
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 8 (2024), Article ID: JPHIP-222
https://doi.org/10.33790/jphip1100222Research Article
A Needs Assessment of Mental Healthcare Among inmates in Madison County Jail: Recommendations for Improvement
Huaibo Xin1*,Ph.D, MD, MPH, Denise J. Bradley, MS2, Deborah L. Humphrey2, MBA, BSN, RN, Siglock, Alyson3, MPH
1Professor of Public Health, Department of Applied Health, Southern Illinois University Edwardsville, Campus Box 1147, SIUE, Edwardsville, IL62026, U.S.
2Madison County Mental Health Board, Edwardsville, IL,U.S.
3Madison County Mental Health Alliance,U.S.
*Corresponding Author Details: Huaibo Xin, Ph.D, MD, MPH, Professor of Public Health, Department of Applied Health, Southern Illinois University Edwardsville, Campus Box 1147, SIUE, Edwardsville, IL62026, U.S.
Received date: 20th December, 2023
Accepted date: 25th January, 2024
Published date: 27th January, 2024
Citation: Xin, H., Bradley, D. J., Humphrey, D. L., & Alyson, S., (2024). A Needs Assessment of Mental Healthcare Among inmates in Madison County Jail: Recommendations for Improvement. J Pub Health Issue Pract 8(1): 222.
Copyright: ©2024, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
The current study examined the inmates’ mental healthcare needs in local county jails in Madison County, Illinois and explored approaches for future improvement. It used a mixed method with both a quantitative descriptive study design and a qualitative case study design. Non-probability sampling was used to recruit study participants. Mental health screening data from 222 adult inmates at a local Madison County jail were included in the quantitative study, and 15 professionals working with Madison County’s criminal justice system participated in the qualitative case study to complete an online in-depth survey. Results indicated that at the initial screening, about 30.6% of inmates reported that they had a psychiatric history (n=68), and 69.4% did not think that they ever had a psychiatric history (n=154). However, at the second assessment, 50 (23%) more inmates showed psychiatric symptoms. Female inmates were more likely to report a psychiatric history than males (40% vs. 30%); inmates who were younger than 48 years old had a higher rate of psychiatric history than those at the age of 48 and above (43.7% vs. 33%); and Hispanic inmates had the highest rate of psychiatric history compared to other races (75.0%). Participants in the case study stated that there was a significant lack of mental healthcare services provided in diagnosis, treatment, and referral while a considerable proportion of jail inmates were suffering from serious mental illness. Recommendations were made for future improvement, such as strengthening partnerships with mental health professionals and agencies to ensure the adequate and prompt mental health services in jails; increasing facilities to host mentally ill inmates; improving the comprehensiveness and accuracy of mental health screening/assessment tools. The study advocated for structural/systemic changes and more innovative and evidence-based practice to address inmates’ mental health concerns.
Keywords: Mental Healthcare, Inmates, Jails, structural/systemic changes, evidence-based practice
Introduction
The 2011-2012 U.S. National Inmate Survey surveyed a total of 106,532 adult inmates in 233 state and federal prisons, 358 jails, and 15 special facilities. Approximately, 24% of prisoners reported that they were told they had a major depressive disorder compared to 31% of jail inmates. A major depressive disorder was the most prevalent diagnosis being reported among both prisoner and jail inmates [1]. Compared to the prevalence of serious psychological distress (SPD) among the general U.S. population, respectively, it was three times higher among prisoners and five times higher among jail inmates. More jail inmates reported SPD than prisoners; more female prisoners and jail inmates reported SPD in the past 30 days; and more white prisoners and jail inmates reported SPD in the past 30 days than black and Hispanic prisoners and jail inmates [1]. The 2016 U.S. Survey of Prison Inmates collected data from 24,848 adult prisoners in 364 state and federal prisons. About 43% of state and 23% of federal prisoners reported that they had a history of mental illness; about 14% of state prisoners and 8% of federal prisoners had SPD; repeatedly, more female prisoners and white prisoners indicated SPD in the past 30 days [2]. Consistently, a thorough review of articles published between 1989 and 2013 focusing on the prevalence of mental distress in prisons in 16 states suggested that regardless of the discrepancies in definitions of mental disorder, sampling strategies, etc., both current and lifetime prevalence rates of mental disorders among incarcerated populations were higher than in non-incarcerated populations [3]. Later studies further confirmed these previous findings, as well as stressed the age, sex, and racial disparities and delays in mental health diagnosis and treatment [4,5]. In 2020, the National Alliance on Mental Illness continued to report that in the U.S., about 37% of state and federal prisoners and 44% of jail inmates suffered from mental illness; about 66% of female prisoners had a history of mental illness, which was twice higher than the percentage of male prisoners; the number of times among people with serious mental illness being booked into jails was about 2 million each year [6].
