
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 7 (2023), Article ID: JPHIP-221
https://doi.org/10.33790/jphip1100221Research Article
The Effect of Social Isolation Due to the COVID-19 Pandemic on the Mental Health of Geriatric Patients in Outpatient Clinic in Illinois: An Exploratory Pilot Study
Lakshmi Praneetha Vennam1*, Kalyan C. Kandra2, Alice Ma3, Amber S. Fifer4, Vivek Prakash5, and Cedric Harville II3
1Southern Illinois University Edwardsville, 62026, Illinois, United States.
2Psychiatry Faculty, Southern Illinois University School of Medicine, Springfield, 62794, Illinois, United States.
3Assistant Professor, Department of Applied Health, Southern Illinois University Edwardsville, 62026, Illinois, United States.
4Director of Clinical Research, Neuroscience Institute, Southern Illinois University School of Medicine, Springfield, 62794, Illinois, United States.
5Statistical Research Specialist, Center for Clinical Research, Southern Illinois University School of Medicine, United States.
*Corresponding Author Details: Lakshmi Praneetha Vennam, Southern Illinois University Edwardsville, 62026, Illinois, United States.
Received date: 12th October, 2023
Accepted date: 20th November, 2023
Published date: 22th November, 2023
Citation: Vennam, L.P., Kandra, K. C., Ma, A., Fifer, A. S., Prakash, V., & Harville, C., (2023). The Effect of Social Isolation Due to the COVID-19 Pandemic on the Mental Health of Geriatric Patients in Outpatient Clinic in Illinois: An Exploratory Pilot Study. J Pub Health Issue Pract 7(2): 221.
Copyright: ©2023, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
The COVID-19 pandemic contributed to a severe burden on the physical and mental health of people around the globe. It contributed to fear, uncertainty, stress, isolation, and loneliness amongst the geriatric population. These feelings were often higher in people with mental health disorders. Having a prior history of psychiatric disorders can be a risk factor for increased psychological distress after going through any disaster-related traumatic experience. The present exploratory pilot study aimed to understand the adverse effects of social isolation due to the pandemic on geriatric patients’ mental health and awareness of the available resources provided by both government and private agencies, to cope with stress. The study included a questionnaire that was administered to 50 geriatric patients. Descriptive statistics were conducted using Microsoft Excel. The results showed that 56% of the participants reported that their mental health was affected due to the social isolation from the pandemic. Statistical significance (p<0.05) was observed amongst the participants who reported feeling socially isolated and lonely during the pandemic. Worsening of mood, anxiety, sleep disturbances, loss of interest, appetite changes, weight issues, and concentration difficulties were statistically significant. Statistical significance was also observed for symptom worsening compared to the pre-pandemic period and for the awareness of lack of resources. About 60% of participants reported that they were not aware of the resources to cope with stress during the pandemic. The study findings suggest that the mental health of geriatric patients was adversely affected by the social isolation from the COVID-19 pandemic. It is important to focus on the physical and mental health of vulnerable populations, such as geriatric patients, and to carefully monitor them during difficult times including pandemics and other emergency situations.
Keywords: COVID-19 pandemic, Geriatric patients, Mental health, Social isolation, Illinois
Introduction
Newly emerging viral diseases have become a major public health threat around the world in recent years. The most recent and ongoing viral disease, the novel coronavirus (COVID-19), contributed to severe burden on the entire world [1]. Older adults are at high risk for morbidity and mortality due to COVID-19 and, on that basis, are likely to experience prolonged isolation [2]. In communities where “stay-at-home” instructions were imposed, older persons, especially those in residential or long-term care facilities, may be restricted from interacting with spouses, family, and friends who live within or outside these communities [3,4]. Thus, although social isolation during COVID-19 can be lifesaving, it can also deprive older adults of fundamental human needs for companionship and community. Many older adults are less likely to have access to email, social media, or videoconferencing, which have been widely implemented to compensate for the lack of in-person social contacts [4].
