
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 7 (2023), Article ID: JPHIP-220
https://doi.org/10.33790/jphip1100220Research Article
The Use of Wearable Devices as a Self-Help Approach to Wellness Promotion, Overcoming Health Disparities and Reducing Medical Distrust Among African Americans
Andre L. Hines1*, Lena Jones1, Candis Pizzetta1, Girmay Berhie1, Alfred A. Cecchetti2, Fidelis Ikem1, Mario Azevedo1, Edith Davidson1, Monique White1, Sheila Malone1
1Department of Public Health, Jackson State University, United States.
2Department of Clinical and Translational Sciences, John C. Edwards School of Medicine, Marshall University,United States.
*Corresponding Author Details: Andre L. Hines, PhD, Associate Professor, Department of Health Care Management, Jackson State University, United States.
Received date: 26th April, 2023
Accepted date: 14th November, 2023
Published date: 16th November, 2023
Citation: Hines, A.L., Jones, L., Pizzetta, C., Berhie, G., Cecchetti, A. A., Ikem, F., Azevedo, M., Davidson, E., White, M., & Malone, S., (2023). The Use of Wearable Devices as a Self-Help Approach to Wellness Promotion, Overcoming Health Disparities and Reducing Medical Distrust Among African Americans. J Pub Health Issue Pract 7(2): 220.
Copyright: ©2023, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Introduction
Wearable health technologies, ranging from smartwatches to fitness trackers, have developed as promising tools in health self management and disease prevention. Offering real-time monitoring, feedback, and data analytics, these devices are bridging the gap between patients and healthcare providers, potentially leading to early interventions, better patient outcomes, and heightened user engagement in personal health management. Devices like smartwatches and fitness trackers offer users real-time monitoring and analysis of various health parameters. These devices hold the promise of transforming patient engagement and empowerment and have potential implications for the broader public health landscape.
However, as is often the case with rapid technological advancements, there is a dichotomy of access. Despite their transformative potential, wearable devices highlight a persistent concern in the world of public health: the issue of equity. The question of who has access to these technologies and how they are utilized is as much about socioeconomic determinants as technological adoption. For historically marginalized communities, especially African Americans, this question becomes even more complex due to. Medical mistrust stemming from deep rooted systemic inequities and unethical practices, which could influence community members’ perspectives on modern medical technologies. Especially the African American population, in underserved areas, may not uniformly benefit from the advantages offered by wearables due to various socio-economic, educational, and trust-related barriers.
This study, conducted in Mississippi, investigates perceptions, knowledge, and usage patterns of wearable devices among African American clergy and students at a major Historically Black College and University (HBCU). Chosen for their influential roles in the community and potential as active technology users, these groups reflect the unique sociocultural dynamics of the region. Given their pivotal role in offering guidance and support, churches in African American communities are key to understanding technology adoption.
The students at the HBCU, provide insight into the next generation's perspectives, inherently influenced by a more digital, connected world. This exploration aims to answer vital research questions concerning knowledge about the health benefits of wearables, attitudes toward data collection and sharing, and actual usage patterns among the target population. Our objectives include understanding the factors that influence the adoption of wearable technology in these communities, assessing the level of trust in these devices, and examining how wearable technology can contribute to self-managed healthcare. By exploring these aspects, the study seeks to provide insights into the potential of wearable devices as a tool for enhancing health outcomes and reducing medical distrust in African American populations.
The survey questions tap into deeper themes highlighted in our literature review. Our review encompasses the potential of consumer wearables in healthcare, disparities in access and usage, and the historical context of African Americans' interactions with the medical establishment, a history riddled with mistrust and misgivings. By framing the adoption of wearable technology within these historical, cultural, and socioeconomic dynamics, the study seeks to provide comprehensive insights, particularly for underserved populations in Mississippi.
The findings from this research aim to inform public health initiatives and policy, highlighting areas for intervention to ensure equitable benefits from technological advancements in healthcare. Understanding the influences shaping the attitudes and behaviors of African Americans towards wearable health technologies, this study informs strategies that cater to their unique needs and concerns, promoting broader adoption and better health outcomes.
Mississippi's socioeconomic profile, characterized by a high poverty rate and lower median household income compared to the national average. In 2021, Mississippi had a population of 2.97 million people with a median age of 37.8. Between 2020 and 2021, like other distressed areas, it witnessed a population decline (0.497 percent), and approximately one in five residents’ lives below the poverty line [1,2]. Although its median household income grew from $46,511 to $49,111, representing a 5.6 percent increase, it was still only two-thirds of the national average, which stands at $69,021 with an annual growth of 6.2 percent [3].