Current literature suggested that the rapid and continued growth of mentally ill inmates in the U.S. prisons and jails was a result of the “failure to treat addiction and mental illness as medical conditions” [7], deinstitutionalization, and transinstitutionalization [7-9]. Addiction often anticipates later or co-occurring behavioral and mental health problems [7]. Rich et al. argued that jails had become the largest facilities to house psychiatric patients in the U.S. instead of hospitals. The burden of care for drug or alcohol addiction, and mental illness had been shifted to jails and prisons due to transinstitutionalization [7]. Raphael and Stoll’s 2013 study estimated that between 1980 2000, there were significant transinstitutionalization rates for all men and women with a relatively larger transinstitutionalization rate for men compared to women and with the largest rate for white men compared to other ethnicities [8]. Similarly, a study conducted among 79,211 inmates who began serving sentences between 2006 and 2007 indicated that inmates with major psychiatric disorders had a substantially increased risk of multiple incarcerations; inmates with bipolar disorder were about three times more likely to have multiple incarcerations compared to inmates had no major psychiatric disorders [10]. Moreover, during fiscal year 2005 and 2006, a total of 4,544 incarceration records from a county jail system were obtained and reviewed. Records showed that substance-related diagnoses, and schizophrenia, bipolar, or other psychotic disorder diagnoses were among some of the major risk factors for being incarcerated or re-incarcerated [11]. The 2006 special report of Bureau of Justice Statistics also revealed that among the incarcerated with mental illness, being female, white, or young inmates, homeless and foster care experiences, low rates of employment and high rates of illegal income, past physical or sexual abuse, substance dependence or abuse were much more common [12]. Green et al. and Wolff et al. further illustrated the relationship between high prevalence of traumatic life events and an increased risk of mental illness among inmates [13,14]. In addition, incarceration was specifically related to subsequent long-lasting mood disorders and aggravated mental distress due to social and physical isolation, loss of autonomy, lack of purpose, witnessing violence, family disconnection, overcrowding, etc. [7,15,16,17].
Deinstitutionalization and transinstitutionalization both appear to be much costly and ineffective. Based on the 2018 data, the average cost of holding people in criminal justice system was more expensive than the cost of psychiatric treatment in a community hospital. Vanable estimated and explained that the cost of 35 to 83 days in a federal prison or six to 15 days in a juvenile detention center would suffice for a psychiatric hospitalization with a promising treatment and recovery [18]. Studies showed that mentally ill inmates also tended to be incarcerated longer than other inmates because they were more likely to be charged with facility rule violations and accounted for more infractions [19]. Unsurprisingly, Van Dorn et al. compared service costs from 2005 to 2012 in Florida between 1,263 individuals who were at least arrested once and individuals who were not. The average costs and the average number of encounters for acute care services including psychiatric hospitalization and emergency mental health services among individuals who were involved in the criminal justice system were significantly higher, and the costs remained higher even after the justice system costs were excluded. In particular, high medication possession and receipt of routine outpatient services could prevent individuals from being arrested, which were significantly lacking among individuals who were ever arrested [20]. Adding to the existing literature, the purpose of the current study is to evaluate the inmates’ mental healthcare needs in local county jails in Madison County, Illinois, U.S. and to identify approaches for future improvement.
Materials and Methods
Subjects
The study used a mixed method approach with a quantitative descriptive study design and a qualitative case study design. Non probability sampling strategies, including convenience sampling, criterion sampling, and snowball sampling, were applied to recruit participants for the qualitative study. Anonymous quantitative mental health screening records completed in 2021 with 222 adult inmates who were arrested and placed in a local county jail in Madison County, Illinois during that time, were obtained, reviewed, and included. Through personal connections and snowball sampling, a total of 29 individuals who were working with Madison County’s criminal justice system (e.g., mental health counselors, nurses, law enforcement officers) were contacted and invited to participate in the qualitative case study for further information. Individuals who were working for other districts were excluded.
Measures
A 14-item self-reported mental health screening questionnaire administered by the county sheriff’s office and used for inmates at Madison County jails at the entry, collected initial data on demographics, including race, age, and sex, psychiatric history, and yes or no binary questions like holds a position of respect in the community; appears to feel unusually embarrassed or ashamed; expresses thoughts about killing or injuring self; has a suicidal plan and/ or suicide instrument in possession; has previous suicide attempt; shows signs of depression; appears overly anxious, afraid, or angry.