Mental health comprises emotional, psychological, and social well being. About 28% of older adults in the United States, or 13.8 million people, live alone, according to a report by the Administration for Community Living’s Administration on Aging of the U.S. Department of Health and Human Services [5]. Older people face unique physical and mental health challenges which need to be recognized, including heart disease, osteoarthritis or osteoporosis, respiratory diseases, vision or hearing loss, risk for some types of cancer, isolation, affective and anxiety disorders, dementia, and psychosis [6]. More than 20% of older people age 60 years and over suffer from a mental or neurological disorder (excluding headache disorders). These disorders in older people account for 17.4% of years lived with disability (YLDs) [7].
Loneliness is often stigmatized, trivialized, or ignored [8]. With the rapidly growing number of older adults in industrialized countries, the increased likelihood of premature mortality, and the deleterious effect of loneliness are emerging as a public health problem. This has been identified in animal models and human longitudinal investigations [9,10]. Loneliness has been associated with objective social isolation, depression, introversion, or poor social skills [8]. Physicians are encountering this condition, but most do not have the information needed to deal effectively with loneliness in their patients [8]. Meta-analyses have found that social isolation or loneliness in older adults is associated with a 50% increased risk of developing dementia [11], a 30% increased risk of incident coronary artery disease or stroke [2,12], and a 26% increased risk of all-cause mortality [12].
Accordingly, the present observational exploratory pilot study aimed to understand the adverse effects of social isolation due to the pandemic on geriatric patients’ mental health and their awareness of the available resources to cope with the stress.
Materials and Methods
To test the effects of social isolation due to the COVID-19 pandemic among geriatric patients, this exploratory pilot study was conducted at Southern Illinois University’s (SIU) psychiatry outpatient clinic in Springfield, Illinois. The Springfield Committee for Research Involving Human Subjects (SCRIHS) and Southern Illinois University Edwardsville (SIUE) approved study protocols. The inclusion criteria included geriatric patients between the ages of 60-89 years with previous psychiatric conditions and visits SIU psychiatry outpatient clinic for follow ups. There was a cover letter to the questionnaire which explained that by completing and returning the anonymous questionnaire, they agreed to participate in the study. The feasibility of using an online survey and a hardcopy survey was assessed by the research team, and found that a hard copy survey would help the participants without any burden. A hardcopy questionnaire about participants’ mental health status was given. They were asked to complete it if they were interested in the survey. The patients who were waiting in the reception area either before or after their appointment were asked to volunteer to answer anonymously to the questionnaire. Patient identifiers were not recorded at any step during the study. The only demographic questions that were included were age, sex, and their living condition (alone in a community, adult care facility, or living with family). The purpose of the study was explained by a study team member and psychiatry residents and assured that personal information would not be recorded. The questions were formulated based on the DSM-5 criteria and Patient Health Questionnaire (PHQ-9). PHQ-9 has shown validity and reliability in content and internal consistency [13,14]. The questionnaire included questions regarding whether the participant experienced any stress, isolation, depression, and other mental health concerns during the lockdown in the last 18 months, with “No” or “Yes” response options (e.g., Were you depressed during the pandemic? [Feeling low or hopeless]) [14,15]. The quality of sleep and level of fatigue were also examined, with “Yes” or “No” response options (e.g., Was your sleep impacted during the pandemic? (Trouble falling or staying asleep, or sleeping too much?) [15]. Participants were asked about their appetite and weight with no change, increase, or decrease response options (e.g., Did your appetite get affected during the pandemic?). Participants were asked if their symptoms worsened compared to before the pandemic with “Yes” or “No” response options. Questions about participants’ awareness of the resources from the state to cope with the stress were also examined, with Yes/ No response options (e.g., Were you aware of resources that you could use to help you with your mental health during the pandemic?).
Data Analysis
Participants’ data were collected and managed using REDCap secure electronic data capture tools [16]. The data were exported into Microsoft’s Excel application for interpretation. All charts and tables were generated within the REDCap software and Microsoft’s Excel application. All data were de-identified and stored in a password protected domain. Descriptive statistics were used to analyze the data. Chi-square models using Monte Carlo simulation were conducted with p<0.05 [17]. All statistical analyses were conducted using Microsoft’s Excel.