In Mississippi, where African Americans constitute over a third (37.8%) of the population, the economic challenges are particularly acute [1]. This is especially true for many African American residents working in blue- and pink-collar sectors, where pursuing higher education often represents a pathway out of subsistence living. Reflecting this, at Jackson State University—the HBCU from which study participants were drawn—89% of its 7920 students received need-based assistance in 2021 [4]. These disadvantages underscore the importance of this research in understanding the complex interplay of societal roles, generational perspectives, and historical contexts in the adoption of wearable technology among African American communities.
Discussion
The COVID-19, pandemic, has unexpectedly increased the popularity and use of e-health technology, especially smartwatches for self monitoring health. Prior to this, there was and continues to be a critical interest in improving health outcomes related to obesity, hypertension, and diabetes [5-9]. These cardiovascular risk factors disproportionately affect low-income populations in general and people of color in particular across the nation. For various reasons, these groups are less likely to achieve recommended levels of physical activity and respond favorably to other counteracting measures to avoid more extreme consequences, such as stroke, eyesight failure, dialysis, and limb amputation [10].
Smartphones and their health applications can serve as digital early detection tools, alerting owners of internal health risks and preventing such issues from escalating. This is a particularly useful advantage in efforts to mitigate health disparities among racial and ethnic minorities, as they have a greater tendency to own such devices [11].
In their study of mobile and wearable technology among student athletes in Lebanon, Bardies et al. [12] provided a fundamental justification for the dearth of research regarding this population in non-Western, less prosperous countries. Our study seeks to fill a similar void by gauging the familiarity with and ownership of wearable devices among African American religious leaders and HBCU students in Mississippi. Mississippi is a state distinguished by its pervasive and persistent poverty, resulting. In a growing number of medically underserved individuals disproportionately affected by higher rates of morbidity and mortality, aggravated by health disparities [13].
This research focuses on the potential of wearable devices to have beneficial impacts on personal and congregational outcomes among African American faith-based leaders and HBCU students. Exploring the degree of acceptance within the African American educationally inclined population, the study also examines their health-oriented motivation for owning wearable devices. Despite mixed evidence regarding the broad acceptance and use of smartwatches [8], our mixed-method approach targets these specific groups, considering the significant influence of churches in Black life and culture.
From slavery to freedom, the Black Church has been a recognized source of hope and healing for congregational members and the larger African American community. Available evidence indicates many worship centers with predominantly Black congregations have health outreach ministries in partnerships with public health agencies and private providers and are engaged in activities devoted to preventive health and grief counseling along with special social services to at risk populations [14-17].
This study focused on religious affiliation, considering Mississippi's high level of religiosity—tied with Alabama as the most religious state, where 77% of residents are highly religious [18]. Religious involvement varies among different populations, with African Americans and women generally more engaged in religious practices [19]. The Pew Research Center reports notable differences in religious beliefs and practices between African Americans and Whites: 94% of African Americans believe in God (compared to 81% of Whites), 83% attend religious services at least monthly (compared to 66% of Whites), and 86% pray weekly (compared to 68% of Whites) [20]. These distinctions underscore the potential effectiveness of health promotion programs led by African American faith-based leaders.
This study aimed to assess and compare the familiarity with and ownership of wearable devices among students and faith-based leaders. The hypothesis was that students, primarily Generation X (born 1965-1980), Generation Y (1981-1996), and partially Generation Z (1997-2012), in the Information Age and were more familiar with digital devices but were less likely to own them due to affordability factors. Conversely, faith-based leaders, mainly Baby Boomers (born mid-1940s to mid-1960s), were expected to have less difficulty affording smart devices but were likely more hesitant to adopt new digital technologies.
Research conducted nationally indicates that people of color and women are the more likely owners of dual-use health monitoring tools, such as smartwatches [11]. Part of their appeal is that these devices offer continuous monitoring of physical activity, heart rate, sleep patterns, safety alerts, and more. However, there is a paucity of research regarding how effective feedback derived from wearable devices is in promoting healthy lifestyle choices and preventing serious illness [21]. Also, little is known about the factors driving the adoption of smartwatches by students to monitor their health rather than to serve as a trendy gadget. Even rarer still is research pertaining to potential adult owners of wearable devices involving future professionals (students) and existing community influencers (faith-based leaders) in Mississippi and how these devices are and can improve health outcomes and bridge the trust gap between healthcare providers and their patients.