The case study used an online survey instrument with nine open ended questions for in-depth information specifically related to Madison County jails, including (1) Based on your experience, what could be your major concerns about current mental healthcare services? (2) What mental healthcare services, including different types of therapies, screening/diagnosis, referrals, etc., are unavailable to inmates due to personnel, financial…constraints, which you think should be provided? (3) What are the diagnostic/screening tools regularly used for mental illness? (4) Among inmates with any form of mental illness, in your opinion, what could be a rough estimate of the percentage of inmates with mental illness who have a serious mental illness? (5) In your opinion, what could be a rough estimate of the percentage of inmates with a serious mental illness who have received any form of psychiatric treatment? (6) What could be your rough estimate of the time it usually takes for an inmate to receive any form of mental healthcare before they are convicted? (7) What could be the assistance that correctional officers and other personnel may need to work with inmates with any form of mental illness, such as documented policy/ protocol for a proper referral, mental health first aid training, etc.? (8) What are the differences you observed in availability and accessibility of mental healthcare services before the COVID-19 pandemic occurred compared to during the COVID-19 pandemic? (9) What could be the approaches (e.g., structural, system, policy, or environmental, etc.) you would like to suggest to improve mental healthcare for inmates? The questionnaire was reviewed and validated by both mental health and public health professionals.
Procedures
The current study was approved by university’s Institutional Review Board. The quantitative portion of this study used secondary/existing mental health screening data collected from inmates in a Madison County jail. A total of 222 de-identified aggregated electronic screening records were included in this study. Only race, sex and age were specified as subjects' characteristics and records were numerically numbered. In Fall 2021, a case study was conducted to further assess inmates’ mental healthcare needs in Madison County jails, Illinois, and identify approaches for future improvement. A Qualtrics online anonymous survey with nine open-ended questions was sent out to 29 individuals who worked closely with inmates in Madison County jails and were mental health counselors, nurses, probation officers, correctional officers, and individuals from the Public Defender’s Office. A total of 15 of these individuals (52% response rate) completed the survey and provided in-depth information, which met the data saturation.
Analysis
The quantitate data were analyzed using IBM SPSS and descriptive statistics (e.g., frequencies, percentages) on variables, including age, sex, race, and each of these questions on the mental health screening instrument. Within-case theme analysis was applied to analyze the qualitative data. Themes were generated under each domain defined by the open-ended questions, such as severity of inmates’ mental illness, availability and accessibility of mental healthcare, adoption of diagnostic/screening tools, law enforcement training needs, and approaches for improvements.
Results
Among the 222 adult inmates who received the screening at the entry, 95.5% of them were male (n=212), and only 4.5% of them were female (n=10). Besides eight Hispanic inmates, the numbers of white and black inmates were equal (n=107). Approximately, 35.6% of the inmates were younger than 28 years old (n=79); 36% of them were between 28 and 38 years old (n=80); 20.3% of them were between 38 and 48 years old (n=45); and only 8.1% of them aged 48 years or older (n=18).
Data shows (Table 1) that at the initial screening, about 30.6% of inmates reported that they had a psychiatric history (n=68), and 69.4% did not think that they ever had a psychiatric history (n=154). All inmates reported that they didn’t hold a position of respect in the community. More than 95% of the inmates denied that they felt unusually embarrassed or ashamed, had thoughts about killing or injuring themselves, had a suicide plan, instrument in possession, or previous suicide attempt, had signs of depression, anxiety, were acting and/or talking in a strange manner, were individual incoherent, had signs of withdrawals, or had a family member ever committed suicide. More than 80% of these individuals reported that they did not have normal eating habits (n=178), and about 77% of them did not have normal sleeping habits (n=171). After being broken down by sex, age, and race (Figure 1), data also indicated that female inmates were more likely to report a psychiatric history than males (40% vs. 30%); inmates who were younger than 48 years old had a higher rate of psychiatric history than those at the age of 48 and above (43.7% vs. 33%); and Hispanic inmates had the highest rate of psychiatric history compared to other races (75.0% vs. 35.5% vs. 22.4%).
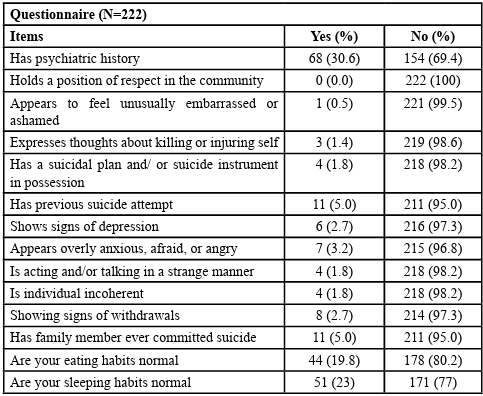
Table 1:Descriptive Statistics of 14-Item Self-Reported Mental Health Screening Questionnaire (N=222)
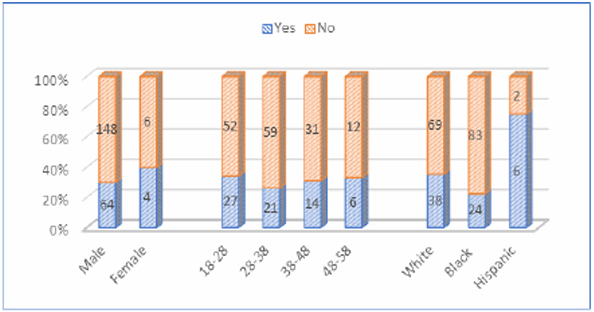
Figure 1: Self-Reported Psychiatric History by Sex, Age, and Race (N=222)
However, at a later diagnostic assessment, 50 (23%) more inmates showed psychiatric symptoms in addition to the 68 inmates who initially reported that they had a psychiatric history. Among those 50 inmates who had the psychiatric symptoms at a later diagnostic screening, 46 of them were male inmates, and 4 were females; 28 of them were white, 20 were black, and 1 was Hispanic.