Results
A total of 50 participants completed the questionnaire. The median age was approximately 73 years (±5.4 years) (Table 1), with 32% males and 68% females. The results showed that 56% of the participants reported that their mental health was affected due to the social isolation from the pandemic, and 44% reported that their mental health was not affected. Statistical significance was observed among participants who reported feeling socially isolated and lonely during the pandemic. The results showed that anxiety (x2= 39.29, p<0.001) and depression (x2=27.76, p<0.001) were statistically significant. Worsening of mood, sleep disturbances, loss of interest, appetite changes, weight issues, and concentration difficulties were statistically significant. Statistical significance was also observed for symptom worsening compared to the pre-pandemic period (x2=29.70, p<0.01). About 60% of participants reported that they were not aware of the resources to cope with stress during the pandemic (Table 2). Statistical significance was observed in the living condition and the mental health status due to the COVID-19 pandemic (x2=8.32, p=0.032).
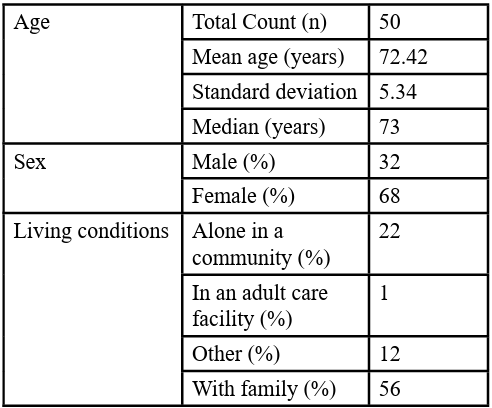
Table 1: Demographic information
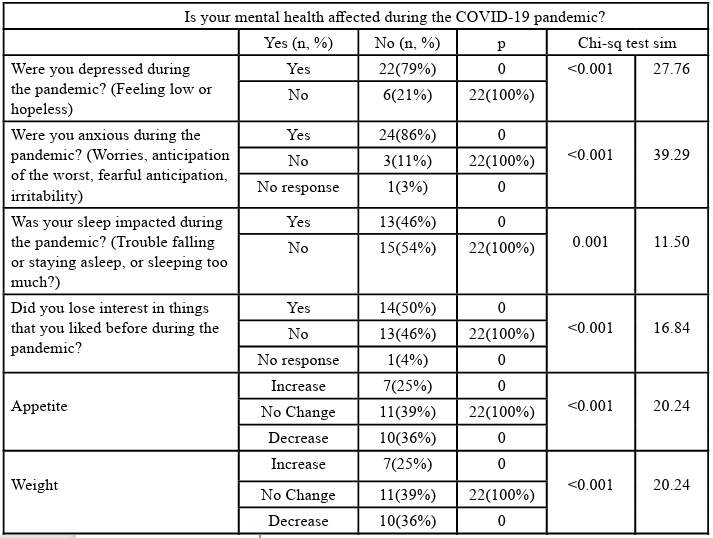
Table 2: Chi-square results of participants’ mental health during the COVID-19 pandemic (last 18 months)
Discussion
About 56% of the participants reported that their mental health was affected by the COVID-19 pandemic. This percentage was greater compared to a recent nationwide survey study conducted in China, which showed that 37% of the 52,730 respondents experienced mental distress during the COVID-19 pandemic [18]. Anxiety and depression were among the main symptoms of social isolation and loneliness [19]. In this study, the percentage of participants who reported anxiety was 48% and the persons who reported depression were 44%. According to a survey of 1,556 older people in China, 37.1% of the seniors experienced depression and anxiety during the pandemic [20]. Other minor symptoms regarding appetite, weight, sleep, and loss of interest were also seen in participants. These results align with the initial results of surveys on the pandemic conducted in China [18] and Iran [21], which showed an increase in psychological distress because of the pandemic. However, as reported by Qiu [18], it is noteworthy that people’s distress did not reach a pathological level (M = 23.65), with only 5% of the sample suffering from severe distress and 29% from mild or moderate distress.