To help shed light on these uncertainties, we used self-reported data to gauge the prevalence of ownership and use of smart devices and townhall engagements where adult students and community leaders freely expressed their use (or non-use) of wearable devices, how they relied on them (or not) as a health monitoring tool, and what concerns, if any, they had regarding privacy compromises and medical distrust.
We did so using surveys and town hall meetings, with the results analyzed using a logistic regression model to identify social factors (gender, race/ethnicity, education, income, and denomination) that could play a possible role in faith-based leaders’ tendency to own and promote the use of such devices. Although lower economic status and reduced education would suggest a similar pattern of inequality driving the ownership of personal wearable devices, consistent with Pew findings [11]. we found this was not the case; interestingly, a comparable cohort, African American students, overwhelmingly owned one or more, such self-monitoring devices while generally older, faith-based community leaders expressed a greater appreciation for standard watches but immediately expressed favorable acceptance of smartwatches once other audience members expressed their usefulness as group fitness promoters and preliminary indicators of certain health disorders.
There are multifactorial causes of health disparities among African Americans compared to other groups. However, while some barriers to better health are structural and require a more just society, many risk factors are modifiable. Research indicates that a harmful lifestyle consisting of poor eating habits, poor nutrition, and physical inactivity are major risk factors for chronic diseases that unevenly affect some population groups more than others. As many African American churches in Mississippi have adopted formal health ministries and wellness programs, it made much practical sense to explore the mindset of leaders relative to wearable devices.
Methods
The study design involved a cross-sectional survey conducted among African American clergy and students at a Historically Black College and University (HBCU) in Mississippi. The participants were chosen to reflect the unique sociocultural dynamics of African American communities in the region. To ensure a representative sample, the selection process included consultations with experts to align the final selections with the religious diversity of the state and the nine health districts defined by the Mississippi State Department of Health.
The basic criteria governing selection was that participants had to be active leaders in their faith community, irrespective of their race or ethnicity. Consequently, while most participants were African American, the group included a few were White clergy assigned to Catholic churches located in African American communities.
Most faith-based leaders selected represented Pentecostal and Protestant denominations, specifically the Church of God, Church of God in Christ, Baptists, and Methodists. These denominations reflect the breakdown in the Pew Research Center [20] survey “Religious Landscape Study: Blacks in Mississippi.” The final participants included in the townhall forums and individual surveys were a balanced mixture of adult African American men and women who may or may not have been the senior ministers at their worship centers but were the acknowledged leaders in their respected congregations.
Survey instruments included questionnaires designed to gather data on perceptions, knowledge, and usage patterns of wearable devices. The questionnaire comprised multiple-choice and Likert scale questions, addressing topics such as trust in technology, health benefits, and data privacy concerns. The participants' responses were anonymized and confidential.
Data analysis was conducted using SPSS version 28.0.1.1. A logistic regression model was employed to analyze the data, with a significance level set at p ≤ 0.05. The analysis aimed to identify social factors (gender, race/ethnicity, education, income, denomination) influencing the adoption and use of wearable technology. In cases where low expected cell frequencies were encountered, Fisher's Exact Test was used to ensure accuracy in the findings.
For studies involving human participants, ethical approval was obtained from the Institutional Review Board (IRB) of Jackson State University. Informed consent was obtained from all participants prior to their participation in the study. The research adhered to ethical standards for human subject research, ensuring the confidentiality and anonymity of the participants.
Results
Missing Church 22/276 = 7.97%, Missing Student 29/239 = 12.13%. Actual Analysis will include 254 Church members and 210 students, or 464 combined subjects (Table 1).
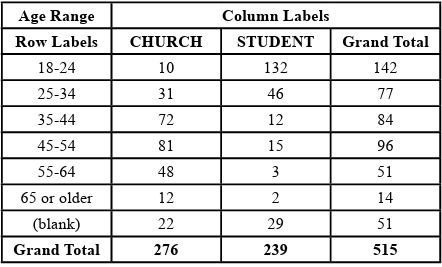
Table 1: Breakdown of students and church members by age groups
The data is divided into church and student groups. Questions 1 to 13 (Table 2) provided five possible responses (agree, disagree, neutral, strongly agree, strongly disagree) with age groups of 18-24, 25-34, 35-44, 45-54, 55-64, and 65 and older. This analysis compared the responses given by each age group to each other with questions that focused on trust issues concerning wearable technology.