Themes also emerged from the qualitative data obtained by the case study.
Severity of Inmates’ Mental Illness
Theme 1 27% of respondents indicating 40% or more of inmates with mental illness had a serious mental illness
“50%”
“50-75%”
“70 percent”
“40%”
Theme 2 40% of respondents indicating 20% to 39% of inmates with mental illness had a serious mental illness
“20%”
“Of the mentally ill clients in the jail, I would estimate that 20% are seriously mentally ill.”
“30 percent”
“25% maybe higher”
“At least 20% of the population with SMI.”
Theme 3 60% of respondents indicating only 10% or less of inmates with a serious mental illness received some form of psychiatric treatment
“5%”
“1%”
“2 percent”
“10 Percent”
Theme 4 Only 20% of respondents indicating most of inmates with a serious mental illness received some form of psychiatric treatment
“Almost all of my seriously mentally ill clients have received some form of mental health treatment, but it usually consists of short hospital stays with little follow up.”
“Depends on the type of treatment. The jail provides medication for those that they know have a prescription. A Dr. also visits the jail regularly (weekly), and he can prescribe medication. If someone appears to be seriously ill, an outside agency is contacted (I believe). That outside agency would then do an assessment. Other than medication, I do not believe there is any other form of mental health treatment or therapy for incarcerated individuals at the county jail.” “Most (95% or more) of the inmates with serious mental illness have already received some form of psychiatric treatment either as a juvenile or as an adult.”
“Most of the severe mentally ill clients at the jail have received some type of mental health treatment in the past.”
Availability and Accessibility of Mental Healthcare
Theme 1. Significant mental healthcare needs among inmates but limited mental healthcare services provided in diagnosis, treatment, and referral
“That there is not enough. This is not a "knock" on the Madison County Jail. Mental Health services and interventions, on a national level, have been lacking throughout the criminal justice/corrections profession for years.”
“We currently have a large percentage of inmates that suffer from mental illness and there are essentially no service offered to them.”
“Very few Madison County Jails have ongoing therapy services, rather crisis only services for most.”
“That there are not enough professional services for the inmates that come in to the Madison County Jail.”
“My major concern about the mental healthcare services in the Madison County Jail is that the only resource available to detainees is to speak with a crisis worker on certain days.”
“We have a person on-site for them to talk to twice weekly. There are no other on-site services other than that.”
“I am not sure. I know there is a crisis service but other than that I do not think there are very few [of] it not any.”
“They have Crisis Services, but not sure what that entails. I hear many stories where clients are unable to get the right meds at the jail.”
“Medications, medical and psychiatric. Therapy. Evaluations. Humane treatment. Psych care in general is lacking.”
“The only resource available to them is one on one counseling with a mental health professional.”
“Many of my mentally ill clients do not access to housing or reliable transportation which is obviously a barrier to obtaining any mental health services.”
Theme 2. A prolonged period of time to wait for mental healthcare services
“The length of time it takes to get mental health facilities to intake detainees in need of help.”
“When a detainee is sent to a mental health facility, the wait for a spot to open for them takes an excessive amount of time, in my opinion.”
Theme 3. Lack of proper and consistent medication for mentally ill inmates
“Based on my experience, the major concern for mental health care services for inmates is them getting proper medication and giving it to them consistently.”
Theme 4. Lack of separate facilities/housing/jail cells for mentally ill inmates
“That there are not separate facilities for mentally ill prisoners (for example: a segregated wing).”
“Jail is used to house the mentally ill instead of placing them in supervised living facilities.”
Theme 5 Ideals of improving inmates’ mental healthcare
“I think that with the integration of tablets in our facility in the near future, I would like to see either some type of app or game on the tablet that could help detainees with mental illness.”
“I believe that individuals should be screened and be allowed to participate in some form of counseling prior to the point of needing crisis intervention.”
“It would be beneficial to have a full or part-time Psychologist or Psychiatrist. Cognitive therapy and informed trauma therapy should also be available.”