Approximately 42% of the participants reported their symptoms worsened compared to the pre-pandemic period. However, responses from a large panel survey in the UK (n > 70,000) revealed that depression and anxiety, which were very high in March 2020, decreased precipitously in the first few weeks of lockdown and then plateaued [22]. The participants in this study might also have experienced this trajectory with their symptoms and did not know which answer to pick as the response options were binary (Yes/No).
Statistical significance was found for anxiety, depression, sleep, loss of interest, appetite, weight, feeling lonely, symptoms worsening compared to pre-pandemic, and loss of concentration on things. Most of the participants who felt distressed were unaware of the resources during the lockdown period. A few participants (16 participants) among the distressed participants were aware of the resources and obtained help. Statistical significance was also found in the living conditions of the participants. These results are supported by recent studies where researchers found the negative consequences of isolation and the potential for increased loneliness across all age groups, but especially among already isolated older adults [23,24].
There were a few limitations to this study. This analysis was based on observational data, and causal interpretations are not possible. This small sample consisted of geriatric patients who were willing to participate from one psychiatry outpatient clinic in Illinois and findings may not be generalizable; however, whereas this was a relatively small sample of willing participants, this is also a hard to-reach population. Further research with more diverse geriatric patients (i.e., more males and transgender/non-binary), as well as an evaluation of pre- and post-condition records, would provide more thorough results to further understand the impacts of the pandemic on mental health. The study was also based on participants’ memory at that point of time, thus recall bias could be a possibility [25]. To overcome this, the patients were given ample time to answer the questions. There could be some disbeliefs about COVID-19 among the participants. However, the study did show that the majority were affected due to the COVID-19 lockdown.
In conclusion, the pilot study findings suggest that the mental health of geriatric patients was adversely affected by social isolation from the COVID-19 pandemic. It is important to focus on the physical and mental health of vulnerable populations, such as geriatric patients, and to carefully monitor during difficult times, including pandemics and other emergency situations. Public health agencies should also focus on ensuring that they reach out and provide resources to vulnerable populations during difficult times in the future by having appropriate and tailored support services.
Competing Interests:
The authors declare that they have no competing interests.
References
Majumder, J., & Minko, T. (2021). Recent developments on therapeutic and diagnostic approaches for COVID-19. The AAPS journal, 23, 1-22.View
Valtorta, N. K., Kanaan, M., Gilbody, S., Ronzi, S., & Hanratty, B. (2016). Loneliness and social isolation as risk factors for coronary heart disease and stroke: systematic review and meta analysis of longitudinal observational studies. Heart, 102(13), 1009-1016.View
Centers for Disease Control and Prevention, “Considerations for Retirement Communities and Independent Living Facilities”,https://www.cdc.gov/coronavirus/2019-ncov/ community/retirement/index.html, (Accessed Apr. 19, 2021).View
Donovan, N. J., & Blazer, D. (2020). Social isolation and loneliness in older adults: review and commentary of a national academies report. The American Journal of Geriatric Psychiatry, 28(12), 1233-1244.View
U.S. Census Bureau, American Community Survey; Current Population Survey, Annual Social and Economic Supplement 1967 to 2022; Table AD3. Living arrangements of adults 65 to 74 years old, 1967 to 2022; Table AD3. Living arrangements of adults 75 and over, 1967 to 2022.View