Question 1, “I use controls provided by my wearable device to restrict data collected through the device.”, the 18-24, 25-34, and 35 44 age groups were significantly different (p=.026, p< 0.001, P < 0.001, respectively)
When analyzing the clergy and students in the younger age groups, from 18 to 44, variations emerge in their utilization of controls to limit data access. Conversely, those in the older age groups, aged 45 to 65 and beyond, report consistent findings.
Question 2, “If it improves my health, I am willing to share data from my wearable device with healthcare professionals (e.g., doctors, nurses, etc.).” The ages groups 25-34 and 35-44 significantly differed (p=0.041 and p=.007). All other age groups were not significant.
When examining the clergy and students in the younger age groups, precisely 25 to 44, distinctions become evident in their willingness to authorize the sharing of collected data with healthcare professionals. In contrast, those in the younger 18-24 age groups and individuals aged 45 and older present similar findings.
Question 3, “If it will improve my health, I am willing to share data obtained from my wearable device with other device users.” The age groups 18-24, 35-44, 45-54, and 65 or older were significantly different (p=.003, p=0.018, p=0.14 and p=.042, respectively).
When assessing the perspectives of clergy and students within the age groups 18-24, 35-44, 45-54, and 65 or older, variances arise in their readiness to allow the sharing of collected data with other device users. In contrast, those in the younger 25 to 34 age groups express similar findings.
Question 4, “If it will improve my health, I am willing to share data obtained from my wearable device with family and friends that I choose.” only the age group 35-44 was significantly different(p=.006).
When examining the clergy and students across the age groups 18-24, 25-34, 45-54, 55-64, and 65 and older, there is a unanimous consensus in their willingness to allow the sharing of collected data with family and friends. Conversely, within the younger 35-44 age group distinctions emerge between the attitudes of clergy and students regarding their inclination to share data with their family and friends.

Table 2: Survey Questions and Variable Names Used in SPSS
Question 5, “I believe that manufacturers of wearable health devices have a way to ensure the safe handling of my personal information.” only the age group 35-44 was significant (p=.021).
When evaluating the perspectives of clergy and students across the age groups 18-24, 25-34, 45-54, 55-64, and 65 and older, there is a consistent agreement in their faith that manufacturers of health devices possess means to secure the responsible management of personal data. In contrast, within the younger 35 to 44 age range, variances become evident between the convictions of clergy and students concerning the manufacturers' capacity to guarantee the safe handling of personal data derived from wearable devices.
Question 6, “I believe that the manufacturers of wearable health devices will not pass on my personal information to unauthorized third parties without my consent.” only the age group 35-44 was significant (p=.001).
When examining the clergy and students across the age groups 18-24, 25-34, 45-54, 55-64, and 65 and older, there is a unanimous consensus in their trust that manufacturers will not share personal information with unauthorized third parties without consent. Conversely, within the younger 35-44 age group distinctions arise between the beliefs of clergy and students regarding the manufacturers' commitment to not divulging personal information to unauthorized third parties without consent.
Question 7, “I feel that I can trust the data obtained from wearable health devices.” only the age group 35-44 was significant (p=.002).
When analyzing the clergy and students across the age groups 18-24, 25-34, 45-54, 55-64, and 65 and older, there is a uniform consensus in their confidence regarding the reliability of data gathered from wearable health devices. On the contrary, within the younger 35 to 44 age range, disparities emerge between the trust levels of clergy and students concerning the data derived from wearable health devices.
Question 8, “I feel I can depend on wearable health devices to provide me with reliable information.”, only the age group 35-44 was significant (p=.002).
When assessing the perspectives of clergy and students across the age groups 18-24, 25-34, 45-54, 55-64, and 65 and older, there is a consistent agreement in their trust that wearable health devices can deliver reliable information. Conversely, within the younger 35-44 age range, there are discernible distinctions between the views of clergy and students regarding their confidence in wearable health devices to furnish them with dependable information.
Question 9, “I believe that data from wearable devices cannot be easily hacked or compromised.” only the age group 35-44 was significant (p=.004).
When examining the clergy and students within the age brackets of 18-24, 25-34, 45-54, 55-64, and 65 and older, there is a uniform consensus that data from wearable devices is not easily susceptible to hacking or compromise. Conversely, the 35-44 age group among the younger population highlights distinctions in the beliefs of clergy and students regarding the security of data from wearable devices.
Question 10, “I believe that the wearable device can not cause serious health issues.” only the age group 35-44 was significant (p=.011).