“Most of these individuals need a mental health advocate to help them follow through and continue with services so they don’t end up coming back into the court system. Also, most agencies have a long wait for services which in turn leave the inmate w/o services which they need immediately.”
““Ideally the jail would provide therapy and medication to those that are incarcerated for an extended period of time and offer referrals for treatment, medication and housing when they are released.”
“Ongoing therapy, screening for suicide risk, linkage to housing upon release.”
Adoption of Diagnostic/Screening Tools
Theme 1 Mental health screening tool(s) used for inmates’ mental illness
“None by regular staff. The mental health person does evaluate them. I have [no] idea what she uses for her guidelines.”
“Screening past Dx, med list.”
“We have mental health staff come to the jail to assess inmates in need.”
“During intake there is a brief mental health screening process and also there are some mental health questions during a detainee’s 14 day assessment with the nursing staff.”
“During, or immediately following, transportation, in custody individuals are asked if they have any mental health issues, or if they are having thoughts of suicide.”
“The only way an inmate gets screened is if either if a note [psychiatric note] is made in the police report, the client's attorney recommends one, or the judge sees that the inmate might be unfit. Then the inmate would be referred to an agency for a mental health screening.”
Theme 2 Crisis assessment tool(s) used for inmates’ mental crisis
“IMCAT (Illinois Medicaid Crisis Assessment Tool), Stanley Brown Safety Plans (for those who have partnerships with local Community Mental Health agencies that come in and assess for crisis.”
“Crisis Worker 16 hours weekly for 300+ inmates.”
Law Enforcement Needs of Training and Assistance
Theme 1 Mental health/mental health first aid training to improve awareness and response of mental illness
“I think more mental health training would help.”
“Training to recognize when an inmate has a mental health issue.”
“I think that more mental health training would be beneficial for us correctional officers, but also being able to recognize the mental illness quicker would be more beneficial.”
“Mental Health First Aid training for sure. The probation department needs it as well as we receive mentally ill cases with no support or direction. All correctional officers should be trained in some style of mental health intervention technique.”
Theme 2. Mental health policies and protocols in place to provide consistent guidance
“Clear policies on when inmates need assessed, clear information for inmates on services requested and process to access those services.”
“We have policies in place.”
“Protocol”
Theme 3. Established partnerships with mental health professionals and agencies to provide consistent assistance
“The presence of mental health professionals that have access to recourses to help the clients would be paramount.”
“ A partner agency would probably be the most cost effective and realistic approach. They could provide personnel, resource materials, and even training.”
“They need the assistance of licensed and trained mental health professionals.”
Theme 4 Continued funding support for mental healthcare services
“They need funding to provide all services in the jail while individuals wait on evaluations or even trial.”
Theme 5. Reliable and valid mental health screening tool(s)
“A highly reliable screening tool to use on each inmate that comes into the Madison County Jail.”
Approaches for Improvements
Theme 1. Strengthening partnerships with mental health professionals and agencies
“As I indicated above, we need mental health professionals who go to the jail and that have the ability to refer the clients to services when they are released.”
“Partnering with a local mental health provider.”
“If we could have a psychologist make rounds at the jail at least a couple times a week, I think it could help.”
“ A medical doctor and psychiatrist should be on staff. A psych trained nurse should be employed at the jail. Therapists should be allowed in routinely.”
“A doctor that comes to the facility to see detainees that are in need of care. Not just to evaluate them for trial fitness.”
Theme 2 Increasing facilities to host mentally ill inmates
“The state needs to open more facilities to house inmates in the county jails.”
“They would be better served to be sent to a mental facility.”
“First and foremost, DHS [Department of Human Services] needs more beds and need to be held accountable for getting the most seriously ill clients out of the jail and into their facility.”
“A separate facility for inmates with serious mental issues.”
Theme 3. Improving mental health screening/assessment tool(s)
“A highly reliable screening tool”
“ A comprehensive assessment of where the prisoner is at in terms of their mental state at point of entry. This would help in the prisoners' care and also help in safety for the officers.”
Theme 4. Changing/establishing policies and procedures to improve inmates’ mental healthcare access
“I think that maybe putting a policy in place to help detainees with mental illness would be beneficial and getting them that help they need quicker.”
“Access to mental health care should be similar to the process used to receive physical health care. IF the inmate is having trouble, they should be allowed to put in a ticket allowing them some access to a mental health professional. The jail CO's [Correctional Officer] should also be able to either refer or do an assessment on an inmate that is exhibiting concerning behaviors and then let a mental health professional know of their concerns.”
“There’s should be policies implemented to ensure mentally ill inmates are in a separate area of the jail and receive proper care.”
Theme 5. Continuing to seek opportunities for funding, advocacy, and training to improve inmates’ mental healthcare access
“An agency which could start looking at services for the inmate before he/she gets out of jail and once the inmate is released and a mental health advocate assigned to an inmate if it is deemed, he/she might have mental health issues.”