Hong Teo R, Hui Cheng W, Jie Cheng L, Lau Y, Tiang Lau S. (2023). Global prevalence of social isolation among community-dwelling older adults: a systematic review and meta analysis. Arch Gerontol Geriatr,107,104904. doi:10.1016/j. archger.2022.104904View
World Health Organization, “Mental health of older adults”, https://www.who.int/news-room/fact-sheets/detail/mental health-of-older-adults, (Accessed December 12, 2022).View
Cacioppo, J. T., & Cacioppo, S. (2018). The growing problem of loneliness. The Lancet, 391(10119), 426.View
Holt-Lunstad, J., & Perissinotto, C. (2023). Social isolation and loneliness as medical issues. New England Journal of Medicine, 388(3), 193-195.View
Murthy. V, “Work and the loneliness epidemic”. Harvard Business Review (Brighton), https://hbr.org/cover-story/2017/09/work and-the-loneliness-epidemic , (Accessed Sep 27,2021).View
Kuiper, J. S., Zuidersma, M., Voshaar, R. C. O., Zuidema, S. U., van den Heuvel, E. R., Stolk, R. P., & Smidt, N. (2015). Social relationships and risk of dementia: A systematic review and meta-analysis of longitudinal cohort studies. Ageing research reviews, 22, 39-57.View
Holt-Lunstad, J., Smith, T. B., Baker, M., Harris, T., & Stephenson, D. (2015). Loneliness and social isolation as risk factors for mortality: a meta-analytic review. Perspectives on psychological science, 10(2), 227-237.View
Corapcioglu, A., & Ozer, G. U. (2004). Adaptation of revised Brief PHQ (Brief-PHQ-r) for diagnosis of depression, panic disorder and somatoform disorder in primary healthcare settings. International Journal of Psychiatry in Clinical Practice, 8(1), 11-18.View
Sawaya, H., Atoui, M., Hamadeh, A., Zeinoun, P., & Nahas, Z. (2016). Adaptation and initial validation of the Patient Health Questionnaire–9 (PHQ-9) and the Generalized Anxiety Disorder–7 Questionnaire (GAD-7) in an Arabic speaking Lebanese psychiatric outpatient sample. Psychiatry research, 239, 245-252.View
Droit-Volet, S., Gil, S., Martinelli, N., Andant, N., Clinchamps, M., Parreira, L., & Dutheil, F. (2020). Time and Covid-19 stress in the lockdown situation: Time free,«Dying» of boredom and sadness. PloS one, 15(8), e0236465.View
Harris, P. A., Taylor, R., Thielke, R., Payne, J., Gonzalez, N., & Conde, J. G. (2009). Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. Journal of biomedical informatics, 42(2), 377-381.View
Hope, A. C. (1968). A simplified Monte Carlo significance test procedure. Journal of the Royal Statistical Society Series B: Statistical Methodology, 30(3), 582-598.View
Qiu, J., Shen, B., Zhao, M., Wang, Z., Xie, B., & Xu, Y. (2020). A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. General psychiatry, 33(2).View
Robinson, E., Sutin, A. R., Daly, M., & Jones, A. (2022). A systematic review and meta-analysis of longitudinal cohort studies comparing mental health before versus during the COVID-19 pandemic in 2020. Journal of affective disorders, 296, 567-576.View
Meng, H., Xu, Y., Dai, J., Zhang, Y., Liu, B., & Yang, H. (2020). Analyze the psychological impact of COVID-19 among the elderly population in China and make corresponding suggestions. Psychiatry research, 289, 112983.View
Jahanshahi, A. A., Dinani, M. M., Madavani, A. N., Li, J., & Zhang, S. X. (2020). The distress of Iranian adults during the Covid-19 pandemic–More distressed than the Chinese and with different predictors. Brain, behavior, and immunity, 87, 124.View
Fancourt, D., Steptoe, A., & Bu, F. (2021). Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: a longitudinal observational study. The Lancet Psychiatry, 8(2), 141-149.View
Armitage, R., & Nellums, L. B. (2020). COVID-19 and the consequences of isolating the elderly. The Lancet Public Health, 5(5), e256.View
Shaw, M.L. ‘’Preventing loneliness among the senior population during the COVID 19 crisis’’. Am J Manag Care (In Focus Blog). Retrieved from https://www.ajmc.com/view/preventing loneliness-among-the-senior-population-during-the-covid19 crisis. Retrieved on Feb 2022.View
Catalogue of Bias Collaboration, Spencer EA, Brassey J, Mahtani K. ‘’Recall bias’’. In: Catalogue Of Bias. https://www. catalogueofbiases.org/biases/recall-bias, (Accessed on Jan 2023).View