The comparison between the clergy and students in the age groups 18-24, 25-34, 45-54, 55-64, and 65 and older shows no difference in their belief that the wearable device can not cause serious health issues. Those in the younger 35 to 44 age groups report differences between clergy and students in their belief that wearable devices can not cause serious health issues.
Question 11, “Everyone in my community has access to all available health-related resources to be as healthy as possible regardless of economic status.” The age groups 18-24,25-34,35-44,45-54, and 55 64 were significantly different (p=.004, p=.009, p< 0.001, p< 0.001, p=0.030 respectively). The 65 or older group was not significantly different.
When comparing clergy and students across age groups 18-24, 25-34, 45-54, and 55-64, it is evident that they share a common belief: not everyone in their community has access to all available health-related resources. However, those clergy and students aged 65 or older express no variance in their belief that everyone in their community can access such resources.
Question 12, “If a wearable device allowed for data to be collected regarding the health status of my community, I would willingly provide this information.” The age group 25-34 was significantly different (p=0.021). All the other age groups were not significantly different.
The analysis of beliefs regarding sharing health-collected data within the age groups 18-24, 45-54, 55-64, and 65 and older reveals no discernible distinction between clergy and students. However, clergy and students in the 25-34 age category exhibit varying perspectives on sharing health-collected data with their community.
Question 13,” I would encourage others to share wearable data to improve the health status of our community.” The age group 25-34 was significantly different (p=0.050). All the other age groups were not significantly different.
There is no distinction in the belief regarding advocating for the sharing of wearable data to enhance community health status between clergy and students across age groups 18-24, 45-54, 55-64, and 65 and above. However, clergy and students in the 25-34 age bracket exhibit varying beliefs in encouraging others to share wearable data to improve community health.
Questions 1, 2, and 13 revealed disparities primarily within the younger clergy and student demographics concerning the implementation of data control measures. On the other hand, Questions 4 to 10 and 12 displayed notable variations in response patterns between clergy and students, specifically within the 35-44 age bracket. This age group appears to exhibit a pronounced lack of trust. In contrast, Questions 3 and 11 exhibited a more widespread array of discrepancies across multiple age groups. In general, the 35-44 age group consistently demonstrated dissimilar responses compared to other age groups for most questions, indicating a disagreement between students and clergy.
The sample size of this population is small, with some expected frequencies falling below 5. Minor expected cell frequencies suggest the test may not accurately reflect the underlying population distribution. There is also an increased risk of Type II errors, which may incorrectly conclude that there is no significant relationship when there is one. In this paper, the analysis used the Fisher's Exact Test when low expected cell frequencies were found.
Conclusion
Given the growing acceptance of consumer wearables in the medical field, wearable devices will play an important role in providing real time data to objectively monitor patients at home [22]. These devices will be especially important for improving the health and control of chronically ill patients with conditions like asthma, COPD, diabetes, and cardiovascular disease as well as monitoring infectious diseases. One of the goals of this study was to understand the motivations fueling African Americans' use of consumer wearables. The results suggest that strengthening the trust of African Americans could lead to increased use of consumer wearables among this population, potentially helping to address. Health disparities and support positive outcomes among African Americans.
Residents of more impoverished areas generally experience poorer health and shorter lifespans. Emerging technologies such as wearable devices and smartphone applications for activity tracking have generated new opportunities for promoting healthy lifestyles across diverse patient groups. Wearable devices are increasingly affordable and owned by a broad spectrum of society, spanning various age groups. Once seen as fashion accessories for younger generations, smartwatches are now widely used across all age groups for various purposes, including health management. Of interest to this study, however, is their potential for improving health outcomes, reducing disparities, and decreasing medical mistrust.
The paradigm shift in healthcare delivery services toward a more patient-centered model globally has emphasizes the medical consumer as a key member of the healthcare team. Consumer wearables, when used as self-monitoring health devices, enhance a patient’s ability to collect, store, and retrieve data reflecting diagnostic trend patterns and real-time accuracy.
Cognizant that the Information Age and the accompanying digital revolution have resulted in a more technologically savvy society, the goal of this research was to explore the usefulness of wearable devices among high-risk groups to promote a stronger culture of wellness and eliminate barriers, such as access to care and medical distrust, which can contribute to significant disparities in health outcomes.
There is a notable gap in research focusing on whether the racial gap that exists for healthcare also exists for technologies utilized in digital healthcare. This research contributes to further understanding those factors that fuel African Americans use of consumer wearables and the purposes for which they are used. Additional research is needed to ensure the health benefits attainable through consumer wearables are available to and utilized by minority and socially and economically disadvantaged populations for the promise of reduction of health disparities to be fully realized.