“Funding”
“Everyone at the jail should be trained to recognize mental illness and how to advocate for treatment.”
Discussion
Results are consistent with the current literature [1-6]. Mental illness was prevalent among inmates in Madison County jails. Female inmates, inmates younger than 48 years old, or Hispanics in this study appeared to be more susceptible to mental illness. Significant mental healthcare needs among inmates but limited mental healthcare services provided in diagnosis, treatment, and referral; a prolonged period of time to wait for mental healthcare services; lack of proper and consistent medication for mentally ill inmates; and lack of separate facilities/housing/jail cells for mentally ill inmates were among the major concerns expressed by the survey participants working in the county criminal justice system. The survey participants further demonstrated the needs of strengthening partnerships with mental health professionals and agencies to ensure the adequate and prompt mental health services in jails; increasing facilities to host mentally ill inmates; improving the comprehensiveness and accuracy of mental health screening/assessment tools; changing/establishing policies and procedures to expand inmates’ mental healthcare access; and continuing to seek opportunities for funding, advocacy, and training to improve inmates’ mental healthcare access, including “an agency which could start looking at services for the inmate before he/she gets out of jail and once the inmate is released, a mental health advocate assigned to an inmate if it is deemed he/she might have mental health issues”. Similarly, in Mulvey and Schubert’s study, they discussed five aspects for improvement (1) “expand the reach of standard and innovative mental health services in jails and prisons to avert crises related to psychiatric deterioration”; (2) “divert mentally ill individuals charged with less serious crimes out of the criminal justice process at the earliest stages of official processing”; (3) “enrich training of criminal justice personnel” so they have the knowledge and skills to react to individuals who are mentally ill; (4) use individuals’ mental health data more effectively and collect consistent and actionable data that can aid decision-making; (5) “promote interdisciplinary aftercare programs for people with mental illness when they are released from jails and prisons, and return to the community” [21]. In Kennedy-Hendricks et al.’s review, within the Sequential Intercept Framework used for mental and substance use disorders, existing interventions were identified, which can effectively reduce mentally ill inmates’ criminal justice involvement, such as inclusion of trained law enforcement on a crisis response team, collaboration between law enforcement and behavioral health agencies, pre-trial diversion, linkage established between discharged inmates, and health and social services, supported housing and employment after discharge [22].
Specifically, Testa summarized diversion into pre-booking diversion and post-booking diversion. Pre-booking diversion aimed to prevent mentally ill individuals from being arrested and diverts them to proper care through using strategies like having specialized law enforcement officers who experienced crisis intervention training, can recognize signs and symptoms of mental illness, and have communication and de-escalation skills; or having law enforcement officers partnering with mental health professionals on a crisis response team [23]. Post-booking diversion aimed to divert individuals who had been arrested or charged to mental healthcare system through jail-based and court-based diversion programs before being sentenced and incarcerated [23]. The Eleventh Judicial Circuit Criminal Mental Health Project (CMHP) in Miami-Dade County, FL is a successful application of pre-booking and post-booking diversions. This ongoing program was established in 2000 to “divert individuals with serious mental illnesses away from the criminal justice system and into comprehensive community-based treatment and support services” [24]. The CMHP pre-booking diversion also involves trained law enforcement officers on a crisis response team [24]. The Stepping Up initiative established in 2015 is another example of “building community-based services and supports to reduce incarceration/reincarceration” through interdisciplinary collaborations [25]. These early intervention strategies have been proven to be effective to intercept jail entries/re-entries and alleviate overcrowding in jails and prisons [20,23-27].
Significantly strengthening mental health services in jail/prison is also crucial and urgent [28]. As one of the survey participants in the current study stated that “there is not enough. This is not a "knock" on the Madison County Jail. Mental Health services and interventions, on a national level, have been lacking throughout the criminal justice/corrections profession for years.” Forrester et al. described the essential mental health service needs in jail/prison settings as “Screening, Triage, Assessment, Intervention and Reintegration (STAIR)” [29]. More effective and innovative psychological/ psychiatric assessment tools and treatment approaches are needed. Samele et al.’s study found that establishing an open referral system to receive referrals from inmates, families, and others, having a health nurse to screen all new inmates at the entry, and triaging emergency and non-emergency cases were deemed to be successful [30]. Other scholars also believed that training correctional officers about mental health crisis response and management, such as brain’s response to trauma and trauma-informed care, would hugely and positively impact inmates’ mental well-being [27]. A comprehensive curriculum was recently developed to train correctional officers about mental health issues in the criminal justice system, signs and symptoms of mental illness, screening and response to mental illness, and self-care for correctional offices. Training outcomes were favorable [31]. Simpson and colleagues recently conducted a systematic review of correctional mental health services using STAIR as a framework. Their findings suggested that the greatest knowledge gained through research studies was in the areas of screening, triage, psychological therapies such as cognitive behavioral therapy (CBT), and reintegration in certain jurisdictions. However, even with independently validated screening tools, false positive rates could be high; there was a lack of evidence or high-quality evidence of efficacy and effectiveness of many other psychological therapies and treatment modalities other than CBT; evidence from reintegration studies was often not generalizable due to jurisdictional specifics [32].
