade Administration Malaysia Healthcare Non communicable Diseases. 2022. View
Fisher-Naomi, D.L. and G. Curfman, (2018). Hypertension - A Public Health Challenge of Global Proportions. JAMA. 320(17): p. 1757-1759.View
Centers for Disease Control and Prevention Getting Blood Pressure Under Control. 2012.View
Matsuda, M. and I. Shimomura, (2013). Increased oxidative stress in obesity: Implications for metabolic syndrome, diabetes, hypertension, dyslipidemia, atherosclerosis, and cancer. Obesity Research & Clinical Practice, 7(5): p. e330–e341.View
Daugherty, S.L., et al., (2011). Age Dependent Gender Differences in Hypertension Management. Journal of Hypertension, 29(5): p. 1005–1011.View
Institute of Public Health National Health and Morbidity Survey 2019. Technical Report. NCDs - Noncommunicable diseases: Risk factors and other health problems. 2019.View
Ong, K.L., et al., (2007). Prevalence, Awareness, Treatment, and Control of Hypertension Among United States Adults 1999–2004. Hypertension, 49(1): p. 69-75.View
Wenger, N.K., et al., (2018). Hypertension Across a Woman’s Life Cycle. J Am Coll Cardiol., 71(16): p. 1797–1813.View
Vasan, R.S., et al., (2002). Antecedent blood pressure and risk of cardiovascular disease: the Framingham Heart Study. Circulation, 105: p. 48–53.View
Turner, S.T., et al., (2010). Plasma renin activity predicts blood pressure responses to beta-blocker and thiazide diuretic as monotherapy and add-on therapy for hypertension. Am J Hypertens, 23: p. 1014–1022.View
Hamadeh, I.S., et al., (2014). Impact of CYP2D6 polymorphisms on clinical efficacy and tolerability of metoprolol tartrate. Clin Pharmacol Ther, 96: p. 175-181.View
August, P., (1999). Hypertension in Men. The Journal of Clinical Endocrinology & Metabolism, 84(10): p. 3451-3454.View
Mendelsohn, M.E. and R.H. Karas, (1999). The protective effects of estrogen on the cardiovascular system. N Engl J Med, 340: p. 1801–1811.View
Ong, K.L., et al., (2008). Gender Difference in Blood Pressure Control and Cardiovascular Risk Factors in Americans With Diagnosed Hypertension. Hypertension, 51(4): p. 1142-1148.View
Health Poverty Action Essentials for Health. 2018.View
Dept of Statistics Malaysia. Population distribution and basic demographic characteristics (2000). [cited 2021 30th December]; Available from: https://www.mycensus.gov.my/index.php/ census-product/publication/census-2000/650-population distribution-and-basic-demographic-characteristics-2000 View
Palafox, B., et al., (2018). Responsive and Equitable Health Systems-Partnership on Non-Communicable Diseases (RESPOND) study: a mixed-methods, longitudinal, observational study on treatment seeking for hypertension in Malaysia and the Philippines. BMJ Open, 8(7): p. e024000.View
Chow, C.K., et al., (2013). Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. Jama, 310(9): p. 959 68.View
Institute of Public Health National Health and Morbidity Survey (2019). Non–communicable diseases, healthcare demand, and health literacy. Key Findings. 2019. National Institutes of Health, Ministry of Health.View
Mirzaei, M., et al., (2020). Awareness, treatment, and control of hypertension and related factors in adult Iranian population. BMC Public Health, 20: p. 667.View
The Commonwealth Fund Why Even Healthy Low-Income People Have Greater Health Risks Than Higher-Income People. 2018.View
Annamalai, C., Govindaraja C., and C. Chandramouli, (2011). Prevalence, awareness and control of hypertension in estate workers in Malaysia. North American Journal of Medical Sciences, 3(12): p. 540-543.View
Khatib, R., et al., (2014). Patient and healthcare provider barriers to hypertension awareness, treatment and follow up: a systematic review and meta-analysis of qualitative and quantitative studies. PLoS One, 9(1): p. e84238.View
Petrie, J.R., T.J. Guzik, and R.M. Touyz, (2018). Diabetes, Hypertension, and Cardiovascular Disease: Clinical Insights and Vascular Mechanisms. Canadian Journal of Cardiology, 34: p. 575-584.View
Schmieder, R.E. and L.M. Ruilope, (2008). Blood Pressure Control in Patients With Comorbidities. The Journal of Clinical Hypertension, 10(8): p. 624-631.View
Mensah, G.A. and G. Bakris, (2010). Treatment and control of high blood pressure in adults. Cardiol Clin., 28(4): p. 609-622.View
Risso-Gill I, et al., (2015). Understanding the modifiable health systems barriers to hypertension management in Malaysia: a multi-method health systems appraisal approach. BMC Health Services Research, 15: p. 254.View
Free Malaysia Today 8,000 family medicine specialists needed at govt clinics, says DG. 2022.View
Shah, S.-A., et al., (2022). Prevalence and determinants of unmet needs for hypertension care among the older population in Selangor: cross-sectional study. Health Research Policy and System, 20(Suppl 1): p. 127.View
Chew, K.S., T.W. Tan, and Y.T. Ooi, (2011). Influence of Chinese cultural health beliefs among Malaysian Chinese in a suburban population: a survey. Singapore Med J, 52(4): p. 252-256.View
Ministry of Health Malaysia, National Strategic Plan for Non-Communicable Disease. Medium Term Strategic Plan to Further Strengthen the NCD Prevention and Control Program in Malaysia (2016-2025). 2016: Putrajaya.View
Yusoff, K., et al., (2021). Hypertension control: lessons from Malaysia, an upper-middle-income country. Journal of Cardiology & Current Research, 14(4): p. 69-73.View