Acknowledgement:
This project was funded by the W. K. Kellogg Foundation, which was instrumental in the realization of this project. Their commitment to fostering research and innovation has enabled us to conduct this important study.
Statement of Competing Interests:
The authors of this manuscript, titled "The Use of Wearable Devices as a Self-Help Approach to Wellness Promotion, Overcoming Health Disparities and Reducing Medical Distrust Among African Americans," hereby declare that there are no competing interests regarding the publication of this paper. This includes any financial, personal, or professional interests that could be construed to have influenced the work.
References
US Census. (2021). Quick facts: Mississippi. Retrieved February 16, 2023.View
DATAUSA. (2021). Mississippi. Retrieved from https://datausa. io/profile/geo/mississippiView
DATAUSA. (2022). United States.View
Jackson State University. (2021). Admission & Aid.View
Mohammed, A. M., Adda, M., Bouzouare, A., & Ibrahim, H. (2022). Machine learning and smart devices for diabetes management: Systemic review. Sensors, 1843, 24.View
Wang, W., Cheng, J., Song, W., & Shen, Y. (2022). The effectiveness of wearable devices as physical activity interventions for preventing and treating obesity in children and adolescents: Systemic review and meta-analysis. JMIR Mhealth Uhealth, 10(4), 332435.View
Rodriquez-Leon, C., Villalonga, C., Munoz-Torres, M., Ruiz, J., & Banos, O. (2021). Mobile and wearable technology for monitoring diabetes-related parameters: Systemic review. JMIR Mhealth Uhealth, 9(6), e25138.View
Claudel, S. E., et al. (2020). Time to listen: A mixed-method study examining community-based views of mobile technology for interventions to promote physical activity. BMJ Health & Care Informatics, 27, e00140.View
Hamasaki, H. (2018). Efficacy of wearable devices to measure and promote physical activity in the management of diabetes. European Medical Journal: Diabetes, 6(1), 62–69.View
Olanlesi-Aliu, A., Alaazi, D., & Salami, B. (2023). Black health in Canada: Protocol for a scoping review. JMIR Research Protocols, 12, e42212.View
Vogels, E. A. (2020). About one in five Americans use a smartwatch or fitness tracker. Pew Research Center.View
Bardies, M., Vorgi, C., El-Harakeh, M., Gherbal, T., Kharroubi, S., & Elie-Jacques, F. (2021). Exploring the use of mobile and wearable technology among university student-athletes in Lebanon: A cross-sectional study. Sensors, 21(4472), 17.View
Carratala, S., & Maxwell, C. (2020). Fact sheet: Health disparities by race and ethnicity. Retrieved from https://www. americanprogress.org/article/health-disparities-race-ethnicity/View
Sutherland, M., & Hale, C. (1994). Community health promotions. Journal of Primary Prevention, 16, 201–216.View
Brewer, L. C., & Williams, D. R. (2019). We've come this far by faith: The role of the Black Church in public health. American Journal of Public Health, 109(3), 385–386.View
Markens, S., Fox, S. A., & Taub, B. (2002). Role of Black churches in health promotion programs: Lessons from the Los Angeles Mammography Promotion in Churches Program. American Journal of Public Health, 92(5), 6.View
Baskin, M. L., Resnicow, K., & Campbell, M. K. (2001). Conducting health interventions in Black churches: A model for building effective partnerships. Ethnicity & Disease, 11(4), 823–833.View
Pew Research Center. (2014). Religious landscape study: Religious composition of adults in Mississippi. Retrieved from https://www.pewresearch.org/religion/religious-landscape study/state/mississippi/View
Majee, W., et al. (2022). Participant perspectives on the effects of an African American faith-based health promotion educational intervention: A qualitative study. Journal of Racial and Ethnic Health Disparities, 10(3), 1125–1126.View
Pew Research Center. (2022). Religious landscape study: Blacks who are in Mississippi. Retrieved from https://www. pewresearch.org/religion/religious-landscape-study/state/ mississippi/racial-and-ethnic-composition/black/View
Li, M., Li, Q., Budhathoki, C., Li, S., & Szanton, S. L. (2022). Factors associated with electronic wearable device use among older adults. Supplement 1, 372.
Greiwe, J., & Nyenhuis, S.M., (2020). Wearable Technology and How This Can Be Implemented into Clinical Practice. Current Allergy and Asthma Reports. 20: 36. https://doi.org/10.1007/ s11882-020-00927-3View