Conclusion
Mental illness among inmates remains alarming, and their needs of mental healthcare remain significant. There has been an “increased risk of suicide, self-harm, violence, and victimization” among inmates with mental illness [33]. Policies/procedures need to be established/changed to ensure the availability and accessibility of mental healthcare for mentally ill inmates through strategies like diversion, expansion of in-jail/prison services, cross system collaborations, community-based programs, housing and employment, and social and medical benefits [20,21-27,34]. More research/evaluations should be done to support innovations in mental healthcare and evidence-based practice in jail/prison settings, and inform a structural/systemic change [32,34].
Competing Interests:
The authors declare that they have no competing interests.
References
Bronson, J., & Berzofsky, M. (2017). Indicators of mental health problems reported by prisoners and jail inmates, 2011 12. Bureau of Justice Statistics, (Special Issue):1-16. https://bjs. ojp.gov/content/pub/pdf/imhprpji1112.pdfView
Maruschak, L. M., Bronson, J., Alper, M. (2021). Indicators of mental health problems reported by prisoners: Survey of prison inmates, 2016. https://bjs.ojp.gov/library/publications/ indicators-mental-health-problems-reported-prisoners-survey prison-inmates View
Prins., S. J. (2014). Prevalence of mental illnesses in US state prisons: A systematic review. Psychiatric Services. 65(7):862 872. DOI: 10.1176/appi.ps.201300166View
Gottfried, E. D., & Christopher, S. C. (2017). Mental disorders among criminal offenders: A review of the literature. Journal of Correctional Health Care. 23(3):336-346. DOI: 10.1177/1078345817716180 View
Al-Rousan, T., Rubenstein, L., Sieleni, B., Deol, H., Wallace, R. B. (2017). Inside the nation’s largest mental health institution: A prevalence study in a state prison system. BMC Public Health. 17(1):1-9. DOI: 10.1186/s12889-017-4257-0 View
National Alliance on Mental Illness. (2023). Mental Health by the numbers, https://nami.org/mhstatsView
Rich, J. D., Wakeman, S. E., Dickman, S. L. (2011). Medicine and the epidemic of incarceration in the United States. The New England Journal of Medicine. 364(22):2081-2083. DOI: 10.1056/NEJMp1102385View
Raphael, S., & Stoll, M. A. (2013). Assessing the contribution of the deinstitutionalization of the mentally ill to growth in the US incarceration rate. The Journal of Legal Studies. 42(1):187-222. DOI: 10.1086/667773View
Harcourt, B. E. (2011). Reducing mass incarceration: Lessons from the deinstitutionalization of mental hospitals in the 1960s. Ohio State Journal of Criminal Law. 9:53-87. DOI: 10.2139/ ssrn.1748796View
Baillargeon, J., Binswanger, I. A., Penn, J. V., Williams, B. A., Murray, O. J. (2009). Psychiatric disorders and repeat incarcerations: The revolving prison door. American Journal of Psychiatry. 166(1):103-109. DOI: 10.1176/appi. ajp.2008.08030416View
Hawthorne, W. B., Folsom, D. P., Sommerfeld, D. H., Lanouette, N. M., Lewis, M., Aarons, G. A., ... Jeste, D. V. (2012). Incarceration among adults who are in the public mental health system: Rates, risk factors, and short-term outcomes. Psychiatric Services, 63(1): 26-32. DOI: 10.1176/appi.ps.201000505View
D. J. James, & Glaze, L. E. (2015). Mental health problems of prison and jail inmates. https://biblioteca.cejamericas.org/ bitstream/handle/2015/2829/Mental_Health_Problems_Prison_ Jail_Inmates.pdf?sequence=1&isAllowed=yView
Green, B. L., Dass-Brailsford, P., Hurtado de Mendoza, A., Mete, M., Lynch, S. M., DeHart, D. D., Belknap, J. (2016). Trauma experiences and mental health among incarcerated women. Psychological Trauma: Theory, Research, Practice, and Policy. 8(4):455-463. DOI: 10.1037/tra0000113 View
Wolff, N., Huening, J., Shi, J., Frueh, B. C. (2014). Trauma exposure and posttraumatic stress disorder among incarcerated men. Journal of Urban Health. 91:707-719. DOI: 10.1007/ s11524-014-9871-xView
Edgemon, T. G., Clay-Warner, J. (2019). Inmate mental health and the pains of imprisonment. Society and Mental Health. 9(1): 33-50. DOI: 10.1177/2156869318785424 View
Schnittker, J., Massoglia, M., Uggen, C. (2012). Out and down: Incarceration and psychiatric disorders. Journal of Health and Social Behavior. 53(4):448-464. DOI: 10.1177/0022146512453928View
Quandt, K. R., & Jones, A. (2021). Incarceration can cause lasting damage to mental health. https://www.prisonpolicy.org/ blog/2021/05/13/mentalhealthimpacts/View
Vanable, J. (2021). The cost of criminalizing serious mental illness. https://www.nami.org/Blogs/NAMI-Blog/March-2021/ The-Cost-of-Criminalizing-Serious-Mental-Illness View
Treatment Advocacy Center. (2016). Serious mental illness (SMI) prevalence in jails and prisons. https://www. treatmentadvocacycenter.org/reports_publications/serious mental-illness-prevalence-in-jails-and-prisons/View
Van Dorn, R. A., Desmarais, S. L., Petrila, J., Haynes, D., Singh, J. P. (2019). Effects of outpatient treatment on risk of arrest of adults with serious mental illness and associated costs. Psychiatric Services. 64(9):856-86. DOI: 10.1176/appi. ps.201200406 View
Mulvey, E. P., Schubert, C. A. (2017). Mentally ill individuals in jails and prisons. Crime and Justice. 46(1):231-277. DOI: 10.1086/688461 View
Kennedy-Hendricks, A., Huskamp, H. A., Rutkow, L., Barry, C. L. (2016). Improving access to care and reducing involvement in the criminal justice system for people with mental illness. Health Affairs, 35(6):1076-1083. DOI: 10.1377/hlthaff.2016.0006 View
Testa, M. (2015). Imprisonment of the mentally ill: A call for diversion to the community mental health system. Albany Government Law Review, 8(8):405-438. https://www. albanygovernmentlawreview.org/article/23949.pdfView
Eleventh Judicial Circuit of Florida. (2024). Criminal mental health project. https://www.jud11.flcourts.org/Criminal-Mental Health-Project View
Stepuptogether. (2024). Stepping Up. https://stepuptogether. org/about/the-problem/ View
Pettus-Davis, C., & Epperson, M. W. (2014). From mass incarceration to smart decarceration. https://openscholarship. wustl.edu/cgi/viewcontent.cgi?article=1575&context=csd_ researchView
Stringer, H. (2019). Improving mental health for inmates. Monitor on Psychology. 50(3):46-50. http://www.antoniocasella. eu/archipsy/Stringer_march2019.pdf View
Reingle Gonzalez, J. M., & Connell, N. M. (2014). Mental health of prisoners: Identifying barriers to mental health treatment and medication continuity. American Journal of Public Health. 104(12):2328-2333. DOI: 10.2105/AJPH.2014.302043View
Forrester, A., Till, A., Simpson, A., Shaw, J. (2018). Mental illness and the provision of mental health services in prisons. British Medical Bulletin. 127(1):101-109. DOI: 10.1093/bmb/ ldy027View
Samele, C., Forrester, A., Urquía, N., Hopkin, G. (2016). Key successes and challenges in providing mental health care in an urban male remand prison: A qualitative study, Social Psychiatry and Psychiatric Epidemiology. 51:589-596. DOI: 10.1007/s00127-016-1170-2 View
DeHart, D., & Iachini, A. L. (2019). Mental health & trauma among incarcerated persons: Development of a training curriculum for correctional officers. American Journal of Criminal Justice. 44:457-473. DOI: 10.1007/s12103-019 9473-y View
Simpson, A. I., Gerritsen, C., Maheandiran, M., Adamo, V., Vogel, T., Fulham, L., ... & Jones, R. M. (2022). A systematic review of reviews of correctional mental health services using the STAIR Framework. Frontiers in Psychiatry, 12:1-15. DOI: https://doi.org/10.3389/fpsyt.2021.747202View
Fazel, S., Hayes, A. J., Bartellas, K., Clerici, M., Trestman, R. (2016). Mental health of prisoners: Prevalence, adverse outcomes, and interventions. The Lancet Psychiatry. 3(9):871 881. DOI: 10.1016/S2215-0366(16)30142-0View
American Psychiatric Association. (2022). Decriminalizing mental illness and promoting mental health equity. https://www. psychiatry.org/news-room/apa-blogs/decriminalizing-mental illness View
Zielinski, M. J., Allison, M. K., Brinkley-Rubinstein, L., Curran, G., Zaller, N. D., Kirchner, J. A. E. (2020). Making change happen in criminal justice settings: Leveraging implementation science to improve mental health care. Health & Justice. 8(1):1 10. DOI: 10.1186/s40352-020-00122-6 View